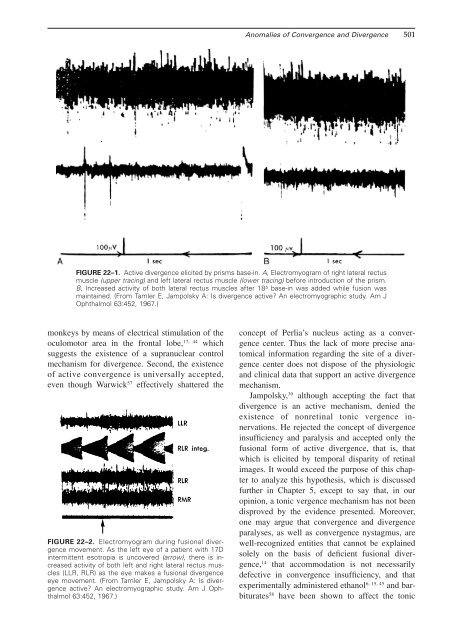
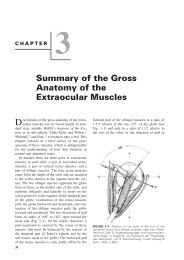
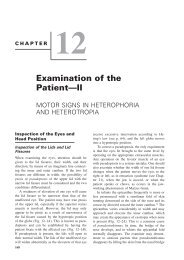
<strong>Anomalies</strong> <strong>of</strong> <strong>Convergence</strong> <strong>and</strong> <strong>Divergence</strong> 501FIGURE <strong>22</strong>–1. Active divergence elicited by prisms base-in. A, Electromyogram <strong>of</strong> right lateral rectusmuscle (upper tracing) <strong>and</strong> left lateral rectus muscle (lower tracing) before introduction <strong>of</strong> the prism.B, Increased activity <strong>of</strong> both lateral rectus muscles after 18 base-in was added while fusion wasmaintained. (From Tamler E, Jampolsky A: Is divergence active? An electromyographic study. Am JOphthalmol 63:452, 1967.)monkeys by means <strong>of</strong> electrical stimulation <strong>of</strong> the17, 44oculomotor area in the frontal lobe, whichsuggests the existence <strong>of</strong> a supranuclear controlmechanism for divergence. Second, the existence<strong>of</strong> active convergence is universally accepted,even though Warwick 57 effectively shattered theFIGURE <strong>22</strong>–2. Electromyogram during fusional divergencemovement. As the left eye <strong>of</strong> a patient with 17Dintermittent esotropia is uncovered (arrow), there is increasedactivity <strong>of</strong> both left <strong>and</strong> right lateral rectus muscles(LLR, RLR) as the eye makes a fusional divergenceeye movement. (From Tamler E, Jampolsky A: Is divergenceactive? An electromyographic study. Am J Ophthalmol63:452, 1967.)concept <strong>of</strong> Perlia’s nucleus acting as a convergencecenter. Thus the lack <strong>of</strong> more precise anatomicalinformation regarding the site <strong>of</strong> a divergencecenter does not dispose <strong>of</strong> the physiologic<strong>and</strong> clinical data that support an active divergencemechanism.Jampolsky, 30 although accepting the fact thatdivergence is an active mechanism, denied theexistence <strong>of</strong> nonretinal tonic vergence innervations.He rejected the concept <strong>of</strong> divergenceinsufficiency <strong>and</strong> paralysis <strong>and</strong> accepted only thefusional form <strong>of</strong> active divergence, that is, thatwhich is elicited by temporal disparity <strong>of</strong> retinalimages. It would exceed the purpose <strong>of</strong> this chapterto analyze this hypothesis, which is discussedfurther in <strong>Chapter</strong> 5, except to say that, in ouropinion, a tonic vergence mechanism has not beendisproved by the evidence presented. Moreover,one may argue that convergence <strong>and</strong> divergenceparalyses, as well as convergence nystagmus, arewell-recognized entities that cannot be explainedsolely on the basis <strong>of</strong> deficient fusional divergence,14 that accommodation is not necessarilydefective in convergence insufficiency, <strong>and</strong> thatexperimentally administered ethanol 6, 15, 45 <strong>and</strong> barbiturates58 have been shown to affect the tonic
502 Clinical Characteristics <strong>of</strong> Neuromuscular <strong>Anomalies</strong> <strong>of</strong> the Eyevergence mechanism. Furthermore, Scott 50 reportedelectromyographic findings in a patientwith V exotropia that could not have been causedby anything but tonic divergence.<strong>Anomalies</strong> <strong>of</strong> <strong>Convergence</strong><strong>Convergence</strong> InsufficiencyETIOLOGY AND CLINICAL FINDINGS. <strong>Convergence</strong>insufficiency is one <strong>of</strong> the most commoncauses <strong>of</strong> ocular discomfort <strong>and</strong>, in fact, is themost common cause <strong>of</strong> muscular asthenopia;therefore it is <strong>of</strong> considerable clinical significance.There is frequently an etiologic connectionwith associated accommodative difficulties. Forinstance, a convergence insufficiency as a result<strong>of</strong> disuse <strong>of</strong> the accommodative convergencemechanism may have been caused by uncorrectedhigh hypermetropia or myopia. Patients with hypermetropiaexceeding, say, 5D or 6D, make littleor no effort to accommodate, <strong>and</strong> in those withmyopia there is no need to accommodate to obtainclear vision at near fixation. Likewise, a patientwith beginning presbyopia may develop convergenceinsufficiency after wearing a bifocal prescriptionfor the first time. The relief <strong>of</strong> sustainedaccommodative effort afforded by the new prescriptioncauses a decrease <strong>of</strong> accommodativeconvergence; thus an exophoria that had been controlledby accommodative convergence may becomemanifest. In other patients without refractiveproblems the condition may arise without anyobvious cause.Some ophthalmologists consider patients withconvergence insufficiency to be neurotic <strong>and</strong> believethat their problem is something to be dealtwith by a psychiatrist. We emphatically reject thisgeneralization. 