

PDF version - Australian Prescriber
PDF version - Australian Prescriber
PDF version - Australian Prescriber

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
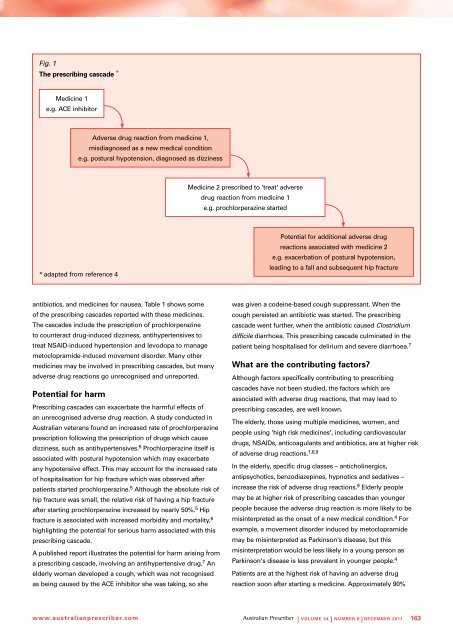
Fig. 1The prescribing cascade *Medicine 1e.g. ACE inhibitorAdverse drug reaction from medicine 1,misdiagnosed as a new medical conditione.g. postural hypotension, diagnosed as dizzinessMedicine 2 prescribed to 'treat' adversedrug reaction from medicine 1e.g. prochlorperazine started* adapted from reference 4Potential for additional adverse drugreactions associated with medicine 2e.g. exacerbation of postural hypotension,leading to a fall and subsequent hip fractureantibiotics, and medicines for nausea. Table 1 shows someof the prescribing cascades reported with these medicines.The cascades include the prescription of prochlorperazineto counteract drug-induced dizziness, antihypertensives totreat NSAID-induced hypertension and levodopa to managemetoclopramide-induced movement disorder. Many othermedicines may be involved in prescribing cascades, but manyadverse drug reactions go unrecognised and unreported.Potential for harmPrescribing cascades can exacerbate the harmful effects ofan unrecognised adverse drug reaction. A study conducted in<strong>Australian</strong> veterans found an increased rate of prochlorperazineprescription following the prescription of drugs which causedizziness, such as antihypertensives. 5 Prochlorperazine itself isassociated with postural hypotension which may exacerbateany hypotensive effect. This may account for the increased rateof hospitalisation for hip fracture which was observed afterpatients started prochlorperazine. 5 Although the absolute risk ofhip fracture was small, the relative risk of having a hip fractureafter starting prochlorperazine increased by nearly 50%. 5 Hipfracture is associated with increased morbidity and mortality, 6highlighting the potential for serious harm associated with thisprescribing cascade.A published report illustrates the potential for harm arising froma prescribing cascade, involving an antihypertensive drug. 7 Anelderly woman developed a cough, which was not recognisedas being caused by the ACE inhibitor she was taking, so shewas given a codeine-based cough suppressant. When thecough persisted an antibiotic was started. The prescribingcascade went further, when the antibiotic caused Clostridiumdifficile diarrhoea. This prescribing cascade culminated in thepatient being hospitalised for delirium and severe diarrhoea. 7What are the contributing factors?Although factors specifically contributing to prescribingcascades have not been studied, the factors which areassociated with adverse drug reactions, that may lead toprescribing cascades, are well known.The elderly, those using multiple medicines, women, andpeople using 'high risk medicines', including cardiovasculardrugs, NSAIDs, anticoagulants and antibiotics, are at higher riskof adverse drug reactions. 1,8,9In the elderly, specific drug classes – anticholinergics,antipsychotics, benzodiazepines, hypnotics and sedatives –increase the risk of adverse drug reactions. 9 Elderly peoplemay be at higher risk of prescribing cascades than youngerpeople because the adverse drug reaction is more likely to bemisinterpreted as the onset of a new medical condition. 4 Forexample, a movement disorder induced by metoclopramidemay be misinterpreted as Parkinson's disease, but thismisinterpretation would be less likely in a young person asParkinson's disease is less prevalent in younger people. 4Patients are at the highest risk of having an adverse drugreaction soon after starting a medicine. Approximately 90%www.australianprescriber.com| Volume 34 | NUMBER 6 | decemBER 2011 163













