Ready or Not? - Turner Broadcasting
Ready or Not? - Turner Broadcasting
Ready or Not? - Turner Broadcasting
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
Initial 21 CRI Areas as of2004 — Expected to BeFunded in FY 2012Atlanta, GABoston, MAChicago, ILCleveland, OHDallas, TXDenver, CODetroit, MIDistrict of ColumbiaHouston, TXLas Vegas, NVLos Angeles, CAMiami, FLMinneapolis, MNNew Y<strong>or</strong>k City, NYPhiladelphia, PAPhoenix, AZPittsburgh, PASan Diego, CASan Francisco, CASeattle, WASt. Louis, MO15 CRI Areas (Added in2005) At Risk f<strong>or</strong> Eliminationin FY 2012Baltim<strong>or</strong>e, MDCincinnati, OHColumbus, OHIndianapolis, INKansas City, MOMilwaukee, WIOrlando, FLP<strong>or</strong>tland, ORProvidence, RIRiverside, CASacramento, CASan Antonio, TXSan Jose, CATampa, FLVirginia Beach, VA36 CRI Areas (Addedin 2006) At Risk f<strong>or</strong>Elimination in FY 2012Albany, NYAlbuquerque, NMAnch<strong>or</strong>age, AKBaton Rouge, LABillings, MTBirmingham, ALBoise, IDBuffalo, NYBurlington, VTCharleston, WVCharlotte, NCCheyenne, WYColumbia, SCDes Moines, IADover, DEFargo, NDFresno, CAHartf<strong>or</strong>d, CTHonolulu, HIJackson, MSLittle Rock, ARLouisville, KYManchester, NHMemphis, TNNashville, TNNew Haven, CTNew Orleans, LAOklahoma City, OKOmaha, NEPe<strong>or</strong>ia, ILP<strong>or</strong>tland, MERichmond, VASalt Lake City, UTSioux Falls, SDTrenton, NJWichita, KSSource: http://www.rand.<strong>or</strong>g/pubs/technical_rep<strong>or</strong>ts/2009/RAND_TR640.pdf, p. 55-569
B. Public Health Lab<strong>or</strong>at<strong>or</strong>y Response Netw<strong>or</strong>k:Chemical Threat Testing At Risk in All 10 State Labs withAdequate Chemical Capabilities and CapacitiesPublic health labs have shown dramatic progressin the past decade. In 2010, every lab exceptone increased <strong>or</strong> maintained their capability t<strong>or</strong>espond to chemical threats.In addition, the lab<strong>or</strong>at<strong>or</strong>ies created an effectiveand efficient netw<strong>or</strong>k, the Lab<strong>or</strong>at<strong>or</strong>y ResponseNetw<strong>or</strong>k (LRN-c) to respond chemical threats. 14The LRN-c includes:n Nine Level 3 lab<strong>or</strong>at<strong>or</strong>ies, which perf<strong>or</strong>m thebasic functions that all of the LRN labs have— w<strong>or</strong>king with hospitals and other first responderswithin their jurisdiction to maintaincompetency in clinical specimen collection,st<strong>or</strong>age, and shipment; andn Thirty-four Level 2 lab<strong>or</strong>at<strong>or</strong>ies have chemistswho are trained to detect exposure to a numberof toxic chemical agents (analysis of cyanide,nerve agents, and toxic metals in humansamples are examples of Level 2 activities); andn Ten Level 1 lab<strong>or</strong>at<strong>or</strong>ies provide surge capacityto CDC and can detect exposure toan expanded number of chemical agents,including mustard agents, nerve agents andother toxic industrial chemicals. These labsexpand CDC’s ability to analyze large numbersof patient samples when responding tolarge-scale exposure incidents.Above the Level 1 labs are those at CDC and theDepartment of Defense (DOD), which test themost complex and dangerous samples.A rep<strong>or</strong>t released in September 2011 by CDC,Public Health Preparedness: 2011 State-by-State Updateon Lab<strong>or</strong>at<strong>or</strong>y Capabilities and Response ReadinessPlanning, found the most advanced, “Level1” LRN-c labs increased their capabilities byincreasing the number of methods they use t<strong>or</strong>apidly detect chemical agents, from an averageof 6.7 in 2009 to an average of 8.9 in 2010. 15Over the last two years, funding f<strong>or</strong> Level 1chemical labs has been decreased significantly.It is unlikely that states will continue to operatetheir Level 1 chemical labs without sustainedfunding from CDC and cuts to the PHEP cooperativeagreement threaten that funding.The 10 chemical labs currently at Level 1 status,which are at risk if further funding cuts are enactedinclude:n Calif<strong>or</strong>nian Fl<strong>or</strong>idan Massachusettsn Michigann Minnesotan New Mexicon New Y<strong>or</strong>kn South Carolinan Virginian WisconsinIf the chemical testing capabilities are cut fromthese 10 labs, CDC would be the only remainingpublic health lab in the country with this ability.Lab<strong>or</strong>at<strong>or</strong>y Response Netw<strong>or</strong>k f<strong>or</strong> Biological ThreatsIn addition to responding to chemical threat, thelab<strong>or</strong>at<strong>or</strong>ies created an effective and efficientnetw<strong>or</strong>k, the Lab<strong>or</strong>at<strong>or</strong>y Response Netw<strong>or</strong>k(LRN-bio) to respond biological threats.16 TheLRN-bio includes labs with a hierarchy of differentcapabilities, wherein labs with increased capabilitiesprovide supp<strong>or</strong>t f<strong>or</strong> other labs, consisting of:n National lab<strong>or</strong>at<strong>or</strong>ies - including those operatedby CDC, U.S. Army Medical ResearchInstitute f<strong>or</strong> Infectious Diseases (USAMRIID),and the Naval Medical Research Center(NMRC) — are responsible f<strong>or</strong> specializedstrain characterizations, biof<strong>or</strong>ensics, selectagent activity and handling highly infectiousbiological agents;n Reference lab<strong>or</strong>at<strong>or</strong>ies are responsible f<strong>or</strong> investigationand/<strong>or</strong> referral of specimens. They aremade up of m<strong>or</strong>e than 100 state and local publichealth, military, international, veterinary, agriculture,food and water testing lab<strong>or</strong>at<strong>or</strong>ies; andn Sentinel lab<strong>or</strong>at<strong>or</strong>ies, which provide routinediagnostic services, rule-out and referral stepsin the identification process. While theselab<strong>or</strong>at<strong>or</strong>ies may not be equipped to perf<strong>or</strong>mthe same tests as LRN reference lab<strong>or</strong>at<strong>or</strong>ies,they can test samples.10
2011 by the American Public Health Lab<strong>or</strong>at<strong>or</strong>y Association SurveyAcc<strong>or</strong>ding to a survey conducted by APHL inthe fall of 2011 about capabilities from August10, 2010 to August 9, 2011, funding cuts arenegatively impacting the capabilities of manystate public health lab<strong>or</strong>at<strong>or</strong>ies.Cuts to Biological Terr<strong>or</strong>ismPreparedness ActivitiesF<strong>or</strong>ty-four percent of state public health labsrep<strong>or</strong>t being unable to renew service <strong>or</strong> maintenancecontracts f<strong>or</strong> instrumentation, 40 percentrep<strong>or</strong>t losing a full-time staff position and 40percent rep<strong>or</strong>t being unable to attend trainings.Cuts to Chemical Threat ActivitiesThirty percent of state public health rep<strong>or</strong>tedthat budget cuts meant they would be unableto renew service <strong>or</strong> maintenance contracts f<strong>or</strong>some instruments, 29 percent rep<strong>or</strong>t being unableto expand capabilities f<strong>or</strong> new assays <strong>or</strong>tests, 27 percent rep<strong>or</strong>t being unable to hirestaff due to lack of funds, 25 percent rep<strong>or</strong>tbeing unable to purchase critical equipment and23 percent rep<strong>or</strong>t being unable to attend trainingsand conferences.