Therapeutic Guidelines for Atopic Dermatitis 2002 - Allergology ...
Therapeutic Guidelines for Atopic Dermatitis 2002 - Allergology ...
Therapeutic Guidelines for Atopic Dermatitis 2002 - Allergology ...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
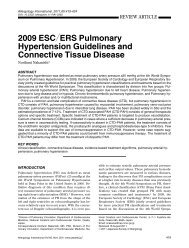
<strong>Allergology</strong> International. 2005;54:45-49REVIEW ARTICLE<strong>Therapeutic</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Atopic</strong><strong>Dermatitis</strong> <strong>2002</strong>Masutaka Furue 1 ,YoichiKohno 2 , Shoso Yamamoto 3 on behalf of The Research Group <strong>for</strong> <strong>Therapeutic</strong>Guideline Construction on <strong>Atopic</strong> <strong>Dermatitis</strong>: Toshiyuki Aoki, Kazuo Akiyama, Shuhei Imayama,Akira Ozawa, Takanobu Kurashige, Osamu Koro, Tuyoshi Sakane, Naoki Shimojo, Yoichi Tanaka,Kunihiko Tamaki, Shinpei Torii, Hidemi Nakagawa, Hideo Nakayama, Sankei Nishima,Fukumi Furukawa, Mitsufumi Mayumi, Masako Mizoguchi, Eishin Morita, Naomi Yamashita andKazuya YamamotoABSTRACTWe summarized the <strong>Therapeutic</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Atopic</strong> <strong>Dermatitis</strong> <strong>2002</strong>, and outlined important points with referenceto medical care and management of atopic dermatitis.KEY WORDSanti−histamine, atopic dermatitis, steroid, tacrolimus, therapeutic guidelinesINTRODUCTIONThe <strong>Therapeutic</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Atopic</strong> <strong>Dermatitis</strong>1999 were first announced by the Research Group <strong>for</strong><strong>Therapeutic</strong> Guideline Construction on <strong>Atopic</strong> <strong>Dermatitis</strong>(Director : Shoso Yamamoto), which was supportedby the Japanese Ministry of Health, Labourand Welfare. These guidelines were further updatedin 2001 and <strong>2002</strong>. They target general physicians .The structure of these guidelines corresponds withthat of the treatment guidelines proposed by the JapaneseDermatological Association, which are aimed atdermatologists ( http : web . kanazawa-u . ac . jp med24atopytherapy.html). The classification of thepotency of topical steroids was unified in both guidelinesAlthough analysis of the pathogenesis and relatedgenes <strong>for</strong> atopic dermatitis ( AD) is currently progressing,this work has not yet elucidated the fundamentalcause of AD. AD is a common, chronic orchronically relapsing, severely pruritic, eczematousskin disease. There<strong>for</strong>e, the patient’s discom<strong>for</strong>t islargely similar to that in other intractable skin diseases.In order to achieve good communication withpatients, it is important <strong>for</strong> physicians to carefully listento how patients describe their discom<strong>for</strong>t, sometimesover a period of many hours. It is also a prerequisiteto help patients understand that the medicationcurrently prescribed is a disease-adapted treatment,although very useful to control disease activity,and to understand that the majority of patients experiencespontaneous regression during follow-upDIAGNOSISThe symptoms of AD chronically fluctuate with remissionsand relapses, and many patients have atopicdiathesis. The Japanese Dermatological Associationhas established criteria <strong>for</strong> the diagnosis of AD (Table1). 1PRINCIPLES FOR THERAPYIt is important to treat each patient by appropriatelycombining the following three fundamental principles: (1) elucidation and avoidance of trigger and aggravatingfactors, (2) skin care, and (3) medication( Fig . 1). In<strong>for</strong>mation about medical treatmentsshould be explained fully to the patient to create agood doctor-patient partnershipGLOBAL CLINICAL SEVERITYIt is necessary to evaluate the global clinical severityin order to select a suitable treatment. Although sev-1Department of Dermatology, Graduate School of Medical Sciences,Kyushu University, Fukuoka, 2 Department of Pediatrics,Graduate School of Medicine, Chiba University, Chiba and 3 Departmentof Dermatology, Hiroshima University, Hiroshima, Japan.Correspondence: Masutaka Furue, Department of Dermatology,Kyushu University, 3 − 1 − 1 Maidashi Higashiku, Fukuoka 812 −8582, Japan.Email: furue@dermatol.med.kyushu−u.ac.jpReceived 19 January 2004.2005 Japanese Society of <strong>Allergology</strong><strong>Allergology</strong> International Vol 54, No1, 2005 www.js-allergol.gr.jp 45
