Critical Incident Report User Guide Form 470-4698 - Iowa Medicaid ...
Critical Incident Report User Guide Form 470-4698 - Iowa Medicaid ...
Critical Incident Report User Guide Form 470-4698 - Iowa Medicaid ...
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
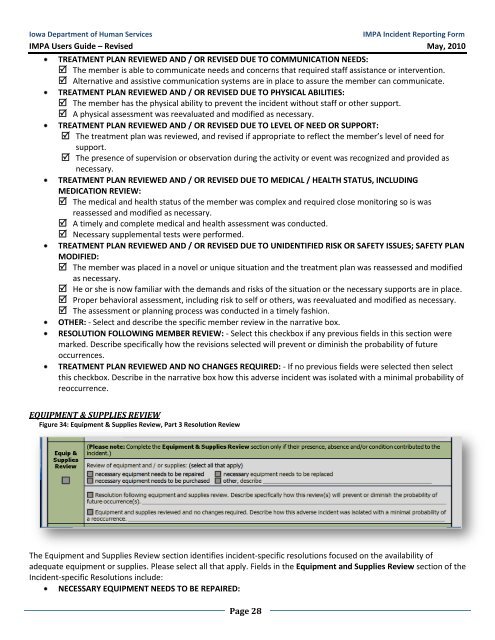
<strong>Iowa</strong> Department of Human ServicesIMPA <strong>Incident</strong> <strong>Report</strong>ing <strong>Form</strong>IMPA <strong>User</strong>s <strong>Guide</strong> – Revised May, 2010TREATMENT PLAN REVIEWED AND / OR REVISED DUE TO COMMUNICATION NEEDS: The member is able to communicate needs and concerns that required staff assistance or intervention. Alternative and assistive communication systems are in place to assure the member can communicate.TREATMENT PLAN REVIEWED AND / OR REVISED DUE TO PHYSICAL ABILITIES: The member has the physical ability to prevent the incident without staff or other support. A physical assessment was reevaluated and modified as necessary.TREATMENT PLAN REVIEWED AND / OR REVISED DUE TO LEVEL OF NEED OR SUPPORT: The treatment plan was reviewed, and revised if appropriate to reflect the member’s level of need forsupport. The presence of supervision or observation during the activity or event was recognized and provided asnecessary.TREATMENT PLAN REVIEWED AND / OR REVISED DUE TO MEDICAL / HEALTH STATUS, INCLUDINGMEDICATION REVIEW: The medical and health status of the member was complex and required close monitoring so is wasreassessed and modified as necessary. A timely and complete medical and health assessment was conducted. Necessary supplemental tests were performed.TREATMENT PLAN REVIEWED AND / OR REVISED DUE TO UNIDENTIFIED RISK OR SAFETY ISSUES; SAFETY PLANMODIFIED: The member was placed in a novel or unique situation and the treatment plan was reassessed and modifiedas necessary. He or she is now familiar with the demands and risks of the situation or the necessary supports are in place. Proper behavioral assessment, including risk to self or others, was reevaluated and modified as necessary. The assessment or planning process was conducted in a timely fashion.OTHER: - Select and describe the specific member review in the narrative box.RESOLUTION FOLLOWING MEMBER REVIEW: - Select this checkbox if any previous fields in this section weremarked. Describe specifically how the revisions selected will prevent or diminish the probability of futureoccurrences.TREATMENT PLAN REVIEWED AND NO CHANGES REQUIRED: - If no previous fields were selected then selectthis checkbox. Describe in the narrative box how this adverse incident was isolated with a minimal probability ofreoccurrence.EQUIPMENT & SUPPLIES REVIEWFigure 34: Equipment & Supplies Review, Part 3 Resolution ReviewThe Equipment and Supplies Review section identifies incident-specific resolutions focused on the availability ofadequate equipment or supplies. Please select all that apply. Fields in the Equipment and Supplies Review section of the<strong>Incident</strong>-specific Resolutions include:NECESSARY EQUIPMENT NEEDS TO BE REPAIRED:Page 28