*48 out of 50 states responded to the survey.Sentinel Lab<strong>or</strong>at<strong>or</strong>y Partnerships and OutreachOne of the key components of public health preparednessand response is the ability f<strong>or</strong> lab<strong>or</strong>at<strong>or</strong>iesto quickly and accurately detect and rep<strong>or</strong>tpublic health threats. To ensure that a robust systemis in place, state and local public health lab<strong>or</strong>at<strong>or</strong>iesthat receive CDC Public PHEP cooperativeagreement funding must build strong partnershipswith clinical lab<strong>or</strong>at<strong>or</strong>ies. These relationships assurethat specimens are quickly referred into thepublic health system. The APHL supp<strong>or</strong>ts strongand effective communication and collab<strong>or</strong>ationbetween the public health reference lab<strong>or</strong>at<strong>or</strong>iesand the sentinel clinical lab<strong>or</strong>at<strong>or</strong>ies of the nationalLab<strong>or</strong>at<strong>or</strong>y Response Netw<strong>or</strong>k (LRN). Thesepublic-private partnerships are the foundation f<strong>or</strong> asuccessful system poised to detect the next threat.In fall 2011, APHL conducted a survey of the50 state and Washington, D.C. public healthlab<strong>or</strong>at<strong>or</strong>ies. F<strong>or</strong>ty-eight (94 percent) of lab<strong>or</strong>at<strong>or</strong>iesresponded to this survey and providedthe following inf<strong>or</strong>mation on sentinel lab<strong>or</strong>at<strong>or</strong>ypreparedness and outreach:n F<strong>or</strong>ty-eight state public health lab<strong>or</strong>at<strong>or</strong>ies maintaineda list of m<strong>or</strong>e than four thousand activesentinel clinical lab<strong>or</strong>at<strong>or</strong>ies in their jurisdiction.F<strong>or</strong>ty-one of these lab<strong>or</strong>at<strong>or</strong>ies utilized a rapidmethod, such as the Health Alert Netw<strong>or</strong>k(HAN), blast-email <strong>or</strong> fax, to send messages tosentinel clinical lab<strong>or</strong>at<strong>or</strong>ies. Public health lab<strong>or</strong>at<strong>or</strong>iesalso utilized the same tools to send routineupdates and inf<strong>or</strong>mation on training eventsand drills to these clinical lab<strong>or</strong>at<strong>or</strong>ies.In addition to routine communications with theirsentinel clinical partners, public health lab<strong>or</strong>at<strong>or</strong>iesprovide training on rule-out testing, packagingand shipping and biosafety to thousandsof lab<strong>or</strong>at<strong>or</strong>ians across the US. However, thisoutreach and training is in jeopardy as decliningfunds threaten to reduce personnel, supply andtravel budgets.APHL has established a Sentinel Lab<strong>or</strong>at<strong>or</strong>yPartnerships and Outreach group, comprisedof representatives from state and local publichealth lab<strong>or</strong>at<strong>or</strong>ies, clinical partners such as theAmerican Society f<strong>or</strong> Microbiology (ASM) andthe American Society f<strong>or</strong> Clinical Pathology, andthe CDC, to address the status of sentinel andpublic health lab<strong>or</strong>at<strong>or</strong>y relationships to enhanceoverall preparedness and response to emergingthreats. In the coming year, the group willreview and make recommendations to adopta definition of sentinel clinical lab<strong>or</strong>at<strong>or</strong>ies, developa list of common database elements thatPHEP funded state and local public health LRNreference lab<strong>or</strong>at<strong>or</strong>ies could use to contactsentinel lab<strong>or</strong>at<strong>or</strong>ies in their jurisdiction andfurther articulate the broad role of public healthlab<strong>or</strong>at<strong>or</strong>ies in supp<strong>or</strong>t of the sentinel clinicallab<strong>or</strong>at<strong>or</strong>ies. The m<strong>or</strong>e standardized definitionand contact databases will help public healthlab<strong>or</strong>at<strong>or</strong>ies to perf<strong>or</strong>m m<strong>or</strong>e targeted outreachto sentinel clinical partners.11
EXPERT COMMENTARYSelect Agents and Toxins — Impact ofProposed Regulat<strong>or</strong>y Changes on PublicHealth Lab<strong>or</strong>at<strong>or</strong>iesBy Chris N. Mangal, MPH, Direct<strong>or</strong> of Public Health Preparedness and Response, APHLThe events of September 11, 2001 reinf<strong>or</strong>cedthe need to enhance public health preparednessand response across the United States. Recognizingthis gap, Congress passed the Public HealthSecurity and Bioterr<strong>or</strong>ism Preparedness and ResponseAct of 2002 (“the Bioterr<strong>or</strong>ism ResponseAct” <strong>or</strong> “the Act”) (PL107-188) 17 , which PresidentGe<strong>or</strong>ge W. Bush signed into law on June 12, 2002.In addition to bolstering lab<strong>or</strong>at<strong>or</strong>y preparednessand response capability at CDC and in public healthlab<strong>or</strong>at<strong>or</strong>ies across the United States, the Act alsoaddressed the need to enhance controls on dangerousbiological select agents and toxins (BSAT) agentsby establishing a BSAT list; regulating the possession,transfer and use of BSAT; maintaining databases ofand inspecting facilities that possessed the agents; andscreening personnel with access to such agents. TheAct culminated with the implementation of the finalSelect Agents Regulations (SAR) (42 CFR Part 73, 7CFR Part 331 and 9 CFR Part 121) in April 2005.Since the implementation of the SAR, CDC and theUS Department of Agriculture (USDA) have maintainedthe National Select Agent Registry (NSAR)and have routinely inspected facilities which possessBSAT. Public health lab<strong>or</strong>at<strong>or</strong>ies which possess limitedquantities of biological select agents and toxinsf<strong>or</strong> quality assurance and control purposes are typicallyregulated by the CDC Select Agent Program(SAP). Further, these lab<strong>or</strong>at<strong>or</strong>ies are also regulatedunder Occupational Safety and Hazard Administration(OSHA), National Environmental Lab<strong>or</strong>at<strong>or</strong>yAccreditation Commission (NELAC), Clinical Lab<strong>or</strong>at<strong>or</strong>yImprovement Amendments (CLIA), and theCollege of American Pathologists (CAP).In July 2010, President Barack Obama signed ExecutiveOrder 13546, Optimizing the Security of BiologicalSelect Agents and Toxins in the United States, notingthat the “absence of clearly defined, risk-based securitymeasures in the SAR/SAP has raised concernabout the need f<strong>or</strong> optimized security and f<strong>or</strong> riskmanagement.” 18 The Executive Order directed theSecretaries the Department of Health and HumanServices (HHS) and the USDA to designate a subsetof the select agents and toxins list (Tier 1) thatpresents the greatest risk of deliberate misuse withthe most significant potential f<strong>or</strong> mass casualties <strong>or</strong>devastating effects to the economy, critical infrastructure;<strong>or</strong> public confidence; expl<strong>or</strong>e options f<strong>or</strong>graded protection f<strong>or</strong> these Tier 1 agents and toxinsto permit tail<strong>or</strong>ed risk management practices basedupon relevant contextual fact<strong>or</strong>s; and consider reducingthe overall number of agents and toxins on theselect agents and toxins list. Further, the Order establishedthe Federal Experts Security Advis<strong>or</strong>y Panel(FESAP) to provide advice to the Secretaries on theSelect Agent Program security including:n The composition and potential reduction of theBiological Select Agents and Toxins (BSAT) list,including the development of “Tier 1 agents,”which pose the greatest risk f<strong>or</strong> intentional misusen Measures to enhance reliability of personnelwith access to Tier 1 BSATn Standards f<strong>or</strong> physical and cyber security f<strong>or</strong>facilities possessing Tier 1 BSATn Emerging policy issues relevant to the securityof BSATThe concept of a tiered approach to regulating selectagents and toxins assumes that m<strong>or</strong>e optimizedsecurity measures can be implemented f<strong>or</strong> agentsthat pose a higher risk to public health and safety.However, the proposed changes articulated in theOctober 2011 Federal Register <strong>Not</strong>ice, Possession,Use and Transfer of Select Agents and Toxins; BiennialReview; Proposed Rule, per the Federal Registervolume 76, No. 191, October 3, 2011, 19 does nottake into account the unique role public health labo-12
