

Paediatric Surgery: A Comprehensive Text For Africa ... - Global HELP
Paediatric Surgery: A Comprehensive Text For Africa ... - Global HELP
Paediatric Surgery: A Comprehensive Text For Africa ... - Global HELP

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
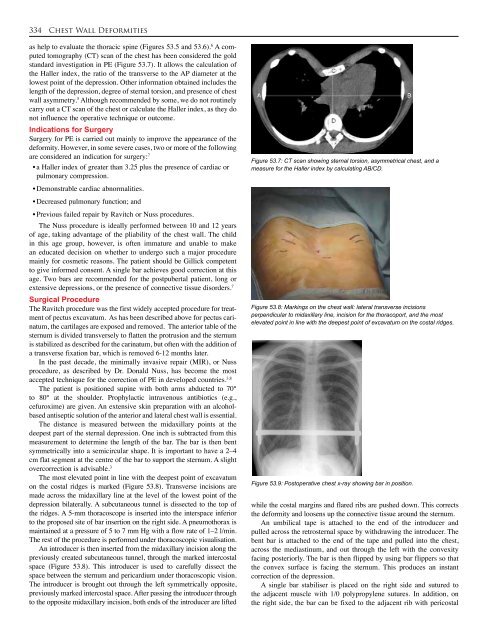
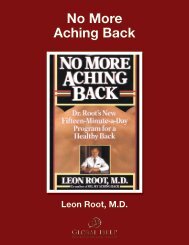
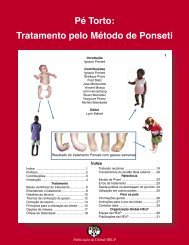
334 Chest Wall Deformitiesas help to evaluate the thoracic spine (Figures 53.5 and 53.6). 6 A computedtomography (CT) scan of the chest has been considered the goldstandard investigation in PE (Figure 53.7). It allows the calculation ofthe Haller index, the ratio of the transverse to the AP diameter at thelowest point of the depression. Other information obtained includes thelength of the depression, degree of sternal torsion, and presence of chestwall asymmetry. 5 Although recommended by some, we do not routinelycarry out a CT scan of the chest or calculate the Haller index, as they donot influence the operative technique or outcome.Indications for <strong>Surgery</strong><strong>Surgery</strong> for PE is carried out mainly to improve the appearance of thedeformity. However, in some severe cases, two or more of the followingare considered an indication for surgery: 7• a Haller index of greater than 3.25 plus the presence of cardiac orpulmonary compression.• Demonstrable cardiac abnormalities.• Decreased pulmonary function; and• Previous failed repair by Ravitch or Nuss procedures.The Nuss procedure is ideally performed between 10 and 12 yearsof age, taking advantage of the pliability of the chest wall. The childin this age group, however, is often immature and unable to makean educated decision on whether to undergo such a major proceduremainly for cosmetic reasons. The patient should be Gillick competentto give informed consent. A single bar achieves good correction at thisage. Two bars are recommended for the postpubertal patient, long orextensive depressions, or the presence of connective tissue disorders. 7Surgical ProcedureThe Ravitch procedure was the first widely accepted procedure for treatmentof pectus excavatum. As has been described above for pectus carinatum,the cartilages are exposed and removed. The anterior table of thesternum is divided transversely to flatten the protrusion and the sternumis stabilized as described for the carinatum, but often with the addition ofa transverse fixation bar, which is removed 6-12 months later.In the past decade, the minimally invasive repair (MIR), or Nussprocedure, as described by Dr. Donald Nuss, has become the mostaccepted technique for the correction of PE in developed countries. 3,8The patient is positioned supine with both arms abducted to 70°to 80° at the shoulder. Prophylactic intravenous antibiotics (e.g.,cefuroxime) are given. An extensive skin preparation with an alcoholbasedantiseptic solution of the anterior and lateral chest wall is essential.The distance is measured between the midaxillary points at thedeepest part of the sternal depression. One inch is subtracted from thismeasurement to determine the length of the bar. The bar is then bentsymmetrically into a semicircular shape. It is important to have a 2–4cm flat segment at the centre of the bar to support the sternum. A slightovercorrection is advisable. 3The most elevated point in line with the deepest point of excavatumon the costal ridges is marked (Figure 53.8). Transverse incisions aremade across the midaxillary line at the level of the lowest point of thedepression bilaterally. A subcutaneous tunnel is dissected to the top ofthe ridges. A 5-mm thoracoscope is inserted into the interspace inferiorto the proposed site of bar insertion on the right side. A pneumothorax ismaintained at a pressure of 5 to 7 mm Hg with a flow rate of 1–2 l/min.The rest of the procedure is performed under thoracoscopic visualisation.An introducer is then inserted from the midaxillary incision along thepreviously created subcutaneous tunnel, through the marked intercostalspace (Figure 53.8). This introducer is used to carefully dissect thespace between the sternum and pericardium under thoracoscopic vision.The introducer is brought out through the left symmetrically opposite,previously marked intercostal space. After passing the introducer throughto the opposite midaxillary incision, both ends of the introducer are liftedFigure 53.7: CT scan showing sternal torsion, asymmetrical chest, and ameasure for the Haller index by calculating AB/CD.Figure 53.8: Markings on the chest wall: lateral transverse incisionsperpendicular to midaxillary line, incision for the thoracoport, and the mostelevated point in line with the deepest point of excavatum on the costal ridges.Figure 53.9: Postoperative chest x-ray showing bar in position.while the costal margins and flared ribs are pushed down. This correctsthe deformity and loosens up the connective tissue around the sternum.An umbilical tape is attached to the end of the introducer andpulled across the retrosternal space by withdrawing the introducer. Thebent bar is attached to the end of the tape and pulled into the chest,across the mediastinum, and out through the left with the convexityfacing posteriorly. The bar is then flipped by using bar flippers so thatthe convex surface is facing the sternum. This produces an instantcorrection of the depression.A single bar stabiliser is placed on the right side and sutured tothe adjacent muscle with 1/0 polypropylene sutures. In addition, onthe right side, the bar can be fixed to the adjacent rib with pericostal
![Clubfoot: Ponseti Management [Vietnamese] - Global HELP](https://img.yumpu.com/51276842/1/184x260/clubfoot-ponseti-management-vietnamese-global-help.jpg?quality=85)



![Steenbeek Brace For Clubfoot [2nd Edition] - Global HELP](https://img.yumpu.com/46612972/1/190x245/steenbeek-brace-for-clubfoot-2nd-edition-global-help.jpg?quality=85)


![Basics Of Wound Care [Indonesia] - Global HELP](https://img.yumpu.com/41566370/1/190x245/basics-of-wound-care-indonesia-global-help.jpg?quality=85)
