download - World Vision's Nutrition Centre of Expertise
download - World Vision's Nutrition Centre of Expertise
download - World Vision's Nutrition Centre of Expertise
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
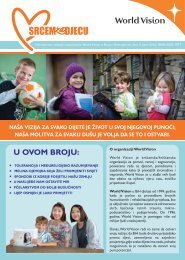
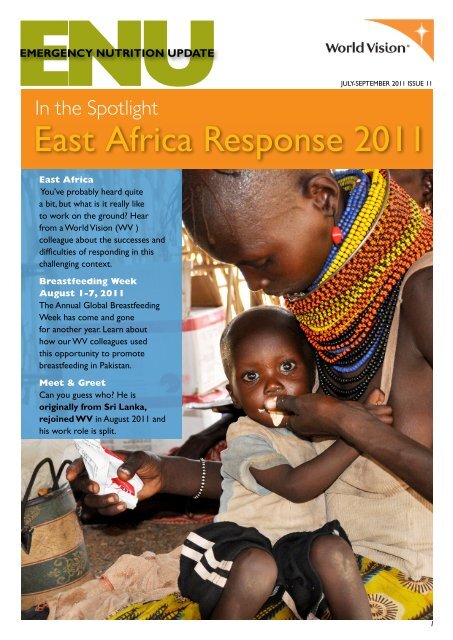
<strong>Nutrition</strong> Situation• As <strong>of</strong> 28 October 2011, 450,000 children inSomalia are acutely malnourished <strong>of</strong> whom190,000 suffer from severe acute malnutrition(SAM) (Source: UN Office for the Coordination<strong>of</strong> Humanitarian Affairs - OCHA). Ongoinginterventions supported by WV includeoperationalising outpatient therapeuticprogrammes (OTP) and stabilisation centers (SC)and targeted and blanket supplementary feedingprogrammes.Total Number <strong>of</strong> People affected• The UN estimates 13 million people across EastAfrica are currently affected by the drought. Fourmillion <strong>of</strong> these people are in Somalia where750,000 are at risk <strong>of</strong> death before the end <strong>of</strong> theyear.<strong>World</strong> Vision’s ResponseWV is responding across four countries to mitigatethe effects <strong>of</strong> the drought and famine:• Between 20-27 October, WV provided foodassistance to 82,495 people in Kenya, 28,513people in Ethiopia and 13,386 people in Tanzania.• Between February and November 2011, WVEthiopia’s CMAM OTP programme admittedand treated 6,812 children with SAM in theircommunities, with a recovery rate <strong>of</strong> 97%.• Between February and November 2011, WVSomalia’s CMAM OTP programme admittedand treated 2,254 children with SAM in theircommunities, with a recovery rate <strong>of</strong> 83%.• Somalia: water, sanitation and hygiene (WASH),non-food items (NFIs), child protection, shelter,health and nutrition, disaster risk reduction (DRR),livelihoods• Kenya: WASH, food distributions, supplementaryfeeding programme (SFP), outpatient therapeuticprogramme (OTP) stabilization centers (SC),blanket supplementary feeding programme, health• Ethiopia: WASH, livelihoods, food distributions, fuelefficient stoves, solar torches, education, health,therapeutic and supplementary feeding• Tanzania: food distributions, WASH, targetedsupplementary feeding, health, livelihoodsA Beneficiary’sExperienceKume Mohammed, a three year old girl from Ethiopia,is one <strong>of</strong> many children affected by the current droughtacross East Africa. Kume’s mother Bosie Kasim toldWV that she did not have enough food for her smallfamily, and that Kume, her second daughter, has beenmost affected by the food shortage. She was severelymalnourished with swollen feet, hands and face whenBosie took her to the WV Ethiopia supported villagehealth post where she was diagnosed with severe acutemalnutrition (SAM). Kume was treated with de-wormingtreatment, iron supplements, vitamins and antibiotics, andher mother was given sachets <strong>of</strong> ready to use therapeuticfoods (RUTF) to administer at home. A WV Ethiopiatrained community health worker visits Kume and hermother regularly to monitor her progress and is pleasedwith her recovery from SAM. WV’s support in training,essential drugs and therapeutic food has helped thehealth post where Kume was rehabilitated, along withother health posts in Shashemene ADP operational areas,to respond to the needs <strong>of</strong> malnourished children inpartnership with the district.Kume Mohammed (3) and Bosie Kasim, Kenya3
CMAM Africa UpdateCMAM Africa Update: Summary <strong>of</strong> FunctionalIndicators and Influencing Factors as <strong>of</strong> 28 Oct 2011Submitted by Cyprian Ouma – Africa CMAM Technical AdvisorCountryS. SudanKenyaEthiopiaSomaliaZimbabweNigerEDRCWDRCZambiaMauritaniaSierraLeoneProjectareas /ADP’scoveredProjectstatus(O=ongoing)FoodsecuritysituationTonj Sth,Tonj Nth,GogrialWestUp to end<strong>of</strong> 2011Very Poor- receivingfood aid9 21 1 6 17 2 9 2 5 2Up to end<strong>of</strong> 2011Very poor– nationaldisasterOPoor –need foodaidClosed insome parts.PuntlandopenedVery poor– receivingfood aidGwandaphasedout.RushingaandLupanestillongoingPoor –receivingfood aidin someareas buteconomystabilising0In responseto SahelfaminePoor –receivingfood aidFundraisingfor MasisiandRwangubaPoor –receivingfood aidmainly dueto conflictOPoor –receivingfood aidmainly dueto conflictPhased out.Waitingfor fundsto dointegrationandcapacitybuildingPoor –receivingfood aidODataNotReceivedPoorODataNotReceivedPoorGeneralsecurityPoor -cattlerustlingand clanviolencePoor -cattlerustlingGenerallygoodVery poor Good ModeratePoor -sporadicrebelattacksGoodGenerallygoodGoodGoodAccess topopulationPoor dueto rainsModerateGoodPoordue toinsecurityGood Good Poor GoodGoodexceptduringrainsGoodGoodTotalnumber <strong>of</strong>sitesOTP=31SFP=31OTP=66SFP= 83OTP=61SFP=N/AOTP=39SFP=33OTP=20SFP=20OTP=33SFP=52OTP=17SFP=0OTP=37SFP=0OTP=16SFP=16OTP=22SFP=305NumberadmittedsinceprogrammesetupOTP=618SFP=7686OTP=2909 OTP=2304 OTP=633 OTP=385OTP=4127SFP=7622OTP=2808OTP=3484SFP=16688OTP=587SFP=969OTP=NADUNumbertrained inCMAMCV=98MOH=10WV=44CV=112MOH=36WV=82CV=560MOH=173WV=14CV=592MOH=11WV=37CV=210MOH=23WV=4CV=1329MOH=282WV=16CV=333MOH=14WV=6CV=89MOH=53WV=11CV=1208MOH=36WV=12DUDURecovered 85% >80% 93% 81.3% 70% 85 90% OTP 84% 67%Deaths inprogramme