at<strong>or</strong>ies play in the Lab<strong>or</strong>at<strong>or</strong>y Response Netw<strong>or</strong>k(LRN), a national asset in place to ensure a rapid responseto public health and emerging threats. TheLRN, f<strong>or</strong>med in 1999 through a partnership betweenCDC, the Federal Bureau of Investigation (FBI) andAPHL, is the nation’s premier lab<strong>or</strong>at<strong>or</strong>y netw<strong>or</strong>kserving as a model f<strong>or</strong> all other netw<strong>or</strong>ks, respondingto actual events on a daily basis and continuallyproving its utility during events such as Amerithrax,the H1N1 pandemic, disease outbreaks and naturaldisasters. The true value of the LRN is demonstratedthrough the communications and relationships builtwith clinicians, hospitals, law enf<strong>or</strong>cement, first responderand epidemiology communities. These wellestablished partnerships are the c<strong>or</strong>nerstone that allowsthe LRN to effectively respond to all threats.The proposed changes would adversely impactthe public health lab<strong>or</strong>at<strong>or</strong>ies, which comprise 70percent of the LRN, by jeopardizing the ability ofthese lab<strong>or</strong>at<strong>or</strong>ies to respond to biological threats.In September 2010 20 and again in July 2011 21 , APHLparticipated in meetings of the FESAP to provideinput on the final recommendations issued in theirrep<strong>or</strong>t, Recommendations Concerning the SelectAgent Program released on June 12, 2011. 22 APHLinf<strong>or</strong>med the panel of existing biosecurity practiceswithin state and local public health lab<strong>or</strong>at<strong>or</strong>ies thatcomprise the LRN and the impact of changes to theselect agent regulations on these lab<strong>or</strong>at<strong>or</strong>ies.APHL has publicly commented on the proposedrule, calling f<strong>or</strong>:n Exemption of all LRN reference lab<strong>or</strong>at<strong>or</strong>ies fromthe proposed Tier 1 requirements. APHL encouragedthe Select Agent Program to consider therecommendation from the FESAP, where theynoted: The FESAP recognizes that there are uniquefacilities such as diagnostic, public health, animalhealth, and environmental lab<strong>or</strong>at<strong>or</strong>ies, such as thelab<strong>or</strong>at<strong>or</strong>ies of the Lab<strong>or</strong>at<strong>or</strong>y Response Netw<strong>or</strong>k,which perf<strong>or</strong>m a vital national security function andmay require different methods of implementation ofthe recommended standards. In these instances, theFESAP encourages the Select Agent Program, throughtheir auth<strong>or</strong>ity in Section 4 of E.O. 13546, to “expl<strong>or</strong>eoptions f<strong>or</strong> graded protection of Tier 1 agentsand toxins… to permit tail<strong>or</strong>ed risk managementpractices based upon relevant contextual fact<strong>or</strong>s.”n Representation of local and state public healthlab<strong>or</strong>at<strong>or</strong>ies during the development of codifyingchanges and guidance documents; andn Removal of Bacillus anthracis Pasteur Strain, botulinumneurotoxin, and toxin-producing strainsof Clostridium botulinum from Tier 1 designation.Further, APHL also noted:n Additional costs to comply with the proposedchanges to the rule would adversely impactother critical public health programs that aresupp<strong>or</strong>ted by state and local public health lab<strong>or</strong>at<strong>or</strong>ies,many of which have had to take significantbudget reductions during the past three years.n Public health lab<strong>or</strong>at<strong>or</strong>ies already foster anenvironment of biosafety and biosecurity toprotect against physical and cyber attacks andinsider threats.n Promoting continued exemplary practices of engagingleadership, encouraging teamw<strong>or</strong>k, buildingrelationships with employees and providingethics training has greater value than the use of a“spot in time” personnel reliability program.n Additional requirements f<strong>or</strong> select agents mayresult in some lab<strong>or</strong>at<strong>or</strong>ies abandoning theLRN, resulting in a weakened capability f<strong>or</strong>national response.n Modifying occupational health programs <strong>or</strong> addingpersonnel reliability program requirementswill put further strain, including legal ramificationsf<strong>or</strong> request f<strong>or</strong> health inf<strong>or</strong>mation, onlab<strong>or</strong>at<strong>or</strong>ies already facing w<strong>or</strong>ker sh<strong>or</strong>tages.n Increased biosecurity requirements will bedamaging to public health lab<strong>or</strong>at<strong>or</strong>ies st<strong>or</strong>inglimited quantities of BSAT used during responseto public health emergencies and would compromiselab preparedness and the ability of theUS to detect and respond to threats.APHL continues to monit<strong>or</strong> changes to the SelectAgent Regulations, providing feedback to federalofficials to ensure that public health lab<strong>or</strong>at<strong>or</strong>ies arenot adversely affected and that robust biosecurityand biosafety practices implemented within publichealth lab<strong>or</strong>at<strong>or</strong>ies remain in place to protectagainst public health threats.13
C. Career Epidemiology Field Officer Program: 24 StatesAt Risk to Lose Epidemiology Supp<strong>or</strong>tIn 2002, CDC developed a program to helpstate, territ<strong>or</strong>ial, and local health departmentsstrengthen their epidemiologic capability f<strong>or</strong>public health preparedness and response. TheCareer Epidemiology Field Officer (CEFO) Programassigns CDC epidemiologists at the requestof state, territ<strong>or</strong>ial <strong>or</strong> local health departments.The program has filled a critical gap by establishinga system to assign well trained, highly capableepidemiology staff to provide direct supp<strong>or</strong>tand assistance to health departments. 23All CEFOs have completed CDC’s Epidemic IntelligenceService (EIS) training <strong>or</strong> comparabletraining. Once assigned to a location, CEFOstake on a range of roles:n Developing and strengthening state and localsurveillance systems;n Investigating maj<strong>or</strong> health problems;n Training local staff;n Helping develop local public health emergencyplans and disaster-response exercises;n Co<strong>or</strong>dinating local response to disasters and outbreakswith CDC and other federal agencies; andn Fostering cooperation between emergencyresponders, health care providers and otheragencies involved in disaster response.Over the past decade, CEFOs have played essentialroles in a wide range of incidents. F<strong>or</strong>example, a CEFO assigned in New Y<strong>or</strong>k Cityhelped the city respond in the early stages of theH1N1 flu epidemic, tracking cases among highschool students who had returned from springbreak in Mexico. 24 A CEFO in Kentucky <strong>or</strong>ganizedand led the emergency needs assessmentsf<strong>or</strong> over 7,000 persons in temp<strong>or</strong>ary shelters followingthe 2009 ice st<strong>or</strong>m. The CEFO in N<strong>or</strong>thDakota served as Planning Chief f<strong>or</strong> the state’spublic health emergency response to the 2010Red River flooding. The CEFO in Mississippi establishedsurveillance to monit<strong>or</strong> health effectsin coastal residents following the Gulf oil spill.As of November 2011, the program had 32epidemiologists w<strong>or</strong>king in 24 states. 25 Theprogram is supp<strong>or</strong>ted as part of the PHEP cooperativeagreement. If the President’s proposedcuts to the PHEP cooperative agreement areenacted, states that currently have CEFOs couldlose the supp<strong>or</strong>t, including:n Alabaman Arizonan Calif<strong>or</strong>nian Fl<strong>or</strong>idan Idahon Kentuckyn Mainen Michigann Minnesotan Mississippin Montanan N<strong>or</strong>th Carolinan N<strong>or</strong>th Dakotan Nebraskan Nevadan New Y<strong>or</strong>kn Pennsylvanian South Dakotan Tennesseen Texasn Virginian Vermontn West Virginian Wyoming14
D. Preparedness and Emergency Response LearningCenters: 14 Universities At Risk to Lose Funds fromProposed Elimination of the Training ProgramIn 2010, 14 universities around the country receivedfunding to create Preparedness and EmergencyResponse Learning Centers (PERLCs) tohelp train and educate public health w<strong>or</strong>kers ondisaster preparedness and response. PERLCsare designed to help integrate federal and localdisaster response by educating w<strong>or</strong>kers and officialson federal standards and strategies. 26A number of local public health officials havesaid these programs help fill a crucial gap.“Many people in critical public health rolesdon’t come through with f<strong>or</strong>mal training,” saidthen New Y<strong>or</strong>k State Health Commissioner Dr.Richard F. Daines. “They… desperately needthe supp<strong>or</strong>t of academic training.” 27Some PERLCs are expanding on schools’ existingw<strong>or</strong>k. F<strong>or</strong> instance, at Harvard, the PERLCreplaces the Harvard Center f<strong>or</strong> Public HealthPreparedness, which began in 2002. Over thelast nine years, the center has trained nearly33,000 students and <strong>or</strong>ganized drills and exercisesinvolving m<strong>or</strong>e than 6,000 public healthofficials. 28 Over the past decade, Columbia University’sPERLC, the Columbia Regional LearningCenter (CRLC), has trained 100,000 publichealth w<strong>or</strong>kers across the country. Becausethe center uses online training f<strong>or</strong> many of itsclasses, a significant number of these w<strong>or</strong>kersare outside the school’s immediate area. 29CDC <strong>or</strong>iginally announced that the centerswould be funded f<strong>or</strong> five years. But in the FY2011federal budget, the PERLC budget was reducedby 30 percent. The program is proposed30, 31to be eliminated in 2012.In FY 2011, $13 million in grants were awardedto the 14 institutions listed below, with thegrants totaling approximately $940,000 each. 32The federal funds f<strong>or</strong> these programs are proposedf<strong>or</strong> elimination in 2012:n Columbia University Mailman School of PublicHealth, New Y<strong>or</strong>k, NYn Harvard University School of Public Health,Boston, MAn Johns Hopkins University Bloomberg Schoolof Public Health, Baltim<strong>or</strong>e, MDn Texas A&M School of Rural Public Health,College Station, TXn University at Albany SUNY School of PublicHealth, Albany, NYn University of Alabama School of PublicHealth, Birmingham, ALn University of Arizona College of PublicHealth, Tuscan, AZn University of Illinois, Chicago, Illinoisn University of Iowa College of Public Health,Iowa City, IAn University of Minnesota School of PublicHealth, Minneapolis, MNn University of N<strong>or</strong>th Carolina Gillings Schoolof Global Public Health, Chapel Hill, NCn University of Oklahoma College of PublicHealth, Oklahoma City, OKn University of South Fl<strong>or</strong>ida College of PublicHealth, Tampa, FLn University of Washington School of PublicHealth, Seattle, WA15
