Request for Service Form - CNIB
Request for Service Form - CNIB
Request for Service Form - CNIB

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
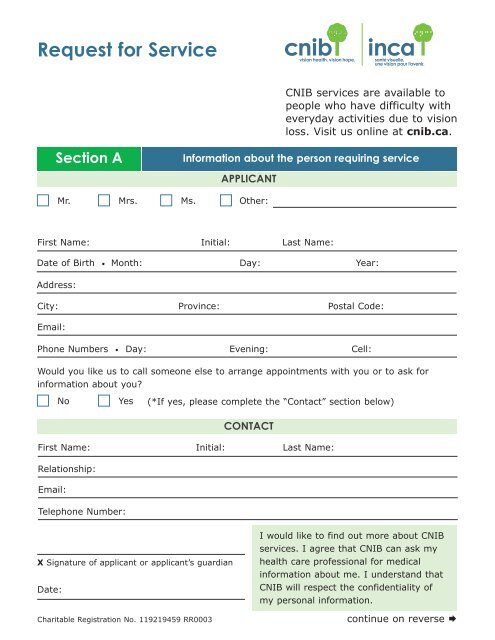
<strong>Request</strong> <strong>for</strong> <strong>Service</strong><strong>CNIB</strong> services are available topeople who have difficulty witheveryday activities due to visionloss. Visit us online at cnib.ca.Section AIn<strong>for</strong>mation about the person requiring serviceAPPLICANTMr.Mrs.Ms.Other:First Name:Initial:Last Name:Date of Birth • Month:Day:Year:Address:City:Email:Province:Postal Code:Phone Numbers • Day:Evening:Cell:Would you like us to call someone else to arrange appointments with you or to ask <strong>for</strong>in<strong>for</strong>mation about you?No Yes (*If yes, please complete the “Contact” section below)CONTACTFirst Name:Relationship:Email:Initial:Last Name:Telephone Number:X Signature of applicant or applicant’s guardianDate:Charitable Registration No. 119219459 RR0003I would like to find out more about <strong>CNIB</strong>services. I agree that <strong>CNIB</strong> can ask myhealth care professional <strong>for</strong> medicalin<strong>for</strong>mation about me. I understand that<strong>CNIB</strong> will respect the confidentiality ofmy personal in<strong>for</strong>mation.continue on reverse
First Name: Last Name: Date of Birth:Section BIn<strong>for</strong>mation about referralREFERRAL SOURCEPlease complete this section when you are referring an applicant to <strong>CNIB</strong>. Ophthalmologist Optometrist Doctor Family Seniors Residence Other: Hospital Community Agency FriendContact Name:Title:Organization: Telephone: ext:Email:Section CEye In<strong>for</strong>mation to be completed by a Doctor Normal Hemianopsia Less than 20° diameter both eyes (describe)BESTCORRECTEDACUITYOD:OS:OU:FIELD OF VISIONDISTANCEOther abnormality: (describe)OD:OS:OU:NEARCORRECTIONOD:Add:OS:Add:KNOWN CAUSE OF VISION LOSSPrimary diagnosis: OD:Other eye conditions: OD:Other related health conditions:Comments:OS:OS:Date of examination:Doctor’s Name: Ophthalmologist Optometrist Telephone:Fax:Email:Other: (describe)X Signature:Date:<strong>CNIB</strong> USE ONLYStatus Y N Date Received:Signature:ICD9 Code: