

health questionnaire - Mount Sinai Hospital
health questionnaire - Mount Sinai Hospital
health questionnaire - Mount Sinai Hospital

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
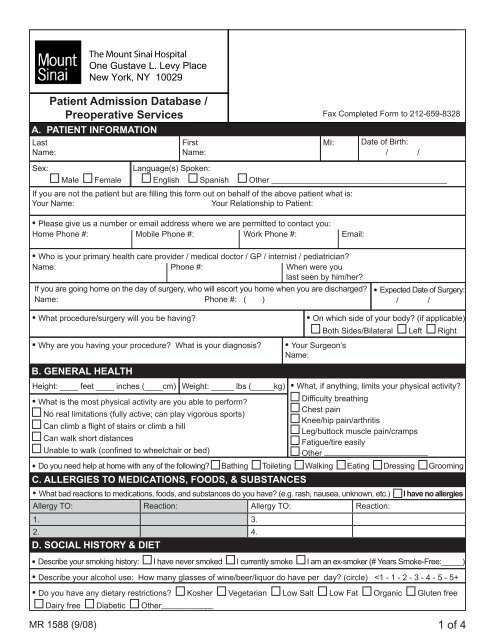
The <strong>Mount</strong> <strong>Sinai</strong> <strong>Hospital</strong>One Gustave L. Levy PlaceNew York, NY 0029LastName:Patient Admission Database /TITLEPreoperative ServicesA. PATIENT INFORMATIONFirstName:Fax Completed Form to 212-659-8328MI:Date of Birth:/ /Sex:MaleFemaleLanguage(s) Spoken:English Spanish Other _______________________________________If you are not the patient but are filling this form out on behalf of the above patient what is:Your Name:Your Relationship to Patient:• Please give us a number or email address where we are permitted to contact you:Home Phone #: Mobile Phone #: Work Phone #: Email:• Who is your primary <strong>health</strong> care provider / medical doctor / GP / internist / pediatrician?Name: Phone #: When were youlast seen by him/her?If you are going home on the day of surgery, who will escort you home when you are discharged?Name: Phone #: ( )• Expected Date of Surgery:/ /• What procedure/surgery will you be having?• Why are you having your procedure? What is your diagnosis?B. GENERAL HEALTHHeight: ____ feet ____ inches (____cm) Weight: _____ lbs (_____kg)• What is the most physical activity are you able to perform?No real limitations (fully active; can play vigorous sports)Can climb a flight of stairs or climb a hillCan walk short distancesUnable to walk (confined to wheelchair or bed)• On which side of your body? (if applicable)• Your Surgeon’sName:Both Sides/Bilateral Left Right• What, if anything, limits your physical activity?Difficulty breathingChest painKnee/hip pain/arthritisLeg/buttock muscle pain/crampsFatigue/tire easilyOther _______________________• Do you need help at home with any of the following? Bathing Toileting Walking Eating Dressing GroomingC. ALLERGIES TO MEDICATIONS, FOODS, & SUBSTANCES• What bad reactions to medications, foods, and substances do you have? (e.g. rash, nausea, unknown, etc.) I have no allergiesAllergy TO: Reaction: Allergy TO: Reaction:1. 3.2. 4.D. SOCIAL HISTORY & DIET• Describe your smoking history: I have never smoked I currently smoke I am an ex-smoker (# Years Smoke-Free:_____)• Describe your alcohol use: How many glasses of wine/beer/liquor do have per day? (circle)
E. SURGERY & ANESTHESIA HISTORY• Have you had any of the following types of surgery or procedures?I have never had surgeryHead/Neck: Brain Eyes Nose Tonsils Thyroid Throat Other ______________Chest: Heart Lungs Breast IV Catheter / Port Implant Esophagus Aorta Other____________Abdomen: Gall Bladder Appendix Colon Liver Stomach Kidney Pancreas Other_____________Pelvis: Hernia Uterus/Ovaries C-Section Bladder Prostate Other_______________Extremities: Knee Hip Shoulder Hand/Wrist Arteries/Veins Other_______________• Did you have any problems with the anesthesia for any of those surgeries?I have not had problems with anesthesiaNausea and/or Vomiting Muscle Aches Sore ThroatUncontrolled post-operative pain Damaged Teeth Eye PainAwareness or memories of surgery Back Pain HeadacheDifficulty having breathing tube inserted Long time to get back to “normal” Malignant hyperthermiaPseudocholinesterase deficiency Delirium/Confusion Other ______________• Do any blood relatives have problems with anesthesia that you are aware of? No Yes (please explain):F. DENTAL HISTORY• Do you have any of the following? Ihave no dental problemsLoose Teeth Bridges Temporomandibular Joint Disease (TMJ)Chipped Teeth Dentures Caps / VeneersG. GASTROINTESTINAL DISEASE HISTORY• Do you have a history of any of the following liver or intestinal problems? I have no liver or intestinal problemsAcid reflux (GERD) / heartburn GI bleeding / rectal bleeding Pancreatitis Cirrhosis of liverInflammatory bowel disease(Crohn’s disease, ulcerative colitis)Stomach / duodenal ulcer Esophageal varices / vomiting bloodIrritable bowel syndrome Stool incontinence Hiatal herniaProblems swallowing or digesting Diarrhea / Constipation Jaundice