Furue M et al.Table1 DefinitionandDiagnosticCriteria<strong>for</strong><strong>Atopic</strong><strong>Dermatitis</strong>byTheJapaneseDermatologicalAssociationDefinition<strong>Atopic</strong>dermatitisisapruritic,eczematousdermatosis,thesymptomsofwhichchronicalyfluctuatewithremissionsandrelapses.Mostindividualswithatopicdermatitishaveatopicdiathesis.<strong>Atopic</strong>diathesis:(1)personalorfamilyhistory(asthma,alergicrhinitisand/orconjunctivitis,andatopicdermatitis),and/or(2)predispositiontooverproductionofimmunoglobulinE(IgE)antibodies.Diagnosis1.Pruritus2.Typicalmorphologyanddistribution:(1)Eczematousdermatitis・Acute lesions: erythema, exudation, papules,vesiculopapules,scalesandcrusts・Chroniclesions:infiltratederythema,lichenification,prurigo,scalesandcrusts(2)Distribution・SymmetricalPredilection sites:<strong>for</strong>ehead,periorbitalarea,perioralarea,lips,periauriculararea,neck,jointareasoflimbs,trunk・Age-relatedcharacteristicsInfantilephase:startsonthescalpandface,oftenspreadstothetrunkandextremitiesChildhoodphase:neck,theflexuralsurfacesofthearmsandlegsAdolescentandadultphase:tendencytobesevereontheupperhalfofthebody(face,neck,anteriorchest,andback)3.Chronicorchronicalyrelapsingcourse(usualycoexistenceofoldandnewlesions):MorethantwomonthsininfancyMorethansixmonthsinchildhood,adolescence,andadulthoodDefinitediagnosisofatopicdermatitisrequiresthepresenceofalthreefeatureswithoutanyconsiderationofseverity.Othercasesshouldbeevaluatedonthebasisoftheclinicalcoursewiththetentativediagnosisofacuteorchronic,nonspecificeczema.DiferentialDiagnosis・Contactdermatitis・Seborheicdermatitis・Prurigosimplex・Scabies・Miliaria・Ichthyosis・Xeroticeczema・Handdermatitis(non-atopic)DiagnosticAids・Familyhistory(bronchialasthma,allergicrhinitisand/orconjunctivitis,atopicdermatitis)・Complications(bronchialasthma,alergicrhinitisand/orconjunctivitis)・Folicularpapules(goose-skin)・Elevatedserum IgElevelClinicalTypes(notapplicabletotheinfantilephase)・Flexuralsurfacetype・Extensorsurfacetype・Dry<strong>for</strong>m inchildhood・Head/face/neck/upperchest/backtype・Prurigotype・Erythrodermatype・CombinationsofvarioustypesarecommonSignificantComplications・Ocular complications (cataracts and/or retinaldetachment):especialyinpatientswithseverefaciallesions・Kaposi’svariceli<strong>for</strong>m eruption・Moluscum contagiosum・Impetigocontagiosaeral scoring systems have been reported <strong>for</strong> theevaluation of the severity of AD, we herein propose asimple method considering the affected body surfaceareas in order to make it convenient <strong>for</strong> general physiciansto use (Table 2).TRIGGER AND AGGRAVATING FACTORSBecause trigger and aggravating factors vary amongpatients (Fig. 2), it is necessary to know an individualpatient’s trigger and aggravating factors be<strong>for</strong>e recommendingavoidance of any of the known trigger oraggravating factors <strong>for</strong> AD.SKIN CAREPatients with AD have several functional abnormalitiesof the skin, such as decreased ability of moisture46 <strong>Allergology</strong> International Vol 54, No1, 2005 www.js-allergol.gr.jp
<strong>Therapeutic</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Atopic</strong> <strong>Dermatitis</strong> <strong>2002</strong>DiagnosisEvaluation of SeverityEducation and Avoidance ofTrigger and Aggravating FactorsSkin Care(compensation <strong>for</strong> the functionalabnormalities of the skin)MedicationsFig.1 Principles<strong>for</strong>therapyInfantile(less than 2 years old)Childhood(2 to 12 years old)Adolescence and Adult(13 years old and older)FoodsSweatingEnvironmental factorsBacteria, fungietceteraEnvironmental factorsSweatingBacteria, fungiContact allergensStressFoodsetceteraBecause the trigger and aggravating factors vary among patients, it is important to carefullyelucidate the trigger and aggravating factors be<strong>for</strong>e recommending their avoidance.Fig.2 TriggerandAggravatingFactorsTable2 GlobalClinicalSeverityMildModerateSevereVerySevere:Beingcoveredwithmildskinlesions*only,irespectiveofbodysurfaceareaafected:Inflamed skin lesions*covering lessthan10% ofthebodysurface:Inflamed skin lesions covering morethan 10% butless than 30% ofthebodysurface:Inflamed skin lesions covering morethan30% ofthebodysurface*Mildskinlesions:Dryskin,scalingandfainterythema.