Transcatheter Aortic Valve Implantation (TAVI) - Papworth Hospital
Transcatheter Aortic Valve Implantation (TAVI) - Papworth Hospital
Transcatheter Aortic Valve Implantation (TAVI) - Papworth Hospital
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
A patient’s guideValvular heart diseaseThe heart is a muscle whichpumps blood to your lungs andaround the body. There arefour valves within the heart.These valves normally opento let blood flow through, orout, of the heart, and thenshut to prevent blood flowingbackwards.If a valve becomes diseased ordamaged this can affect theflow of blood in two ways:1. If the valve does not openfully it will obstruct the flow.This is called valve stenosis.2. If the valve does not closeproperly it will allow blood toflow backwards in the wrongdirection. This is called valveregurgitation.<strong>Aortic</strong> valve stenosisYou have been diagnosedwith aortic valve stenosis.The aortic valve is on theleft side of the heart. Whenthe valve opens blood isnormally pumped from theleft pumping chamber of theheart (ventricle) around thebody. When the aortic valveis narrowed the blood flowout of the heart is restricted.This can cause symptoms ofchest pain, breathlessness and/or dizziness when exercising,and can lead to fainting. Therestriction may also put a strainonto your heart pump, leadingto heart muscle weakness, fluidon the lungs or swollen ankles.The preferred treatment forsevere symptomatic aorticvalve stenosis is conventionalaortic valve replacement. Thisinvolves open-heart surgeryto replace the narrowedvalve with a new artificialone. However, due to youroverall medical condition,you are considered a high-riskcandidate for conventionalsurgery, but may be suitablefor a transcatheter aortic valvereplacement.What is <strong>Transcatheter</strong> <strong>Aortic</strong><strong>Valve</strong> <strong>Implantation</strong>?<strong>Transcatheter</strong> aortic valveimplantation (<strong>TAVI</strong>) involvesinserting a new artificial heartvalve inside the old tight valveusing a balloon catheter. Thevalve is made up of a metalframe (stent) and the outerlining (pericardium) of a cow’sheart. The procedure is carriedout under general anaesthetic.1
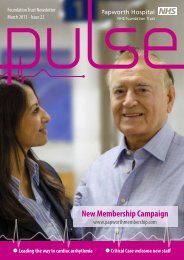
A patient’s guideEdwards Sapien <strong>Valve</strong> (one pence coin to assist with scale)There are two common routesof new valve insertion:1. Transfemoral - through thefemoral artery, the main arteryin your groin which leads backto the heart.The ‘<strong>TAVI</strong> team’, including yourcardiologist, cardiac surgeonand anaesthetist will reviewyour medical condition andscreening tests to decide themost appropriate treatmentand access route for you.22. Transapical - through a smallcut on the left side of yourchest to get to the apex (tip) ofyour heart.
