Nobel missing teeth survey presented at AO Annual Meeting
Nobel missing teeth survey presented at AO Annual Meeting
Nobel missing teeth survey presented at AO Annual Meeting
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
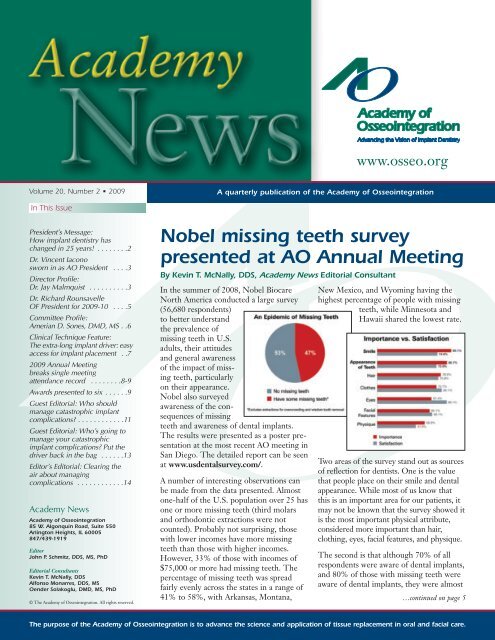
www.osseo.orgVolume 20, Number 2 • 2009A quarterly public<strong>at</strong>ion of the Academy of Osseointegr<strong>at</strong>ionIn This IssuePresident’s Message:How implant dentistry haschanged in 25 years! . . . . . . . .2Dr. Vincent Iaconosworn in as <strong>AO</strong> President . . . .3Director Profile:Dr. Jay Malmquist . . . . . . . . . .3Dr. Richard RounsavelleOF President for 2009-10 . . . .5Committee Profile:Amerian D. Sones, DMD, MS . .6Clinical Technique Fe<strong>at</strong>ure:The extra-long implant driver: easyaccess for implant placement . .72009 <strong>Annual</strong> <strong>Meeting</strong>breaks single meeting<strong>at</strong>tendance record . . . . . . . .8-9Awards <strong>presented</strong> to six . . . . . .9Guest Editorial: Who shouldmanage c<strong>at</strong>astrophic implantcomplic<strong>at</strong>ions? . . . . . . . . . . . .11Guest Editorial: Who’s going tomanage your c<strong>at</strong>astrophicimplant complic<strong>at</strong>ions? Put thedriver back in the bag . . . . . .13Editor’s Editorial: Clearing theair about managingcomplic<strong>at</strong>ions . . . . . . . . . . . .14Academy NewsAcademy of Osseointegr<strong>at</strong>ion85 W. Algonquin Road, Suite 550Arlington Heights, IL 60005847/439-1919EditorJohn P. Schmitz, DDS, MS, PhDEditorial ConsultantsKevin T. McNally, DDSAlfonso Monarres, DDS, MSOender Solakoglu, DMD, MS, PhD© The Academy of Osseointegr<strong>at</strong>ion. All rights reserved.<strong>Nobel</strong> <strong>missing</strong> <strong>teeth</strong> <strong>survey</strong><strong>presented</strong> <strong>at</strong> <strong>AO</strong> <strong>Annual</strong> <strong>Meeting</strong>By Kevin T. McNally, DDS, Academy News Editorial ConsultantIn the summer of 2008, <strong>Nobel</strong> BiocareNorth America conducted a large <strong>survey</strong>(56,680 respondents)to better understandthe prevalence of<strong>missing</strong> <strong>teeth</strong> in U.S.adults, their <strong>at</strong>titudesand general awarenessof the impact of <strong>missing</strong><strong>teeth</strong>, particularlyon their appearance.<strong>Nobel</strong> also <strong>survey</strong>edawareness of the consequencesof <strong>missing</strong><strong>teeth</strong> and awareness of dental implants.The results were <strong>presented</strong> as a poster present<strong>at</strong>ion<strong>at</strong> the most recent <strong>AO</strong> meeting inSan Diego. The detailed report can be seen<strong>at</strong> www.usdental<strong>survey</strong>.com/.A number of interesting observ<strong>at</strong>ions canbe made from the d<strong>at</strong>a <strong>presented</strong>. Almostone-half of the U.S. popul<strong>at</strong>ion over 25 hasone or more <strong>missing</strong> <strong>teeth</strong> (third molarsand orthodontic extractions were notcounted). Probably not surprising, thosewith lower incomes have more <strong>missing</strong><strong>teeth</strong> than those with higher incomes.However, 33% of those with incomes of$75,000 or more had <strong>missing</strong> <strong>teeth</strong>. Thepercentage of <strong>missing</strong> <strong>teeth</strong> was spreadfairly evenly across the st<strong>at</strong>es in a range of41% to 58%, with Arkansas, Montana,New Mexico, and Wyoming having thehighest percentage of people with <strong>missing</strong><strong>teeth</strong>, while Minnesota andHawaii shared the lowest r<strong>at</strong>e.Two areas of the <strong>survey</strong> stand out as sourcesof reflection for dentists. One is the valueth<strong>at</strong> people place on their smile and dentalappearance. While most of us know th<strong>at</strong>this is an important area for our p<strong>at</strong>ients, itmay not be known th<strong>at</strong> the <strong>survey</strong> showed itis the most important physical <strong>at</strong>tribute,considered more important than hair,clothing, eyes, facial fe<strong>at</strong>ures, and physique.The second is th<strong>at</strong> although 70% of allrespondents were aware of dental implants,and 80% of those with <strong>missing</strong> <strong>teeth</strong> wereaware of dental implants, they were almost…continued on page 5…continued on page 13The purpose of the Academy of Osseointegr<strong>at</strong>ion is to advance the science and applic<strong>at</strong>ion of tissue replacement in oral and facial care.
