Course transcript - Northwest Center for Public Health Practice
Course transcript - Northwest Center for Public Health Practice
Course transcript - Northwest Center for Public Health Practice
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
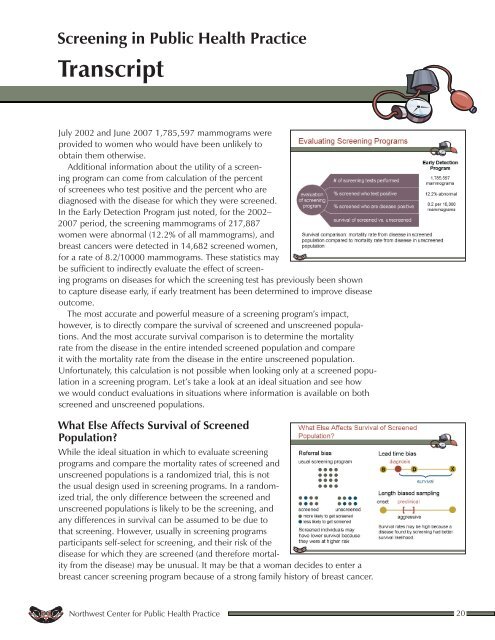
Screening in <strong>Public</strong> <strong>Health</strong> <strong>Practice</strong>TranscriptJuly 2002 and June 2007 1,785,597 mammograms wereprovided to women who would have been unlikely toobtain them otherwise.Additional in<strong>for</strong>mation about the utility of a screeningprogram can come from calculation of the percentof screenees who test positive and the percent who arediagnosed with the disease <strong>for</strong> which they were screened.In the Early Detection Program just noted, <strong>for</strong> the 2002–2007 period, the screening mammograms of 217,887women were abnormal (12.2% of all mammograms), andbreast cancers were detected in 14,682 screened women,<strong>for</strong> a rate of 8.2/10000 mammograms. These statistics maybe sufficient to indirectly evaluate the effect of screeningprograms on diseases <strong>for</strong> which the screening test has previously been shownto capture disease early, if early treatment has been determined to improve diseaseoutcome.The most accurate and powerful measure of a screening program’s impact,however, is to directly compare the survival of screened and unscreened populations.And the most accurate survival comparison is to determine the mortalityrate from the disease in the entire intended screened population and compareit with the mortality rate from the disease in the entire unscreened population.Un<strong>for</strong>tunately, this calculation is not possible when looking only at a screened populationin a screening program. Let’s take a look at an ideal situation and see howwe would conduct evaluations in situations where in<strong>for</strong>mation is available on bothscreened and unscreened populations.What Else Affects Survival of ScreenedPopulation?While the ideal situation in which to evaluate screeningprograms and compare the mortality rates of screened andunscreened populations is a randomized trial, this is notthe usual design used in screening programs. In a randomizedtrial, the only difference between the screened andunscreened populations is likely to be the screening, andany differences in survival can be assumed to be due tothat screening. However, usually in screening programsparticipants self-select <strong>for</strong> screening, and their risk of thedisease <strong>for</strong> which they are screened (and there<strong>for</strong>e mortalityfrom the disease) may be unusual. It may be that a woman decides to enter abreast cancer screening program because of a strong family history of breast cancer.<strong>Northwest</strong> <strong>Center</strong> <strong>for</strong> <strong>Public</strong> <strong>Health</strong> <strong>Practice</strong> 20