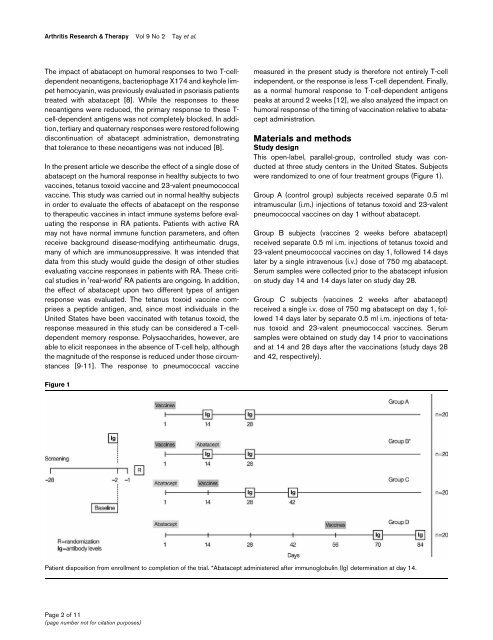
Arthritis Research & Therapy Vol 9 No 2 Tay et al.The impact of abatacept on humoral <strong>response</strong>s <strong>to</strong> two T-celldependentneoantigens, bacteriophage X174 <strong>and</strong> keyhole limpethemocyanin, was previously evaluated in psoriasis patientstreated with abatacept [8]. While the <strong>response</strong>s <strong>to</strong> theseneoantigens were reduced, the primary <strong>response</strong> <strong>to</strong> these T-cell-dependent antigens was not completely blocked. In addition,tertiary <strong>and</strong> quaternary <strong>response</strong>s were res<strong>to</strong>red followingdiscontinuation of abatacept administration, demonstratingthat <strong>to</strong>lerance <strong>to</strong> these neoantigens was not induced [8].In the present article we describe the effect of a single dose ofabatacept on the humoral <strong>response</strong> in healthy subjects <strong>to</strong> twovaccines, <strong>tetanus</strong> <strong>to</strong>xoid vaccine <strong>and</strong> <strong>23</strong>-valent pneumococcalvaccine. This study was carried out in normal healthy subjectsin order <strong>to</strong> evaluate the effects of abatacept on the <strong>response</strong><strong>to</strong> therapeutic vaccines in intact immune systems before evaluatingthe <strong>response</strong> in RA patients. Patients with active RAmay not have normal immune function parameters, <strong>and</strong> oftenreceive background disease-modifying antirheumatic drugs,many of which are immunosuppressive. It was intended thatdata from this study would guide the design of other studiesevaluating vaccine <strong>response</strong>s in patients with RA. These criticalstudies in 'real-world' RA patients are ongoing. In addition,the effect of abatacept upon two different types of antigen<strong>response</strong> was evaluated. The <strong>tetanus</strong> <strong>to</strong>xoid vaccine comprisesa peptide antigen, <strong>and</strong>, since most individuals in theUnited States have been vaccinated with <strong>tetanus</strong> <strong>to</strong>xoid, the<strong>response</strong> measured in this study can be considered a T-celldependentmemory <strong>response</strong>. Polysaccharides, however, areable <strong>to</strong> elicit <strong>response</strong>s in the absence of T-cell help, althoughthe magnitude of the <strong>response</strong> is reduced under those circumstances[9-11]. The <strong>response</strong> <strong>to</strong> pneumococcal vaccinemeasured in the present study is therefore not entirely T-cellindependent, or the <strong>response</strong> is less T-cell dependent. Finally,as a normal humoral <strong>response</strong> <strong>to</strong> T-cell-dependent antigenspeaks at around 2 weeks [12], we also analyzed the impact onhumoral <strong>response</strong> of the timing of vaccination relative <strong>to</strong> abataceptadministration.Materials <strong>and</strong> methodsStudy designThis open-label, parallel-group, controlled study was conductedat three study centers in the United States. Subjectswere r<strong>and</strong>omized <strong>to</strong> one of four treatment groups (Figure 1).Group A (control group) subjects received separate 0.5 mlintramuscular (i.m.) injections of <strong>tetanus</strong> <strong>to</strong>xoid <strong>and</strong> <strong>23</strong>-valentpneumococcal vaccines on day 1 without abatacept.Group B subjects (vaccines 2 weeks before abatacept)received separate 0.5 ml i.m. injections of <strong>tetanus</strong> <strong>to</strong>xoid <strong>and</strong><strong>23</strong>-valent pneumococcal vaccines on day 1, followed 14 dayslater by a single intravenous (i.v.) dose of 750 mg abatacept.Serum samples were collected prior <strong>to</strong> the abatacept infusionon study day 14 <strong>and</strong> 14 days later on study day 28.Group C subjects (vaccines 2 weeks after abatacept)received a single i.v. dose of 750 mg abatacept on day 1, followed14 days later by separate 0.5 ml i.m. injections of <strong>tetanus</strong><strong>to</strong>xoid <strong>and</strong> <strong>23</strong>-valent pneumococcal vaccines. Serumsamples were obtained on study day 14 prior <strong>to</strong> vaccinations<strong>and</strong> at 14 <strong>and</strong> 28 days after the vaccinations (study days 28<strong>and</strong> 42, respectively).Figure 1Patient disposition from enrollment <strong>to</strong> completion of the trial. *Abatacept administered after immunoglobulin (Ig) determination at day 14.Page 2 of 11(page number not for citation purposes)
Available online http://arthritis-research.com/content/9/2/R38Group D subjects (vaccines 8 weeks after abatacept)received a single i.v. dose of 750 mg abatacept on day 1,followed 56 days later by separate 0.5 ml i.m. injections of <strong>tetanus</strong><strong>to</strong>xoid <strong>and</strong> <strong>23</strong>-valent pneumococcal vaccines.Serum samples were obtained for subjects of Groups A <strong>and</strong>B at study days 14 <strong>and</strong> 28, for Group C subjects at study days28 <strong>and</strong> 42, <strong>and</strong> for Group D subjects at study days 70 <strong>and</strong> 84.Healthy male or female subjects (aged 18–65 years inclusive)with a body weight ≥ 60 kg <strong>and</strong> ≤ 100 kg were enrolled. Subjectswere excluded if they had received any live vaccine withinthe prior 4 weeks, had received a <strong>tetanus</strong> booster