President’s MessageHow implant dentistry has changed in 25 years!By Vincent J. Iacono, DMDI am honored to follow Drs. Steven Eckert and Steven Lewisas <strong>AO</strong> President and wish to thank the membership, <strong>AO</strong>Board of Directors and staff for having the confidence in meto lead your Academy as it enters itssilver anniversary year. I accept thechallenges we face and pledge to domy best to lead this premier organiz<strong>at</strong>ionin the world on implantology toachieve its goals and objectives in fulfillingits vision of advancing oralhealth and well being by dissemin<strong>at</strong>ingst<strong>at</strong>e-of-the-art clinical and scientificknowledge of implant dentistry andDr. Vincent Iacono tissue engineering.Your Academy has just completed a most successful year underthe leadership of President Steven Lewis including the outstandingannual meeting in San Diego. <strong>AO</strong>’s ExecutiveDirector, Mr. Kevin Smith, reported th<strong>at</strong> <strong>at</strong>tendance set anall-time record of over 1,900. In addition, student <strong>at</strong>tendancere<strong>presented</strong> 402 of this total, which has established a new student<strong>at</strong>tendance record.The San Diego meeting has received kudos from speakers,<strong>at</strong>tendees and our corpor<strong>at</strong>e sponsors. The successful SanDiego meeting has increased the efforts of Dr. Stuart Froumand his planning committee to develop a “ne plus ultra” programfor the <strong>AO</strong>’s silver anniversary meeting to be held March4-6, 2010 <strong>at</strong> the Walt Disney Dolphin Hotel in Orlando,Florida. The program, entitled “25 Years of Experience – TheFormula for Predictable Implant Success,” is sure to be aw<strong>at</strong>ershed event in implant educ<strong>at</strong>ion.At the outset, I would like to acknowledge my mentors, Drs.Paul Baer and Charles Berman. Through their guidance, Ibecame one of the first 50 periodontists to be trained byProfessor Ingvar Brånemark on osseointegr<strong>at</strong>ed dentalimplants. Indeed, it was an educ<strong>at</strong>ional experience th<strong>at</strong> literallychanged my professional career.It was through Uncle Charlie’s direction th<strong>at</strong> I joined thethen-new Academy 25 years ago and performed my firstimplant surgery in 1985. I can still remember th<strong>at</strong> case. Itincluded inserting five grade 1 commercially pure titaniumexternal hex machined 3.75mm diameter screws into pretappedand countersunk osteotomies in the anterior sextant ofa fully edentulous mandible of a 60-year old woman undergeneral anesthesia for a fixed/detachable denture.How m<strong>at</strong>ters have changed in 25 years! The awesome innov<strong>at</strong>ionsin surgery, prosthodontics, bone biology, m<strong>at</strong>erials scienceand inform<strong>at</strong>ics since then have been mesmerizing.Implant designs and surfaces have been modified to improvethe kinetics and degree of osseointegr<strong>at</strong>ion. Implant abutmentinterfaces have been redesigned to facilit<strong>at</strong>e restor<strong>at</strong>ions andnew surgical procedures have been developed for soft and hardtissue augment<strong>at</strong>ion th<strong>at</strong> optimize implant function andesthetics. The new technologies in imaging and computersoftware for the tre<strong>at</strong>ment planning, surgical guiding, andrestoring of implants have essentially changed how we practiceimplant dentistry today.In recognition of our ever-changing discipline, your Academywill continue to enhance its educ<strong>at</strong>ional initi<strong>at</strong>ives on the <strong>AO</strong>Website, expand regional events for postdoctoral students andresidents, explore the feasibility of developing educ<strong>at</strong>ionalstandards for implantology, and continue its intern<strong>at</strong>ional outreachefforts. These activities will raise the bar for the provisionof implant services throughout the world and enhance theclinical outcomes for our p<strong>at</strong>ients.Two tangible outcomes of our educ<strong>at</strong>ional initi<strong>at</strong>ives include ahands-on workshop during the <strong>AO</strong>’s 25th annual meeting anda scientific workshop to commemor<strong>at</strong>e the <strong>AO</strong>’s silveranniversary. The Hands-On Workshop Committee, under theleadership of Drs. Stephen Wallace and Stephen Parel, isdeveloping an all-day workshop on Wednesday, March 3, 2010on computer based imaging, tre<strong>at</strong>ment planning, implantsurgery, and restor<strong>at</strong>ion of dental implants. As <strong>at</strong>tendance willbe limited for this highly valued educ<strong>at</strong>ional experience, besure to register early!The planning for the Academy’s 25th anniversary event wascrystallized with the recommend<strong>at</strong>ion th<strong>at</strong> the <strong>AO</strong> would holda workshop in the summer of 2010 with the theme,“Challenges for the Future in Implant Dentistry.” TheWorkshop will include two principal areas, each having severalrel<strong>at</strong>ed subtopics, as follows:1. Bioengineering for Soft and Hard Tissuea. Biologics – Growth and Differenti<strong>at</strong>ion Factors/Scaffoldsb. Stem Cell Researchc. Nanotechnologyd. Emerging Surgical Technologies2. Appropri<strong>at</strong>e Measures ofClinical Outcomes for Implant Therapya. P<strong>at</strong>ient Specific Outcome Measuresb. Clinical Specific Outcome MeasuresThe Planning Committee consists of Drs. Peter Moy andmyself, as Co-Chairs, Tara Aghaloo, Neel Bh<strong>at</strong>avadekar,David Cochran, Steven Eckert, Brian Mealey, ThomasO<strong>at</strong>es, Eleni Roumanas, Clark Stanford, and Ulf Wikesjo.The Committee is in the process of finalizing the selection ofcontent experts and participants. The Workshop is tent<strong>at</strong>ivelyscheduled for August 5-8, 2010 <strong>at</strong> the Oak Brook HillsMarriott Resort in Oak Brook, Illinois.…continued on page 132
Dr. Vincent Iacono sworn in as <strong>AO</strong> PresidentDr. Vincent J. Iacono, Stony Brook,NY, was sworn in as 2009-10 <strong>AO</strong>President during the Academy’s annualBusiness <strong>Meeting</strong> in San Diego.Newly elected members of the <strong>AO</strong>Board of Directors with Dr. Iacono are:• Dr. Peter K. Moy, Los Angeles, CA,President-elect;• Dr. Kenneth F. Hinds, LagunaNiguel, CA, Vice President;• Dr. Stephen L. Wheeler, Encinitas,CA, Secretary;• Dr. Jay P. Malmquist, Portland, OR,Director.<strong>AO</strong> President: Dr. Vincent IaconoDr. Iacono is Distinguished ServiceProfessor and Chairman, Departmentof Periodontology, School of DentalMedicine, Stony Brook University. Heis also Director of the school’sAdvanced Educ<strong>at</strong>ion Program inPeriodontics, and Associ<strong>at</strong>e Dean ofPostgradu<strong>at</strong>e Programs.Dr. Iacono co-chaired the Academy’slandmark 2006 Workshop on the St<strong>at</strong>e ofthe Science of Implant Dentistry. He hasserved on the Board of Directors since2000, including terms as <strong>AO</strong> Presidentelect,Vice President and Secretary. Dr.Iacono had been active on many <strong>AO</strong>committees and also served on theOsseointegr<strong>at</strong>ion Found<strong>at</strong>ion Board ofDirectors. In addition, Dr. Iacono is pastPresident of the American Academy ofPeriodontology (AAP).Dr. Peter Moy<strong>AO</strong> President-elect: Dr. Peter MoyDr. Moy is Director of Implant Dentistry<strong>at</strong> UCLA and Associ<strong>at</strong>e Professor ofClinicalDentistry <strong>at</strong> theUCLA School ofDentistry. He isVisitingProfessor, FourthMilitary MedicalUniversity, Xi’an,China, and oper<strong>at</strong>esa priv<strong>at</strong>epractice focusingprimarily in the areas of osseointegr<strong>at</strong>edimplants and reconstruction of severely<strong>at</strong>rophic ridges.An Academy Fellow, Dr. Moy isAssoci<strong>at</strong>e Editor of the Intern<strong>at</strong>ionalJournal of Oral and Maxillofacial Implants(IJOMI), <strong>AO</strong>’s official journal. He previouslyserved as <strong>AO</strong> Vice President andTreasurer, chaired the organiz<strong>at</strong>ion’sMembership Committee, and served onthe Research Committee and Ad HocCommittee on Practice Management.