E. Preparedness and Emergency Response ResearchCenters: Nine Universities At Risk to Lose Funds fromProposed Elimination of the ProgramOne of the maj<strong>or</strong> ongoing gaps in preparednessis understanding ways to measure standards andcreate perf<strong>or</strong>mance metrics.In 2008 and 2009, CDC awarded $13.6 millionto nine schools of public health around thecountry to help them f<strong>or</strong>m Preparedness andEmergency Response Research Centers (PER-RCs). 33 The goal of these centers is to study keyquestions about how best to respond to disastersand emergencies, and then to translate thatknowledge into practical guidelines that can beadopted by public health departments acrossthe country.Each center is undertaking three <strong>or</strong> four researchprojects, focusing on a different area ofstudy. The research topics, which have beenrecommended by the Institute of Medicine(IOM), include:School Research Pri<strong>or</strong>ity AwardEm<strong>or</strong>y University (Atlanta, GA) Create and maintain sustainable preparedness and $1,562,676response systemsHarvard University (Boston, MA) Generate criteria and metrics to measure effectiveness $1,717,286and efficiencyJohns Hopkins UniversityPreparedness to address the risks of vulnerable populations $1,495,398(Baltim<strong>or</strong>e, MD)University of Calif<strong>or</strong>nia (Berkeley, CA)* Achieve public health and community readiness f<strong>or</strong> today’s $1,506,306challenges and future threatsUniversity of Calif<strong>or</strong>nia*Preparedness and Emergency Response Centers: A public $1,193,365(Los Angeles, CA)health systems approachUniversity of Minnesota (Minneapolis,MN)Enhance the usefulness of training $1,470,307University of N<strong>or</strong>th Carolina(Chapel Hill, NC)University of Pittsburgh (Pittsburgh, PA)Create and maintain sustainable preparedness and responsesystemsCreate and maintain sustainable preparedness and responsesystems and generate criteria and metrics to measureeffectiveness and efficiency$1,695,189$1,701,845University of Washington (Seattle, WA) Improve communications in preparedness and response $1,270,632*Funded FY 2003-2013Source: http://www.cdc.gov/phpr/documents/science/PERRC_Fact_Sheet.pdfSo far, the research has resulted in the publicationof 64 peer-reviewed articles. 34F<strong>or</strong> FY 2011, CDC cut the overall PERRC budgetby approximately 40 percent. 35 The President’sproposed FY 2012 budget completely eliminatesfunding f<strong>or</strong> PERRCs. 36 If Congress passes thisproposal unchanged, none of the nine researchprograms would receive any new federal fundingand the program will be eliminated.16
F. National Center on Environmental Health (NCEH)and Agency f<strong>or</strong> Toxic Substances and Disease Registry(ATSDR) Program: Comprehensive Response Capabilitiesf<strong>or</strong> Nuclear Detonation, Radiological Attacks,Chemical Attacks and Natural Disasters At RiskThe National Center f<strong>or</strong> Environmental Healthand the Agency f<strong>or</strong> Toxic Substances and DiseaseRegistry (NCEH/ATSDR) lead CDC in developingnational, co<strong>or</strong>dinated, science-based responses todeal with the health concerns resulting from environmentalthreats. Environmental health threatscomprised eight out of 15 “all-hazard” planningscenarios that were released in 2005 f<strong>or</strong> use in national,federal, state and local homeland securitypreparedness activities including:n Nuclear detonation;n Radiological attacks <strong>or</strong> accidents;n Chemical attacks <strong>or</strong> accidents, including blisteragents, toxic industrial chemicals, nerveagents and chl<strong>or</strong>ine explosions; andn Natural disasters, including maj<strong>or</strong> earthquakesand hurricanes. 37These scenarios were “designed to be the foundationalstructure f<strong>or</strong> the development of nationalpreparedness standards from whichhomeland security capabilities can be measuredbecause they represent threats <strong>or</strong> hazards of nationalsignificance with high consequence.” 38Additionally, natural disasters to date havecaused m<strong>or</strong>e fatalities and destruction in theUnited States than any others.In FY 2011, NCEH received around $2.7 millionto supp<strong>or</strong>t emergency preparedness and responseactivities. In addition, in FY 2011, NCEHreceived $3.5 million in supp<strong>or</strong>t from CDC’s Officeof Public Health Preparedness and Response(OPHPR) f<strong>or</strong> activities related to radiologicalemergency preparedness and response and $2.3million from OPHPR f<strong>or</strong> maintaining and enhancingCDC radiological lab<strong>or</strong>at<strong>or</strong>y capacity t<strong>or</strong>espond to a radiological <strong>or</strong> nuclear emergency.NCEH/ATSDR has led CDC’s response to thepublic health challenges of diverse environmentalemergencies. These include the DeepwaterH<strong>or</strong>izon oil spill, the Fukushima nuclear powerplant disaster, and every hurricane response includingmaj<strong>or</strong> disasters such as Katrina (2005)and Gustav and Ike (2008).With cuts proposedto CDC’s preparedness activities in the FY 2012President’s budget, the agency would need topri<strong>or</strong>itize where internal resources should be targeted.CDC officials have indicated that supp<strong>or</strong>tf<strong>or</strong> preparedness activities at NCEH/ATSDR, likesupp<strong>or</strong>t f<strong>or</strong> other CDC preparedness programsaddressing infectious diseases, mass trauma, andother threats, could be eliminated in <strong>or</strong>der toprovide sufficient resources to other pri<strong>or</strong>ities.Without these funds, CDC would have limitedcapability to assist all 50 states and Washington,D.C. in the response to natural disasters <strong>or</strong> withincidents involving toxic substance releases <strong>or</strong> radiologicalexposures through contamination assessments,field investigations and issuing expertguidance on protective actions.In addition, if the approximately 1.7 million inpreparedness funding f<strong>or</strong> poison center surveillancewas cut, it would mean:n All national surveillance eff<strong>or</strong>ts f<strong>or</strong> chemicaland radiological exposures and illness wouldstop (there is currently no alternative systemavailable which could replace this);n NCEH-CDC would no longer be able tohon<strong>or</strong> requests f<strong>or</strong> assistance from otherDepartments, including DHS, and Agencies,FDA, EPA in particular, with regard to poisoncenter data in a public health emergency;n Maintenance and supp<strong>or</strong>t would cease f<strong>or</strong>the web-based National Poison Control DataSystem (NPDS) services used by state publichealth departments and BioSense agencies;n Maintenance and supp<strong>or</strong>t of PC upload ofdata to NPDS would cease;n NCEH-CDC would lose their unrestricted accessto the national poison center database; andn NCEH-CDC would no longer be able to perf<strong>or</strong>mcustomized, incident-specific surveillancef<strong>or</strong> exposures and illness from a publichealth threats where this has been utilized inthe past such as carbon monoxide poisoningfrom hurricanes, oil exposures from theDeepwater H<strong>or</strong>izon incident, adverse effectsfrom medical countermeasures used duringthe 2011 Japan nuclear incident.17
