

health questionnaire - Mount Sinai Hospital
health questionnaire - Mount Sinai Hospital
health questionnaire - Mount Sinai Hospital

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
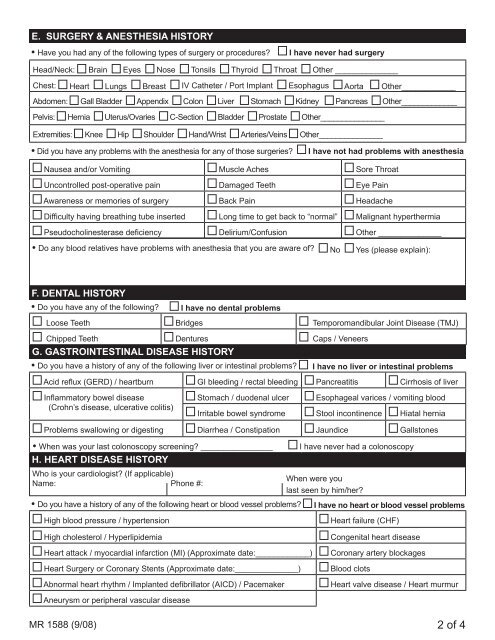
E. SURGERY & ANESTHESIA HISTORY• Have you had any of the following types of surgery or procedures?I have never had surgeryHead/Neck: Brain Eyes Nose Tonsils Thyroid Throat Other ______________Chest: Heart Lungs Breast IV Catheter / Port Implant Esophagus Aorta Other____________Abdomen: Gall Bladder Appendix Colon Liver Stomach Kidney Pancreas Other_____________Pelvis: Hernia Uterus/Ovaries C-Section Bladder Prostate Other_______________Extremities: Knee Hip Shoulder Hand/Wrist Arteries/Veins Other_______________• Did you have any problems with the anesthesia for any of those surgeries?I have not had problems with anesthesiaNausea and/or Vomiting Muscle Aches Sore ThroatUncontrolled post-operative pain Damaged Teeth Eye PainAwareness or memories of surgery Back Pain HeadacheDifficulty having breathing tube inserted Long time to get back to “normal” Malignant hyperthermiaPseudocholinesterase deficiency Delirium/Confusion Other ______________• Do any blood relatives have problems with anesthesia that you are aware of? No Yes (please explain):F. DENTAL HISTORY• Do you have any of the following? Ihave no dental problemsLoose Teeth Bridges Temporomandibular Joint Disease (TMJ)Chipped Teeth Dentures Caps / VeneersG. GASTROINTESTINAL DISEASE HISTORY• Do you have a history of any of the following liver or intestinal problems? I have no liver or intestinal problemsAcid reflux (GERD) / heartburn GI bleeding / rectal bleeding Pancreatitis Cirrhosis of liverInflammatory bowel disease(Crohn’s disease, ulcerative colitis)Stomach / duodenal ulcer Esophageal varices / vomiting bloodIrritable bowel syndrome Stool incontinence Hiatal herniaProblems swallowing or digesting Diarrhea / Constipation Jaundice Gallstones• When was your last colonoscopy screening? ________________H. HEART DISEASE HISTORYWho is your cardiologist? (If applicable)Name: Phone #:• Do you have a history of any of the following heart or blood vessel problems?I have never had a colonoscopyWhen were youlast seen by him/her?I have no heart or blood vessel problemsHigh blood pressure / hypertension Heart failure (CHF)High cholesterol / HyperlipidemiaCongenital heart diseaseHeart attack / myocardial infarction (MI) (Approximate date:____________) Coronary artery blockagesHeart Surgery or Coronary Stents (Approximate date:______________) Blood clotsAbnormal heart rhythm / Implanted defibrillator (AICD) / Pacemaker Heart valve disease / Heart murmurAneurysm or peripheral vascular diseaseMR 1588 (9/08) of 4
![December 2, 2012 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/51092274/1/190x245/december-2-2012-pdf-mount-sinai-hospital.jpg?quality=85)
![January 21, 2013 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/50916550/1/190x245/january-21-2013-pdf-mount-sinai-hospital.jpg?quality=85)
![February 3, 2013 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/50584982/1/190x245/february-3-2013-pdf-mount-sinai-hospital.jpg?quality=85)
![March 18, 2012 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/50462098/1/190x245/march-18-2012-pdf-mount-sinai-hospital.jpg?quality=85)


![Partners Program Guide [PDF] - Mount Sinai Hospital](https://img.yumpu.com/49411954/1/190x245/partners-program-guide-pdf-mount-sinai-hospital.jpg?quality=85)

![March 19 - April 1, 2012 [PDF] - Mount Sinai Hospital](https://img.yumpu.com/48990923/1/190x245/march-19-april-1-2012-pdf-mount-sinai-hospital.jpg?quality=85)
![PGY-1 Residency Application [PDF] - Mount Sinai Hospital](https://img.yumpu.com/48577701/1/190x245/pgy-1-residency-application-pdf-mount-sinai-hospital.jpg?quality=85)