<strong>AO</strong> Vice President:Dr. Kenneth HindsDr. Hinds oper<strong>at</strong>es a priv<strong>at</strong>e practiceemphasizing comprehensive, estheticand implantdentistry, andis a VisitingLecturer(Restor<strong>at</strong>iveDentistry)<strong>at</strong> UCLA.An <strong>AO</strong> Fellow,Dr. HindsDr. Kenneth Hinds served as <strong>AO</strong>Secretary,chaired the Academy’s ScientificProgram Committee for its 2005<strong>Annual</strong> <strong>Meeting</strong> in Orlando, FL, andserved as <strong>Annual</strong> <strong>Meeting</strong> Chair for the2006 meeting in Se<strong>at</strong>tle, WA.<strong>AO</strong> Secretary: Dr. Stephen WheelerDr. Wheeler’s priv<strong>at</strong>e practice is basedin Encinitas, CA, where he provides afull scope of oral, maxillofacial and dentalimplant surgery. One of the firstdoctors in the U.S. to begin titaniumdental implant placement in the mid-1980s, he went on to establish theRancho Santa Fe Dental ImplantDentistry Club as a forum for implantdentistry training and educ<strong>at</strong>ion.…continued on page 11Director’s ProfileCommanding officer encouraged Dr. Jay Malmquist’s dental careerAcademy Director Dr. Jay Malmquist,Portland, OR, credits the influence ofhis former U.S. Army commanding officerfor setting him on the p<strong>at</strong>h to a successful30-year career as an oral andmaxillofacial surgeon.Following gradu<strong>at</strong>ion from theUniversity of Oregon Dental School,Dr. Malmquist completed an Armyrot<strong>at</strong>ing internship <strong>at</strong> Fort Jackson, SC.There, he was inspired by ColonelWilliam Bond’s integrity, leadership andprofessionalism.“Col. Bond was a n<strong>at</strong>ural leader; an iconin the eyes of the clinicians who servedunder him,” Dr. Malmquist recalls. “His<strong>at</strong>tention to detail and professionaldemeanor had a profound impact inhelping me become the person I wantedto be. He encouraged me to pursue acareer in oral and maxillofacial surgery,something I probably would not haveconsidered without his guidance.”Dr. Jay Malmquist is very proud of his two sons,Michael (left) and Chris (right).During two years of active duty serviceas a General Dentistry Officer <strong>at</strong> theYuma Proving Grounds, Yuma, AZ, Dr.Malmquist achieved the rank of Captain.Following his discharge, he completedresidency training in oral and maxillofacialsurgery <strong>at</strong> Oregon Health ScienceUniversity. He established a priv<strong>at</strong>epractice in Portland in 1977.In 1984, Dr. Malmquist was introducedto the concept of osseointegr<strong>at</strong>ion duringa weeklong educ<strong>at</strong>ional programheld <strong>at</strong> the University of Washington,one of four training centers establishedto dissemin<strong>at</strong>e inform<strong>at</strong>ion about thenew technique across North America.…continued on page 113
EXTR<strong>AO</strong>RDINARYIntroducing a new implant from the most respected name in dentistry - Sybron.Our newincorpor<strong>at</strong>es an extraordinary array of fe<strong>at</strong>uresproven to address immedi<strong>at</strong>e stability 1 , preserv<strong>at</strong>ion of crestal bone 2 ,and long-term aesthetics.Call us today to experience the EXTR<strong>AO</strong>RDINARY for yourself!1 Surgical and Mechanical Techniques to Increase Stability of Dental Implants. Kharouf, Zeineb; Oh, Hyeong Cheol; Saito, Hanae; Cardaropoli, Giuseppe; Bral, Michael;Cho, Sang-Choon; Froum, Stuart; Tarnow, Dennis. Ashman Department of Periodontology and Implant Dentistry, New York University. Research <strong>presented</strong> <strong>at</strong> the <strong>AO</strong> Boston 2008.2 Implant Design and Its Effect on Preserv<strong>at</strong>ion of Crestal Bone Levels. Jang, Bong-Joon; Pena, Maria Luisa; Kim, Mean Ji; Eskow, Robert; Elian, Nicolas; Cho, Sang-Choon;Froum, Stuart; Tarnow, Dennis. Ashman Department of Periodontology and Implant Dentistry, New York University. Research <strong>presented</strong> <strong>at</strong> the <strong>AO</strong> Boston 2008.EuropeJulius-Bamberger-Str. -Str.8a28279 Bremen, GermanyT 49.421.43939.0Sybron - Celebr<strong>at</strong>ing over 100years of dental excellenceUnited KingdomFrance# 5 & 6, Tadcaster House16 Rue du Sergent BobillotKempton Rd Keytec 7 Business Pk 93100 Montreuil, FrancePershore, Worchestershire, WR10 2TAT33.149.88.60.85T 44.1386.561.845HEADQUARTERSAustraliaUSA# 10, 112-118 Talavera Rd1717 West Collins AvenueNorth Ryde, NSW2113Orange, California 92867T 61.2.8870.3099T 714.516.7800www.sybronimplants.com
Dr. Richard Rounsavelle OF President for 2009-10Dr. Richard RounsavelleDr. Richard K. Rounsavelle,Torrance, CA, has been elected 2009-10 President of the Osseointegr<strong>at</strong>ionFound<strong>at</strong>ion, succeeding Dr. Fraya I.Karsh, New York, NY, who remainson the Board as Immedi<strong>at</strong>e PastPresident. Dr. Rounsavelle was <strong>AO</strong>President in 2006-07.Other officers elected during theFound<strong>at</strong>ion’s meetings in San Diego are:Drs. James H. Doundoulakis, New York, NY, Vice President,and Jon<strong>at</strong>han H. Orenstein, Marlton, NJ, Secretary-Treasurer.<strong>AO</strong>’s Immedi<strong>at</strong>e Past President, Dr. Steven G. Lewis,Cincinn<strong>at</strong>i, OH, joins the Board as Academy LiaisonDirector. Newly elected Found<strong>at</strong>ion Directors are Drs.Clarence C. Lindquist, Washington, DC, and Kevin T.McNally, Culver City, CA.Continuing as OF Directors are Drs. Edward M. Amet,Overland Park, KS, and Luis J. Fujimoto, New York, NY.Two of the OF officers and directors are general practitioners,two periodontists, four prosthodontists, and one an oral andmaxillofacial surgeon.<strong>Nobel</strong> Survey …continued from page 1three times more likely to be tre<strong>at</strong>edwith a fixed bridge to restore <strong>missing</strong><strong>teeth</strong>. Forty percent of those with a fixedbridge were unaware th<strong>at</strong> it was not apermanent solution.Another r<strong>at</strong>her glaring finding was th<strong>at</strong>when tre<strong>at</strong>ment options were discussedwith these p<strong>at</strong>ients, dentists recommendedimplants just 14% of the time.Other options, such as fixed bridges andremovable dentures, were similarly recommended.A whopping 45% of thetime, nothing was discussed.While <strong>survey</strong> d<strong>at</strong>a may often be interpretedcritically, the general inform<strong>at</strong>iong<strong>at</strong>hered can be useful for discussion.The <strong>Nobel</strong> <strong>survey</strong> certainly has pointedout potential weaknesses in our assumptionsabout p<strong>at</strong>ient <strong>at</strong>titudes and ourown consider<strong>at</strong>ion of implant replacementof <strong>missing</strong> n<strong>at</strong>ural <strong>teeth</strong>. <strong>AO</strong> membersalmost by definition perhaps don’tfit this d<strong>at</strong>a set, but if these d<strong>at</strong>a are correct,dentistry as a whole has some roomto grow in its discussion and recommend<strong>at</strong>ionof dental implants. Our p<strong>at</strong>ientscertainly seem to be ready.5
