Design Level Cross Connection Survey - City of Cambridge
Design Level Cross Connection Survey - City of Cambridge
Design Level Cross Connection Survey - City of Cambridge

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
G:\Common Graphics\DEPARTMENT PLANNING\2011 Form-<strong>Design</strong> <strong>Level</strong> <strong>Cross</strong> <strong>Connection</strong> <strong>Survey</strong>\<strong>Design</strong><strong>Level</strong><strong>Cross</strong><strong>Connection</strong><strong>Survey</strong>MG.indd<br />
Planning Services Dept<br />
Building & Enforcement<br />
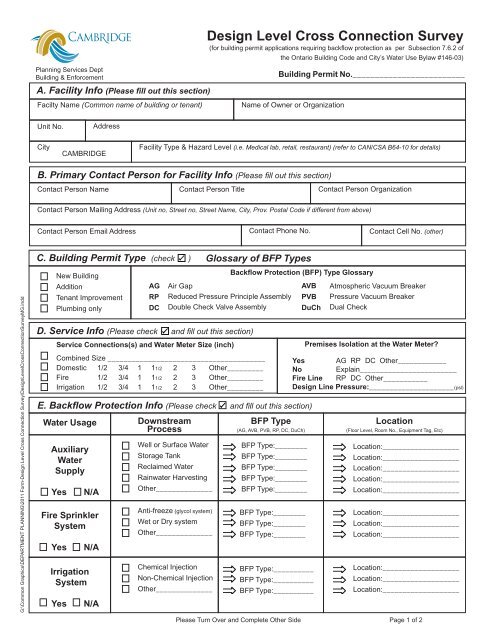
A. Facility Info (Please fi ll out this section)<br />
Facilty Name (Common name <strong>of</strong> building or tenant)<br />
Unit No.<br />
<strong>City</strong><br />
CAMBRIDGE<br />
Address<br />
<strong>Design</strong> <strong>Level</strong> <strong>Cross</strong> <strong>Connection</strong> <strong>Survey</strong><br />
(for building permit applications requiring backfl ow protection as per Subsection 7.6.2 <strong>of</strong><br />
the Ontario Building Code and <strong>City</strong>’s Water Use Bylaw #146-03)<br />
Building Permit No._________________________<br />
Name <strong>of</strong> Owner or Organization<br />
Facility Type & Hazard <strong>Level</strong> (i.e. Medical lab, retail, restaurant) (refer to CAN/CSA B64-10 for details)<br />
B. Primary Contact Person for Facility Info (Please fi ll out this section)<br />
Contact Person Name<br />
Contact Person Title<br />
Contact Person Mailing Address (Unit no, Street no, Street Name, <strong>City</strong>, Prov. Postal Code if different from above)<br />
Contact Person Email Address Contact Phone No.<br />
C. Building Permit Type (check<br />
New Building<br />
Addition<br />
Tenant Improvement<br />
Plumbing only<br />
AG<br />
RP<br />
DC<br />
)<br />
Glossary <strong>of</strong> BFP Types<br />
Air Gap<br />
Reduced Pressure Principle Assembly<br />
Double Check Valve Assembly<br />
D. Service Info (Please check and fi ll out this section)<br />
Service <strong>Connection</strong>s(s) and Water Meter Size (inch)<br />
Combined Size _______________________________________<br />
Domestic 1/2 3/4 1 11/2 2 3 Other _________<br />
Fire 1/2 3/4 1 11/2 2 3 Other _________<br />
Irrigation 1/2 3/4 1 11/2 2 3 Other _________<br />
Contact Person Organization<br />
Backfl ow Protection (BFP) Type Glossary<br />
E. Backfl ow Protection Info (Please check and fi ll out this section)<br />
Water Usage<br />
Auxiliary<br />
Water<br />
Supply<br />
Yes N/A<br />
Fire Sprinkler<br />
System<br />
Yes N/A<br />
Irrigation<br />
System<br />
Yes N/A<br />
Downstream<br />
Process<br />
Well or Surface Water<br />
Storage Tank<br />
Reclaimed Water<br />
Rainwater Harvesting<br />
Other______________<br />
Anti-freeze (glycol system)<br />
Wet or Dry system<br />
Other______________<br />
Chemical Injection<br />
Non-Chemical Injection<br />
Other______________<br />
BFP Type<br />
(AG, AVB, PVB, RP, DC, DuCh)<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
AVB<br />
PVB<br />
DuCh<br />
BFP Type:__________<br />
BFP Type:__________<br />
BFP Type:__________<br />
Contact Cell No. (other)<br />
Atmospheric Vacuum Breaker<br />
Pressure Vacuum Breaker<br />
Dual Check<br />
Premises Isolation at the Water Meter?<br />
Yes AG RP DC Other____________<br />
No Explain________________________<br />
Fire Line RP DC Other___________<br />
<strong>Design</strong> Line Pressure:_____________________(psl)<br />
Location<br />
(Floor <strong>Level</strong>, Room No., Equipment Tag, Etc)<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Please Turn Over and Complete Other Side Page 1 <strong>of</strong> 2
