

JUNE 11â14, 2013 - Mount Sinai Hospital
JUNE 11â14, 2013 - Mount Sinai Hospital
JUNE 11â14, 2013 - Mount Sinai Hospital
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
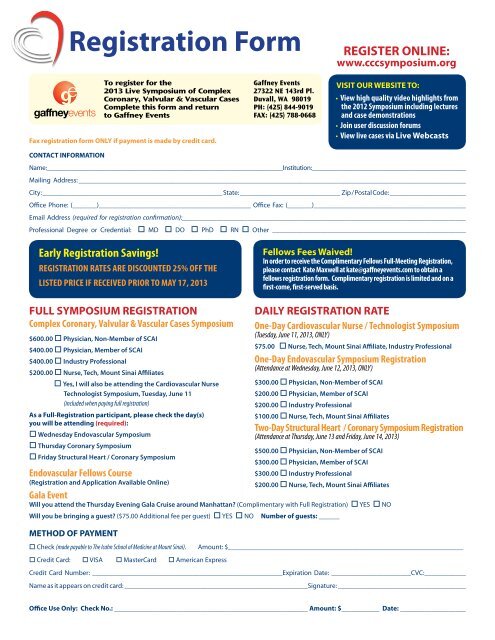
Registration FormREGISTER ONLINE:www.cccsymposium.orgTo register for the<strong>2013</strong> Live Symposium of ComplexCoronary, Valvular & Vascular CasesComplete this form and returnto Gaffney EventsFax registration form ONLY if payment is made by credit card.Gaffney Events27322 NE 143rd Pl.Duvall, WA 98019PH: (425) 844-9019FAX: (425) 788-0668VISIT OUR WEBSITE TO:• View high quality video highlights fromthe 2012 Symposium including lecturesand case demonstrations• Join user discussion forums• View live cases via Live WebcastsCONTACT INFORMATIONName:________________________________________________________________________Institution:_______________________________________________Mailing Address: ________________________________________________________________________________________________________________City: ____________________________________________________ State: _____________________________ Zip / Postal Code: ______________________Office Phone: (_______)____________________________________________ Office Fax: (_______)____________________________________________Email Address (required for registration confirmation):__________________________________________________________________________________Professional Degree or Credential: o MD o DO o PhD o RN o Other ________________________________________________________Early Registration Savings!REGISTRATION RATES ARE DISCOUNTED 25% OFF THELISTED PRICE IF RECEIVED PRIOR TO MAY 17, <strong>2013</strong>Fellows Fees Waived!In order to receive the Complimentary Fellows Full-Meeting Registration,please contact Kate Maxwell at kate@gaffneyevents.com to obtain afellows registration form. Complimentary registration is limited and on afirst-come, first-served basis.FULL SYMPOSIUM REGISTRATIONComplex Coronary, Valvular & Vascular Cases Symposium$600.00 o Physician, Non-Member of SCAI$400.00 o Physician, Member of SCAI$400.00 o Industry Professional$200.00 o Nurse, Tech, <strong>Mount</strong> <strong>Sinai</strong> Affiliateso Yes, I will also be attending the Cardiovascular NurseTechnologist Symposium, Tuesday, June 11(included when paying full registration)As a Full-Registration participant, please check the day(s)you will be attending (required):o Wednesday Endovascular Symposiumo Thursday Coronary Symposiumo Friday Structural Heart / Coronary SymposiumEndovascular Fellows Course(Registration and Application Available Online)Gala EventDAILY REGISTRATION RATEOne-Day Cardiovascular Nurse / Technologist Symposium(Tuesday, June 11, <strong>2013</strong>, ONLY)$75.00 o Nurse, Tech, <strong>Mount</strong> <strong>Sinai</strong> Affiliate, Industry ProfessionalOne-Day Endovascular Symposium Registration(Attendance at Wednesday, June 12, <strong>2013</strong>, ONLY)$300.00 o Physician, Non-Member of SCAI$200.00 o Physician, Member of SCAI$200.00 o Industry Professional$100.00 o Nurse, Tech, <strong>Mount</strong> <strong>Sinai</strong> AffiliatesTwo-Day Structural Heart / Coronary Symposium Registration(Attendance at Thursday, June 13 and Friday, June 14, <strong>2013</strong>)$500.00 o Physician, Non-Member of SCAI$300.00 o Physician, Member of SCAI$300.00 o Industry Professional$200.00 o Nurse, Tech, <strong>Mount</strong> <strong>Sinai</strong> AffiliatesWill you attend the Thursday Evening Gala Cruise around Manhattan? (Complimentary with Full Registration) o YES o NOWill you be bringing a guest? ($75.00 Additional fee per guest) o YES o NO Number of guests: ______METHOD OF PAYMENTo Check (made payable to The Icahn School of Medicine at <strong>Mount</strong> <strong>Sinai</strong>). Amount: $____________________________________________________________________o Credit Card: o VISA o MasterCard o American ExpressCredit Card Number: _______________________________________________________Expiration Date: _______________________CVC:____________Name as it appears on credit card: _____________________________________________________Signature: _____________________________________Office Use Only: Check No.: ________________________________________________________ Amount: $___________ Date: ___________________19
![December 2, 2012 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/51092274/1/190x245/december-2-2012-pdf-mount-sinai-hospital.jpg?quality=85)
![January 21, 2013 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/50916550/1/190x245/january-21-2013-pdf-mount-sinai-hospital.jpg?quality=85)
![February 3, 2013 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/50584982/1/190x245/february-3-2013-pdf-mount-sinai-hospital.jpg?quality=85)
![March 18, 2012 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/50462098/1/190x245/march-18-2012-pdf-mount-sinai-hospital.jpg?quality=85)


![Partners Program Guide [PDF] - Mount Sinai Hospital](https://img.yumpu.com/49411954/1/190x245/partners-program-guide-pdf-mount-sinai-hospital.jpg?quality=85)

![March 19 - April 1, 2012 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/48990923/1/190x245/march-19-april-1-2012-pdf-mount-sinai-hospital.jpg?quality=85)
![PGY-1 Residency Application [PDF] - Mount Sinai Hospital](https://img.yumpu.com/48577701/1/190x245/pgy-1-residency-application-pdf-mount-sinai-hospital.jpg?quality=85)