*Inflamed skin lesions:Lesionswith erythema,papules,erosion,infiltration,lichenification,andsoon.maintenance, decreased threshold of itch sensationand tendencies toward bacterial and viral infections.It is known that these abnormalities are strongly relatedto the development of symptoms and aggravationof dermatitis. Suitable skin care is there<strong>for</strong>e requiredto compensate <strong>for</strong> these abnormalities (Table3).MEDICATIONSuitable medication is required to control cutaneousinflammation . Topical steroids and oral antihistamineanti-allergic drugs are the mainstay oftreatment of AD. Figure 3 shows fundamental topicalsteroid therapy according to severity grading in patientsless than 2 years old, 2 to 12 years old, and 13years old or older. Table 4 shows a classification ofthe potency of topical steroids. The following pointsare important <strong>for</strong> drug treatment. We must select thepotency and vehicle <strong>for</strong>mulation of topical steroids accordingto the patient’s age and distribution andmanifestation of each eruption. We recommend thatgeneral physicians prescribe topical steroids of lowerpotency and smaller volume and <strong>for</strong> as short a periodof time as possible <strong>for</strong> facial lesions to reduce the occurrenceof adverse effects. The adverse effects oftopical steroids, such as teleangiectasia and skin atrophy,occur more frequently with longer periods of application.Physicians must monitor the potency anddosage of topical steroids <strong>for</strong> their patients. 2 If a patientsuddenly stops the application of topical steroids,the eruptions may exacerbate rapidly . Physiciansshould ask their patients to tell them when they<strong>Allergology</strong> International Vol 54, No1, 2005 www.js-allergol.gr.jp 47
<strong>Therapeutic</strong> <strong>Guidelines</strong> <strong>for</strong> <strong>Atopic</strong> <strong>Dermatitis</strong> <strong>2002</strong>Table4 PotencyoftopicalsteroidsStrongest0.05% clobetasolpropionate05% diflorasonediacetateVerystrong0.1% mometasonefuroate0.05% betamethasonebutyratepropionate0.05% fluocinonide0.064% betamethasonedipropionate0.05% difluprednate0.05% budesonide0.1% amcinonide0.1% diflucortolonevalerate1% hydrocortisonebutyratepropionateStrong0.3% deprodonepropionate0.1% dexamethasonepropionate0.12% dexamethasonevalerate0.1% halcinonide0.12% betamethasonevalerate0.025% beclomethasonedipropionate025% fluocinoloneacetonideMild0.3% prednisolonevalerateacetate0.1% triamcinoloneacetonide0.02% flumetasonepivalate0.1% alclometasonedipropionate0.05% clobetasonebutyrate0.1% hydrocortisonebutyrate1% dexamethasoneWeak0.5% prednisolone1% hydrocortisoneacetatemodulatory drug or calcineurin inhibitor) is effective,in particular <strong>for</strong> facial lesions. Treatment guidelines<strong>for</strong> use of topical tacrolimus can be found elsewhere. 3CHECKPOINTS DURING FOLLOW-UPOver long periods of follow-up, physicians must beaware of the possibility of various complications andmanage them appropriately. AD is frequently associatedwith impetigo contagiosum, Kaposi’s varicelli<strong>for</strong>meruption and molluscum contagiosum. Thesecomplications require early diagnosis and appropriatetreatment. AD is also frequently associated with ophthalmicdisorders such as cataract and retinal detachment. Repeated rubbing and patting of the orbitalarea may be responsible <strong>for</strong> the exacerbation of ophthalmiclesions. Special attention should be paid tothe occurrence of contact dermatitis due to topicalointments, because the contact dermatitis aggravatesthe severity of lesions. These guidelines only outlinethe general points of therapeutic management of AD,and there<strong>for</strong>e, many additional factors must be consideredin individual cases. Physicians have to considerreferring the patients to experts and specialclinics, if good control is not achieved after 1 monthof treatment according to these guidelinesREFERENCES1. Japanese Dermatological Association criteria <strong>for</strong> the diagnosisof atopic dermatitis. Jap. J. Dermatol. 1966;106:64-65.2. Furue M, Terao H, Rikihisa W et al. Clinical dose and adverseeffects of topical steroids in daily management ofatopic dermatitis. Br.J.Dermatol.2003;148:128-133.3. The Japanese FK 506 Ointment Study Group . Clinicalguidance <strong>for</strong> treatment of patients with atopic dermatitisby tacrolimus ointment 0.1% and 0.03%. Rinsho Hifuka2003;57:1217-1234 (in Japanese).<strong>Allergology</strong> International Vol 54, No1, 2005 www.js-allergol.gr.jp 49