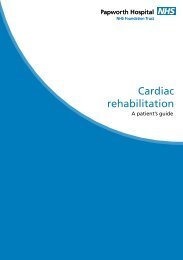
A patient’s guideRetrograde TransfemoralApproachThe delivery system isintroduced through thefemoral artery allowingpositioning of the prostheticvalve within the nativestenotic aortic valve.Antegrade TransvenousApproachThe delivery system isadvanced through thefemoral vein to the rightatrium across the interatrialseptum and mitral valve tobe subsequently positionedin the stenotic aortic valve.This approach is rarely used.Transapical ApproachThe left ventricular apex isreached by anterolateralminithoracotomy. The valvedelivery system is introducedthrough the left ventricularapex and subsequentlypositioned in the stenoticaortic valve.<strong>Transcatheter</strong> <strong>Aortic</strong> <strong>Valve</strong> <strong>Implantation</strong> Techniques3
A patient’s guide4Screening testsYou may have at varying times:• A physical examination• An electrical heart trace (ECG)• A chest X-ray (CXR)• Blood tests• An ultrasound probe andgel placed on the chestto obtain pictures ofyour heart (transthoracicechocardiogram)• Possibly a transoesophagealechocardiogram (TOE) ifclearer pictures are needed(this involves swallowingan ultrasound probe undersedation)• An angiogram, whichinvolves passing a tube(catheter) into your groinor wrist artery and takingX-ray pictures of your bloodvessels supplying your heart(coronary arteries), yourbody’s main blood vessel(aorta) and groin arteries.• Other possible tests includeCT or MRI body scans<strong>Hospital</strong> admissionOnce accepted by the medicalteam, and the funding for youroperation is available, you willbe invited in for the operation.You will receive a letter withyour admission details. Thiswill usually ask you to stop anyblood thinning medications fivedays before your operation.You will be asked to come inthe day before your procedurefor preparation. Before theoperation, you will be seenby members of the operatingteam. You will be kept ‘nil bymouth’ for a few hours priorto your procedure and thenurses will assist you to shaveyour chest, wrists and groinsand also to shower.The procedure will be donein the X-ray laboratory(similar room to where youhad the coronary angiogram)using contrast dye andechocardiography to guide thevalve into the correct position.ProcedureYou will be anaesthetisedand then have a drip insertedinto your neck and arm and aurinary catheter inserted intoyour bladder. You will havesome tubes put through theblood vessels in your groin todeliver the contrast dye and apacing wire to speed up the
A patient’s guideheart during the valve insertionto ensure correct positioning.The surgeon will gain accessmaking a small incision eitherin your groin or chest wall.A catheter (narrow tube)is passed from the femoral(groin) artery to the aorta(transfemoral) or through theheart muscle near to the aorticvalve (transapical). The catheterallows a balloon to be placedinto your tight valve, theballoon is inflated to stretchthe valve open. This part ofthe procedure is called balloonaortic valvuloplasty (BAV).The new valve for implantationwill be carefully compressedand mounted onto a balloondelivery catheter. When thevalve is in the correct positionyour heart rate will beincreased using the temporarypacing wire for a few seconds.This reduces the blood pressureand the motion of the heartmaking the procedure safer.The balloon is then expandedopening up the replacementvalve in to a permanentposition. The balloon isdeflated and removed leavingthe new valve to functionimmediately.The operation site is repairedby the cardiac surgeon. Apleural (chest) drain is insertedif access has been via thetransapical route, to drain anyexcess fluid or air from thechest cavity. The proceduretakes one to two hours.Following your procedureYou will go from the X-raydepartment to the recoveryarea for several hours whereyou will be closely monitored.Following this you will returneither to the ward or the highdependency unit. Normallyyou are woken up early afterthe operation but occasionallyyou may need to stay asleepso will be kept sedated and ifnecessary admitted to intensivecare.Over the next 48 hours youwill have your drips and drainsremoved. It is not uncommonto access both groin bloodvessels. Whilst there are tubesin your groin you will have tobe on bed rest. When thesetubes are removed you can sitout and start to walk about.5