Officials Voice Concern Over Preparedness Spending CutsIn a September 2011 commentary in the Britishmedical journal The Lancet, Ali S. Khan, M.D.,M.P.H, direct<strong>or</strong> of CDC’s OPHPR, noted thatstate and local health departments had lost m<strong>or</strong>ethan 44,000 jobs between 2008 and 2010. Sincethen, the number as risen to nearly 50,000.Khan wrote that “(s)tates cannot adequatelymeet everyday needs, let alone increased eff<strong>or</strong>tsf<strong>or</strong> emergency incidents that have potential nationalimplications, without reliable, dedicated, <strong>or</strong>sustained federal funding. Because all responsesare initially local, this limitation is the primary vulnerabilityto national preparedness.” 39Khan argued that in the aftermath of the Sept.11, 2001, terr<strong>or</strong>ist attacks and the anthrax attackslater that year, the country realized that itwasn’t properly prepared f<strong>or</strong> such events. Sincethen, federal, state and local governments havetaken imp<strong>or</strong>tant steps to improve their capacityto respond to attacks and disasters: 40n In 2006, Congress passed the Pandemic andAll-Hazards Preparedness Act (PAPHA),which created a comprehensive framew<strong>or</strong>kf<strong>or</strong> dealing with threats;n Increased federal funding helped improve epidemiologicalcapacity, as well as the stockpileof medicines to respond to specific threats,including anthrax, smallpox, tularemia, andsome chemical and nerve agents;n CDC funding expanded the netw<strong>or</strong>k oflab<strong>or</strong>at<strong>or</strong>ies that analyze and diagnosebioterr<strong>or</strong>ism agents as well as naturallyoccurring hazardous microbes; andn CDC now has a cutting-edge emergencyoperations center; 10 years ago, it had only amakeshift center.Khan said that these improvements in preparednesshave helped public health departments’ability to respond to a range of emergencies.He noted that in 2009, CDC and other groupsresponded effectively to the discovery of theH1N1 flu strain, quickly developing a vaccine.He also pointed out that the increased capacityhelps in public health departments’ routine operation.“The US Government is increasingly recognising[sic] that preparedness and c<strong>or</strong>e (routine)investments in public health are synergistic,” hewrote. “Large-scale and unpredictable natural, accidental,<strong>or</strong> intentionally caused disease outbreaksand environmental disasters need many of thesame routine surveillance, lab<strong>or</strong>at<strong>or</strong>y, risk communication,and other c<strong>or</strong>e public health systems.”At the same time, he said, recent funding cuts,driven by the economic crisis as well as politicalconsiderations, have threatened these developments.He noted that a 2009 survey found that35 percent of state epidemiologists rep<strong>or</strong>tedthat they did not have substantial-to-full capacityf<strong>or</strong> an emergency response to a bioterr<strong>or</strong> attack— a 10 percent increase since federal preparednessfunding hit a peak seven years ago. 41In the same issue of The Lancet, two New Y<strong>or</strong>kCity Health Department officials auth<strong>or</strong>ed acommentary on how their agency has improvedits disaster response abilities. 42 Thomas A. Farleyand Isaac Weisfuse, both of the New Y<strong>or</strong>kCity Department of Health and Mental Health(DHMH), write that over the past decade, theagency has taken several key steps. It has:n Created a volunteer Medical Reserve C<strong>or</strong>ps,made up of 9,000 medical professionals, whocan help the city during emergencies;n Established a f<strong>or</strong>mal incident command system,which gives all of the agency’s 6,000 w<strong>or</strong>kersspecific responsibilities during an emergency;n Set up two emergency operations centers at differentsites, in case one is unusable in a disaster; andn Developed an electronic medical surveillancesystem that includes almost all city hospitalemergency departments. 43The auth<strong>or</strong>s single out two areas in which thedisaster community must improve: strategies f<strong>or</strong>cleaning up anthrax from the environment, andhow to most efficiently distribute medicine tolarge populations during a disaster <strong>or</strong> epidemic.In another September commentary in the Journal ofthe American Medical Association, Thomas V. Inglesbyof the Center f<strong>or</strong> Biosecurity of the University ofPittsburg agreed that disaster preparedness hadimproved significantly over the past decade, largelybecause the federal government increased funding. 44He also noted that social media, including Facebookand Twitter, have played a key role in helping boththe public and responders share inf<strong>or</strong>mation quickly.At the same time, he wrote, the disaster responsecommunity must continue to hone itsstrategies and provide adequate funding. 45“Commitment to a stable level of investment indisaster preparedness at the federal, state, andlocal levels is needed,” he wrote. “The gains ofthe last 10 years are now at risk with this decreasedfunding and will be further threatened ifresources continue to decline.” 4618
EXPERT COMMENTARYComponents of a System Put to the Test: A Look atN<strong>or</strong>th Dakota’s Public Health Preparedness SystemBy Tim Wiedrich, Section Chief Emergency Preparedness and Response Section, N<strong>or</strong>th Dakota Department of HealthTo safeguard the public’s health and ensure public safety,N<strong>or</strong>th Dakota has built an integrated preparedness systemthat features six main components. These components are theresult of a strategic approach to preparedness focusing on anall-hazards approach.The investments in public health and preparedness over thelast decade have helped us develop our preparedness systemsand these components. These investments have been criticalf<strong>or</strong> building capabilities and capacity. As the economic situationcontinues to w<strong>or</strong>sen, the potential f<strong>or</strong> further funding cuts couldput these advancements at significant risk.Component 1: Statewide Tactical CommunicationsN<strong>or</strong>th Dakota has a secure and redundant wide-area netw<strong>or</strong>kthat includes a variety of technologies (video conference, data,Voice Over IP, teleconference, web streaming and others) toconnect public health, hospitals, long-term care facilities andemergency medical services (EMS).We also have wireless routers in every hospital and trailer-based(which includes satellites, VHF public safety, VHF repeaters andcell phone repeaters) and kit-based (which includes Satellite-Bganwith data and voice, public safety radios with VHF and commercialwireless with data and voice) communication systems.To truly be prepared, responders must be able to communicatewith each other during public health emergencies. N<strong>or</strong>th Dakotastrategically created flexible communications channels that canbe utilized during any kind of emergency. Through our statewidetactical communications component, everyone involved in publichealth preparedness shares a common operating picture and canstay in contact no matter the emergency.Component 2: Command and ControlThe N<strong>or</strong>th Dakota Department of Health, like most other statehealth departments, has an emergency operations center. Ouroperations center houses a trained staff of 50 personnel whoundergo quarterly training programs. In addition, the departmentis committed to the National Incident Management System(NIMS), which ensures public health proactively w<strong>or</strong>ks withother parts of government, nongovernment <strong>or</strong>ganizations andthe private sect<strong>or</strong> to respond to emergencies.Through our statewide situational awareness, each aspect of anemergency response is integrated and connected; f<strong>or</strong> example,from the vehicle (such as ambulances) and staff staging areas tothe sending facility to the receiving facility. Every part of the staff,patient, transp<strong>or</strong>tation and destination is tracked step by stepthrough command and control.N<strong>or</strong>th Dakota has also built a statewide Health Alert Netw<strong>or</strong>k<strong>Not</strong>ification System that ensures public health departments andthe medical community share inf<strong>or</strong>mation rapidly.Our command and control systems allow responders to takeaction on a common operating picture, which is shared throughthe statewide tactical communications, to co<strong>or</strong>dinate operationsamong a variety of different responders in different locations.Component 3: State Medical CacheMuch like the Strategic National Stockpile, N<strong>or</strong>th Dakota has astate medical cache that includes:n Warehouse and delivery;n