Committee Profile: Amerian D. Sones, DMD, MS20-year member, now active Committee Vice Chair,Dr. Sones shows residents advantages of <strong>AO</strong> membershipDr. Amerian D. Sones, Santa Maria,CA, has been a very active Vice Chairof <strong>AO</strong>’s Membership and AwardsCommittee.Under her leadership, the Committeehas sponsored four major events toshow California’s postgradu<strong>at</strong>e residentsthe many advantages of Academymembership. Inform<strong>at</strong>ional meetingsDr. Amerian Soneswere held last May and June for residents<strong>at</strong> UCLA, USC, and Loma Linda University. Then, inJanuary, the Committee hosted an elegant evening reception<strong>at</strong> the Los Angeles County Museum of Art. The events certainlycontributed to a record turnout of student registrants <strong>at</strong>the Academy’s San Diego <strong>Annual</strong> <strong>Meeting</strong>.<strong>AO</strong>’s immedi<strong>at</strong>e past president, Dr. Steven G. Lewis,Cincinn<strong>at</strong>i, OH, has enjoyed a long friendship with Dr. Sones,having first met her as a co-resident <strong>at</strong> UCLA in 1982. “She’svery serious and hardworking, but wh<strong>at</strong> makes her unique isth<strong>at</strong> she always has a gre<strong>at</strong> sense of humor,” Dr. Lewis says.<strong>AO</strong>’s president-elect, Dr. Peter K. Moy, Los Angeles, a colleaguewhose friendship with Dr. Sones also d<strong>at</strong>es back 25years, when they were both UCLA residents, describes her asan “all around wonderful person.” Her energy and outgoing,friendly personality contributed gre<strong>at</strong>ly to the success of theevents for postgradu<strong>at</strong>e residents, he believes.Dr. Moy also remembers Dr. Sones as a very effective memberof the UCLA School of Dentistry faculty. “She’s one of thebrightest people I know, and she’s able to take th<strong>at</strong> knowledgeand transfer it with her hands. I’ve never seen anyone workbetter with her hands,” he says.Another colleague from her days on the UCLA faculty, Dr.Robert E. Garfield, Los Angeles, describes her as a “highlyskilled, extremely capable prosthodontist who’s very good withp<strong>at</strong>ients.” Her energy and willingness to work contributed significantlyto the success of regional meetings he chaired severalyears ago to <strong>at</strong>tract general dentists to the Academy’smembership, says Dr. Garfield. “When she’s on a committee,she gives it her all,” he says.Dr. Sones’ early involvement in the Academy began as aspeaker on the scientific program in Dallas, Texas in 1989, presentingone of the earliest papers on “Complic<strong>at</strong>ions of DentalImplants.” She was involved in the first regional meetings theAcademy sponsored in southern California, and co-organizedthe first labor<strong>at</strong>ory program sponsored by the Academy fordental labor<strong>at</strong>ory technicians. At the request of Dr. WilliamLaney, Rio Verde, AZ, she was a contributing author on thetopic of “immedi<strong>at</strong>e loading of dental implants” for theIntern<strong>at</strong>ional Journal of Oral and Maxillofacial Implants (IJOMI).After completing her dental training <strong>at</strong> the Tufts School ofDental Medicine, Boston, MA, in 1979, Dr. Sones served twoyears in the Indian Health Service as a general staff dentist <strong>at</strong>the Sells Indian Health Dental Clinic, near Tucson, AZ. Herinterest in prosthodontics brought her to the UCLA School ofDentistry, where she completed a two-year residency inProsthodontics. She also completed a one-year residency inmaxillofacial prosthodontics and received a Masters of OralBiology in 1984.As a full-time faculty member in the Department of RemovableProsthodontics <strong>at</strong> UCLA, from 1984 to1987, she became interestedin Implant Prosthodontics and was co-organizer of theinitial Brånemark Training Center <strong>at</strong> UCLA. Since th<strong>at</strong> time,she has remained very active in the area of implant prosthetics.She has lectured extensively throughout the United St<strong>at</strong>es ondental implant rel<strong>at</strong>ed topics and has provided numerous clinicalresidency programs, teaching the restor<strong>at</strong>ive aspects of dentalimplants to general dentists and dental specialists.In addition to <strong>AO</strong>, she is an active member of the AmericanCollege of Prosthodontics, the California Dental Associ<strong>at</strong>ion,the American Dental Associ<strong>at</strong>ion, and the Pacific CoastSociety for Prosthodontics. She has been in priv<strong>at</strong>e practice inSanta Monica, California for 12 years and Westlake Village,California for 4 years. Since October 2000, she has maintaineda priv<strong>at</strong>e practice of implant prosthodontics in Santa Maria,serving California’s beautiful central coast.Dr. Sones’ husband,Lawrence Wolinsky,PhD, D.M.D., isAssoci<strong>at</strong>e Dean ofthe UCLA, Schoolof Dentistry. Theyare the proud parentsof three youngadults: Julia, 23, aUCLA School ofArt andArchitecture gradu<strong>at</strong>e,Zachary, 19, asophomore <strong>at</strong>University ofCalifornia, SantaThe Sones/Wolinsky family: Zachary, Julia, Andrew,and GusCruz, and Andrew, 17, a junior <strong>at</strong> Santa Ynez Valley UnionHigh school. A recent addition to her family is her 7-monthold“titanium colored” Weimeraner puppy, Gus.Dr. Sones is an avid runner, gardener, and bread and pie baker.Her recent baking endeavours won first place recognition forthree consecutive years in the Los Olivos Apple Pie Contest,during the annual town event, “A Day in the Country,”October 17, 2004, 2005, and 2006.6
Clinical Technique Fe<strong>at</strong>ureThe extra-long implant driver: easy access forimplant placement in the pterygomaxillary regionBy S<strong>at</strong>oshi K<strong>at</strong>o, DDS, and Michiko K<strong>at</strong>o, DDSA number of reports have described the surgical procedurefor placement of screw-type implants in the pterygomaxillaryregion and have revealed a good tre<strong>at</strong>ment outcome (1-5). Inmany cases,the implantsare inserted inan antero -l<strong>at</strong>eral direction(Fig 1).However,it is not easyto deliver theimplant covercap, healingcap, and theDrs. S<strong>at</strong>oshi K<strong>at</strong>o and Michiko K<strong>at</strong>oabutmentscrew with thecommercially available implant driver, due to access problemsin this region.We developed an extra-long driver combining custom-madeand commercially available driver parts, using a custom-madedriver from <strong>Nobel</strong>Biocare Japan K.K., Tokyo Japan(www.nobelbiocare.com). Commercially available driversinclude the Unigrip Driver, <strong>Nobel</strong> Biocare AB, Göteborg,Sweden) (Fig 2). Our extra-long implant driver consists of aconventional driver head <strong>at</strong>tached to a 50 mm-long shaft. Ithas helped to shorten the chairside time in many of our cases.The long shaft driver makes it possible to manipul<strong>at</strong>e thedriver head extra-orally by improving the visibility conditions(Fig 3). Furthermore, other instruments such as theHandpiece Zygoma 20:1 (<strong>Nobel</strong> Biocare AB, Göteborg,Sweden), can be used to place not only zygoma implants, butalso pterygomaxillary implants. Screw Post Removing PliersCurved Type (YDM Corpor<strong>at</strong>ion/Yamaura, Tokyo Japan,Email ydm@ydm.co.jp, URL http://ydm.co.jp), can be used tosmoothly remove the guidance pins while making an immedi<strong>at</strong>eprovisional bridge (Fig 4).We have found th<strong>at</strong> the extra-long implant driver mayimprove access for implant placements in the pterygomaxillaryregion, compared to the conventional commercially availableimplant drivers.References:1. Tulasne