NCAA Medical Exception Documentation Reporting Form to Support ...
NCAA Medical Exception Documentation Reporting Form to Support ...
NCAA Medical Exception Documentation Reporting Form to Support ...
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
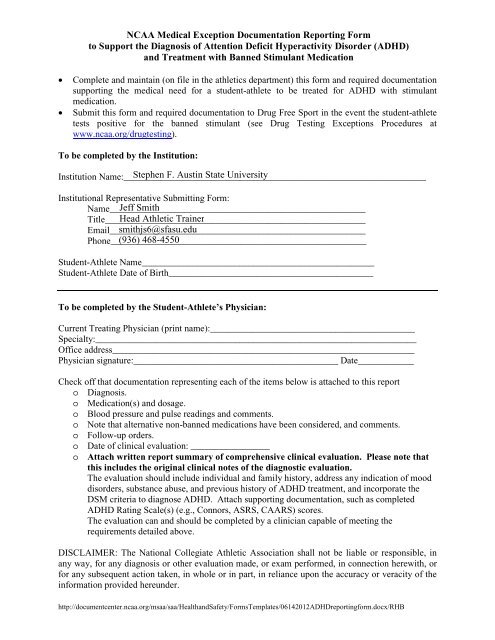
<strong>NCAA</strong> <strong>Medical</strong> <strong>Exception</strong> <strong>Documentation</strong> <strong>Reporting</strong> <strong>Form</strong><strong>to</strong> <strong>Support</strong> the Diagnosis of Attention Deficit Hyperactivity Disorder (ADHD)and Treatment with Banned Stimulant Medication• Complete and maintain (on file in the athletics department) this form and required documentationsupporting the medical need for a student-athlete <strong>to</strong> be treated for ADHD with stimulantmedication.• Submit this form and required documentation <strong>to</strong> Drug Free Sport in the event the student-athletetests positive for the banned stimulant (see Drug Testing <strong>Exception</strong>s Procedures atwww.ncaa.org/drugtesting).To be completed by the Institution:Institution Name:_________________________________________________________________Institutional Representative Submitting <strong>Form</strong>:Name_______________________________________________________Title________________________________________________________Email_______________________________________________________Phone_______________________________________________________Student-Athlete Name__________________________________________________Student-Athlete Date of Birth____________________________________________To be completed by the Student-Athlete’s Physician:Current Treating Physician (print name):____________________________________________Specialty:_____________________________________________________________________Office address_________________________________________________________________Physician signature:____________________________________________ Date____________Check off that documentation representing each of the items below is attached <strong>to</strong> this repor<strong>to</strong> Diagnosis.o Medication(s) and dosage.o Blood pressure and pulse readings and comments.o Note that alternative non-banned medications have been considered, and comments.o Follow-up orders.o Date of clinical evaluation: _________________o Attach written report summary of comprehensive clinical evaluation. Please note thatthis includes the original clinical notes of the diagnostic evaluation.The evaluation should include individual and family his<strong>to</strong>ry, address any indication of mooddisorders, substance abuse, and previous his<strong>to</strong>ry of ADHD treatment, and incorporate theDSM criteria <strong>to</strong> diagnose ADHD. Attach supporting documentation, such as completedADHD Rating Scale(s) (e.g., Connors, ASRS, CAARS) scores.The evaluation can and should be completed by a clinician capable of meeting therequirements detailed above.DISCLAIMER: The National Collegiate Athletic Association shall not be liable or responsible, inany way, for any diagnosis or other evaluation made, or exam performed, in connection herewith, orfor any subsequent action taken, in whole or in part, in reliance upon the accuracy or veracity of theinformation provided hereunder.http://documentcenter.ncaa.org/msaa/saa/HealthandSafety/<strong>Form</strong>sTemplates/06142012ADHDreportingform.docx/RHB
ATTACHMENTAttention Deficit Hyperactivity Disorder (ADHD) Guideline AttachmentCriteria for letter from prescribing Physician <strong>to</strong> provide documentation <strong>to</strong> the AthleticsDepartment/Sports Medicine staff regarding assessment of student-athletes taking prescribedstimulants for Attention Deficit Hyperactivity Disorder (ADHD), in support of an <strong>NCAA</strong><strong>Medical</strong> <strong>Exception</strong> request for the use of a banned substance.The following must be included in supporting documentation:Student-athlete name.Student-athlete date of birth.Date of clinical evaluation.Clinical evaluation components including:o Summary of comprehensive clinical evaluation (referencing DSM-IV criteria) -- attachsupporting documentation.o ADHD Rating Scale(s) (e.g., Connors, ASRS, CAARS) scores and report summary -- attachsupporting documentation.o Blood pressure and pulse readings and comments.o Note that alternative non-banned medications have been considered, and comments.o Diagnosis.o Medication(s) and dosage.o Follow-up orders.Additional ADHD evaluation components if available:Report ADHD symp<strong>to</strong>ms by other significant individual(s).Psychological testing results.Physical exam date and results.Labora<strong>to</strong>ry/testing results.Summary of previous ADHD diagnosis.Other comments.<strong>Documentation</strong> from prescribing physician must also include the following:Physician name (Printed)Office address and contact information.Specialty.Physician signature and date.DISCLAIMER: The National Collegiate Athletic Association shall not be liable or responsible, inany way, for any diagnosis or other evaluation made, or exam performed, in connection herewith, orfor any subsequent action taken, in whole or in part, in reliance upon the accuracy or veracity of theinformation provided hereunder.The National Collegiate Athletic AssociationJanuary 30, 2009MEW:rhb
<strong>NCAA</strong> <strong>Medical</strong> <strong>Exception</strong>s Policy<strong>Reporting</strong> GuidelinesJanuary 30, 2009Page No. 3_________5. Requesting an <strong>NCAA</strong> <strong>Medical</strong> <strong>Exception</strong>:a. The student-athlete should report the banned medication <strong>to</strong> the institution upon matriculationor when treatment commences in order for the student-athlete <strong>to</strong> be eligible for a medicalexception in the event of a positive drug test.b. A student-athlete’s medical records or physician’s letter should not be sent <strong>to</strong> the <strong>NCAA</strong>,unless requested by the <strong>NCAA</strong>.c. The use of the prescribed stimulant medication does not need <strong>to</strong> be reported at the time of<strong>NCAA</strong> drug testing.d. <strong>Documentation</strong> should be submitted by the institution in the event a student-athlete testspositive for the banned stimulant.Note: The <strong>NCAA</strong> Committee on Competitive Safeguards and <strong>Medical</strong> Aspects of Sports mayapprove stimulant medication use for ADHD without a prior trial of a non-stimulant medication.Although the <strong>NCAA</strong> <strong>Medical</strong> <strong>Exception</strong> Policy requires that a non-banned medication be considered,the medical community has generally accepted that the non-stimulant medications may not be aseffective in the treatment of ADHD for some in this age group.The National Collegiate Athletic AssociationJanuary 30, 2009MEW:rhb