11 The <strong>of</strong>ten dramatic subjective improvementafter appropriate therapy, noted concurrentlywith the objective clinical finding <strong>of</strong> improvednear point <strong>of</strong> convergence <strong>and</strong> fusionalconvergence amplitudes, clearly puts this conditionon an innervational basis.In rare instances acquired convergence insufficiencymay occur on an organic basis, such assecondary to a subdural hematoma. 52An admirably concise description <strong>of</strong> the symptomsarising from convergence insufficiency wasgiven by von Graefe, who pointed out as early as1855 26, 27 that such patients complain about eyestrain<strong>and</strong> a sensation <strong>of</strong> tension in <strong>and</strong> about theglobes. After brief periods <strong>of</strong> reading, the letterswill blur <strong>and</strong> run together; crossed diplopia occasionallyoccurs during near work. Characteristically,one eye will be closed or covered whilereading to obtain relief from visual fatigue. Littlecan be added to this classic description except thatocular headaches are another frequent complaint.Von Graefe thought that convergence insufficiencywas myogenic, that is, caused by a congenitalweakness <strong>of</strong> the medial rectus muscles secondaryto overaction <strong>of</strong> the lateral rectus muscle. He recommendedprisms base-out to exercise the action<strong>of</strong> the medial rectus muscles in some patients,prisms base-in to eliminate symptoms in others,or a weakening procedure <strong>of</strong> the lateral rectusmuscles. Except for prisms base-out, which arestill used by some, his views on the etiology <strong>of</strong>convergence insufficiency <strong>and</strong> therapeutic suggestionshave not withstood the test <strong>of</strong> time.DIAGNOSIS. The diagnosis <strong>of</strong> convergence insufficiencyis based on the finding <strong>of</strong> a remote nearpoint <strong>of</strong> convergence <strong>and</strong> decreased fusional convergenceat near fixation. The reader is referred to<strong>Chapter</strong> 12 for a discussion <strong>of</strong> diagnostic methods<strong>and</strong> the clinically important differentiation betweenthe subjective <strong>and</strong> objective near point <strong>of</strong>convergence. Most patients with convergence insufficiencyexhibit varying degrees <strong>of</strong> exophoriaat near fixation; however, this disorder also occursin patients with orthophoria <strong>and</strong> occasionally evenin those with esophoria. The near point <strong>of</strong> accommodationis normal <strong>and</strong> corresponds to the age <strong>of</strong>the patient. However, to identify patients who sufferfrom a combined insufficiency <strong>of</strong> convergence<strong>and</strong> accommodation (see p. 503) <strong>and</strong> who requirea different form <strong>of</strong> therapy, the near point <strong>of</strong>accommodation should be determined in eachcase. 41<strong>Convergence</strong> insufficiency seldom becomes aclinical problem until a patient reaches the teenageyears. Increased schoolwork <strong>and</strong> prolonged periods<strong>of</strong> reading may then exacerbate the characteristicsymptoms. The type <strong>of</strong> patient most <strong>of</strong>tenencountered is a high-school, college, or universitystudent who is especially prone to developsymptoms before examinations when special dem<strong>and</strong>sare made on the near vision complex duringextended periods <strong>of</strong> studying. Needless to say,symptoms are aggravated by lack <strong>of</strong> sleep, reduction<strong>of</strong> general well-being, <strong>and</strong> anxiety.THERAPY. Therapy for convergence insufficiencyis in the realm <strong>of</strong> orthoptics. Indeed its treatment