JF. Osseointegr<strong>at</strong>ed fixtures in the pterygoid region. InWorthington P, Brånemark PI,(eds). Advanced osseointegr<strong>at</strong>ionsurgery: Applic<strong>at</strong>ion in the maxillofacial region. Quintessence publishingco, inc. Illinois 1992:182-188.2. Bah<strong>at</strong> O. Osseointegr<strong>at</strong>ed Implants in the Maxillary Tuberosity:Report on 45 Consecutive P<strong>at</strong>ients. Int J Oral Maxillofac Implants1992;7:459-467.3. Valeron JF, Velazquez JF, Placement of screw-type implants in thepterygomaxillary-pyramidal region: Surgical procedure and preliminaryresults. Int J Oral Maxillofac Implants 1997;12:814-819.4. Balshi TJ, Wolfinger GJ, Balshi SF. Analysis of 356 pterygo-maxillaryimplants in edentulous arches for fixed prothesis anchorage. Int JOral Maxillofac Implants 1999;14: 398-406.5. Valeron JF, Valeron PF. Long-term Results in Placement of Screw-Type Implants in the Pterygomaxillary-Pyramidal Region. Int J OralMaxillofac Implants 2007;22:195-200.Drs. S<strong>at</strong>oshi and Michiko K<strong>at</strong>o, oper<strong>at</strong>e a priv<strong>at</strong>e practice, MedicalCorpor<strong>at</strong>ion Meishinkai, K<strong>at</strong>o Dental Clinic, Implant Center,Osaka, Japan. Email: samurai@k<strong>at</strong>osika.dental-net.jpFigure 1. The direction of implants inthe pterygomaxillary region.Figure 2. The extra-long implantdriver and three commer cially availableUnigrip drivers.Figure 3. The long shaft makes it easyto handle the driver head extra-orally.Figure 4. Handpiece zygoma (upper)and Screw post removing pliers curvedtype (lower).7
2009 <strong>Annual</strong> <strong>Meeting</strong> breaks single meeting <strong>at</strong>tend<strong>AO</strong>’s first president and longtime IJOMI editor, Dr.William R. Laney, accepts the <strong>Nobel</strong> Biocare BrånemarkOsseointegr<strong>at</strong>ion Award to honor an individual’s impacton implant dentistry.Attendance <strong>at</strong> the Academy’s San Diego <strong>Annual</strong><strong>Meeting</strong> broke the record for a single (not jointlysponsored) meeting, with 1,911 dentists (members,non-members, students, and faculty). In total,including auxiliary staff, lab techs, non-physicians,exhibitors, spouses and guests, the meeting drew3,667, also a single meeting record. Only thecollabor<strong>at</strong>ive meetings in Boston in 2003 and 2008have been bigger.Program Chair Dr. David L. Guichetaddresses the opening session.The posters <strong>at</strong>tracted many viewers and provokedprofessional interaction.Their smiles show something clicked for this poster team.The audience is following every word of this scientificpresent<strong>at</strong>ion.Much of the <strong>Annual</strong> <strong>Meeting</strong>’s action took place in theexhibit area.Thank youfor your supportThe Academy of Osseointegr<strong>at</strong>ionthanks the following companies fortheir generous support of theAcademy’s 24th <strong>Annual</strong> meeting:• ACE Surgical Supply• Astra Tech Inc.• Bio-Horizons• BIOMET 3i• DENTSPLY Tulsa Dental Specialties• Keystone Dental• Medtronic• Neoss Inc.• <strong>Nobel</strong> Biocare• Osteohealth Company• Piezosurgery• Quintessence Publishing Co.• Straumann Company• Sybron Implant Solutions• Zimmer DentalPassing of the gavel from outgoing President Dr.Steven G. Lewis (left) to incoming President Dr.Vincent J. Iacono.First hands-on workshop to debut<strong>at</strong> Academy’s 2010 <strong>Annual</strong> <strong>Meeting</strong>A hands-on workshop th<strong>at</strong> focuses oncomputer-guided tre<strong>at</strong>ment programswill take place in advance of theAcademy’s 2010 <strong>Annual</strong> <strong>Meeting</strong> inOrlando, FL, Hands-On WorkshopCommittee Chair Dr. Stephen S.Wallace, W<strong>at</strong>erbury, CT, reports.The pre-meeting program, to be heldWednesday, March 3, will offer a series ofconcurrent surgical and restor<strong>at</strong>ive workshops.Attendees will have opportunitiesto explore how 3-D imaging and navig<strong>at</strong>iontechnology helps providers fabric<strong>at</strong>esurgical templ<strong>at</strong>es, gener<strong>at</strong>e final prosthesisand place implants more effectively aspart of the “team approach” concept.“Increasingly, 3-D imaging and computerizedsoftware programs are enhancingthe team approach to implant dentistryThere was time to make friends, renew friendships, and enjoy themeeting’s social side.by providing comprehensive tre<strong>at</strong>mentplanning,” Dr. Wallace explains. “Thegoals of this session will be to give registrantsfirst-hand experience in the applic<strong>at</strong>ionof three-dimensional imaging andnavig<strong>at</strong>ion technology, and demonstr<strong>at</strong>ehow these systems aid in the diagnosisand tre<strong>at</strong>ment of p<strong>at</strong>ients.”The Hands-On Workshop Committeehas secured the support of Astra,BioHorizons, BioMet 3i, KeystoneDental and <strong>Nobel</strong> BioCare to provideequipment, supplies and speakers foreach session. Each presenter’s submittedprogram and educ<strong>at</strong>ional objectives aresubject to approval by the Academy.More inform<strong>at</strong>ion on the hands-onworkshop will be fe<strong>at</strong>ured in upcomingissues of Academy News.8
ance recordDr. Daniel Buser makes a point during hisopening symposium present<strong>at</strong>ion.Awards <strong>presented</strong> to sixDr. Tiziano T. Testori (leftphoto, far left) accepts theWilliam R. Laney Awardfor best IJOMI article fromEditor Dr. Steven E. Eckert(center) and Dr. Laney.<strong>AO</strong>/OF Research GrantCommittee Chair Dr.James L. Robbins (rightphoto, right) presents the<strong>AO</strong> Research Grant toDr. Ajay K. Dhingra.President Dr. Steven G.Lewis presents the awardsfor best oral scientificresearch present<strong>at</strong>ion toDr. Gustavo Mendonca(left) and for best oralclinical research present<strong>at</strong>ionto Dr. Juan Ibanez(right).New electronic signage made it easier for<strong>at</strong>tendees to find their way to programs.Poster present<strong>at</strong>ion awardswent to Dr. YoungBumPark (left) for bestscientific poster andDr. Ilser Turkyilmaz(right) for best clinicalposter. Dr. Lewis makesthe present<strong>at</strong>ions.Photographers are often drawn to the happiestpeople <strong>at</strong> the reception.<strong>AO</strong> President Dr. Steven Lewis shares a lightmoment with Dr. Sean Avera, Auburn, CA.An enthusiastic group of pre-meeting <strong>AO</strong> bikersjoined a Harley Bike Ride through San Diego’sback roads, following routes mapped by hostDr. Stephen Wheeler.Dr. Stephen Wheeler (fourth from right) played host again for post-meetinggolf <strong>at</strong> The Crosby Club <strong>at</strong> Rancho Sante Fe, followed by a cocktail reception <strong>at</strong>his nearby home.A social foursome (left to right): Allison Adams, of AstraTech,Valerie Sternberg-Smith, Craig Rodriguez, of AstraTech,and Jeffrey Cebula.Academy leaders aboard the ship CaliforniaPrincess for the President’s VIP Dinner cruise tothe Hotel del Coronado: Director Dr. Russell D.Nishimura (left) and Membership and AwardsCommittee Chair Dr. Luis J. Fujimoto.Incoming President Dr. Vincent J. Iacono (second from right)hosts Prof. Ludovico Sbordone (left), Chair of Implantology andPeriodontology <strong>at</strong> the University of Pisa in Italy, his wife,P<strong>at</strong>rizia, and Dr. Wayne Aldredge.9