ThisPageIntentionallyLeftBlank
<strong>NCAA</strong> Guidelines <strong>to</strong> Document ADHD Treatment with Banned Stimulant MedicationsAddendum <strong>to</strong> the January 2009 GuidelinesQ & A March 2009Updated July 2010(*New Questions)1. *What is the outcome in the case of a student-athlete who tests positive for stimulantmedication prescribed <strong>to</strong> them by a legitimate medical provider but has no documentation<strong>to</strong> support the diagnosis, and who subsequently undergoes an evaluation that determinesthe student-athlete does not have ADD/ADHD? This case above will be reviewed under the drug-testing appeals process. Theoutcome of that process may be not <strong>to</strong> penalize the student-athlete, but require thestudent-athlete <strong>to</strong> discontinue using the banned medication.2. *Is the documentation of a diagnostic assessment required <strong>to</strong> meet the <strong>NCAA</strong> <strong>Medical</strong><strong>Exception</strong> Policy for treatment with stimulants for ADD/ADHD the same as that requiredfor academic accommodations through the institution’s disability resource center?No, the diagnostic evaluation <strong>to</strong> meet the <strong>NCAA</strong> documentation criteria does notneed <strong>to</strong> include the full battery of testing for learning disabilities generally conductedfor the institution’s disability resource center review. In order <strong>to</strong> meet <strong>NCAA</strong>criteria, the institution must submit documentation of the clinicians write up, <strong>to</strong>include a comprehensive his<strong>to</strong>ry and assessment as it relates <strong>to</strong> DSM criteria forADHD, including the measures used <strong>to</strong> rate the student-athlete’s symp<strong>to</strong>ms ofattention deficit. This evaluation should be accompanied by a signed letter from theprescribing physician describing the course of treatment and current prescription.3. Why is the <strong>NCAA</strong> instituting a stricter application of the medical exception policy for theuse of banned stimulant medications <strong>to</strong> treat ADHD?The stricter application reflects a stronger stand on policy enforcement, protecting thestudent-athlete competing while using these stimulants, and the integrity of the sport.This stricter application of the medical exception policy is intended <strong>to</strong> provideclearer documentation of the student-athlete’s evaluation, and not intended <strong>to</strong>replace the clinician’s evaluation and treatment.As experienced across campus, more and more college students-athletes are beingtreated with stimulant medications for ADHD. These stimulants are banned for use in<strong>NCAA</strong> competition for both performance and health reasons, and using them mayresult in a positive drug test and loss of eligibility, unless the student-athlete providesadequate documentation of a diagnostic evaluation for ADHD and appropriatemoni<strong>to</strong>ring of treatment. In recent years, the number of student-athletes testing
Addendum <strong>to</strong> January 2009 ADHD TreatmentWith Banned Stimulants GuidelinesJuly 20, 2009Page No. 2_________positive for these stimulant medications has increased 3 fold, and in many cases therehas been inadequate documentation submitted in support of the request for a medicalexception <strong>to</strong> the <strong>NCAA</strong> banned drug policy.4. Who was consulted in the development of the guidelines?The <strong>NCAA</strong> sought consultation from MDs, Psychiatrists, Psychologists and others inthe development of the guidelines for appropriate documentation requirements; thesewere then reviewed and approved by the <strong>NCAA</strong> Committee on CompetitiveSafeguards and <strong>Medical</strong> Aspects of Sports.5. How was the change communicated <strong>to</strong> the membership?Beginning in January 2008, the membership received notification of the effective dateof the stricter application -- August 2009 – in the form of <strong>NCAA</strong> News articles,notices in email communications, and the posting of a video describing the rationaland expectations of the stricter application. This 18 month period of notice wouldallow member institutions <strong>to</strong> inform current and incoming student-athletes <strong>to</strong> beprepared <strong>to</strong> gather the necessary documentation of the diagnosis, course of treatmentand current prescription.6. Who needs <strong>to</strong> conduct the evaluation?The initial evaluation may be conducted by clinicians with experience in assessingADHD; these include school psychologists, clinical psychologists, psychiatrists, otherMD’s and their supervised clinicians.7. What type of ADHD evaluation documentation needs <strong>to</strong> be submitted <strong>to</strong> support anADHD diagnosis and treatment with banned stimulant medication? What is acceptableand what is not acceptable proof an evaluation has been conducted?The documentation should include a comprehensive clinical evaluation, recordingobservations and results from ADHD rating scales, a physical exam and any labwork, previous treatment for ADHD, and the diagnosis and recommended treatment.The physician can provide documentation of the above either with a cover letter andattachments or provide the medical record. This documentation should be kept on filein the athletics department until such time that the student-athlete tests positive for the
