Pediatric Dental Treatment Consent Other Guardian ... - ProSites
Pediatric Dental Treatment Consent Other Guardian ... - ProSites
Pediatric Dental Treatment Consent Other Guardian ... - ProSites

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<strong>Pediatric</strong> <strong>Dental</strong> <strong>Treatment</strong> <strong>Consent</strong>I understand the Dentist and <strong>Dental</strong> Assistant may treat my child for the following dental procedures, which may benecessary to provide dental treatment. I also understand I will be explained why treatment will be performed, butunderstand the normal procedure for a first time patient may include a comprehensive or limited exam, dental cleaning,fluoride application, sealants and radiographs(x-rays) as necessary. However, this is subject to change depending on thenumerous factors including patient’s behavior, amount of future work and time.*Application of sealants*Root canals (permanent teeth) pulpotomies (primary teeth)*Porcelain crowns or stainless crowns*Restoration of broken teeth or fillings*<strong>Treatment</strong> of infected teeth or gums*Extractions of 1 or more teeth*Use of supports to safely perform necessary dental procedures*Use of nitrous oxide to help reduce anxiety as needed*Use of local anesthetics, oral anesthesia or oral sedatives as neededMy child’s treatment, alternative methods of treatment, as well as the advantages and disadvantages of each will beexplained to me. We will advise you that although the best results are expected, there is no way within reason ofanticipating complications. Therefore, it is not possible to guarantee the results or care of the treatment. Although theoccurrence is remote, it is known that some risks are associated with dental procedures. I understand and accept thatcertain complications may be fatal or require medical intervention.<strong>Other</strong> <strong>Guardian</strong> <strong>Consent</strong>In the event that I may not be present for my child’s appointment, I, ______________________, give permission for thefollowing adult(s) to make decisions concerning my child’s dental treatment and financial payment. PLEASE PRINT!Name: ______________________________________ Relationship to Patient: __________________________________Name: ______________________________________ Relationship to Patient: __________________________________Name: ______________________________________ Relationship to Patient: __________________________________Name: ______________________________________ Relationship to Patient: __________________________________Parent/<strong>Guardian</strong> Signature_______________________________________ Date ________________________________
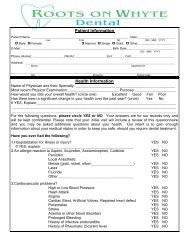
Patient's NamePatlent's SSl.:Patient'e BirthdetePatient's AddresseilvHm#sex Female-MateState_Zipwk#ResB, Party's NameResp. Party's $SNResp. Party's BirthdateResp. Party's Employeflnsurance CarrierMilitary RankAHCCCS PlanHOW DID YOU HEAR ABOUT US?DOYOU HAVE OTHER DENTALCOVERAGE? YES NO1. Are you under a physician's care? Physician's nameSince when?whv?2. When was your last physical exann?3. Are you taking any medication or substances?Wtrat?4. De you have any problems with penicillin, antibiotics, local anestheticsiNovacaini or other allergies?5, Are you allergic to any medication or subgtances? What?6. Do you have any other allergies!7. Are you sensitive to any metalsror latex?8. Are you pregnant or suspect you are?9" Ds you take birth csntrolmedications?1O. Have you ever been treatCd'for heart disease?11. Do you have a pacemaker or an artificial heart valve implant!12, Have you ever had,rheumatic fever?13. Are you awarerof,having a,,hgarl murmur?'14. Do you have high blood pressure!15. HaVe ysU ever had a serioUs,illness or major surgery?16,Haveyoueverhadradiationtreatment,chemotherapy,oranyother?-,lZ, Do you'have soreness, clicking, or popping in your jaw ioint?_18. Do you have any blood disorders, such as anemia, leukemia, hemophiria, etc?