Research and Global ParticipationGlobal<strong>Nutrition</strong>ClusterMeeting,New York,3 to 5October,2011The Inter-Agency Standing Committee (IASC) Global <strong>Nutrition</strong> Cluster (GNC) held itssixth face-to-face meeting in New York, USA between 3 and 5 October 2011, which wasattended by 41 persons from NGOs, UN agencies, universities and technical and researchgroups. Mesfin Teklu attended the meeting on behalf <strong>of</strong> <strong>World</strong> Vision International.The meeting was opened by Louis George Arsenault (Deputy Director, EmergencyOperations, UNICEF) who provided members with an update on the key outcomes anddecisions resulting from the an internal UNICEF review <strong>of</strong> its cluster lead functions. Keyoutcomes included a decision to relocate a number <strong>of</strong> clusters, including the GNC, fromthe UNICEF Programme Division in New York to the Emergency Operation in Geneva, as<strong>of</strong> January 1, 2012. This move will ensure that all UNICEF led cluster coordination teamsare closer to decision-making and other mechanisms within the IASC, as well as providebetter support to the cluster countries and improve service delivery.A key theme <strong>of</strong> the meeting was defining the relationship between the GNC and otherclusters, as well as the relationship between the GNC and specific technical initiativesrelevant to emergency nutrition. During this meeting, representatives from the FoodSecurity Cluster (gFSC) and the Health Cluster were invited in order to draw outlinkages between those clusters and the GNC, in addition to sharing progress made todatein the respective clusters. In order to highlight practical ways in which coordinationcan be improved, the <strong>Nutrition</strong> Cluster response as well as intercluster and interagencycoordination around the Horn <strong>of</strong> Africa response was also an important focus <strong>of</strong> themeeting.One <strong>of</strong> the key objectives <strong>of</strong> the meeting was to present <strong>Nutrition</strong> Cluster achievementsas well as gaps since the last GNC meeting in March 2011, and then using this informationand other emerging priorities from the discussion to develop the working group workplans for the next 24 months. In order to highlight areas for incorporation <strong>of</strong> relevantsupport and engagement <strong>of</strong> partners into the GNC work plan, the meeting also providedan overview <strong>of</strong> a number <strong>of</strong> key technical initiatives in emergency nutrition.Please visit the Global <strong>Nutrition</strong> Cluster website for the full meeting report: http://oneresponse.info/GlobalClusters/<strong>Nutrition</strong>/Pages/Global%20Cluster%20Meetings.aspxWV Emergency <strong>Nutrition</strong> StaffMEETAntony PeterYears with WV: I worked with WV Lankaand WVI for nearly five years following theAsia Tsunami before moving to work for otherNGOs and the UN. I recently started back withWV in August 2011.Current position: Emergency <strong>Nutrition</strong>AssociateCurrent work location: I am based inCanada however can be deployed anywhere inthe world.Main work responsibilities/activities: Iwork 50% with the WV Global Rapid Response Team (GRRT) during which I am available fordeployment to major emergencies to provide support to National Offices in the midst <strong>of</strong> aresponse, and 50% with WV Canada supporting their ongoing nutrition programming.What you may not know about me: My passion for humanitarian work started duringmy school days when I was an internally displaced person (IDP) in my own country (SriLanka) and then a refugee for many years. These experiences motivated me to complete myMasters in Food and <strong>Nutrition</strong> and become a humanitarian worker.When you’re not working what do you enjoy doing?Spending time with my family who include my wife and two boys aged 5 years and 19 months.The NextENUIf you have anysuggestions, stories orreports which you thinkwould be helpful for ENUreaders, please email tokaitrin.both@worldvision.com.au by Tuesday,January 10, 2012. Ourtheme topic for Oct-Dec11 issue will focus onManagement <strong>of</strong> ModerateAcute Malnutrition(MAM).6