Addendum <strong>to</strong> January 2009 ADHD TreatmentWith Banned Stimulants GuidelinesJuly 20, 2009Page No. 3_________stimulant. A simple statement from the prescribing physician that he or she istreating the student-athlete for ADHD with said medication IS NOT adequatedocumentation.8. Will an assessment conducted more than three-five years ago be acceptable?Yes, in fact the expectation is that for many student-athletes, the evaluation andinitiation of treatment likely began during grade school. <strong>Documentation</strong> of thatevaluation, along with the his<strong>to</strong>ry of treatment and current prescription, should besubmitted by the student-athlete <strong>to</strong> their sports medicine staff upon matriculation.9. What is required of a student-athlete who for years has been prescribed stimulantmedication <strong>to</strong> treat ADHD but has not undergone a full assessment?In order <strong>to</strong> obtain a medical exception, the student-athlete must undergo a fullassessment as described above. This may be conducted on campus, through acommunity mental health service, or by any experienced clinician.10. Does a student-athlete need <strong>to</strong> have an updated letter from the prescribing physician onfile each year of their eligibility?Yes, an annual follow-up with the prescribing physician is the minimum standard,and that can be reflected in a letter from the physician or a copy of the medicalrecord, with written indication of the current treatment.11. Do physicians have <strong>to</strong> use a certain form when performing the evaluation for ADHD? There is no specific form physicians need <strong>to</strong> use <strong>to</strong> perform an evaluation. Theguidelines present the criteria identifying what <strong>to</strong> report, and several ADHD ratingscales are listed, but it is the <strong>to</strong>tality of the clinician’s evaluation that should bereflected in the documentation. This evaluation should be conducted by a clinicianexperienced in assessing ADHD12. Can an institution pay for the evaluation <strong>to</strong> diagnose ADHD?From an interpretation: Institution paying for academic performance testing
Addendum <strong>to</strong> January 2009 ADHD TreatmentWith Banned Stimulants GuidelinesJuly 20, 2009Page No. 4_________Date Issued: Oc<strong>to</strong>ber 26, 1988 Date Published: Oc<strong>to</strong>ber 26, 1988 (Item Ref: g).g. Institution Paying for Academic Performance Testing: Determined thatConstitution 3-1-(h)-(4)-(i) [incidental benefits -- tu<strong>to</strong>ring expenses] would permit aninstitution <strong>to</strong> pay for tests <strong>to</strong> determine the academic performance level of enrolledstudent-athletes in order <strong>to</strong> identify potential academic problems, inasmuch as such adiagnostic test is considered part of the tu<strong>to</strong>ring process. Recommended that thisinterpretation be published in LAC subsequent <strong>to</strong> review by LIC.13. What happens if neither the school nor student-athlete can afford <strong>to</strong> pay for the testing?In each division, the institution can submit an incidental expense waiver. ForDivision I, SAOF may be used if it is approved by their conference office.14. Some student-athletes are embarrassed and don’t reveal that they are taking medicationfor ADHD. How does the institution address this issue?The institution should be proactive in communicating the importance <strong>to</strong> all studentathletesabout reporting <strong>to</strong> sports medicine all medical issues and medications – inorder <strong>to</strong> avoid loss of eligibility and <strong>to</strong> respond appropriately in any medicalemergency. The need for this reporting should be expressed <strong>to</strong> the student-athlete asstandard operating procedure and addressed during initial medical assessments andsubsequent health his<strong>to</strong>ries. The <strong>NCAA</strong> is preparing a poster <strong>to</strong> remind studentathletes<strong>to</strong> report all medications.15. Does the student-athlete need <strong>to</strong> first try non-stimulant medication <strong>to</strong> treat ADHD?The student-athlete does not need <strong>to</strong> be put on a trial of non-stimulant medication, butthe documentation must note that a non-stimulant alternative was considered and whythe stimulant medication was chosen.16. If a student-athlete received a medical exception for the use of banned stimulantmedication <strong>to</strong> treat ADHD prior <strong>to</strong> August 2009, will that student-athlete be required <strong>to</strong>meet this policy application?There is no ‘grandfathering’ on this issue; for any positive drug test occurring fromAugust 1, 2009, a medical exception for the use of banned stimulant medication must
Addendum <strong>to</strong> January 2009 ADHD TreatmentWith Banned Stimulants GuidelinesJuly 20, 2009Page No. 5_________include the required documentation, even if a student-athlete has received a medicalexception for ADHD stimulant medication prior <strong>to</strong> August 2009.17. How will the policy address a student-athlete who tests positive for a banned stimulantprescribed by their physician but has not undergone a full assessment for an ADHDdiagnosis?If a student-athlete has not undergone an evaluation and/or cannot produce documentsat the time the positive test is confirmed with the institution, the student-athlete mustbe declared ineligible until 1) the documentation can be produced or 2) a drug-testappeal is heard and approved.18. Does a student-athlete currently on stimulant medication but lacking a formal evaluationneed <strong>to</strong> discontinue the medicine in order <strong>to</strong> undergo the assessment?If a student-athlete has been on a prescribed stimulant medication, but no evaluationdocumentation is available, and the student-athlete will be referred for evaluation <strong>to</strong>document the diagnosis of ADHD, they can continue the medication if helpful andthey are <strong>to</strong>lerating it. Clinicians familiar with ADHD regularly seepatients who aretaking ADHD medications and have no formal documentation at the time. There isno need <strong>to</strong> s<strong>to</strong>p the medication and interfere with appropriate treatment of the medicalcondition. The evaluation is a clinical evaluation which includes taking acomprehensive his<strong>to</strong>ry, evaluation current/past symp<strong>to</strong>ms, reviewing the effects ofmedications (including getting information from the patient's prescription/medbottle), checklists, etc. There is no need <strong>to</strong> take the patient off the medication forevaluation especially if they are doing well.19. How will clinical notes and testing results be secure once the institution sends thesedocuments <strong>to</strong> the <strong>NCAA</strong>?The information provided by the school <strong>to</strong> the <strong>NCAA</strong> <strong>to</strong> address drug-testing issues iscovered by the Student-Athlete Statement and Drug-Testing Consent complianceforms. All subsequent use of these materials by <strong>NCAA</strong> review committees followstrict <strong>NCAA</strong> confidentiality pro<strong>to</strong>cols20. How will this policy be communicated <strong>to</strong> student-athletes?
