DHHS 4041 Vaccine Administration Record - Immunization Branch
DHHS 4041 Vaccine Administration Record - Immunization Branch
DHHS 4041 Vaccine Administration Record - Immunization Branch

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
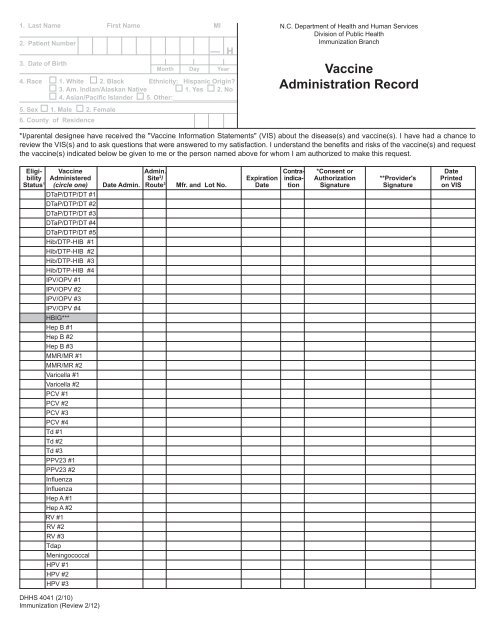
1. Last Name First Name MI2. Patient Number3. Date of Birth— H4. Race o 1. White o 2. Black Ethnicity: Hispanic Origin?o 3. Am. Indian/Alaskan Native o 1. Yes o 2. Noo 4. Asian/Pacific Islander o 5. Other:__________________5. Sex o 1. Male o 2. Female6. County of ResidenceMonth Day YearN.C. Department of Health and Human ServicesDivision of Public Health<strong>Immunization</strong> <strong>Branch</strong><strong>Vaccine</strong><strong>Administration</strong> <strong>Record</strong>*I/parental designee have received the "<strong>Vaccine</strong> Information Statements" (VIS) about the disease(s) and vaccine(s). I have had a chance toreview the VIS(s) and to ask questions that were answered to my satisfaction. I understand the benefits and risks of the vaccine(s) and requestthe vaccine(s) indicated below be given to me or the person named above for whom I am authorized to make this request.Eligi- <strong>Vaccine</strong> Admin. Contra- *Consent or Datebility Administered Site 2 / Expiration indica- Authorization **Provider's PrintedStatus 1 (circle one) Date Admin. Route 3 Mfr. and Lot No. Date tion Signature Signature on VISDTaP/DTP/DT #1DTaP/DTP/DT #2DTaP/DTP/DT #3DTaP/DTP/DT #4DTaP/DTP/DT #5Hib/DTP-HIB #1Hib/DTP-HIB #2Hib/DTP-HIB #3Hib/DTP-HIB #4IPV/OPV #1IPV/OPV #2IPV/OPV #3IPV/OPV #4HBIG***Hep B #1Hep B #2Hep B #3MMR/MR #1MMR/MR #2Varicella #1Varicella #2PCV #1PCV #2PCV #3PCV #4Td #1Td #2Td #3PPV23 #1PPV23 #2InfluenzaInfluenzaHep A #1Hep A #2RV #1RV #2RV #3TdapMeningococcalHPV #1HPV #2HPV #3<strong>DHHS</strong> <strong>4041</strong> (2/10)<strong>Immunization</strong> (Review 2/12)
<strong>Vaccine</strong> <strong>Administration</strong> <strong>Record</strong>Name: _____________________________________________________________________DOB:__ __/__ __/__ __ __ __(Last) (First) (Middle) Mo. Day Year*I/parental designee have received the "<strong>Vaccine</strong> Information Statements" (VIS) about the disease(s) and vaccine(s). I have had a chance toreview the VIS(s) and to ask questions that were answered to my satisfaction. I understand the benefits and risks of the vaccine(s) and requestthe vaccine(s) indicated below be given to me or the person named above for whom I am authorized to make this request.Eligi- <strong>Vaccine</strong> Admin. Contra- *Consent or Datebility Administered Site 2 / Expiration indica- Authorization **Provider's PrintedStatus 1 (circle one) Date Admin. Route 3 Mfr. and Lot No. Date tion Signature Signature on VISAllergies, TB Skin Test, Notes:*I am authorized by the parent, guardian, or person standing in loco parentis of the above-named child to obtain needed immunizations for the child.**I have asked about immunizations and prior reactions. According to informant, none have occurred.***An infant receiving HBIG should be evaluated for hepatitis B vaccine (Engerix 10 mcg/0.5ml OR Recombivax 5 mcg/0.5ml) within 12 hours of birth, and atand 6 months of age.1Eligibility Status: A – American Indian /Alaskan Native 2Admin. Site: RA = Right ArmM – MedicaidLA = Left ArmN – Not InsuredRT = Right ThighU – Underinsured (insurance does not cover fullLT = Left Thighcost of immunizations) 3Admin. Route: IM = IntramuscularH – NC Health Choice for ChildrenSC = SubcutaneousI – InsuredOralPurpose:Preparation:Directions:Distribution:Disposition:Ordering Information:To document vaccines administered.Update demographic information and complete at each vaccine administration.Complete all requested information for each vaccine administered.Health Care Provider will maintain <strong>Vaccine</strong> <strong>Administration</strong> <strong>Record</strong> in individual's medical record.This form is to be retained in accordance with the <strong>Record</strong>s Retention and Disposition Schedule of medical recordsas issued by the NC Division of Archives and History.Additional forms may be ordered from:Division of Public Health – <strong>Immunization</strong> <strong>Branch</strong>NC Department of Health and Human Services1917 Mail Service CenterRaleigh, NC 27699-1917Phone (877) 873-6247FAX (800) 544-3058<strong>DHHS</strong> <strong>4041</strong> (2/10)<strong>Immunization</strong> (Review 2/12)