Tools, Guidelines and RecommendationsDo you knowabout the keyupdates to the<strong>World</strong> Visionpolicy governingthe procurementand use <strong>of</strong> milkproducts in fieldprogrammes?UPDATED!To ensure effective infant feeding practices and avoidance <strong>of</strong> harm to children, <strong>World</strong>Vision (WV) has set an internal policy regarding the procurement and use <strong>of</strong> milk and milkderived products in both emergency and non-emergency contexts. The 2007 version <strong>of</strong>WV’s Milk Policy was recently updated to include the recommendations in the <strong>World</strong> HealthOrganization’s 2010 Guidelines on HIV and Infant Feeding.The policy emphasises that WV protects, promotes and supports breastfeeding and safeand appropriate infant and young child feeding practices and upholds the provisions <strong>of</strong> theInternational Code <strong>of</strong> Marketing <strong>of</strong> Breast Milk Substitutes. It also includes clear guidelinesregarding the distribution <strong>of</strong> breast milk substitutes. WV will not accept unsolicited donations<strong>of</strong> breast milk substitute and milk products. WV will not accept donations <strong>of</strong> liquid or semiliquidmilk, including evaporated, condensed and Ultra High Temperature milk, and will notaccept or supply bottles and teats (nipples). WV will accept, source and distribute driedmilk products only if they can be used under strict control in hygienic conditions either foron-the-spot consumption in a strictly supervised environment, such as therapeutic feedingprogrammes and wet supplementary feeding programmes or pre-mixed centrally with cerealflour, sugar and oil to produce a dry take-away premix for cooking at household level. Driedmilk should not be distributed as a single commodity or in general food rations.In an HIV specific context, <strong>World</strong> Vision supportsthe WHO 2010 guidelines on HIV and Infant Feeding.WVMilkPolicySubmitted by Magalie Nelson,WVI Emergency <strong>Nutrition</strong>Technical Specialist, NCOEWhere HIV status <strong>of</strong> mother is positive:The country infant feeding strategy should be followed, based on WHO Guidelines (eitherbreastfeeding plus anti-retroviral (ARV) prophylaxis or totally avoid breastfeeding). The secondoption (totally avoid breastfeeding) is only recommended when all <strong>of</strong> the following criteria aremet:• access to safe water and sanitation and• sufficient infant formula milk is provided to support normal growth and development and• infant formula can be prepared cleanly and frequently enough to be safe and• for the first six months, infant is exclusively formula fed and• family is supportive <strong>of</strong> this practice and• access to health care that <strong>of</strong>fers comprehensive child health services.If conditions needed to safely formula feed are not met and mothers are HIV positive, thentheir infants should be breastfed (whether or not the mothers are accessing ARVs) forgreatest chances <strong>of</strong> survival.Note:In the majority <strong>of</strong> countries in which WV works, these criteria cannot be met bymost families and therefore exclusive breastfeeding for the first six months <strong>of</strong> life andcontinued breastfeeding with appropriate complementary feeding until environmental,economic and social circumstances are safe for and supportive <strong>of</strong> replacement feedingis strongly recommended.When HIV status <strong>of</strong> mother is unknown or known to be HIV-negative:WV encourages and supports the mother to exclusively breastfeed her infant for the first sixmonths <strong>of</strong> life, and continue breastfeeding for two years or beyond, with timely and correctuse <strong>of</strong> adequate and appropriate complementary foods starting at six months <strong>of</strong> age.Global Health & WASH<strong>Nutrition</strong> <strong>Centre</strong> <strong>of</strong> <strong>Expertise</strong>The complete policy is available on wvcentral: https://www.wvcentral.org/cop/hnh/Documents/WVMilkPolicy2011.pdfFor questions or contributions to the WV ENU,please contact the WV <strong>Nutrition</strong> <strong>Centre</strong> <strong>of</strong> <strong>Expertise</strong>nutrition_coe@wvi.orgNCOE is hosted by WVCanada.7