Addendum <strong>to</strong> January 2009 ADHD TreatmentWith Banned Stimulants GuidelinesJuly 20, 2009Page No. 6_________The institution is responsible <strong>to</strong> communicate <strong>to</strong> all student-athletes <strong>NCAA</strong> banneddrug policies, including the medical exception policy. The medical exception policyinformation is available in the Drug-Testing Program handbook, on-line at <strong>NCAA</strong>.organd also included in the Drug-Education and Drug-Testing video (<strong>to</strong> be updatedsummer 2009). In addition, the <strong>NCAA</strong> will provide posters spring 2009 <strong>to</strong> all <strong>NCAA</strong>institutions that alert student-athletes <strong>to</strong> the need <strong>to</strong> report all medications.The National Collegiate Athletic AssociationJuly 20, 2010MEW:rhb
Adult Attention Deficit Hyperactivity Disorder (ADHD)Sample Evaluation <strong>Form</strong>at*Comprehensive Clinical Assessment.1. Careful Longitudinal His<strong>to</strong>ry Identifying Lifelong Symp<strong>to</strong>ms and Current Impairment.**Evaluate for other conditions in addition <strong>to</strong> ADHD that would explain the symp<strong>to</strong>ms and impairmentincluding:Mood disorders (major depressive disorder, bipolar disorder)Anxiety disorders (panic, obsessive-compulsive, generalized anxiety, social anxiety, posttraumaticstress)Substance use disordersAntisocial disorderLearning disorders2. Past His<strong>to</strong>ry.PsychiatricGeneral <strong>Medical</strong> (focus on cardiovascular disease risk fac<strong>to</strong>rs)OccupationalRelationshipLegalMedications (prescribed, over-the-counter, alternative, supplements)Substance use (alcohol, caffeine, nicotine, illicit)Review of previous medical records if available3. Personal/Social His<strong>to</strong>ry (includes corroboration of patient ADHD symp<strong>to</strong>m reports if available).4. Family His<strong>to</strong>ry.PsychiatricGeneral <strong>Medical</strong> (focus on cardiovascular disease risk fac<strong>to</strong>rs)5. Review of Systems.General (focus on cardiovascular disease risk fac<strong>to</strong>rs)SleepAppetiteWeightSuicide/Homicide6. Mental Status Examination.7. Physical Exam/Indicated Labora<strong>to</strong>ry/Testing*** (e.g., blood pressure, pulse, electrocardiogram).