Pre-hospital stabilization and staging, which include trailerbasedkits that feature ten beds that can surge to 20;n State medical shelters f<strong>or</strong> low acuity patients;n Ancillary medical equipment;n Bus conversion kits, which ensure transp<strong>or</strong>t f<strong>or</strong> wheelchairsand stretchers; andn Tent sheltering.Our state’s warehouse and delivery system is a 23,000 square footfacility that houses medical supplies, pharmaceuticals, wrap-aroundsupplies and equipment and other public health emergency essentials.The entire cache is standardized, palletized and deliverable bycargo. Supplies and equipment are <strong>or</strong>dered by medical and publichealth providers through an online <strong>or</strong>dering process.We can quickly transp<strong>or</strong>t medicines, materials and people acrossthe state during an emergency through our state medical cache.Component 4: Just-in-Time TrainingN<strong>or</strong>th Dakota has the ability to reach out to the medical communityand distribute educational inf<strong>or</strong>mation and rapidly teachthem techniques and inf<strong>or</strong>mation they need using our just-intimetraining component. F<strong>or</strong> example, in 2002, the federal governmentinitiated a smallpox vaccination program to inoculatekey medical and public health responders. Because smallpoxvaccination had not been done f<strong>or</strong> several decades, medicalprofessionals were no longer familiar with the technique. Justin-timetraining delivered through a distance learning systemprovided an effective mechanism to rapidly build this capability.The just-in-time distance learning system includes live and archivedweb/video conference capabilities that can be broadcastthrough dedicated wide area netw<strong>or</strong>ks, the public internet andpublic access television.19
The following states’ budgets went down f<strong>or</strong> thesecond year in a row: Col<strong>or</strong>ado, Connecticut,Delaware, D.C., Ge<strong>or</strong>gia, Idaho, Illinois, Iowa,Missouri, Nevada, New Mexico, New Y<strong>or</strong>k, Oklahoma,Oregon and Vermont.The following states’ budget went down f<strong>or</strong> thethird year in a row: Arizona, Calif<strong>or</strong>nia, Kansas,Maryland, Massachusetts, Minnesota, Mississippi,New Jersey, N<strong>or</strong>th Carolina, Pennsylvania,Rhode Island, South Carolina, Utah, Virginiaand Wyoming.Public health funding is discretionary spendingin most states and, theref<strong>or</strong>e, is at high risk f<strong>or</strong>significant cuts during economic downturns.While few states allocate funds directly f<strong>or</strong> publichealth preparedness, state and local funding isessential f<strong>or</strong> supp<strong>or</strong>ting public health infrastructureand c<strong>or</strong>e capacities of health departments.Several states in this analysis that are identifiedas increasing <strong>or</strong> maintaining spending may nothave actually increased their spending on publichealth programs; this can just be a reflectionof how that state rep<strong>or</strong>ts their budget. F<strong>or</strong> instance,some states include federal funding inthe totals <strong>or</strong> public health dollars within healthcare spending totals, such as the state share ofMedicaid <strong>or</strong> mental health expenditures, whichmakes it very difficult to determine “publichealth” as a separate item.F<strong>or</strong> additional inf<strong>or</strong>mation on the methodology of thebudget analysis, please see Appendix B: Data andMethodology f<strong>or</strong> State Public Health Budgets.In September 2011, the Public Health AccreditationBoard (PHAB) launched the first national accreditationprogram f<strong>or</strong> all public health departments. 47The goal of accreditation is to set standards andmeasures f<strong>or</strong> public health departments, includingin key areas related to preparedness.Acc<strong>or</strong>ding to Kaye Bender, RN, PhD, FAAN,President and CEO of the Board, “PHAB’s visionf<strong>or</strong> accreditation is to create a reliable nationalstandard f<strong>or</strong> public health. PHAB supp<strong>or</strong>tshealth departments in achieving this standard byrecognizing the imp<strong>or</strong>tant w<strong>or</strong>k they do and byproviding supp<strong>or</strong>t to improve their services.”Public Health AccreditationIn a time of budget cuts, accreditation can helpdetermine when cuts are having an impact onthe c<strong>or</strong>e standards and capabilities of publichealth departments. “With shrinking budgetsand a growing number of health challenges toaddress, there has never been a m<strong>or</strong>e imp<strong>or</strong>tanttime f<strong>or</strong> public health departments to focus onthe best and most efficient ways to keep peoplehealthy,” acc<strong>or</strong>ding to James Marks, M.D., MPH,Seni<strong>or</strong> Vice President and Direct<strong>or</strong> of the RobertWood Johnson Foundation’s Health Group.22
A recent study conducted by the National Association ofCounty and City Health Officials (NACCHO) found significantcuts to programs, w<strong>or</strong>kf<strong>or</strong>ce and budgets at local health departments(LHDs) around the country.Since 2008, LHDs have lost a total of 34,400 jobs due to layoffsand attrition. 48 Combined state and local public health joblosses total 49,310 since 2008. 49LOCAL HEALTH DEPARTMENTS CUTSLHDs continue to struggle with budget cuts. In July, 2011nearly half of LHDs rep<strong>or</strong>ted reduced budgets, which is in additionto 44 percent that rep<strong>or</strong>ted lower budgets in November2010. 50 In addition, m<strong>or</strong>e than 50 percent of LHDs expect cutsto their budgets in the upcoming fiscal year.City and County Managers Outline Keys To Disaster PreparednessIn September 2011, city and county managers, who overseeand co<strong>or</strong>dinate jurisdiction-wide responses that encompass arange of aspects beyond public health, outlined key aspects ofpreparedness from their perspective at the annual conferenceof the International City/Management Association (ICMA). 51Five panelists who represent different types of communities-– Ron Carlee, COO of the ICMA, who, managed ArlingtonCounty, Virginia, during the September 11 attacks; WilliamFraser, city manager of Montpelier, Vermont; Aden Hogan,city manager of Evans, Col<strong>or</strong>ado, and f<strong>or</strong>mer assistant citymanager of Oklahoma City, Oklahoma during the 1995bombing; Elizabeth Kellar, President and CEO of the Centerf<strong>or</strong> State and Local Government Excellence; and Ken Pulskamp,city manager of Santa Clarita, Calif<strong>or</strong>nia — identifiedthe following key components to effective disaster response:General Planning and Preparation:n Every disaster is local, and local governments should beprepared to respond in partnership with states.n Many communities, especially smaller ones, have difficultyplanning f<strong>or</strong> emergencies. But preparedness is essential.n The first few hours after a disaster are crucial.n Reduce disaster responsibilities to checklists. On the dayof an emergency no one has time to read pages of text.n Have a plan, but be flexible. The disaster rarely plays out exactlyacc<strong>or</strong>ding to the plan. Be prepared to adjust on the fly.n It is impossible to plan f<strong>or</strong> every contingency. Plan f<strong>or</strong>what is probable. A careful plan that activates resourcescan be effective in many contexts.n Have a plan to make use of residents who want to volunteerduring and after the disaster. This can be a key resource.n Collab<strong>or</strong>ation between departments, and between neighb<strong>or</strong>ingjurisdictions, and with state and federal partners,is critical. It is very imp<strong>or</strong>tant to practice joint responsestrategies with these partners.Communication:n During a disaster, frequent communication with the publicis essential.n It is especially crucial to communicate frequently withthe disabled community, as well as with the elderly andpeople with children.n During emergencies, Twitter and other social media toolscan help keep the public inf<strong>or</strong>med.n Especially in smaller communities, disaster response officialsshould be prepared to act as direct communicat<strong>or</strong>swith the public.n It is imp<strong>or</strong>tant to manage not only those affected directlyby the disaster but also the “w<strong>or</strong>ried well” who can eitherhelp <strong>or</strong> hinder a response depending on how theyare supp<strong>or</strong>ted.What Residents Should Know:n Auth<strong>or</strong>ities may not be able to offer help f<strong>or</strong> 72 hours.Residents should know that they may have to rely ontheir own resources f<strong>or</strong> that time; they should know theirneighb<strong>or</strong>s, be able to turn off water and gas lines, and havestockpiles of essential supplies such as food, water and batteries.They should also consider buying a generat<strong>or</strong>.n The public should know to pay close attention to officialwarnings. Often people don’t take these alerts as seriouslyas they should.n Residents should plan f<strong>or</strong> road closings and maj<strong>or</strong> traffic,and should prepare alternate routes to and from home,w<strong>or</strong>k and school.Challenges:n Recent federal, state and local budget cuts have put astrain on local preparedness eff<strong>or</strong>ts to communicate withthe public in a timely manner to mount the most effectiveresponse as well as to engage partners in a co<strong>or</strong>dinated,strategic and as immediate response as possible.23