G:\Common Graphics\DEPARTMENT PLANNING\2011 Form-<strong>Design</strong> <strong>Level</strong> <strong>Cross</strong> <strong>Connection</strong> <strong>Survey</strong>\<strong>Design</strong><strong>Level</strong><strong>Cross</strong><strong>Connection</strong><strong>Survey</strong>MG.indd<br />
Planning Services Dept<br />
Building & Enforcement<br />
Facility Name________________________________________________________<br />
E. Backfl ow Protection Info (Please check and fi ll out this section)<br />
Water Usage<br />
Heating/<br />
Cooling<br />
Equipment<br />
Yes N/A<br />
Commercial<br />
Kitchen/Bar<br />
Equipment<br />
Yes N/A<br />
Commercial<br />
Laundry/Janitor<br />
and/or<br />
Service Rooms<br />
Yes N/A<br />
Medical/Dental<br />
and/or<br />
Labs<br />
Yes N/A<br />
Misc.<br />
(other equipment)<br />
Yes N/A<br />
Downstream<br />
Process<br />
Water Heater T&P Valve<br />
Boiler (water or steam)<br />
Heat Exchanger<br />
Water Cooled Equip.<br />
Other______________<br />
Dish/Glass washer<br />
Canopy/Hood washer<br />
Beverage Carbonator<br />
Icemaker<br />
Other______________<br />
Washing Machine<br />
Sink (inc. janitor sink)<br />
Dry Cleaning Equip.<br />
Detergent Dispenser<br />
Other______________<br />
Medical Equip.<br />
Sink (inc. lab sink)<br />
Fume Hood (Lab)<br />
Dental Equipment<br />
Other______________<br />
Hose <strong>Connection</strong> (all)<br />
Reverse Osmosis<br />
Car Wash Equip<br />
Other______________<br />
<strong>Design</strong> <strong>Level</strong> <strong>Cross</strong> <strong>Connection</strong> <strong>Survey</strong><br />
(for building permit applications requiring backfl ow protection as per Subsection 7.6.2 <strong>of</strong><br />
BFP Type<br />
(AG, AVB, PVB, RP, DC, DuCh)<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
BFP Type:________<br />
the Ontario Building Code and <strong>City</strong>’s Water Use Bylaw #146-03)<br />
Location<br />
(Floor <strong>Level</strong>, Room No., Equipment Tag, Etc)<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
Location:___________________<br />
F. <strong>Design</strong>er/<strong>Cross</strong> <strong>Connection</strong> Control <strong>Survey</strong> Specialist (Please check and fi ll out this section)<br />
All internal cross connections protected? Yes No<br />
<strong>Design</strong>ed to CAN/CSA B64-10? Yes No If Yes: Version___________________<br />
I, _____________________________certify that the information contained in this form and other attached documentation is true to<br />
the best <strong>of</strong> my knowledge. I also acknowldge that these listed devices will ensure compliance with the Ontario Building Code.<br />
________________________ _________________________________________________<br />
Date Signature <strong>of</strong> Pr<strong>of</strong>essional Engineer OR Licensed Backfl ow<br />
ATTACH TO: Building Permit Application<br />
Prevention Installer defi ned in <strong>City</strong>’s Water Use By-law #146-03<br />
MAIL OR FAX TO: The Corporation <strong>of</strong> the <strong>City</strong> <strong>of</strong> <strong>Cambridge</strong><br />
50 Dickson Street, P.O. Box 669<br />
<strong>Cambridge</strong>, ON N1R 5W8<br />
Attention Building Division Fax:519.622.6184<br />
Personal information contained on this form is collected pursuant to the Building Code and will be used for the purpose <strong>of</strong> responding to your<br />
application. Questions about the collection <strong>of</strong> personal information should be directed to the Corporate Records Coordinator/Deputy <strong>City</strong> Clerk at 519.740.4680<br />
Please Turn Over and Complete Other Side Page 2 <strong>of</strong> 2