Adult ADHD Sample Evaluation <strong>Form</strong>atJanuary 30, 2009Page No. 2_________8. Adult ADHD Rating Scales [e.g., Adult ADHD Self-Report Scale (ASRS); Conners’ Adult ADHDRating Scales (CAARS)].9. Other Testing (e.g., psychological/neuropsychological testing).10. Assessment/Diagnosis.11. Treatment /Follow-up Plan (e.g., initial follow-up +/- 1 month; periodically thereafter).12. Consultation with ADHD experienced practitioner as needed.13. Disability services evaluation as needed.14. Fact sheet for stimulant use for ADHD.15. Review of important safety information regarding stimulant use (e.g., avoidance in symp<strong>to</strong>maticcardiovascular disease, moderate <strong>to</strong> severe hypertension, hyperthyroidism, glaucoma, during orwithin 14 days of MAOI use).16. Practitioner policy for stimulant misuse; lost or s<strong>to</strong>len stimulant prescription.Sample: STUDENT STIMULANT MISUSE POLICY:Stimulants are Schedule-II drugs, which are controlled medications by the DEA (DrugEnforcement Administration). This means your doc<strong>to</strong>r cannot give refills for your stimulantmedication unless a new prescription is written for each refill. Schedule-II medications cannotbe refilled by telephone. Misuse of stimulant medications is a common and recognizedconcern in the USA. THIS OFFICE WILL NOT TOLERATE MISUSE. EVEN THEAPPEARANCE OF MISUSE IS ENOUGH JUSTIFICATION TO CEASESTIMULANT TREATMENT. THERE WILL BE NO REFILLS GIVEN FOR LOSTOR STOLEN PRESCRIPTIONS. Do not give your prescription medication <strong>to</strong> anyone.Keep your medication in a safe place where others do not have access.* <strong>Form</strong>at is intended as a guideline and not as a specific way <strong>to</strong> practice. It is an example drawn fromclinical practice experience and current scientific literature. The prescribing practitioner should useindividual professional judgment.** Impairment defined as relative <strong>to</strong> an average-functioning individual.*** There are no across-the-board recommendations for labora<strong>to</strong>ry testing or diagnostic examinations foradult ADHD. The prescribing practitioner may request testing as individually indicated and appropriate.<strong>NCAA</strong>/01/30/2009/MEW:rhb
The ADHD-RS-rv with Adult Prompts is an I8-item scale based on the DSM-IV-TR" criteria for ADHD that provides a rating of the severity of symp<strong>to</strong>ms. The adult prompts serve as a guide <strong>to</strong> explore more fully the extent and severity ofADHD symp<strong>to</strong>ms and create a framework <strong>to</strong> ascertain impairment. The first 9 items assess inattentive symp<strong>to</strong>ms and the last 9 items assess hyperactive-impulsive symp<strong>to</strong>ms. Scoring is based on a 4-point Likert-type severity scale: 0 =none, I '" 2 '" moderate, 3 =severe. Clinicians should score the highest score that is generated for the prompts for each item. Example: if one prompt generates a "2" and all others are a "1," by convention, the rating for that item is still a "2"Significant symp<strong>to</strong>ms in clinical trials are generally considered at least a "2" moderate.AdultADHD-RS-IV* with Adult Prompts f1. CarelessnessDo you make a lot of mistakes (in school or work)?Is this because you're careless?Do you rush through work or activities?Do you have trouble with detailed work?Do you not check your work?Do people complain that you're careless?Are you messy orIs your desk or workspace so messy that you have difficulty finding things? 2. Difficulty sustaining attention in activitiesDo you have trouble attention whenwatching movies, reading, or attending lectures?Or on fun activities such as sports or board games?Is it hard for you <strong>to</strong> keep your mind on school orwork? Do you have unusual trouble staying focusedon boring or repetitive tasks?Does it take a lot longer than it should <strong>to</strong> completetasks because you can't keep your mind on the task?Is it even harder for you than some others you know?Do you have trouble remembering what you read and do you need <strong>to</strong> re-read the same passage several times? 3. Doesn't listenDo people (spouse, boss, colleagues, friends)complain that you don't seem <strong>to</strong> listen or respond(or daydream) when spoken <strong>to</strong> or when asked <strong>to</strong> dotasks? A lot?Do people have <strong>to</strong> repeat directions?Do you find that you miss the key parts ofconversationsbecause ofdrifting off in your own thoughts? Does it cause problems? 4. No follow throughDo you have trouble finishing things (such as work or chores)?Do you often leave things half done and start another project?Do you need consequences (such as deadlines) <strong>to</strong> finish?Do you have trouble following instructions (especiallycomplex, multistep instructions that have <strong>to</strong> be done ina certain order with different steps)? Do you need <strong>to</strong> write down instructions, otherwise you will forget them? None Mild Moderate Severe None Mild Moderate Severeo 1 2 3 5. Can't organize 0 1 2 3Do you have trouble organizi ng tasks in<strong>to</strong> ordered steps?Is it hard prioritizing work and chores?Do you need others ro plan for you?Do you have trouble with time management? Does itcause problems?Does difficulty in planni ng lead <strong>to</strong> procrastination andputting off tasks until the last moment6. Avoids/dislikes tasks requiring sustained mental effort 0 1 2 3Do you avoid tasks (work, chores, reading, boardo 1 2 3 that are challenging or lengthy because it's hard (Q stayfocused on these <strong>to</strong>r a long time?Do you have <strong>to</strong> force yourself <strong>to</strong> do these tasks?How hard is it?Do you procrastinate and put off tasks until thelast moment possible?7. Loses important items 0 1 2 3Do you lose things important work papers,o 1 2 3 wallet, coats, etc)? A lot? More than others?Are you constantly looking for important items?Do you get in<strong>to</strong> trouble for this (at work or at home)?Do you need <strong>to</strong> put items glasses, wallet, keys) inthe same place each time, otherwise you will lose them?8. Easily distractible 0 1 2 3o 1 2 3 Are you ever vety easily distracted by events aroundyou such as noise (conversation, lV, radio), movement,or clutter?Do you need relative isolation <strong>to</strong> get work done?Can almost anything get your mind off ofwhat you aredoing, such as work, chores, or ifyou're<strong>to</strong> someone?Is it hard <strong>to</strong> get back <strong>to</strong> a task once you s<strong>to</strong>p?9. Forgetful in daily activities 0 1 2 3Do you forget a lot of things in your daily routine? Likewhat? Chores? Work? Appointments or obligations?Do you forget <strong>to</strong> bring things <strong>to</strong> work, such as workmaterials or assignments due that day?Do you need <strong>to</strong> write regular reminders <strong>to</strong> yourself <strong>to</strong> domost activities or tasks, otherwise you will forget?
