Deformational Plagiocephaly - The Royal Children's Hospital
Deformational Plagiocephaly - The Royal Children's Hospital
Deformational Plagiocephaly - The Royal Children's Hospital
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
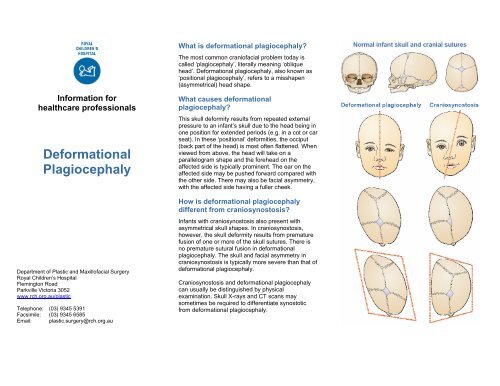
Information forhealthcare professionals<strong>Deformational</strong><strong>Plagiocephaly</strong>Department of Plastic and Maxillofacial Surgery<strong>Royal</strong> Children’s <strong>Hospital</strong>Flemington RoadParkville Victoria 3052www.rch.org.au/plasticTelephone: (03) 9345 5391Facsimile: (03) 9345 6585Email: plastic.surgery@rch.org.auWhat is deformational plagiocephaly?<strong>The</strong> most common craniofacial problem today iscalled ‘plagiocephaly’, literally meaning ‘obliquehead’. <strong>Deformational</strong> plagiocephaly, also known as‘positional plagiocephaly’, refers to a misshapen(asymmetrical) head shape.What causes deformationalplagiocephaly?This skull deformity results from repeated externalpressure to an infant’s skull due to the head being inone position for extended periods (e.g. in a cot or carseat). In these ‘positional’ deformities, the occiput(back part of the head) is most often flattened. Whenviewed from above, the head will take on aparallelogram shape and the forehead on theaffected side is typically prominent. <strong>The</strong> ear on theaffected side may be pushed forward compared withthe other side. <strong>The</strong>re may also be facial asymmetry,with the affected side having a fuller cheek.How is deformational plagiocephalydifferent from craniosynostosis?Infants with craniosynostosis also present withasymmetrical skull shapes. In craniosynostosis,however, the skull deformity results from prematurefusion of one or more of the skull sutures. <strong>The</strong>re isno premature sutural fusion in deformationalplagiocephaly. <strong>The</strong> skull and facial asymmetry incraniosynostosis is typically more severe than that ofdeformational plagiocephaly.Craniosynostosis and deformational plagiocephalycan usually be distinguished by physicalexamination. Skull X-rays and CT scans maysometimes be required to differentiate synostoticfrom deformational plagiocephaly.
Key differencesCraniofacialfeaturesHeadcircumference<strong>Deformational</strong>plagiocephaly• Parallelogramhead shape• Nose generallystraight• Ear moreanterior• Normal rate ofhead growthCausal factors • Externalpressure, e.g.back sleeping,restrictedintrauterineenvironment,musculartorticollis,prematurityDiagnosisTreatingpractitionerTreatment• Clinicalexamination• GP and/orpaediatrician.If concerns,refer to acraniofacialsurgeon• Counterpositioningand/or helmettherapyCraniosynostosis• Rhomboid headshape• Nose rootdeviates towardsfused suture• Orbit on affectedside enlarged• Eyebrowelevated• Ear posterior• Progressiveslowing in headgrowth• Internalmechanisms• Clinicalexamination• Imaging scans• Craniofacialsurgeon• CranialexpansionsurgeryCommon causes of deformationalplagiocephalyBack sleepingInfants who sleep on their backs and/or in car seatswithout alternating their position are at increased riskof deformational plagiocephaly.Muscular torticollisThis is a congenital condition caused by shorteningor tightening of one or more of the neck muscles.This causes the infant’s head to tilt and/or turn tofavour one particular direction.Prematurity<strong>The</strong> cranial bones of premature infants are very softand malleable following birth, and therefore moresusceptible to external pressures.In utero constraintLess frequently, a baby is born with a flattened skulldue to a restricted intrauterine environment or‘crowding’ (i.e. multiple births, breech position, smallmaternal pelvis).Treatment optionsTreatment will vary depending on the nature andseverity of the deformity. Many mild cases do notrequire any treatment and the condition will improvespontaneously when the infant begins to sit. Earlydiagnosis of co-existing torticollis is important as thisdoes require treatment by a paediatricphysiotherapist.More severe deformity may warrant treatment. Inthese cases early referral is advised (between 4-8months of age) as the majority of cranial growth isachieved during the first 12 months of life, and thegreatest amount of correction will be achieved duringthis time.<strong>The</strong> most common forms of treatment are counterpositioning and/or helmet therapy.Counter positioningCounter positioning is recommended where a helmetis not warranted and is most effective between birthand 4 months of age. This involves consistentlyrepositioning the infant’s head so that they do notrest on the flat spot. Increased tummy time and sidelying play when the infant is awake is alsoencouraged. Positioning with rolled up towels cansometimes be of assistance. Counter positioningtechniques can be taught by health professionals,including maternal and child health nurses andpaediatric physiotherapists.Helmet therapyIn moderate to severe cases of deformationalplagiocephaly, and/or where a trial of counterpositioning has failed, a cranial remodelling helmetmay be recommended. <strong>The</strong> helmet assists the skullmoulding process by removing the pressure over theflat area, allowing the skull to grow into the spaceprovided. Helmets are most effective between 4-8months of age. <strong>The</strong> helmet is made of an outer hardshell and is lightweight with a foam lining. <strong>The</strong>y arecustom-made to fit the infant’s head by anexperienced orthotist. This requires the orthotist tomake a casting of the infant’s head. <strong>The</strong> averageduration of helmet therapy is usually 2-6 months,depending on the age of the infant and the severityof the deformational plagiocephaly.<strong>The</strong> helmet is required to be worn for 23 out of 24hours every day. Frequent adjustments are alsorequired on a fortnightly, sometimes weekly, basis toensure proper head growth and optimal correction ofthe deformity.