Time to challenge old truthsAstra Tech Implant System – setting a new standardHow do you achieve optimal long-termtre<strong>at</strong>ment outcomes for your p<strong>at</strong>ients? Thestandard norm regarding dental implanttre<strong>at</strong>ment success from 1986 does not reflectwh<strong>at</strong> is possible to achieve today. There areno reasons why the clinician or the p<strong>at</strong>ientshould accept a marginal bone loss of up to1.5 millimeters based on a standard set 20years ago. It has been proven in study afterstudy th<strong>at</strong> with the Astra Tech Implant Systemthe mean marginal bone level reduction is only0.3 millimeters over five years.01 year 2 years 3 years 5 yearsMean marginal bone level change (mm)- 0.2- 0.4- 0.6- 0.8-1.0-1.2-1.4Optimized marginal bonemaintenance with theAstra Tech Implant SystemV- 0.3Astra Tech Implant System level*-1.5 Standard norm**-1.6Time period (yrs)* Astra Tech Implant System level based on d<strong>at</strong>a from more than 40 published articles presentingradiological d<strong>at</strong>a; liter<strong>at</strong>ure search April 2008** Standard norm according to:Albrektsson T., et al., Int J Oral Maxillofac Implants 1986;1(1):11-25Albrektsson T. and Zarb G.A., Int J Prosthodont 1993;6(2):95-105Roos J., et al., Int J Oral Maxillofac Implants 1997;12(4):504-514How much bone loss are you willing to accept?Visit www.astr<strong>at</strong>echdental.com and vote in the marginalbone maintenance campaign andfind out more about the factsbehind the figures.USA, Astra Tech Inc. 590 Lincoln Street, Waltham, MA 02451, Tel: +1-800-531-3481. Fax: +1-781-890-6808, www.astr<strong>at</strong>echdental.com
Guest EditorialWho should manage c<strong>at</strong>astrophic implant complic<strong>at</strong>ions?By Barry P. Levin, DMD periodontistAs a periodontist, I agree 100% with theconcept of managing dental implantcomplic<strong>at</strong>ions in the Volume 20, Number1 editorial in theAcademy News. Assomeone who hasalso trained withsome of the truepioneers inimplant surgicaltherapy, andsomeone whoDr. Barry Levinteaches dentalimplant surgery<strong>at</strong> the University of Pennsylvania, I amalso concerned about the unfortun<strong>at</strong>edirection implant therapy has taken.These one-stop-shop implant offices arenot only compromising a p<strong>at</strong>ient’s wellbeing,but also making it more difficultfor those of us who consider ourselves“team players" to provide standard ofcare tre<strong>at</strong>ment. More often recently,p<strong>at</strong>ients are refusing implant tre<strong>at</strong>ment,because they have had "bad past experienceswith implants" or know someonewho has shared a similar complic<strong>at</strong>ionstory. The public has no way of knowingwho is qualified to place implants.General practitioners are still the “g<strong>at</strong>ekeepers”to most dental p<strong>at</strong>ients. If theydiagnose a condition warranting implanttherapy, their p<strong>at</strong>ients count on them tonavig<strong>at</strong>e them to the final destin<strong>at</strong>ion. Ifthey aren’t given a choice of a surgicalspecialist to handle this component ofimplant therapy, they usually don't askfor a referral.Public awareness is key. The problemwe face as specialists is th<strong>at</strong> of notoffending our restor<strong>at</strong>ive colleagues.However, this prevents and is divisive tobroad public awareness campaigns.As a fellow lecturer, I am certain th<strong>at</strong> youcan rel<strong>at</strong>e to the dilemma of fieldingquestions from general practitioners andothers clearly trying to milk you for surgicaltips. This is very uncomfortable, aswe don’t wish to be offensive, disrespectful,or elitist. However, we have aresponsibility to our specialties, and Iwould never wish to be one of those specialistsmaking extra bucks by teachingsurgery to those unqualified to do so.Dr. Schmitz’ editorial was well read, andI thought everyone should know th<strong>at</strong> itdid not fall on deaf ears.Director’s Profile …continued from page 3Led by Dr. Per-Ingvar Brånemark,Goteborg, Sweden, the program markedthe first exposure of the BrånemarkMethod in the Pacific Northwest region.“Th<strong>at</strong> program was a game-changer. Tothis day, it remains the most impressiveeduc<strong>at</strong>ional experience I’ve ever been apart of,” Dr. Malmquist explains. “It wascompletely grounded in science andmade everyone who <strong>at</strong>tended a believer.”Dr. Malmquist <strong>at</strong>tended <strong>AO</strong>’s first<strong>Annual</strong> <strong>Meeting</strong> in New York City thefollowing year. A frequent <strong>Annual</strong><strong>Meeting</strong> <strong>at</strong>tendee and presenter sincethen, he marvels <strong>at</strong> how the Academyhas developed into the leading organiz<strong>at</strong>ionfor dental implant professionals.Newly Elected Officers …continued from page 3Dr. Wheeler chairs <strong>AO</strong>’s Ad HocCommittee on Intern<strong>at</strong>ional Rel<strong>at</strong>ions,and helped establish the <strong>AO</strong> DentalForum, accessible via the Academy’sWebsite, www.osseo.org. In addition,he chaired the Academy’s 2002 <strong>Annual</strong><strong>Meeting</strong> in Dallas, TX.<strong>AO</strong> Director: Dr. Jay MalmquistDr. Malmquist (see profile, page 3) is“The <strong>AO</strong>’s gre<strong>at</strong>est strength lies in thetalents and expertise of its individualmembers. No other dental organiz<strong>at</strong>ionenjoys such a cross-section of specialistswho are able to learn from each other ina non-competitive educ<strong>at</strong>ional environment,”Dr. Malmquist says. “Th<strong>at</strong> diversityhas made the <strong>Annual</strong> <strong>Meeting</strong> thepremier educ<strong>at</strong>ional forum for dentalimplant professionals. I consider it aprivilege to serve on the Board.”In addition to his Academy service, Dr.Malmquist served as an examiner withthe American Board of Oral andMaxillofacial Surgery for seven years.He spent eight years on the Board of theAmerican Associ<strong>at</strong>ion of Oral andProfessor of Oral and MaxillofacialSurgery <strong>at</strong> Oregon Health ScienceUniversity, Portland. He has maintaineda priv<strong>at</strong>e practice in Portland for morethan 30 years.Academy Officers and Directors continuingtheir service on the Board ofDirectors are Drs. Steven G. Lewis,Cincinn<strong>at</strong>i, OH (Past President);Maxillofacial Surgeons (A<strong>AO</strong>MS),including a term as its president.Away from the office, Dr. Malmquistenjoys “working in my yard, playing golfand traveling to the Oregon coast.” Heis very proud of his two sons, Chris andMichael. Both are gradu<strong>at</strong>es of theMilitary College of South Carolina (TheCitadel), and are following in theirf<strong>at</strong>her’s career footsteps.Chris completed two tours of duty inthe Middle East with the Marine Corps,and is currently West Coast Manager fora major dental implant manufacturer.Michael is pursuing a Fellowship in Oraland Maxillofacial Surgery <strong>at</strong> BaylorUniversity, Dallas, TX.David L. Cochran, San Antonio, TX(Treasurer); and Directors JosephGian-Grasso, Philadelphia, PA;Frank L. Higginbottom, Dallas, TX;Russell D. Nishimura, WestlakeVillage, CA; Michael R. Norton,London, UK; Alan S. Pollack, NewYork, NY; and James Taylor, Ottawa,Ontario, Canada.11