'From ADHD Rating Scale-IV: Checklists, Norms and ClinicillInmpmation. Reprinted with permiSSion ofThe Guilford Press: New York. {;)1998 George J. DuPaul, Thomas J. Power, Arthur A. Anas<strong>to</strong>poulos and Robert Reid. This scale may not be reproduced in any form withoutwritten permission ofThe Guilrord Press. www.guilford.comtprompts developed by Lenard Adler, MD, Thomas Spencer, MD, and Joseph Biederman, MD.{;)2003 New York University and Massachusetts General Hospital. All rights reserved, DO NOT REPRODUCE W'lTHOUT WRITIEN PERMISSION 01' MASSACHUSETIS GENERAL HOSPITAL OR NEW YORK UNIVERSITY.THERE ARE NO WARRANTIES REGARDING THIS ATTENTION DEFICIT HYPERACTIVITY DISORDER RATING SCALE IVAND ADULT PROMPTS ("SCALE"), EXPRESS OR IMPLIED, INCLUDING WITHour LIMITATION, IMPLIED WARRANTIESOF MERCHANTABILITY AND FITNESS FOR A PARTICULAR PURPOSE, AND ALL OTHER REPRESENTATIONS OR WARRANTIES 01' ANY KIND ARE HEREBY DISCLAIMED. New York Universiry and rhe Massachusetts General Hospital shall neitherexercise comrol over nor incerfere with the physician-patient relationship of users of this Scale and shaJj not be responsible for any use made of this Scale, including any medical decisions regarding the care and treatment of patients using the Scale.ADHD 502 04/0810. Squirms and fidgetsCan you sit still or are you always moving yourhands or teet, or fidgeting in your chair?Do you tap your pencil or your feet? A lot? Do peoplenotice?AdultADHD-RS-IV* with Adult Prompts fNone Mild Moderate Severe0 1 2 315. Talks excessivelyDo you talk a lot? All the time? More than other people?Do people complain about your talking? Is it a problem?Are you often louder than the people you are talking <strong>to</strong>?None Mild Moderate Severe0 1 2 3Do you regularly play with your hair or clothing? 16. Blurts out answers 0 1 2 3Do you consciously resist fidgeting or squirming?Do you give answers <strong>to</strong> questions before someonefinishes asking?11. Can't stay seated0 1 2 3Do you say things before it is your turn?Do you have trouble staying in your seat? At work?Do you say things that don't fit in<strong>to</strong> the conversation?In class? At home (eg, watching TV, dinner)?Do you do things without thinking? A lot?In church or temple?Do you choose <strong>to</strong> walk around rather than sir? 17. Can't wait for tum 0 1 2 3Do you have <strong>to</strong> force yourself <strong>to</strong> remain seated?Is it hard for you <strong>to</strong> wait your rum (in conversation,Is ir difficult for you <strong>to</strong> sit through a long meetingin lines, whileor lecture?Are you frequently frustrated with delavs? Does itDo you try <strong>to</strong> avoid going <strong>to</strong> functions rhat requirecause problems?you <strong>to</strong> sit still for long periods of time?Do you put a great deal ofeffort in<strong>to</strong> planning <strong>to</strong> not be in12. Runs/climbs excessively 0 1 2 3situations where you might have <strong>to</strong> wait?Are you physically restless? 18. Intrudes/interrupts others 0 1 2 3Do you feel restless inside? A lor?Do you talk when others are talking, without waiting untilDo you feel more agitated when you cannot exerciseyou are acknowledged?on an almost daily basis?Do you butt in<strong>to</strong> others' conversations before being invited?Do you interrupt others' activities?13. Can't play/work quiedy0 1 2 3Is it hard for you <strong>to</strong> wait <strong>to</strong> get your point across inDo you have a hard time playing/working quiedy?conversations or atleisure activity (nonstrucrured times or onyour own such as a book, listening <strong>to</strong> music,a board game), are you agitated orDo you always need <strong>to</strong> be busy after work or while onvacation?14. On the go, "driven by a mo<strong>to</strong>r" 0 1 2 3Is it hard for you <strong>to</strong> slow down?Do you feel like you (often) have a lot of energyand that you always have [0 be moving, are always"on the go"?Do you feel like you're driven by a mo<strong>to</strong>r?Do you feel unable <strong>to</strong> relax?