WMD Commission Rep<strong>or</strong>t Finds United States Vulnerableto Bioterr<strong>or</strong>A new rep<strong>or</strong>t, released October 2011, by theBipartisan Weapons of Mass Destruction (WMD)Terr<strong>or</strong>ism Research Center, headed by f<strong>or</strong>merU.S. Senat<strong>or</strong>s Jim Talent (R-MO) and Bob Graham(D-FL), found the United States is not prepared f<strong>or</strong>a bioterr<strong>or</strong> attack, particularly a large-scale event. 52Eleven of the nation’s top biodefense expertsparticipated in the Bio-Response Rep<strong>or</strong>t Cardand gave different aspects of the responsegrades ranging from Bs to Fs.The higher grades were awarded to the abilityto respond to small-scale non-contagious andcontagious events, but dropped f<strong>or</strong> larger-scale,drug-resistant and global health crises.The lowest grade f<strong>or</strong> capability across all of theresponse scenarios was f<strong>or</strong> “attribution,” whichis the ability to identify the source of the attackwhich is imp<strong>or</strong>tant f<strong>or</strong> determining who is responsiblef<strong>or</strong> the attack and how to halt followupattacks if need be. Communication amongfirst responders and stakeholders received thehighest marks across the types of attacks.The ability to detect and diagnose biological events,the availability and ability to distribute vaccines <strong>or</strong>other medicines, and medical management gradeswere higher f<strong>or</strong> the smaller-scale events and significantlylower f<strong>or</strong> larger-scale events. The overallability of the country to develop and approve vaccinesand drugs received a D.Some of the rep<strong>or</strong>t’s top findings and conclusionsinclude:n “A scientifically and legally validated attributioncapability [the ability to identify the source ofan attack] does not yet exist f<strong>or</strong> anthrax <strong>or</strong> virtuallyany other pathogen <strong>or</strong> toxin.”n The Biomedical Advanced Research andDevelopment Auth<strong>or</strong>ity (BARDA), which encouragesthe private sect<strong>or</strong> to develop countermeasures,is significantly underfunded, andis not spurring necessary innovation.n The country has adequate doses of smallpoxvaccine and antibiotics f<strong>or</strong> anthrax, but it doesn’thave adequate countermeasures f<strong>or</strong> the viral diseasesknown collectively as hem<strong>or</strong>rhagic fevers.n The Department of Health and Human Services(HHS) has not yet developed a set ofgoals f<strong>or</strong> research, product requirements anddispensing countermeasures to civilian populations,and is not co<strong>or</strong>dinating these pri<strong>or</strong>itieswith the Department of Defense.n While the government has built up the StrategicNational Stockpile (SNS), it has not paidenough attention to how it will deliver themedicines during an attack.n The usefulness of BioWatch, which is designedto provide early warning of a bioterr<strong>or</strong>attack, remains unclear.n The country’s health system is not equippedto handle the surge of patients that wouldfollow a large-scale attack. Current surgecapacity may be as much as 50 times belowwhat might be needed.n Very few of the recommendations developedby the federally appointed NationalCommission on Children and Disasters havebeen implemented <strong>or</strong> funded. Childrenrepresent one of the largest vulnerable andspecial needs populations in the U.S.; failureto understand and accommodate specialneeds becomes a crisis in any maj<strong>or</strong> disaster.n Most individual citizens are not preparedf<strong>or</strong> a bioterr<strong>or</strong> attack, and don’t understandbasic medical facts about the most likelybioterr<strong>or</strong> agents.n The government has no plan f<strong>or</strong> cleaningup a large area after an attack with a noncontagiousagent such as anthrax. Whilesmall-scale cleanup plans do exist, they arenot likely to be applicable to a larger area.n The federal government has no plan, andprovides little guidance, on local <strong>or</strong> regionalevacuation following an anthrax attack <strong>or</strong> thedetonation of an improvised nuclear device(IND), among other potential large-scaledisasters.24
A Decade of Public HealthPreparedness3SectionTen years ago, the September 11th and anthrax tragedies clearly demonstratedthat the public health system was not prepared f<strong>or</strong> the range of modernhealth threats we face. Since then, significant investments have resulted in thecountry being much better prepared to respond to public health emergenciesranging from threats of bioterr<strong>or</strong>ism to maj<strong>or</strong> infectious disease outbreaks like apandemic flu to natural disasters like hurricanes, t<strong>or</strong>nadoes and floods. Since 2003,in the annual <strong>Ready</strong> <strong>or</strong> <strong>Not</strong>? Protecting the Public’s Health from Diseases, Disasters, andBioterr<strong>or</strong>ism, TFAH has documented progress and ongoing vulnerabilities in thenation’s ability to respond to health crises.A. Progress in Preparedness since 2001Since 2001, maj<strong>or</strong> investments in improving preparednesshave led to significant improvementsin preparedness planning and co<strong>or</strong>dination;public health lab<strong>or</strong>at<strong>or</strong>ies; vaccine manufacturing;the SNS; pharmaceutical and medicalequipment distribution; surveillance; communications;legal and liability protections; increasingand upgrading staff; and surge capacity.25
Planning andCo<strong>or</strong>dinationPublic HealthLab<strong>or</strong>at<strong>or</strong>iesVaccineManufacturingStrategic NationalStockpile (SNS)Pharmaceuticaland MedicalEquipmentDistributionMAJOR AREAS OF IMPROVEMENTSn In June 2002, Congress passed the Public Health Security and Bioterr<strong>or</strong>ism Response Act of 2002, whichincluded cooperative agreement funding supp<strong>or</strong>t f<strong>or</strong> states around the country. In 2006, Congressreauth<strong>or</strong>ized the legislation as the Pandemic and All-Hazards Preparedness Act (PAPHA). Congress isconsidering reauth<strong>or</strong>ization of the bill in 2011.n Homeland Security Presidential Directive-21 (HSPD-21) was issued in 2007 setting a National Strategy f<strong>or</strong>Public Health and Medical Preparedness.n Creation of the National Health Security Strategy in 2009.n Creation of the IOM F<strong>or</strong>um on Medical and Public Health Preparedness f<strong>or</strong> Catastrophic Events.n All 50 states and Washington, D.C. completed initial bioterr<strong>or</strong>ism response plans by September 2003.n The federal government created a comprehensive National Strategy f<strong>or</strong> Pandemic Influenza, involving allfederal agencies and partners within state and local governments, businesses, and communities around thecountry. President Bush requested and Congress appropriated m<strong>or</strong>e than $6 billion to supp<strong>or</strong>t the nationalstrategy, and another $7.7 billion was provided to help respond to the H1N1 pandemic flu outbreak.n All 50 states and Washington, D.C. developed pandemic flu plans that were reviewed by HHS bef<strong>or</strong>e the2009 outbreak of H1N1. In 2003, only 13 states had pandemic flu plans.n 44 states and Washington, D.C. activated their Emergency Operations Center (EOC) a minimum of twotimes in a year as of 2008.***n 44 states and Washington, D.C. rep<strong>or</strong>ted that pre-identified staff were able to acknowledge notification ofemergency exercises <strong>or</strong> incidents within a target time of 60 minutes at least twice as of 2008.