_'19. Do you have any artificialjointslprosthesis?2O, Have you ever bled excecsively after being cut or iniured?2:1. Have you ever received a blood transfusion?22-Do you have kidney problems?23. Do you have stomach problems!24. Do you have any liver problems!25. Are you diabetic?26. Do you have asthma?27. Are you HIV positive?48. Doyou have AIDS?29. Have you had or do you test positive for hepatitis?30. Did you read this question?31, Do you or have you had tuberculosis?32. Do you smoke, chew, use snuff or any other forms of tobaces?33. Do you consume alccholic beverages?34. Do you habitually use controlled substances?35.ls there anything else we shouid know about your heatth that we have notcovered in this .r+rrn?YES NOYES NOI E.iIYES NOYES NOYES NOYES NOYES NOYES NOYES NOYES NOYES NOVES NOYES NOYES NOYES NOYES NOYES NOYES NOYES NOYES NOYES NOYES NOYES NOYES NOYES NOvtrq Nr|YES NOYES NOYES NCIYES NOYES NOYES NO*l he_reb3l *-thori.e tleetrllent,and-,the $se of nito.+s oxlde, anestheeia, oral eedation and/or othermedications neceaaary for dental treatment.*The parent or guardEan is required to remain in the DEHTAL OFFICE during their ehild,e der*altreatment!!nitla! tJisitPatient's {Guardia*i Signatur= Date Revlewed ByYtrSN{'I
6ENERAL DE}'ITAL.1729 Poseo San LuisSierra Visto, AZ 85635520 458-2520Thonk you fo,r choosing General Dentol to serve you in your dentol care.We look forword to providingyou with geritie dental service ond treatment.In order to provide you with the outmost in dentol care, we woud like toestqblish some guidelines.Courtesy Reminders:The doy bef ore your appointment we will call you to remind you of your oppointment.Please keep in mind thot this is provided cs o courtesy only ond thot you(potient/porent/guordion) are uhimotely responsible for ke.eping your oppointment.Concellotion PolicyrWe requre o 24 hour odvon ce notice of concellotion. ff you ore unoble to moke ytlurappointment,plese coll us af 458-?520 so that other potients who ore inneedoftreotment con be scheduled occordingly.n@Potienfs who do not shrrw up to their scheduled oppointments without 24 hour notif icqtionwill be considered missed/fsiled oppoinfments. After 3 missed oppointments, pof ients wrllneed to seek dental treotmenthrough anolher dentol provider.Tardiness:Potients who ore more thon 15 mrnutes late f or their treatment oppointment will not beseen ond will need to be rescheduled. Treotment will be rendered ot the discretion of thedentol providerFomify Member AppointmentsrOnly two (2) members of o fomily will be scheduled on the same doy for treatment Thiswill help us limit the omount of missed oppointmenfs. We apologize f or qnv inconve.ntencell'rr:t {toy couseThonk you, for your time ond cooperotion in this monner. We look forword servrng you inyour dentol care.P oti ent / Gurrrdian SignotureDote
1729 Paseo San LuisSierra Vista, AZ 85635I understand that, under the Health Insurance Portability & Accountability Act of 1996(HIPPA), I have certain rights to privacy regarding my protected information. Iunderstand that this information can and will be used to:• Conduct, plan and direct my treatment and follow-up among the• Providers who may be involved in that treatment directly andindirectly.• Obtain payment from third-party payers.• Conduct normal healthcare operations such as quality assessments anphysician certifications.I have been informed by you of you Notice of Privacy Practices containing a morecomplete description of the uses and disclosures of my health information. I have beengiven the right to review such Notice of Privacy Practices prior to signing this consent. Iunderstand that this organization has the right to change its Notice of Privacy Practicesfrom time to time and that I may contact this organization at any time at the addressbelow to obtain a current copy of the Notice of Privacy Practices.I understand that I may request in writing that you restrict how my private information isused or disclosed to carry out treatment, payment or health care operations. I alsounderstand you are not required to agree to my requested restrictions, but if you do agreethen you are bound to abide by such restrictions, but if you do agree then you are boundto abide by such restrictions.I understand that I may revoke this consent in writing at any time, except to the extentthat you have taken action relying on this consent.Patient Name: __________________________________________________________Patient/<strong>Guardian</strong>: _______________________________________________________Date: _________________________________________________________________