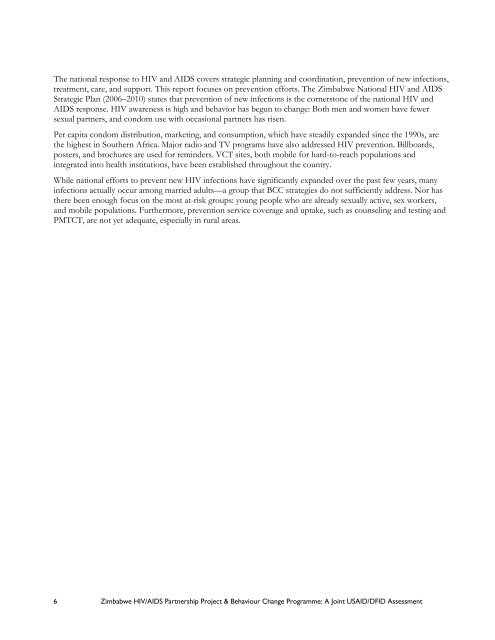
700,000 <strong>Zimbabwe</strong>ans were left homeless in 2005 after their informal urban habitats were demolished in operationmurambatsvina (Operation Restore Order). Although the government claimed the intent was to restore law andorder, it is widely considered to have been a political move against potential strikers and opposition supporters.Promises of re-housing have not been fulfilled. Violence linked to the 2008 elections resulted in furtherdisplacements.Information and Media<strong>Zimbabwe</strong> Broadcasting Holdings—comprising the four radio stations and one television station in <strong>Zimbabwe</strong>—isstate-owned. Fortunately, PSI/Z still has access to radio and TV. The privately owned newspapers are expensiveweeklies (The Independent, The Standard, and The Financial Gazette). No foreign journalists are accredited. New mediatechnologies like blogging and text messaging are publishing trustworthy stories for local and global audiences, butthey are threatened by the new Interception of Communications Act which enables the authorities, with a warrant,to eavesdrop on electronic and telephone communication.<strong>HIV</strong> AND <strong>AIDS</strong>: SITUATION AND RESPONSEThe first reported case of <strong>AIDS</strong> in <strong>Zimbabwe</strong> occurred in 1985. By the end of the 1980s, about 10 percent of theadult population was thought to be infected with <strong>HIV</strong>, mainly through heterosexual contact. This number shot upto peak at 29 percent between 1995 and 1997 and then fell over the next 10 years to 15.6 percent (Ministry ofHealth and Child Welfare (MOHCW) National Estimates, 2005). Today an estimated 1,610,000 <strong>Zimbabwe</strong>ans areliving with <strong>HIV</strong> and <strong>AIDS</strong>, of which 115,000 are under 15 (MOHCW, 2005). Of those known to be infected, 55percent are women. Young women (15–29 years) are the most vulnerable to infection. Among <strong>Zimbabwe</strong>ans 15–24, it is estimated that three times as many women as men have <strong>HIV</strong> (ZNASP, 2006-2010). Although <strong>Zimbabwe</strong> isthe first Southern African country to record a significant drop in <strong>HIV</strong> and <strong>AIDS</strong> among adults 15– 49, the rate isstill unaccepted (Figure 1).Figure 1: <strong>HIV</strong> Incidence/Prevalence in <strong>Zimbabwe</strong>Reasons forprevalencedeclineReasons forincidencedeclineMortalityIncreased mortalityamong persons withhigh infection risk<strong>HIV</strong> prevalence decline<strong>HIV</strong> incidence decline<strong>Behaviour</strong>change?1998: 29.3 %;2007: 15.6 % (adults 15-49)XEmigration ofpersons withriskier behavioursEmigration ofPLWHA<strong>Behaviour</strong>sAbstinence- No clear trend- Age of debuthigh since 1980sPartner Reduction- Decrease in meannumber of partners;Condom use- High levels ofcondom use withnon-regular partnersOther programs:(More likely that thesecontributed to a lowerpeak prevalence than todecline): STI treatment,blood safetyProgrammesOtherfactorsFocus on delayeddebut: FBOs, NGOs,education systemReduced ability toafford multiplepartnersSome focus on partnerreduction and preventionin marriage within ABCPersonal experience ofmorbidity and mortalityStrong public sector& social marketingcondom programsRelatively high levelsof education/ socialcapital<strong>HIV</strong> awareness:media, IPC,schools, clinics,churchesSource: Daniel Halperin, Backson Muchini, Exnavia Gomo, Reko Mate, Tapuwa Magure, Owen Mugurungi, Bruce Campbell, and ClemensBenedict, International <strong>AIDS</strong> Conference Mexico City, August 4, 2008.<strong>Zimbabwe</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Partnership</strong> <strong>Project</strong> & <strong>Behaviour</strong> <strong>Change</strong> Programme: A Joint USAID/DFID Assessment 5
The national response to <strong>HIV</strong> and <strong>AIDS</strong> covers strategic planning and coordination, prevention of new infections,treatment, care, and support. This report focuses on prevention efforts. The <strong>Zimbabwe</strong> National <strong>HIV</strong> and <strong>AIDS</strong>Strategic Plan (2006–2010) states that prevention of new infections is the cornerstone of the national <strong>HIV</strong> and<strong>AIDS</strong> response. <strong>HIV</strong> awareness is high and behavior has begun to change: Both men and women have fewersexual partners, and condom use with occasional partners has risen.Per capita condom distribution, marketing, and consumption, which have steadily expanded since the 1990s, arethe highest in Southern Africa. Major radio and TV programs have also addressed <strong>HIV</strong> prevention. Billboards,posters, and brochures are used for reminders. VCT sites, both mobile for hard-to-reach populations andintegrated into health institutions, have been established throughout the country.While national efforts to prevent new <strong>HIV</strong> infections have significantly expanded over the past few years, manyinfections actually occur among married adults—a group that BCC strategies do not sufficiently address. Nor hasthere been enough focus on the most at-risk groups: young people who are already sexually active, sex workers,and mobile populations. Furthermore, prevention service coverage and uptake, such as counseling and testing andPMTCT, are not yet adequate, especially in rural areas.6 <strong>Zimbabwe</strong> <strong>HIV</strong>/<strong>AIDS</strong> <strong>Partnership</strong> <strong>Project</strong> & <strong>Behaviour</strong> <strong>Change</strong> Programme: A Joint USAID/DFID Assessment