A patient’s guideYou will be in hospital for fiveto ten days depending on howquickly you recover.Potential benefits of a <strong>TAVI</strong>procedureTreatment with the newvalve should improve yoursymptoms. It will give youa more normal aortic valveperformance and improve youroverall heart function. Wewould hope this will increaseyour life expectancy andimprove your quality of life.Potential risks of theprocedure• Risk of heart attack: 1%• Risk of stroke: 2-3%• Risk of death during theprocedure approximately: 2%• Risk of requiring apermanent pacemaker: 3%• Damage to groin arteries• Bleeding• Infection• Kidney failure (if impairedkidney function existed priorto surgery)• Emergency open heartsurgery 0.5%A <strong>TAVI</strong> would berecommended only if yourdoctors feel the risk is lowerthan conventional aortic valvereplacement surgery.Recovery at homeThe following are only generalguidelines as everyone’srecovery is slightly different.It is advisable that you havesomeone to care for you forthe first week after discharge.Please speak to your nurse ordoctor as soon as possible if youthink this will be a problem.ActivityYou should avoid strenuousactivity for a few weeks, sixweeks if your procedure wasvia the transapical approach.This includes heavy lifting (egshopping, suitcases) or pushingand pulling (eg cutting grass,vacuum cleaning).You may feel a little ‘washedout’ and tired and need to restin the afternoon. However itis important for your recoveryto have a short walk everyday. This can be graduallyincreased.6
A patient’s guideYou do not have to avoidclimbing stairs or walking upinclines, you may have to startoff at a slower pace. You mayfeel slightly out of breath onwalking, which should improveas your fitness level increases.There can be some fluidretention as a result of thesurgery; you may notice someswelling of your ankles. Ifthis swelling travels furtherthan your ankles please getreviewed by your GP.WoundsYour wounds should be healedby the time you leave hospital,if they still require a dressingwe will organise a District orpractice nurse to continue this.The stitches are dissolvable sodo not have to be removed. Ifyour wound becomes red orinflamed please get your GP orpractice nurse to check it.You may have bruising toyour groin(s) which is notuncommon and may takeseveral weeks to resolve. Youmay have a hard lump underthe skin due to a collection ofblood (haematoma). Pleaseconsult your GP if this becomespainful or grows bigger.MedicationAs well as your normalmedicines including aspirin,you will usually be dischargedwith an additional bloodthinning medicine calledClopidogrel. This will berequired for at least threemonths. After this you willonly need to take the aspirin.People on warfarin may haveonly aspirin or clopidogrel.You will be discharged withsome painkillers which wewould recommend you totake regularly until you are nolonger getting discomfort fromyour wound.DrivingYou are not allowed by DVLAto drive for four weeks afteryour procedure. If you havea LGV or PCV licence you willneed to undergo an exercisetest before getting your licenceback.WorkIf you were working beforeyour procedure there is noreason why you cannot returnto this after a period ofrecovery up to six weeks.7
A patient’s guideCardiac rehabilitationYou will be invited to attendcardiac rehabilitation about sixweeks after your procedure.This is a programme ofgraduated exercise and generalhealth discussions. If you liveoutside the <strong>Papworth</strong> area youmay be referred to your localhospital. Patients who attendgenerally feel more confidentabout coping with everydaylife. It will also help to increaseyour fitness level.Follow-up careOn discharge you will begiven a letter for your G.Pexplaining what you havehad done and a list of yourmedications. The valve nursespecialist will phone you aweek after discharge to checkon your progress. If you haveany concerns you can call onthe cardiac support nurse line01480 364100 (Monday toFriday 08.30 - 18.00). We wouldlike to hear sooner ratherthan later about any potentialproblems.During this visit you willhave an ECG and if yourprocedure was transapicalalso a Chest X-ray. At a furtherappointment after threemonths you will have anultrasound scan of your heartand see the cardiologist. Thedoctor will then decide aboutany future appointments.How to contact usIf you need further informationplease contact Helen Powellor Elaine Gaines, <strong>Valve</strong> NurseSpecialists, on 01480 3641008You will be invited to attendan outpatient follow upappointment with the nursespecialist approximately sixweeks after your procedure.
A patient’s guide<strong>Papworth</strong> <strong>Hospital</strong> NHS Foundation Trust<strong>Papworth</strong> EverardCambridgeCB23 3RETel: 01480 830541Fax: 01480 831315For more information about <strong>Papworth</strong> <strong>Hospital</strong> pleasevisit our website www.papworthhospital.nhs.ukA member of Cambridge University Health Partners<strong>Papworth</strong> <strong>Hospital</strong> is a smoke free siteLarge print copies andalternative languages canbe made availableon request.Author ID: Helen Powell and <strong>TAVI</strong> TeamDepartment: Cardiac OutpatientsPrinted: July 2011Review date: July 2013Leaflet number: PI 43© <strong>Papworth</strong> <strong>Hospital</strong> NHS Foundation Trust