Bernstein <strong>and</strong> BaxterFig. 5—55-year-oldman with atypicalhangman’s fracture.Transaxial CTangiography imageshows fracturesthrough bothtransverse foramina,with occlusion of rightvertebral artery.Fig. 6—21-yearoldwoman withanterior subluxation.Lateral cervicalspine radiographshows subtle signsof hyperflexion,including C6–7interspinous widening(arrow), uncoveringof facets, <strong>and</strong> slightanterior translation.Courtesy of Rybak L,NYU Langone MedicalCenter, New York, NY.limited to posterior ligament complex injury <strong>and</strong> is stable. Anteriorsubluxation reflects further hyperflexion with disruptionof the posterior longitudinal ligament <strong>and</strong> posterior disk annulus(middle of column of Denis), which leads to instability.The radiologic evaluation of hyperflexion sprain <strong>and</strong> anteriorsubluxation can be challenging. Radiographic <strong>and</strong> CT signsare subtle; even when recognized, the significance may not beappreciated. However, it is important to underst<strong>and</strong> becausemissed injury can lead to significant morbidity, including pain,kyphosis, delayed vertebral dislocation, <strong>and</strong> neurologic deficit.Appearance on Relevant ModalitiesImaging features of progressively severe hyperflexion injuriesinclude (from posterior to anterior) fanning of spinousprocesses or interspinous widening, uncovered facets, widenedposterior disk space, focal kyphosis, <strong>and</strong> anterior subluxation.Vertebral body compression fractures may seen with sufficienthyperflexion <strong>and</strong> axial loading.When CT findings are equivocal, MRI can detect edema ofthe cervical ligaments <strong>and</strong> soft tissues. Flexion <strong>and</strong> extensionradiographs should not be performed in the presence of musclespasm to avoid false-negative results.Differential Diagnosis<strong>Cervical</strong> straightening <strong>and</strong> reversal of the normal lordosis mayoccur in cervical muscle spasm <strong>and</strong> should be distinguished fromtrue anterior subluxation. Close attention to facet alignment onCT <strong>and</strong> posterior disk spacing are most helpful in this regard.Degenerative changes may be confused with traumaticsubluxation. In contrast to traumatic anterior subluxation, retrolisthesisis the usual consequence of cervical spondylosisbecause of normal cervical lordosis <strong>and</strong> posterior inclinationof the articular facets. Degenerated facet joints are most commonlynarrowed, with thinning of the bony facet from longtermwear. In traumatic subluxations, however, the facet jointsare often abnormally widened.Hyperextension-DislocationRelevant Mechanism, Anatomy, <strong>and</strong> CauseHyperextension cervical spine injuries range from the stablehyperextension sprain to the highly unstable hyperextensiondislocation.They are predominantly ligamentous disruptionsthat progress from anterior to posterior, beginning with the anteriorlongitudinal ligament <strong>and</strong> anterior annulus fibrosus <strong>and</strong>extending through the posterior annulus, posterior longitudinalligament, <strong>and</strong> ligamentum flavum. The hyperextensiondislocationinjury often results in major neurologic deficits,typically a central cord syndrome.Approximately 25% of cervical spine injuries are the resultof hyperextension forces, either associated with direct impact,or through a whiplash effect. Direct impact injuries are oftenassociated with frontal head or facial injuries. Conditions predisposingto injury include age older than 65 years, with increasedpropensity for falls <strong>and</strong> motor vehicle crashes, degenerativechanges, spinal canal stenosis, <strong>and</strong> osteopenia.Appearance on Relevant ModalitiesAlthough hyperextension-dislocation injuries are severe <strong>and</strong>unstable, imaging signs are often subtle. Extensive soft-tissueinjury <strong>and</strong> displacement occurs at the moment of trauma, butmuscular spasm <strong>and</strong> immobilization in a cervical collar canresult in an apparently normal spine examination.Hyperextension-dislocation injuries usually involve thelower cervical spine. Signs on lateral radiographs <strong>and</strong> sagittalCT reformations include mild anterior intervertebral disk spacewidening, anterior vertebral body avulsion fragments, <strong>and</strong> facetmalalignment (Fig. 7A). In the normal spine, facets should beparallel. With extension injuries, one may see V-shaped facetjoints that are wide anteriorly <strong>and</strong> tapered posteriorly.MRI reveals the extent of discoligamentous injury. T2-weighted images show ligamentous disruption, soft-tissueedema, disk protrusion, <strong>and</strong> spinal cord injuries (Fig. 7B).Differential DiagnosisLike the hyperflexion sprain <strong>and</strong> anterior subluxation, thehyperextension-dislocation may be overlooked <strong>and</strong> misinterpretedas normal on both radiographs <strong>and</strong> CT. Neurologic24 2012 ARRS Categorical Course
