Champion Lung Fitness Program Referral Form - The Pacific Lung ...
Champion Lung Fitness Program Referral Form - The Pacific Lung ...
Champion Lung Fitness Program Referral Form - The Pacific Lung ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
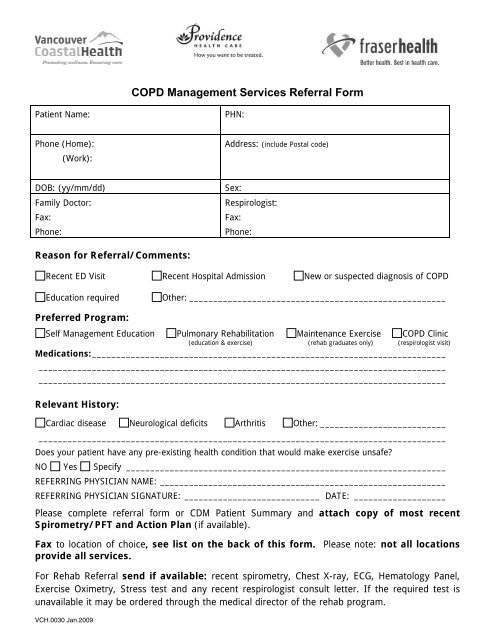
COPD Management Services <strong>Referral</strong> <strong>Form</strong>Patient Name:PHN:Phone (Home):(Work):Address: (include Postal code)DOB: (yy/mm/dd)Family Doctor:Fax:Phone:Sex:Respirologist:Fax:Phone:Reason for <strong>Referral</strong>/Comments:Recent ED Visit Recent Hospital Admission New or suspected diagnosis of COPDEducation requiredOther: _____________________________________________________Preferred <strong>Program</strong>:Self Management Education Pulmonary Rehabilitation Maintenance Exercise COPD Clinic(education & exercise) (rehab graduates only) (respirologist visit)Medications:_________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________Relevant History:Cardiac disease Neurological deficits Arthritis Other: ______________________________________________________________________________________________________________Does your patient have any pre-existing health condition that would make exercise unsafe?NO Yes Specify __________________________________________________________________REFERRING PHYSICIAN NAME: ___________________________________________________________REFERRING PHYSICIAN SIGNATURE: ____________________________ DATE: ___________________Please complete referral form or CDM Patient Summary and attach copy of most recentSpirometry/PFT and Action Plan (if available).Fax to location of choice, see list on the back of this form. Please note: not all locationsprovide all services.For Rehab <strong>Referral</strong> send if available: recent spirometry, Chest X-ray, ECG, Hematology Panel,Exercise Oximetry, Stress test and any recent respirologist consult letter. If the required test isunavailable it may be ordered through the medical director of the rehab program.VCH.0030 Jan.2009
Pulmonary rehabilitation significantly improves dyspnea, exercise endurance, quality of life andrisk of hospitalizations following AECOPD. All Lower Mainland rehab programs providecomprehensive self management education and supervised exercise programs.Speciality COPD Clinics provide a multi disciplinary assessment and treatment plan forsuspected or confirmed COPD patients. <strong>The</strong>se clinics include Respirologist consult and selfmanagement education.Locations Booking & Contact Info Services AvailableVancouverVancouver General Hospital FAX requisition to 604-875-5695Phone: 604-875-4830<strong>The</strong> <strong>Lung</strong> CentreVancouver General HospitalFAX requisiton to 604-875-4695Phone: 604-875-4122St. Paul’s Hospital FAX requisiton to 604-806-9143Phone: 604-806-8115St. Paul’s HospitalEducation Centre<strong>Pacific</strong> <strong>Lung</strong> Health CentreSt. Paul’s HospitalFax requisition to 604-806-8544Phone: 604-806-8808FAX requisition to 604-806-8839Phone: 604-806-8818Kerrisdale Community Centre FAX requisition to 604-267-3993Phone: 604-267-4430West End Community Centre FAX requisition to 604-806-8839Phone: 604-806-8818Pulmonary RehabilitationMaintenance ExerciseCOPD Clinic (includes Respirologist consult andSelf Management Education)Pulmonary RehabilitationMaintenance ExerciseSelf Management EducationSmoking Cessation CounsellingCOPD Clinic ( includes Respirologist consult andSelf Management Education)Pulmonary RehabilitationMaintenance ExerciseMaintenance Exercise onlyNorth ShoreLions Gate Hospital FAX requisition to: 604:984-3766Phone: 604-984-5888RichmondGarratt Wellness Centre FAX requisition to 604-204-2017Phone: 604-204-2007Fraser Health AuthorityCommunity RespiratoryServices (in home service)Fraser NorthiConnect Health CentreNew WestminsterFAX requisition to 604-514-6079Phone: 604-514-6106FAX requisition to 604-523-8801Phone: 604-523-8800Ridge Meadows Hospital FAX requisition to 604-463-1887Phone: 604-463-1855Fraser SouthSurrey Memorial HospitalFAX requisition to 604-585-5922In hospital or YMCAPhone: 604-585-5570Langley Memorial Hospital FAX requisition to 604-533-6449Phone: 604-534-4121 ext 5273Fraser EastChilliwack General Hospital FAX requisition to 604-702-4709Phone: 604-795-4141 ext 614244Abbotsford Regional Hospital FAX requisition to 604-851-4774Phone: 604-851-4700 ext 642215Self Management EducationPulmonary RehabilitationMaintenance ExerciseCOPD Clinic (includes Respirologist consult andSelf Management Education)Smoking Cessation CounsellingSelf Management EducationPulmonary RehabilitationSelf Management EducationSelf Management EducationPulmonary RehabilitationMaintenance ExerciseCOPD Clinic ( includes Respirologist consult andSelf Management Education)Smoking Cessation CounsellingPulmonary RehabilitationMaintenance for O2 dependant patientsSmoking Cessation CounsellingPulmonary RehabilitationMaintenance ExercisePulmonary RehabilitationMaintenance ExerciseSelf Management EducationPulmonary RehabilitationMaintenance ExerciseSelf Management EducationVCH.0030 Jan.2009