<strong>Nobel</strong>Active TMTaking a new direction in implants.Dual-function prostheticconnectionBuilt-in Pl<strong>at</strong>form ShiftingBone-condensing propertyHigh initial stability,even in compromisedbone situ<strong>at</strong>ionsAdjustable implant orient<strong>at</strong>ionfor optimal final placement10 YEARS WITHTIUNITE® SURFACENew d<strong>at</strong>a confirmlong-term stability.<strong>Nobel</strong>Active equally s<strong>at</strong>isfies surgicaland restor<strong>at</strong>ive clinical goals.<strong>Nobel</strong>Active thread design progressivelycondenses bone with each turnduring insertion, which is designed toenhance initial stability. The sharp apexand cutting blades allow surgical cliniciansto adjust implant orient<strong>at</strong>ion foroptimal positioning of the prostheticconnection. Restor<strong>at</strong>ive cliniciansbenefit by a vers<strong>at</strong>ile and secure internalconical prosthetic connection withbuilt-in Pl<strong>at</strong>form Shifting upon whichthey can produce excellent estheticresults. Based on customer feedbackand market demands for <strong>Nobel</strong>Active,the product assortment has beenexpanded – dental professionals willnow enjoy even gre<strong>at</strong>er flexi bility inprosthetic and implant selection.<strong>Nobel</strong> Biocare is the world leaderin innov<strong>at</strong>ive evidence-based dentalsolutions.For more inform<strong>at</strong>ion, contact a<strong>Nobel</strong> Biocare Represent<strong>at</strong>ive <strong>at</strong>800 322 5001 or visit our website.www.nobelbiocare.com/nobelactive<strong>Nobel</strong> Biocare USA, LLC. 22715 Savi Ranch Parkway, Yorba Linda, CA 92887; Phone 714 282 4800; Toll free 800 993 8100;Tech. support 888 725 7100; Fax 714 282 9023<strong>Nobel</strong> Biocare Canada, Inc. 9133 Leslie Street, Unit 100, Richmond Hill, ON L4B 4N1; Phone 905 762 3500; Toll free 800 939 9394; Fax 800 900 4243© <strong>Nobel</strong> Biocare 2009. All rights reserved. www.nobelbiocare.com
Guest EditorialWho’s going to manage your c<strong>at</strong>astrophic implantcomplic<strong>at</strong>ions? Put the driver back in the bagBy Barry R. Franzen, DDS prosthodontistI don’t golf much anymore. It’s too hardto manage my complic<strong>at</strong>ions. I evenbought a $450driver th<strong>at</strong> wasguaranteed tocure any ailmentknown to JoeDuffer, but itonly accentu<strong>at</strong>edeverything th<strong>at</strong>was wrong in theDr. Barry Franzenfirst place.Lessons, practice?Not part of the thought process.When the other members of my foursomestarted to run for cover as myslices headed back to the tee box, I knewit was time to put it back in the bag.Management of complic<strong>at</strong>ions solved!I have been involved with implantssince 1982. Now we see more and more“non-surgeons” placing and restoringtheir own fixtures. I personally fall intoth<strong>at</strong> c<strong>at</strong>egory, as a prosthodontist placingmany of my own fixtures. I hadbeen in the implant game for over 17years and had been seeing fewer implantreferrals, because the surgeons weredoing those cases with the general practitionersI helped educ<strong>at</strong>e. I was seeingsignificant amounts of surgical production“leaking out the door” for the casesI was restoring.So I started thinking: I’ve been drillingPara posts successfully to within 0.2mmfor decades in a medium th<strong>at</strong> doesn’t heal.I have a good baseline knowledge of thesurgical aspect, and I get my Christmastree straight every year, even when mywife helps. Wouldn’t th<strong>at</strong> lost surgicalproduction look better in my pocket?Did I just run out, buy a drilling unitand start planting fixtures? No, it was adeliber<strong>at</strong>e process th<strong>at</strong> involved morethan a weekend course and then off tothe races. I was like Bill Murray in themovie “Wh<strong>at</strong> About Bob?” Baby steps,baby steps. It was an evolution of knowingone’s limit<strong>at</strong>ions, seeking the knowledge,expanding the knowledge, andgaining experience.This awareness was not only in theplacement and restor<strong>at</strong>ion, but also inthe problems th<strong>at</strong> may arise. Slowly andsteadily, this expanded to a point where Ihandle more difficult cases by myself. Ifthere is anything th<strong>at</strong> I feel is beyondmy limit<strong>at</strong>ions, I refer those cases to thesurgeons with whom I have had a rel<strong>at</strong>ionshipfor so many years. Misery doeslove company!So who is going to manage my c<strong>at</strong>astrophicimplant complic<strong>at</strong>ions? Theprosthetic end of it is not a problem. Iam way down th<strong>at</strong> learning curve. Andthere isn’t a week th<strong>at</strong> goes by th<strong>at</strong>someone isn’t calling with a prostheticissue with which I am asked to help.Granted, a prosthodontist placingimplants doesn’t cast a very big shadowin the surgery world, but a lot of goodwillis gener<strong>at</strong>ed when I do retrieve th<strong>at</strong>broken abutment screw for a surgeonand his general practitioner referral.There is even more goodwill when thegeneral dentist is doing both.Surgical complic<strong>at</strong>ions are another issue.While few and far between, when I needhelp, I expect and rely on my surgeons.They do so willingly, because they knowI have reciproc<strong>at</strong>ed in the past and willcontinue to do so in the future. The onetime in the past ten years I did need helpwas an incredible combin<strong>at</strong>ion of badluck and misaligned planets. I didn’tthink twice about calling for helpbecause I am already way ahead on thefavor “chit sheet.”So surgeons are starting to feel the pinchas more “non-surgeons” place implantsbefore taking baby steps. Do I detect justa bit of animosity when they may be askedto help clean up someone else’s mess?When it comes to c<strong>at</strong>astrophic failures,the prosthodontist community hashelped in the bailout since day one. Andwe sit like a faithful lab waiting for th<strong>at</strong>bone of a referral th<strong>at</strong> might be thrownour way as a reward. Maybe we are justnot self-confident enough to say, “Youbroke it. You bought it.” Or perhaps webetter understand th<strong>at</strong> the whole essenceof being a specialist is the ability andwillingness to make the complex routine.To those brother “non-surgeons” placingimplants I say, “Do your homeworkand know your limit<strong>at</strong>ions.” Just don’tstab the lifebo<strong>at</strong> th<strong>at</strong> may save you whenyou are in over your head. Keep a rel<strong>at</strong>ionshipwith a “real” surgeon for casesth<strong>at</strong> are out of your comfort zone.For those who don’t know their limit<strong>at</strong>ions,I say, “Come on in, the w<strong>at</strong>er iswarm!” Personally, I’d keep the clubs inthe bag th<strong>at</strong> get me in trouble but somepeople just can’t resist. Helping out onthose cases just adds to my knowledgebase on my third implant learningcurve, rescue!I sincerely like my Rube Goldberg alterego. I would invite my surgeon colleaguesto get in touch with theirs.Even if DRIMPLNTR deserves to godown in flames, his p<strong>at</strong>ient is worthy ofyour expertise. I guarantee you willhave a hitch in your giddy-up all daylong, especially when you pull a rabbitout of someone else’s h<strong>at</strong>!President’s Message…continued from page 2Regardless of the initi<strong>at</strong>ives to beimplemented, your Board will befiscally responsible in these terribleeconomic times. In this regard, I amconvening a str<strong>at</strong>egic planning sessionin conjunction with the next <strong>AO</strong>Board meeting in June 2009 th<strong>at</strong> willupd<strong>at</strong>e our str<strong>at</strong>egic plan to includegoals and objectives th<strong>at</strong> reflect the<strong>AO</strong>’s vision in a cost-effective manner.As <strong>AO</strong> President, I look forward toworking with my fellow Officers andBoard Members to serve you, themembership, using the philosophy ofthe 3Cs – “Communic<strong>at</strong>ion,Cooper<strong>at</strong>ion and Collabor<strong>at</strong>ion” tofulfill the <strong>AO</strong> vision. For we will bejudged not by our ideas, actions, orefforts, but by our tangible results.13
