(PC) to Specialty Behavioral Health (BH) Referral Form - Alameda ...
(PC) to Specialty Behavioral Health (BH) Referral Form - Alameda ...
(PC) to Specialty Behavioral Health (BH) Referral Form - Alameda ...
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
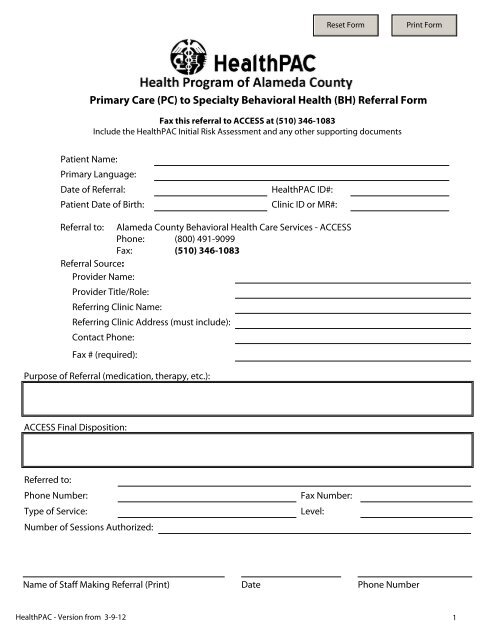
Primary Care (<strong>PC</strong>) <strong>to</strong> <strong>Specialty</strong> <strong>Behavioral</strong> <strong>Health</strong> (<strong>BH</strong>) <strong>Referral</strong> <strong>Form</strong>Fax this referral <strong>to</strong> ACCESS at (510) 346-1083Include the <strong>Health</strong>PAC Initial Risk Assessment and any other supporting documentsPatient Name:Primary Language:Date of <strong>Referral</strong>:Patient Date of Birth:<strong>Health</strong>PAC ID#:Clinic ID or MR#:<strong>Referral</strong> <strong>to</strong>: <strong>Alameda</strong> County <strong>Behavioral</strong> <strong>Health</strong> Care Services - ACCESSPhone: (800) 491-9099Fax: (510) 346-1083<strong>Referral</strong> Source:Provider Name:Provider Title/Role:Referring Clinic Name:Referring Clinic Address (must include):Contact Phone:Fax # (required):Purpose of <strong>Referral</strong> (medication, therapy, etc.):ACCESS Final Disposition:Referred <strong>to</strong>:Phone Number:Type of Service:Number of Sessions Authorized:Fax Number:Level:Name of Staff Making <strong>Referral</strong> (Print)DatePhone Number<strong>Health</strong>PAC - Version from 3-9-121
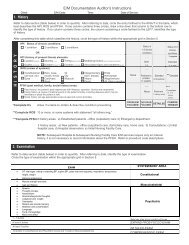
PatientName:<strong>Health</strong>PAC Initial Risk Assessment (<strong>to</strong> be completed face <strong>to</strong> face)1. Date of assessment:2. Demographics/Patient Contact Information:Social Security #: Male Female TransgenderAddress: City: Zip:Tel:Ethnicity/Race:Birthplace:Marital Status:Birth Last Name:Highest Educational Grade completed:Hispanic Origin:Mother's First Name:Preferred Language:Physical Disability:3. Presenting <strong>Behavioral</strong> Problems (check all that apply and/or describe below):Adjustment <strong>to</strong> trauma/major stressors, separation, loss, death, job, school Mania, elevated moodAnger ControlAnxiety, fear, panic, agitationDepression, hopelessnessEating DisturbanceEmployment/School functioning problemsFamily relationship problemsPain without clear medical explanationPsychosis, unreal thoughts or beliefs, audi<strong>to</strong>ry and/or visual hallucinationsResidential instability/Risk of homelessnessSleep DisturbanceSubstance abuse/dependenceVictim of abuse, physical, sexual and/or severe neglectHyperactivityImpulse control problemsOther, describe belowDESCRIBE ONSET, DURATION, AND SEVERITY OF SYMPTOMS/IMPAIRMENTS, INCLUDING RELEVANT HISTORY AND SIGNIFICANT LIFE EVENTS:4. Risk Assessment (check appropriate rating)Danger<strong>to</strong> selfNoneHis<strong>to</strong>ry but norecent intent,ideation orfeasible planRecentideation, nocurrentfeasible planRecent ideation, intention,plan that is feasible and/orhis<strong>to</strong>ry of a potentially lethalattemptCurrent ideation or command hallucinations reself-harm, current intent, plan that isimmediately accessible and feasible, and/orhis<strong>to</strong>ry of multiple potentially lethal attempts.Call 911 IMMEDIATELY.Danger<strong>to</strong>othersNoneHis<strong>to</strong>ry but norecent gestureor ideationRecentideation, nocurrentfeasible planRecent homicidal ideation,physically harmful aggressionor dangerous fire setting, butnot in past 24 hours. Hasfeasible plan <strong>to</strong> harm othersAcute homicidal ideation with an accessible,feasible plan of physically harmful aggression,or command hallucinations involving harm ofothers. Or intentionally set fire that placedothers at significant risk of harm. Call 911IMMEDIATELY.<strong>Health</strong>PAC - Version from 3-9-122
Name:<strong>Health</strong>PAC Initial Risk Assessment (<strong>to</strong> be completed face <strong>to</strong> face)4A. Other Risk Fac<strong>to</strong>rs (if yes, please describe below:)No Yes4B. Previous Psychiatric HospitalizationNo Yes Date/reason of last hosp:4C. Risk Assessment (ELABORATION OF ALL RISK FACTORS)5. Current Mental StatusMoodAffectThought process/contentHallucinationsOrientationCognitiveDepressedAppropriateNormalAudi<strong>to</strong>ryTimeMemory problemAnxiousInappropriateLoose/TangentialVisualPersonLack of insightEuphoricGrandioseOtherPlacePoor judmentOtherParanoidConcrete thinkingMentalStatusComments:6. Substance Use Concerns (Describe screening done, current, and past use, and impact of use):<strong>Health</strong>PAC - Version from 3-9-123
Name:<strong>Health</strong>PAC Initial Risk Assessment (<strong>to</strong> be completed face <strong>to</strong> face)7. LegalIssuesCourt Mandated Treatment Probation/Parole: His<strong>to</strong>ry of arrest:No Yes No Yes No Yes8. Mental<strong>Health</strong>Currently receiving servicesNo YesIf yes, where:ConservedNo YesHis<strong>to</strong>ry of treatmentNo YesCurrent psych medsNo YesIf yes, add <strong>to</strong> medication list9. Primary Careworking mental healthdiagnos(es):10. AdditionalComments (describefunctional impairments,primary care treatmentattempts, and response,other fac<strong>to</strong>rs):Please answer #11 and #12 below OR provide other documents listing current medications and health conditions:11. Current Medications (include allbehavioral and physical meds)Med Allergies:Medication Name Strength Frequency Purpose Prescriber12. Patient's otherhealth conditions:Staff Name (print):Clinician/Staff/Other Appropriate SignatureDate:<strong>Health</strong>PAC - Version from 3-9-124