or pneumococcalvaccine within 5 years or if they had baseline anti-<strong>tetanus</strong>antibodies below clinically detectable levels. Anti-<strong>tetanus</strong><strong>and</strong> anti-pneumococcal (Danish serotypes 2, 6B, 8, 9V, 14,19F <strong>and</strong> <strong>23</strong>F) antibody titers were measured by ELISA at 14<strong>and</strong> 28 days after vaccination by a central labora<strong>to</strong>ry. Abataceptserum concentrations were measured at the same timeas the antibody titers were determined.This study was carried out in accordance with the ethical principlesof the Declaration of Helsinki <strong>and</strong> was approved by InstitutionalReview Boards. All subjects gave informed consent.Drug administration <strong>and</strong> vaccinationAbatacept 750 mg was administered over 30 minutes by i.v.infusion using a calibrated, constant-rate infusion. Tetanus <strong>to</strong>xoidvaccine (Aventis Pasteur Inc., Swiftwater, PA, USA) <strong>and</strong><strong>23</strong>-valent pneumococcal vaccines (Merck & Co Inc., WhitehouseStation, NJ, USA) were administered separately via i.m.injection in either the del<strong>to</strong>id or the lateral mid-thigh.Abatacept <strong>and</strong> antibody assaysSerum samples were used <strong>to</strong> determine antibody levels. Theassay <strong>to</strong> quantify IgG anti-<strong>tetanus</strong> <strong>to</strong>xoid antibody levels wasbased on a previously described methodology [13]. The assay<strong>to</strong> quantify IgG anti-pneumococcal antibody levels was basedon the Procedures of the World Health Organization PneumococcalSerology Reference Labora<strong>to</strong>ries at the Institute ofChild Health, University College, London, UK, <strong>and</strong> on the proceduresof the Department of Pathology, University of Alabamaat Birmingham, AL, USA [14]. All analyses were carriedout at the Center for Vaccine Research <strong>and</strong> Development, StLouis University Health Sciences Center, St Louis, MO, USA.The antibody <strong>response</strong> against <strong>tetanus</strong> <strong>to</strong>xoid vaccine wasexpressed as absolute titers of antibodies. Serum samples forthe quantification of abatacept were collected at baseline,prior <strong>to</strong> vaccinations, <strong>and</strong> at the time when the samples werecollected for antibody determinations [15].Safety assessmentsSubjects were moni<strong>to</strong>red for adverse events (AE), serious AE<strong>and</strong> vital signs prior <strong>to</strong> dosing with abatacept <strong>and</strong> upondiscontinuation.Statistical methodsAll subjects in all four groups were included in the safety analysis.Geometric means <strong>and</strong> the percentage of the coefficien<strong>to</strong>f variation were reported for antibody concentrations. Foreach antibody, point estimates <strong>and</strong> 95% confidence intervalswere constructed for the geometric mean changes from prevaccination<strong>to</strong> postvaccination antibody levels. These constructionswere from the results of repeated-measuresanalyses of covariance on the natural logarithm of the antibodylevels, with the treatment group <strong>and</strong> the study day as fac<strong>to</strong>rs<strong>and</strong> the log of the baseline (prevaccination) antibody level asthe covariate. For each antibody, point estimates <strong>and</strong> 95%confidence intervals for the prevaccination <strong>to</strong> postvaccinationchanges on the log scale were exponentiated <strong>to</strong> obtain estimatesfor geometric means <strong>and</strong> ratios of geometric means(fold increase) on the original scale. A twofold or higherincrease above the baseline levels of specific antibodies wasconsidered a clinically significant or positive immune <strong>response</strong>against <strong>tetanus</strong> <strong>to</strong>xoid <strong>and</strong> <strong>to</strong> each of the seven chosen serotypesof the <strong>23</strong>-valent pneumococcal vaccine [16,17].ResultsThe baseline demographics <strong>and</strong> clinical characteristics of the80 subjects enrolled in this study were similar across the fourgroups. The mean age of subjects was 34–36 years (Table 1).Of the 80 subjects, 77 (96%) completed treatment <strong>and</strong> three(4%) discontinued early from the study.Overall, 59 AE were experienced by 29 subjects (49.2%)treated with abatacept, compared with 25 AE reported in 13subjects (65.0%) who did not receive abatacept (Group A,control group). The most frequently reported AE in Group Asubjects were injection-site pain (50.0%), headache (10.0%)<strong>and</strong> pharyngolaryngeal pain (10.0%). The most frequentlyreported treatment-emergent AE in the abatacept-treatedgroups were headache (20.3%), injection-site pain (10.2%)<strong>and</strong> viral infection (10.2%).One subject (1.7%) in Group D experienced a serious adverseevent of generalized urticaria 5 minutes after the end of thefirst abatacept infusion, which re-occurred at 90 minutespostinfusion. The investiga<strong>to</strong>r reported the event as moderatein intensity <strong>and</strong> probably related <strong>to</strong> the study drug. The subjectwas treated with epinephrine <strong>and</strong> diphenhydramine, remainedhospitalized overnight for observation <strong>and</strong> was discharged onstudy day 2. The event was completely resolved by study day3.Page 3 of 11(page number not for citation purposes)