Gallstones• When was your last colonoscopy screening? ________________H. HEART DISEASE HISTORYWho is your cardiologist? (If applicable)Name: Phone #:• Do you have a history of any of the following heart or blood vessel problems?I have never had a colonoscopyWhen were youlast seen by him/her?I have no heart or blood vessel problemsHigh blood pressure / hypertension Heart failure (CHF)High cholesterol / HyperlipidemiaCongenital heart diseaseHeart attack / myocardial infarction (MI) (Approximate date:____________) Coronary artery blockagesHeart Surgery or Coronary Stents (Approximate date:______________) Blood clotsAbnormal heart rhythm / Implanted defibrillator (AICD) / Pacemaker Heart valve disease / Heart murmurAneurysm or peripheral vascular diseaseMR 1588 (9/08) of 4
M. BLOOD, INFECTIOUS & IMMUNE SYSTEM DISEASE HISTORY• Do you have a history of any of the following blood, infectious, or immune system problems?I have no blood, etc. problemsHepatitis B/C (HBV, HCV) HIV Anemia / low blood countsChicken Pox / Shingles Lupus(Have you ever received a blood transfusion? Yes No)Sickle cell disease / trait Scleroderma Thrombocytopenia / low plateletsFevers / Night sweats Eczema Hemophilia or other clotting disorder / easy bruising or bleedingUnintended weight loss Psoriasis Neutropenia / low white cells• Have you ever been placed on contact isolation orhad an antibiotic resistant infection? Yes NoN. GLAND DISEASE HISTORY• Have you had the following immunizations?Flu shot (date:________ )Pneumovax (date:_________)• Do you have a history of any of the following conditions?I have no gland problemsDiabetes Parathyroid disease Adrenal disease Carcinoid SyndromeHyperthyroidism Hypothyroidism Pituitary disease PheochromocytomaO. BONE, JOINT & SKIN DISEASE HISTORY• Do you have a history of any of the following bone, skin or joint problems?I have no bone, joint, or skin problemsBack pain / herniated disks / slipped disks Rheumatoid arthritis Chronic neck painOsteoarthritis / Degenerative Joint Disease Osteoporosis FibromylagiaScoliosis / Kyphosis / Spine abnormalities Ankylosing spondylitis KeloidsP. CANCER HISTORY• Have you ever had cancer? Yes NoIf you have had cancer, have you been treated with any ofIf yes, what type of cancer? _____________________ the following? Radiation Chemotherapy SurgeryQ. OTHER MEDICAL HISTORY• Please comment on any other relevant medical history not described above:The information provided is true to the best of my knowledge and I understand that it will be reviewed and modified foraccuracy as necessary by a member of the medical center staff.Name (Print) _______________________ Signature_________________________ Date/Time______________Fax Completed Form to 212-659-8328I have reviewed the information provided with the patient (or patient representative) and have verified, appended, and/or modified the informationfor accuracy as necessary.Reviewed By (Print)_________________________(RN) Signature___________________________________Date/Time_____________________MR 1588 (9/08) of 4
![December 2, 2012 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/51092274/1/190x245/december-2-2012-pdf-mount-sinai-hospital.jpg?quality=85)
![January 21, 2013 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/50916550/1/190x245/january-21-2013-pdf-mount-sinai-hospital.jpg?quality=85)
![February 3, 2013 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/50584982/1/190x245/february-3-2013-pdf-mount-sinai-hospital.jpg?quality=85)
![March 18, 2012 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/50462098/1/190x245/march-18-2012-pdf-mount-sinai-hospital.jpg?quality=85)


![Partners Program Guide [PDF] - Mount Sinai Hospital](https://img.yumpu.com/49411954/1/190x245/partners-program-guide-pdf-mount-sinai-hospital.jpg?quality=85)

![March 19 - April 1, 2012 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/48990923/1/190x245/march-19-april-1-2012-pdf-mount-sinai-hospital.jpg?quality=85)
![PGY-1 Residency Application [PDF] - Mount Sinai Hospital](https://img.yumpu.com/48577701/1/190x245/pgy-1-residency-application-pdf-mount-sinai-hospital.jpg?quality=85)