Editor’s EditorialClearing the air about managing complic<strong>at</strong>ionsin implant surgeryBy John P. Schmitz, DDS, MS, PhD, Newsletter EditorMy last Academy News editorial (“Wh<strong>at</strong>happens when implant placement turnsc<strong>at</strong>astrophic? Do we need to call DirtyHarry?” Volume 20, Number 1, 2009)gener<strong>at</strong>ed many emails and commentsto the Editor. The response was overwhelming,to say the least. It has takenme several weeks to begin to understandwh<strong>at</strong> it all means and to formul<strong>at</strong>ea response. I received emails fromDr. John Schmitz my clinician friends, from former residentsI trained, from my former classm<strong>at</strong>es,from former <strong>AO</strong> Presidents, and from people who justwalked up to me <strong>at</strong> the San Diego <strong>Annual</strong> <strong>Meeting</strong> and introducedthemselves.At first, I was going to try and address all the issues peoplehad raised. But as I began to coll<strong>at</strong>e a constructive response, Ifound th<strong>at</strong> some of the r<strong>at</strong>ionale just wasn’t there. I wastempted to print several of the Letters to the Editor intact.However, I decided against this for two reasons. First, it wouldhave taken too much newsletter space. And second, I’m noteven sure th<strong>at</strong> some of the members who wrote commentswould be comfortable having their letters published.The direction I have decided to take is to outline some of thecomments in the hope of clarifying my thoughts for the membershipand increasing understanding of wh<strong>at</strong> the <strong>AO</strong> is reallyabout. With this in mind, I will be the first to admit th<strong>at</strong> noteveryone will be completely s<strong>at</strong>isfied. Th<strong>at</strong> is the n<strong>at</strong>ure of ourdiverse membership. We must all understand th<strong>at</strong> we comefrom diverse specialty memberships, and th<strong>at</strong> the spirit of ourmembership should be educ<strong>at</strong>ion.However, in the spirit of allowing a voice to opposing viewpoints,I extended an offer to two <strong>AO</strong> members who emailedme comments (a prosthodontist, Dr. Barry R. Franzen, WestAllis, WI, and a periodontist, Dr. Barry P. Levin, Elkins Park,PA), to submit mini-editorials of their own. Their topic was:“Who will manage c<strong>at</strong>astrophic implant complic<strong>at</strong>ions?” Theirmini-editorials are published on Pages 13 and 11.As st<strong>at</strong>ed succinctly in the opening pages of our membershipdirectory, the Academy of Osseointegr<strong>at</strong>ion (<strong>AO</strong>) is a multidisciplinary,intern<strong>at</strong>ional dental implant organiz<strong>at</strong>ion th<strong>at</strong>exists to bring together individuals of different backgrounds inorder to share experience and knowledge regarding dentalimplants. Members share the common goal of moving thefield of osseointegr<strong>at</strong>ed implants forward through clinical andevidence-based research and educ<strong>at</strong>ion. The <strong>AO</strong> has publishedGuidelines for the Provision of Dental Implants (2008) andhosted a 2006 Consensus Conference on the St<strong>at</strong>e of theScience on Implant Dentistry.Discussing implant complic<strong>at</strong>ions and their management isimportant to moving the field of dental implant tre<strong>at</strong>ment forward.The <strong>AO</strong> regularly offers a session on complic<strong>at</strong>ions <strong>at</strong>the <strong>Annual</strong> <strong>Meeting</strong>. If a dentist doesn’t believe th<strong>at</strong> managingcomplic<strong>at</strong>ions is important, then the issue of p<strong>at</strong>ient safetymay not be high on his or her priority list. It should be.Managing complic<strong>at</strong>ions is about managing p<strong>at</strong>ient safety.One member responded to my editorial by emailing th<strong>at</strong> Ishould not go public in deline<strong>at</strong>ing other dentists’ shortcomings.P<strong>at</strong>ient safety is embedded in the definition of the <strong>AO</strong>.However, there will always be isol<strong>at</strong>ed dentists who will feelth<strong>at</strong> complic<strong>at</strong>ion management should be someone else’s problem.There are also some who will feel th<strong>at</strong> they have the skillset to manage all dental implant complic<strong>at</strong>ions, regardless ofhow little formal surgical training they received in their postgradu<strong>at</strong>eprepar<strong>at</strong>ion.Let me conclude by summarizing my thoughts after all thisdiscourse. I must admit th<strong>at</strong> most comments directed to mewere surprisingly supportive. Some of the opposing commentsseemed to come from members who misunderstood andtherefore misre<strong>presented</strong> the intended message of my editorial.The editorial was about complic<strong>at</strong>ions, not credentialing. Itwas about managing dental implant complic<strong>at</strong>ions in the bestinterest of p<strong>at</strong>ient safety.In several emails, members conveyed a variety of reasons whythey began to surgically place their own implants. Several reasonswere advanced as justific<strong>at</strong>ion for performing implantsurgery. However, the decision of a dentist to justify why he orshe performs such procedures was not the issue. The editorialwas about complic<strong>at</strong>ions.I believe my editorial was misunderstood by many doctors,who thought it suggested, “General dentists should not placeimplants.” This was not my intended message. The messagewas how to manage complic<strong>at</strong>ions (and indirectly p<strong>at</strong>ient safety).However, many doctors who place implants these daysdon’t recognize their own limit<strong>at</strong>ions.The <strong>AO</strong> Board is still determining the best way to assurep<strong>at</strong>ient safety and maintain the high level of expertise and carein implant dentistry. The response to my editorial shows howimportant and how sensitive this issue can be. I support theBoard’s str<strong>at</strong>egic planning efforts and remain confident th<strong>at</strong>their actions will be in the best interest of implant dentistry.Readers who would like to comment or express a point of view on theeditorial are invited to write via e-mail to the editor <strong>at</strong>schmitzjp@hotmail.com. We will endeavor to publish pertinentcomments or views when space permits.14
6.0 x 5.7mm4.5 x 6.0mm5.0 x 6.0mm6.0 x 5.0mm 5.0 x 5.0mmWITH BICON’S SHORTIMPLANTS YOU CAN: Avoid vital structures Minimize bone grafting procedures Maximize placement possibilities Increase p<strong>at</strong>ient acceptance Offer single unit restor<strong>at</strong>ionswithout splintingCALL FOR MORE INFORMATIONCALL 800.88.BICON today and ask for a Short Implant inform<strong>at</strong>ion packageincluding research articles, or visit www.bicon.com/shortimplantsSince 1985 » Simple. Predictable. Profitable.501 Arborway Boston, MA 02130 800.88.BICON +1 617.524.4443 www.bicon.com
N<strong>at</strong>ural Tapered ImplantPrimary Implant Stability Starts WithThe BIOMET 3i Tapered Implant System“BIOMET 3i’s Tapered Implant provides for primary stability through its macrogeometric design.This Tapered Implant is by far the most widely used implant in my clinical practice.”-Dr. Markus Hürzeler, GermanyTo Find Out How You Can Achieve Primary Implant Stability With BIOMET 3i’s Tapered Implant System,Contact Your BIOMET 3i Represent<strong>at</strong>ive Today. In the USA: 1-800-342-5454 • Outside the USA: +1-561-776-6700or visit us online <strong>at</strong> www.biomet3i.comBIOMET is a registered trademark and BIOMET 3i and design are trademarks of BIOMET, Inc. ©2009 BIOMET 3i LLC. All rights reserved.