Adult ADHD Self-Report Scale (ASRS-v1.1) Symp<strong>to</strong>m ChecklistInstructionsThe questions on the back page are designed <strong>to</strong> stimulate dialogue between you and your patients and <strong>to</strong> helpconfirm if they may be suffering from the symp<strong>to</strong>ms of attention-deficit/hyperactivity disorder (ADHD).Description: The Symp<strong>to</strong>m Checklist is an instrument consisting of the eighteen DSM-IV-TR criteria.Six of the eighteen questions were found <strong>to</strong> be the most predictive of symp<strong>to</strong>ms consistent withADHD. These six questions are the basis for the ASRS v1.1 Screener and are also Part A of theSymp<strong>to</strong>m Checklist. Part B of the Symp<strong>to</strong>m Checklist contains the remaining twelve questions.Instructions:Symp<strong>to</strong>ms1. Ask the patient <strong>to</strong> complete both Part A and Part B of the Symp<strong>to</strong>m Checklist by marking an Xin the box that most closely represents the frequency of occurrence of each of the symp<strong>to</strong>ms.2. Score Part A. If four or more marks appear in the darkly shaded boxes within Part A then thepatient has symp<strong>to</strong>ms highly consistent with ADHD in adults and further investigation iswarranted.3. The frequency scores on Part B provide additional cues and can serve as further probes in<strong>to</strong> thepatient’s symp<strong>to</strong>ms. Pay particular attention <strong>to</strong> marks appearing in the dark shaded boxes. Thefrequency-based response is more sensitive with certain questions. No <strong>to</strong>tal score or diagnosticlikelihood is utilized for the twelve questions. It has been found that the six questions in Part Aare the most predictive of the disorder and are best for use as a screening instrument.Impairments1. Review the entire Symp<strong>to</strong>m Checklist with your patients and evaluate the level of impairmentassociated with the symp<strong>to</strong>m.2. Consider work/school, social and family settings.3. Symp<strong>to</strong>m frequency is often associated with symp<strong>to</strong>m severity, therefore the Symp<strong>to</strong>mChecklist may also aid in the assessment of impairments. If your patients have frequentsymp<strong>to</strong>ms, you may want <strong>to</strong> ask them <strong>to</strong> describe how these problems have affected the ability<strong>to</strong> work, take care of things at home, or get along with other people such as theirspouse/significant other.His<strong>to</strong>ry1. Assess the presence of these symp<strong>to</strong>ms or similar symp<strong>to</strong>ms in childhood. Adults who haveADHD need not have been formally diagnosed in childhood. In evaluating a patient’s his<strong>to</strong>ry,look for evidence of early-appearing and long-standing problems with attention or self-control.Some significant symp<strong>to</strong>ms should have been present in childhood, but full symp<strong>to</strong>mology is notnecessary.
Adult ADHD Self-Report Scale (ASRS-v1.1) Symp<strong>to</strong>m ChecklistPatient NameToday’s DatePlease answer the questions below, rating yourself on each of the criteria shown using thescale on the right side of the page. As you answer each question, place an X in the box thatbest describes how you have felt and conducted yourself over the past 6 months. Please givethis completed checklist <strong>to</strong> your healthcare professional <strong>to</strong> discuss during <strong>to</strong>day’sappointment.NeverRarelySometimesOftenVery Often1. How often do you have trouble wrapping up the final details of a project,once the challenging parts have been done?2. How often do you have difficulty getting things in order when you have <strong>to</strong> doa task that requires organization?3. How often do you have problems remembering appointments or obligations?4.When you have a task that requires a lot of thought, how often do you avoidor delay getting started?5. How often do you fidget or squirm with your hands or feet when you have<strong>to</strong> sit down for a long time?6. How often do you feel overly active and compelled <strong>to</strong> do things, like youwere driven by a mo<strong>to</strong>r?Part A7. How often do you make careless mistakes when you have <strong>to</strong> work on a boring ordifficult project?8. How often do you have difficulty keeping your attention when you are doing boringor repetitive work?9. How often do you have difficulty concentrating on what people say <strong>to</strong> you,even when they are speaking <strong>to</strong> you directly?10. How often do you misplace or have difficulty finding things at home or at work?11. How often are you distracted by activity or noise around you?12. How often do you leave your seat in meetings or other situations in whichyou are expected <strong>to</strong> remain seated?13. How often do you feel restless or fidgety?14. How often do you have difficulty unwinding and relaxing when you have time<strong>to</strong> yourself?15. How often do you find yourself talking <strong>to</strong>o much when you are in social situations?16. When you’re in a conversation, how often do you find yourself finishingthe sentences of the people you are talking <strong>to</strong>, before they can finishthem themselves?17. How often do you have difficulty waiting your turn in situations whenturn taking is required?18. How often do you interrupt others when they are busy?Part B
<strong>NCAA</strong> <strong>Medical</strong> <strong>Exception</strong>s – including case examples for use of stimulants, finasteride (Propecia),and tes<strong>to</strong>sterone. This stricter application will be applied effective August 2009.The <strong>NCAA</strong> list of banned drug classes is composed of substances that are generally reported <strong>to</strong> beperformance enhancing. The <strong>NCAA</strong> bans performance enhancing drugs <strong>to</strong> protect student-athletehealth and safety and ensure a level playing field, and it also recognizes that some of these substancesmay be legitimately used as medications <strong>to</strong> treat student-athletes with learning disabilities and othermedical conditions.Accordingly, the <strong>NCAA</strong> allows exceptions <strong>to</strong> be made for those student-athletes with a documentedmedical his<strong>to</strong>ry demonstrating the need for regular use of such a drug. The benefit of a medicalexception procedure is that in most cases the student-athlete’s eligibility remains intact during theprocess.