Inhaler Physician & Parent Signature form - Lee's Summit R-7 ...
Inhaler Physician & Parent Signature form - Lee's Summit R-7 ...
Inhaler Physician & Parent Signature form - Lee's Summit R-7 ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
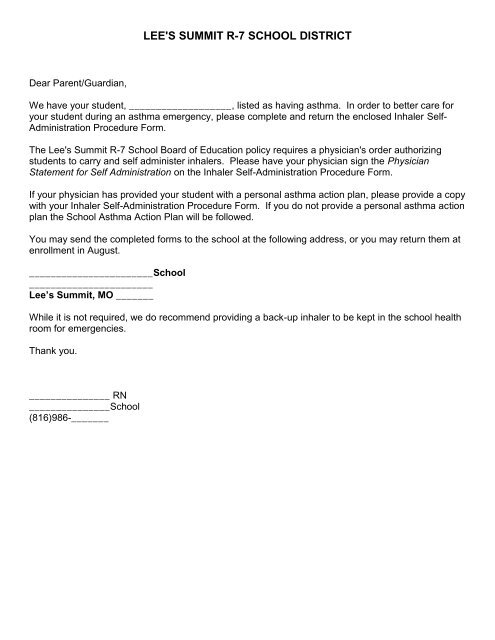
LEE'S SUMMIT R-7 SCHOOL DISTRICTDear <strong>Parent</strong>/Guardian,We have your student, ___________________, listed as having asthma. In order to better care foryour student during an asthma emergency, please complete and return the enclosed <strong>Inhaler</strong> Self-Administration Procedure Form.The <strong>Lee's</strong> <strong>Summit</strong> R-7 School Board of Education policy requires a physician's order authorizingstudents to carry and self administer inhalers. Please have your physician sign the <strong>Physician</strong>Statement for Self Administration on the <strong>Inhaler</strong> Self-Administration Procedure Form.If your physician has provided your student with a personal asthma action plan, please provide a copywith your <strong>Inhaler</strong> Self-Administration Procedure Form. If you do not provide a personal asthma actionplan the School Asthma Action Plan will be followed.You may send the completed <strong>form</strong>s to the school at the following address, or you may return them atenrollment in August._______________________School_______________________Lee’s <strong>Summit</strong>, MO _______While it is not required, we do recommend providing a back-up inhaler to be kept in the school healthroom for emergencies.Thank you._______________ RN_______________School(816)986-_______
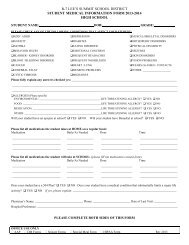
LEE’S SUMMIT R-7 SCHOOL DISTRICTINHALER SELF-ADMINISTRATION PROCEDURE FORMTHIS MEDICATION AUTHORIZATION IS ONLY VALID FOR THE CURRENT YEARStudent Name: ________________________________DOB:________________ School:___________________<strong>Parent</strong>/Guardian: _______________________________________Phone:_______________________________<strong>Physician</strong>: _____________________________________________Phone:________________________________Quick Relief Medications Albuterol inhaler 2 puffs every 4-6 hours as needed for cough/wheezing Albuterol inhaler 2 puffs 15-20 minutes before exercise if needed Other_____________________________________________________________________________________________________________________________________________________________________________________________ <strong>Physician</strong> has provided Personal Asthma Action Plan OR Student will follow School Asthma Action Plan Personal Best, if known: FEV1________________________ PEF_________________________________PHYSICIAN STATEMENT FOR STUDENT TO SELF-ADMINISTER: I certify that the above named student has amedical history of asthma, has been instructed in the proper self-administration of the medication(s) listed above and isjudged to be capable of carrying and self-administering the listed medication(s). The student should notify school staff ifone dose of medication fails to relieve their asthma symptoms in 20 minutes or sustain the student for at least 3 hours.This student understands the hazards of sharing medications with others and has agreed to refrain from this practice.<strong>Physician</strong> <strong>Signature</strong>: ____________________________________________Date:_______________PARENT/GUARDIAN STATEMENT FOR STUDENT TO SELF-ADMINISTER: I, the parent/guardian of theabove named student, give permission for this student to carry and self-administer the above listed medication(s). I haveinstructed my student to notify school staff if one dose of medication fails to relieve asthma symptoms in 20 minutes orsustain my student for at least 3 hours. I acknowledge that the school district and its employees or agents shall incur noliability as a result of any injury arising from the self-administration of medication by my student or the administration ofsuch medication by school staff.<strong>Parent</strong>/Guardian <strong>Signature</strong>: _______________________________________Date: _____________SCHOOL PLAN: School will follow Personal Asthma Action Plan if parents have provided one to the school. If no PersonalAsthma Action Plan has been provided, then the School Asthma Treatment Plan will be followed.Student has Personal Asthma Action Plan in file: yes noRESPONSIBILITIES FOR CARRYING INHALERS: (to be checked by the School Nurse)YES NO Student is able to identify signs and symptoms of asthma. Student agrees to come directly to the Health Room if one dose of medication fails torelieve asthma symptoms in 20 minutes or does not last at least 3 hours. Student provides a second inhaler to be kept in the health room. (This is recommendedbut not required)School Nurse <strong>Signature</strong>: _______________________________________________________________
SCHOOL ASTHMA ACTION PLANSchool Year 2012-2013Name: __________________________ Grade:______________ DOB: ______________Medications at school:Has Personal Asthma Action Plan on file: □ Yes □ No Follow personal asthma action plan if availableEvaluate respiratory status for signs of respiratory distress:● Severe coughing● Blueness of fingernails or lips● Wheezing● Decreased or loss of consciousness● Chest tightness● Shortness of breath● Rapid, labored breathing● Retractions (chest/neck sucks in)● Sitting in a hunched position (tripod position)PLAN OF ACTION: Personal best or best predicted: FEV1__________ / PEF__________Green Zone: Doing Well: No cough, wheeze, chest tightness, or shortness of breath; can do usual activities; O2 sat95%-100%; FEV1 ≥ 80% of personal best or best predicted OR Peak flow ≥80%of personal best. (Green zoneFEV1________ / PEF________)1. Have student rest in the health room for 10-20 min & observe for signs that condition may be worsening.2. May give student sips of warm water.3. Student may return to class.Yellow Zone: Moderate Distress: Cough, wheeze, chest tightness, or shortness of breath; Can do some, but not all,usual activities; O2 sat 91%-94%; FEV1 60-79% of personal best or best predicted OR Peak flow 50-79% of personalbest. (Yellow zone FEV1________ /PEF________)1. Notify RN. RN to assess student (when on-site).2. Student may be given 2-6 puffs of Albuterol MDI via spacer or 1 vial Albuterol via nebulizer, per RN directive.3. Notify parent/guardian.4. Monitor student and recheck O2 sat and/or FEV1 or PEF 20 minutes after administering quick-relief medication.5. If student responds favorably (O2sat ≥95%; FEV1 or PEF ≥ 80%), student may return to class.6. If no response to treatment, or if condition worsens, student may repeat 2-6 puffs of Albuterol MDI via spacer per RNdirective & call 911.Red Zone: Severe Distress: Very short of breath, blueness of fingernails or lips, retractions; Quick-relief medicines havenot helped; O2sat ≤ 90; FEV1