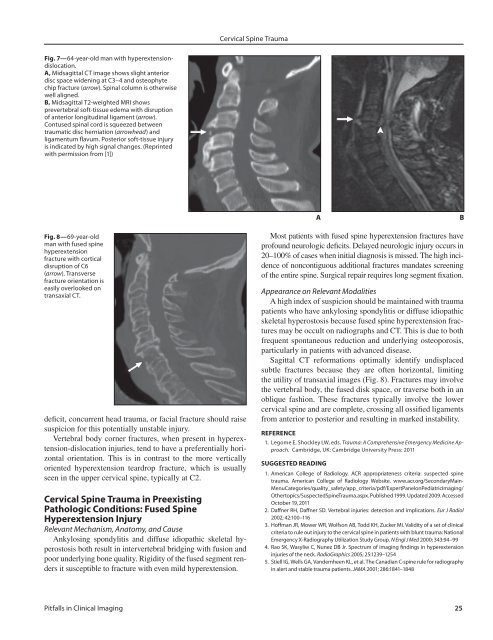
<strong>Cervical</strong> <strong>Spine</strong> <strong>Trauma</strong>Fig. 7—64-year-old man with hyperextensiondislocation.A, Midsagittal CT image shows slight anteriordisc space widening at C3–4 <strong>and</strong> osteophytechip fracture (arrow). Spinal column is otherwisewell aligned.B, Midsagittal T2-weighted MRI showsprevertebral soft-tissue edema with disruptionof anterior longitudinal ligament (arrow).Contused spinal cord is squeezed betweentraumatic disc herniation (arrowhead) <strong>and</strong>ligamentum flavum. Posterior soft-tissue injuryis indicated by high signal changes. (Reprintedwith permission from [1])ABFig. 8—69-year-oldman with fused spinehyperextensionfracture with corticaldisruption of C6(arrow). Transversefracture orientation iseasily overlooked ontransaxial CT.deficit, concurrent head trauma, or facial fracture should raisesuspicion for this potentially unstable injury.Vertebral body corner fractures, when present in hyperextension-dislocationinjuries, tend to have a preferentially horizontalorientation. This is in contrast to the more verticallyoriented hyperextension teardrop fracture, which is usuallyseen in the upper cervical spine, typically at C2.<strong>Cervical</strong> <strong>Spine</strong> <strong>Trauma</strong> in PreexistingPathologic Conditions: Fused <strong>Spine</strong>Hyperextension InjuryRelevant Mechanism, Anatomy, <strong>and</strong> CauseAnkylosing spondylitis <strong>and</strong> diffuse idiopathic skeletal hyperostosisboth result in intervertebral bridging with fusion <strong>and</strong>poor underlying bone quality. Rigidity of the fused segment rendersit susceptible to fracture with even mild hyperextension.Most patients with fused spine hyperextension fractures haveprofound neurologic deficits. Delayed neurologic injury occurs in20–100% of cases when initial diagnosis is missed. The high incidenceof noncontiguous additional fractures m<strong>and</strong>ates screeningof the entire spine. Surgical repair requires long segment fixation.Appearance on Relevant ModalitiesA high index of suspicion should be maintained with traumapatients who have ankylosing spondylitis or diffuse idiopathicskeletal hyperostosis because fused spine hyperextension fracturesmay be occult on radiographs <strong>and</strong> CT. This is due to bothfrequent spontaneous reduction <strong>and</strong> underlying osteoporosis,particularly in patients with advanced disease.Sagittal CT reformations optimally identify undisplacedsubtle fractures because they are often horizontal, limitingthe utility of transaxial images (Fig. 8). Fractures may involvethe vertebral body, the fused disk space, or traverse both in anoblique fashion. These fractures typically involve the lowercervical spine <strong>and</strong> are complete, crossing all ossified ligamentsfrom anterior to posterior <strong>and</strong> resulting in marked instability.REFERENCE1. Legome E, Shockley LW, eds. <strong>Trauma</strong>: A Comprehensive Emergency Medicine Approach.Cambridge, UK: Cambridge University Press: 2011SUGGESTED READING1. American College of Radiology. ACR appropriateness criteria: suspected spinetrauma. American College of Radiology Website. www.acr.org/SecondaryMain-MenuCategories/quality_safety/app_criteria/pdf/ExpertPanelonPediatricImaging/Othertopics/Suspected<strong>Spine</strong><strong>Trauma</strong>.aspx. Published 1999. Updated 2009. AccessedOctober 19, 20112. Daffner RH, Daffner SD. Vertebral injuries: detection <strong>and</strong> implications. Eur J Radiol2002; 42:100–1163. Hoffman JR, Mower WR, Wolfson AB, Todd KH, Zucker MI. Validity of a set of clinicalcriteria to rule out injury to the cervical spine in patients with blunt trauma: NationalEmergency X-Radiography Utilization Study Group. N Engl J Med 2000; 343:94–994. Rao SK, Wasyliw C, Nunez DB Jr. Spectrum of imaging findings in hyperextensioninjuries of the neck. RadioGraphics 2005; 25:1239–12545. Stiell IG, Wells GA, V<strong>and</strong>emheen KL, et al. The Canadian C-spine rule for radiographyin alert <strong>and</strong> stable trauma patients. JAMA 2001; 286:1841–1848<strong>Pitfalls</strong> in Clinical Imaging 25