<strong>Exception</strong>s may be granted for substances included in the following classes of banned drugs:stimulants, beta blockers, diuretics, anti-estrogens, anabolic agents (steroids)*, and peptide hormones*(Bylaw 31.2.3). (*anabolic agents and peptide hormones must be approved by the <strong>NCAA</strong> beforethe athlete is allowed <strong>to</strong> participate while taking these medications. The institution, through itsdirec<strong>to</strong>r of athletics, may request an exception for use of an anabolic agent or peptide hormone bysubmitting <strong>to</strong> The National Center for Drug Free Sport (Drug Free Sport) any medical documentation itwishes <strong>to</strong> have considered.)In all cases, a student-athlete, in conjunction with his or her physician, must document tha<strong>to</strong>ther non-banned alternatives have been considered prior <strong>to</strong> requesting the medical exceptionfor the use of a medication containing a banned substance. It is the responsibility of the institution<strong>to</strong> educate student-athletes about this policy, and <strong>to</strong> follow-up with any student-athlete who identifiesthe use of a banned medication <strong>to</strong> determine if standard non-banned medications have been pursuedand documented.In order for a student-athlete <strong>to</strong> be granted a medical exception for the use of a medication thatcontains a banned substance, the student-athlete must:have declared the use of the substance <strong>to</strong> his or her athletics administra<strong>to</strong>r responsible forkeeping medical records,present documentation of the diagnosis of the condition, andprovide documentation from the prescribing physician explaining the course of treatment andthe current prescription.Requests for medical exceptions will be reviewed by physicians who are members of the <strong>NCAA</strong>Committee on Competitive Safeguards and <strong>Medical</strong> Aspects of Sports. <strong>Medical</strong> exceptions will begranted if the student-athlete has presented adequate documentation noted above.Unless requesting a review for the medical use of an anabolic agent or peptide hormone, a studentathlete'smedical records or physicians' letters should not be sent <strong>to</strong> the <strong>NCAA</strong> unless requested by the<strong>NCAA</strong>. Also, the use of the substance need not be reported at the time of <strong>NCAA</strong> drug testing.________________________________The National Collegiate Athletic AssociationMarch 11, 2008MEW
Following are three treatment issues <strong>to</strong> help illustrate the medical exception procedure:ADHD – Attention Deficit/Hyperactivity Disorder is one of the most common neurobehavioral disordersof childhood and can persist through adolescence and in<strong>to</strong> adulthood. ADHD is generally diagnosed inchildhood, but sometimes not until college or later. The most common medications used <strong>to</strong> treat ADHDare methylphenidate (Ritalin) and amphetamine (Adderall), which are banned under the <strong>NCAA</strong> class ofstimulants. In order for a medical exception <strong>to</strong> be granted for the use of these stimulant medications,the student-athlete must show that he or she has undergone standard assessment <strong>to</strong> identify ADHD.Frequently a student-athlete may find that the demands of college present difficult learning challenges.They may realize that some of their teammates are benefitting from the use of these medications, andfigure they should ask their team physician or family doc<strong>to</strong>r <strong>to</strong> prescribe the same for them. If they donot undergo a standard assessment <strong>to</strong> diagnose ADHD, they have not met the requirements foran <strong>NCAA</strong> medical exception. Most colleges provide these types of assessment through their studentsupport services or counseling and testing centers. The student-athlete should either providedocumentation of an earlier assessment, or undergo an assessment prior <strong>to</strong> using stimulant medicationfor ADHD. If the diagnosis is ADHD, the student-athlete may then pursue treatment with the teamphysician or family physician for a prescription for stimulant medication, and provide all documentation<strong>to</strong> the appropriate athletics administra<strong>to</strong>r <strong>to</strong> keep in the file in the event the student-athlete is selectedfor drug testing and tests positive. At that point, the athletics administra<strong>to</strong>r will be instructed <strong>to</strong> providethe documentation for review by the medical panel, and if all is in order, the student-athlete’s medicalexception is granted.Male-pattern baldness -- Androgenic alopecia is a common form of hair loss in both men and women.In men, this condition is also known as male-pattern baldness. Hair is lost in a well-defined pattern,beginning above both temples. Over time, the hairline recedes <strong>to</strong> form a characteristic "M" shape. Hairalso thins at the crown of the head, often progressing <strong>to</strong> partial or complete baldness. Non-bannedmedications are available <strong>to</strong> treat this condition. Finasteride (trade name Propecia), which isprescribed in some cases <strong>to</strong> treat male-pattern baldness, is a banned substance under the class ofmasking agents, as it interferes with the ability <strong>to</strong> identify steroid use. Before using finasteride, astudent-athlete must exhaust other standard medications and document this effort. All documentationshould be submitted <strong>to</strong> the sports medicine staff <strong>to</strong> review and maintain in the student-athlete’s record.In the event a student-athlete tests positive for the use of finasteride, the institution will then submit thefull record for a medical exception review.Hypogonadism – or tes<strong>to</strong>sterone deficiency, results either from a disorder of the testes (primaryhypogonadism) or of the hypothalamus or pituitary glands (secondary hypogonadism). Causes ofprimary hypogonadism include Klinefelter’s syndrome, undescended testicles, and hemochroma<strong>to</strong>sis.Secondary hypogonadism can be due <strong>to</strong> aging, increasing body mass index, and/or type 2 diabetesmellitus. Treatment for hypogonadism may include tes<strong>to</strong>sterone medication. Tes<strong>to</strong>sterone falls underthe banned drug class “anabolic agents”. A student-athlete must request approval <strong>to</strong> use medicationwith tes<strong>to</strong>sterone prior <strong>to</strong> participation while using this substance. A full medical documentation ofthe diagnosis, course of treatment and prescription his<strong>to</strong>ry must be provided by the institution prior <strong>to</strong>allowing the student-athlete <strong>to</strong> compete on this medication. If a student-athlete tests positive fortes<strong>to</strong>sterone and has not obtained prior approval <strong>to</strong> use this substance, the case must go <strong>to</strong> appeal.In all cases, if a student-athlete does not meet the criteria for a medical exception, the student-athletemay request an appeal hearing of his positive drug test. In this case, the student-athlete’s eligibility willbe suspended pending the outcome of the appeal. Questions about this policy may be directed <strong>to</strong> MaryWilfert, Associate Direc<strong>to</strong>r, Health and Safety, mwilfert@ncaa.org or 317-917-6319.The National Collegiate Athletic AssociationMarch 11, 2008MEW