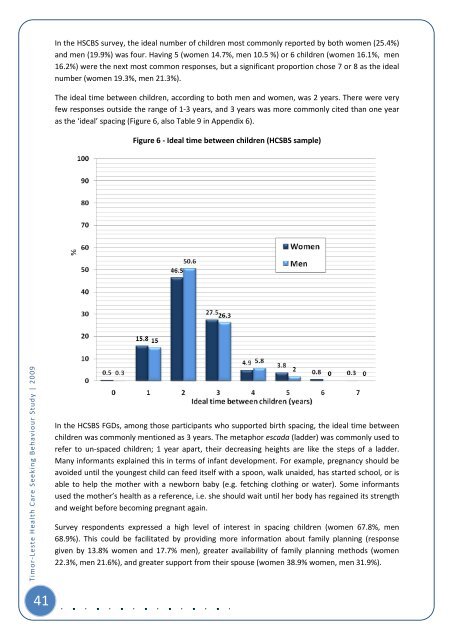
In the HSCBS survey, the i<strong>de</strong>al number of children most commonly reported by both women (25.4%)and men (19.9%) was four. Having 5 (women 14.7%, men 10.5 %) or 6 children (women 16.1%, men16.2%) were the next most common responses, but a significant proportion chose 7 or 8 as the i<strong>de</strong>alnumber (women 19.3%, men 21.3%).The i<strong>de</strong>al time between children, according to both men and women, was 2 years. There were veryfew responses outsi<strong>de</strong> the range of 1-3 years, and 3 years was more commonly cited than one yearas the ‘i<strong>de</strong>al’ spacing (Figure 6, also Table 9 in Appendix 6).Figure 6 - I<strong>de</strong>al time between children (HCSBS sample)<strong>Timor</strong>-<strong>Leste</strong> <strong>Health</strong> <strong>Care</strong> <strong>Seeking</strong> <strong>Behaviour</strong> <strong>Study</strong> | 2009In the HCSBS FGDs, among those participants who supported birth spacing, the i<strong>de</strong>al time betweenchildren was commonly mentioned as 3 years. The metaphor escada (lad<strong>de</strong>r) was commonly used torefer to un-spaced children; 1 year apart, their <strong>de</strong>creasing heights are like the steps of a lad<strong>de</strong>r.Many informants explained this in terms of infant <strong>de</strong>velopment. For example, pregnancy should beavoi<strong>de</strong>d until the youngest child can feed itself with a spoon, walk unai<strong>de</strong>d, has started school, or isable to help the mother with a newborn baby (e.g. fetching clothing or water). Some informantsused the mother’s health as a reference, i.e. she should wait until her body has regained its strengthand weight before becoming pregnant again.Survey respon<strong>de</strong>nts expressed a high level of interest in spacing children (women 67.8%, men68.9%). This could be facilitated by providing more information about family planning (responsegiven by 13.8% women and 17.7% men), greater availability of family planning methods (women22.3%, men 21.6%), and greater support from their spouse (women 38.9% women, men 31.9%).41
In the previous 12 months, 43.3% of women and 40.2% of men had talked about birth spacing orfamily planning, mostly with their spouse (women 47.2%, men 46.2%) or a health provi<strong>de</strong>r (women32.7%, men 33.6%). Most respon<strong>de</strong>nts (>70%) stated that they would prefer to get information andobtain family planning methods from a health provi<strong>de</strong>r, preferably a midwife or a nurse (women77.1%, men 88.8%).As shown in Table 4, contraception was being used by just over a third of survey respon<strong>de</strong>nts(women 38.0%, men 36.7%). Injection was by far the popular method among women, followed bywithdrawal and the oral contraceptive pill. No women, and only six men, reported using condoms.The <strong>de</strong>cision to use family planning was reported as usually being ma<strong>de</strong> jointly by a couple (women81.6%, men 80.7%).Table 4 - Currently used methods of birth spacing reported by men and women (HCSBS sample)MethodWomenn (%)Men*n (%)Injectables 78 (59.1) 44 (41.1)Withdrawal 17 (12.9) 32 (29.9)Pill 16 (12.1) 9 (8.4)Rhythm or periodic abstinence 7 (5.3) 4 (3.7)Female/ Male sterilisation 5 (3.8) 3 (2.8)IUD 2 (1.5) 1 (0.9)Condom 0 (0.0) 6 (5.6)Other 6 (4.6) 7 (6.5)Total 132 (100.0) 107 (100.0)The HCSBS qualitative component shed light on some of the reasons behind contraceptive choices.Injectable (sona or suntik) methods were said to cause weight gain, disinterest in sex, thinning of theuterus (oan fatin neé ema <strong>de</strong>han mihis ona), even <strong>de</strong>ath. The pill was regar<strong>de</strong>d as risky as it had to betaken on a daily basis and could easily be forgotten, and women perceived that men did not likeusing condoms. The calendar method, usually promoted by church clinics, was consi<strong>de</strong>red unreliableas it <strong>de</strong>pen<strong>de</strong>d on mutual abstinence. Some informants preferred natural or traditional methodsbased on root, bark or leaves. In relation to permanently preventing conception, traditional medicinewas mentioned but not neither vasectomy nor tubal ligation. 17 Breastfeeding as contraception wasmentioned as a natural practice of the past.Several informants mentioned switching methods, specifically the pill and injection, when si<strong>de</strong>effects were experienced (see Appendix 2 for birth spacing narrative). Provi<strong>de</strong>rs mentionedlimitations in offering implants due to user fear (Oecusse) and lack of training (Baucau).Among survey respon<strong>de</strong>nts who were not currently using family planning, the main reasons werethat they “liked babies” and “heard of other’s bad experience” (Table 5). Among all men and women(contraceptive users and non-users), the main worries or concerns resulted from hearing about otherpeople’s bad experiences, it being against traditional or religious beliefs, and having their ownprevious bad experience.17 A TBA, or other person knowledgeable about medicine that can stop fertility, may speak to the medicine (hamulak) tocall on its power.42<strong>Timor</strong>-<strong>Leste</strong> <strong>Health</strong> <strong>Care</strong> <strong>Seeking</strong> <strong>Behaviour</strong> <strong>Study</strong> | 2009