***n 48 states and Washington, D.C. developed at least two After-Action Rep<strong>or</strong>ts/Improvement Plans within60 days of an exercise <strong>or</strong> actual incident as of 2008.***n All 50 states and Washington, D.C. rep<strong>or</strong>ted conducting an emergency preparedness drill <strong>or</strong> exercise thatincluded both the health department and the National Guard as of 2007.n 47 states rep<strong>or</strong>ted having enough staffing capacity to w<strong>or</strong>k five, 12-hour days f<strong>or</strong> six to eight weeks in responseto an infectious disease outbreak, such as novel influenza A H1N1 from August 10, 2009 to August 9, 2010.n 49 states and Washington, D.C. increased <strong>or</strong> maintained their Lab<strong>or</strong>at<strong>or</strong>y Response Netw<strong>or</strong>k f<strong>or</strong> ChemicalThreats (LRN-C) chemical capacity from August 10, 2009 to August 9, 2010. In 2005, only 10 statepublic health labs had adequate chemical terr<strong>or</strong>ism response capabilities.n By 2007, 44 states and Washington, D.C. rep<strong>or</strong>ted sufficient bio-testing capabilities, an increase from 6 in 2003.n In 2007, only one state and Washington, D.C. rep<strong>or</strong>ted their labs did not have the capability to provide24/7 coverage to analyze samples.n By 2006, 47 states rep<strong>or</strong>ted having sufficient numbers of trained scientists to test f<strong>or</strong> possible anthrax andplague, an increase from 10 in 2004.n Congress appropriated billions of dollars through Project BioShield and BARDA to invest in vaccineresearch and development, but there are still limited financial and business incentives f<strong>or</strong> companies topursue research and development.n BARDA awarded a contract to develop the first cell-based flu vaccine, expected in 2014.n The SNS has been substantially upgraded to maintain a variety of critical pharmaceuticals and medicalsupplies including antibiotics, chemical nerve agent antidotes, antiviral drugs, pain management drugs,vaccines f<strong>or</strong> a number of agents, and radiological countermeasures. The SNS is positioned in undisclosedlocations throughout the United States and is configured to provide flexible response strategies.n In advance of the H1N1 outbreak, the SNS contained pandemic flu countermeasures, including 50 millionantiviral treatment courses, 105.8 million N95 respirat<strong>or</strong> masks and 51.7 million surgical masks.n All 50 states and Washington, D.C. have adequate plans to receive and distribute supplies from the SNSbased on a CDC evaluation of planning and management. In 2003, only two states had adequate plansacc<strong>or</strong>ding to CDC.n 47 states and Washington, D.C. increased vaccination rates f<strong>or</strong> seni<strong>or</strong>s against the seasonal flu from 2008to 2009. In 2006, only 38 states increased rates from the year bef<strong>or</strong>e.26
SurveillanceCommunications andCommunity ResiliencyLegal and LiabilityProtectionsIncreasing andUpgrading Staff andVolunteer HealthRespondersMAJOR AREAS OF IMPROVEMENTSn 44 states and Washington, D.C. rep<strong>or</strong>ted using a disease surveillancesystem that is compatible with CDC’s National Electronic Disease SurveillanceSystem (NEDSS), as of 2009. In 2004, only 18 states had diseasesurveillance systems that were NEDSS-compatible.n 43 states and Washington, D.C. can send and/<strong>or</strong> receive electronic healthinf<strong>or</strong>mation with health care providers.**n 40 states and Washington, D.C. have an electronic surveillance systemthat can rep<strong>or</strong>t and exchange inf<strong>or</strong>mation.**n 29 states were able to rapidly identify disease-causing E.coli O157:H7 andsubmit the lab results in 90 percent of cases within four days.***n CDC, in partnership with state and local health agencies, was able toprovide real-time summarized daily data f<strong>or</strong> flu surveillance ahead of thesecond wave of the H1N1 flu outbreak in the fall of 2009.n By w<strong>or</strong>king with state health departments, CDC was able to provideweekly surveillance summaries of oil spill-related health complaints fromthe affected Gulf states following the 2010 Deepwater H<strong>or</strong>izon oil spill.n 25 states and Washington, D.C. mandate all licensed child care facilities tohave a multi-hazard written evacuation and relocation plan.n PAHPA, HSPD-21 and the National Health Security Strategy makecommunity resiliency a top pri<strong>or</strong>ity of preparedness.n The Long-Term Disaster Recovery Group, composed of the Secretariesand Administrat<strong>or</strong>s of m<strong>or</strong>e than 20 federal departments, agencies andoffices, was created in 2009 to strengthen disaster recovery and helpcommunities recover m<strong>or</strong>e quickly and effectively after emergencies.n Every state had adequate statut<strong>or</strong>y auth<strong>or</strong>ity to implement quarantine inresponse to a hypothetical bioterr<strong>or</strong>ism attack as of 2005.n By 2009, at least 33 states had liability protection f<strong>or</strong> entities <strong>or</strong><strong>or</strong>ganizations that provide volunteer assistance during emergencies.n All 50 states and Washington, D.C. met three key criteria f<strong>or</strong> the MedicalReserve C<strong>or</strong>ps (MRC) (having a co<strong>or</strong>dinat<strong>or</strong>, a maj<strong>or</strong>ity of units in thestate meeting incident management guidelines, and the maj<strong>or</strong>ity of unitsare part of a registry). The MRC is a national netw<strong>or</strong>k of communitybasedgroups which engage volunteers to strengthen public healthemergency response and community resilience. In 2007, 13 states didnot meet a minimum threshold f<strong>or</strong> MRC volunteers f<strong>or</strong> every 100,000citizens. In 2008, 16 states did not have MRC co<strong>or</strong>dinat<strong>or</strong>s.Surge Capacity n In 2002, the National Bioterr<strong>or</strong>ism Hospital Preparedness Program —renamed the Hospital Preparedness Program (HPP) in 2006 — wascreated and has provided around $400 million annually to supp<strong>or</strong>t hospitalpreparedness and surge capacity development.n In 2009, the IOM published Guidance f<strong>or</strong> Establishing Crisis Standardsof Care f<strong>or</strong> Use in Disaster Situations: A Letter Rep<strong>or</strong>t, which included afive-step process f<strong>or</strong> emergency planners to follow when developing crisisstandards of care.Source: TFAH’s <strong>Ready</strong> <strong>or</strong> <strong>Not</strong> rep<strong>or</strong>ts, data from 2003-2010.** Source: ASTHO Profile Survey, data from 2010.*** Source: CDC’s Strengthening the Nation’s Emergency Response State by State Rep<strong>or</strong>t, data from 2007-08.27
B. Ongoing Gaps in PreparednessThe United States often takes a band-aidapproach to public health preparedness. Asnew emergencies and concerns emerge andattention shifts, resources are often divertedfrom one pressing pri<strong>or</strong>ity to another, leavingother ongoing areas unaddressed.After September 11th and the anthrax attacks,the federal government made an unprecedentedinvestment to quickly sh<strong>or</strong>e up areas ofpreparedness, which have led to maj<strong>or</strong> improvements.However, it was not at a sufficient levelto backfill long-standing gaps in infrastructure<strong>or</strong> update technologies to meet state-of-the-artstandards to protect the public’s health.There is a new threat to preparedness and consequentlyto the public’s health and safety: thecurrent economic climate and budget cuts at thefederal, state and local level mean that the progressmade over the past decade could be lost.A Funding GapA W<strong>or</strong>kf<strong>or</strong>ce GapMAJOR ONGOING GAPSHist<strong>or</strong>ically, funding f<strong>or</strong> emergencies is often substandard until there is an actualemergency, and then there is a call f<strong>or</strong> emergency supplemental supp<strong>or</strong>t. Thisdynamic means the country is often unprepared to immediately respond duringcrises. The current economic difficulties have led to maj<strong>or</strong> cuts in federal, stateand local supp<strong>or</strong>t f<strong>or</strong> public health and preparedness, leaving Americans m<strong>or</strong>evulnerable during emergencies. The economic impact of a disaster can alsobe m<strong>or</strong>e significant if the community cannot return to n<strong>or</strong>mal after an event.Adequate preparedness allows f<strong>or</strong> a strong and m<strong>or</strong>e timely recovery.n State cuts: 40 states and Washington, D.C. cut funding f<strong>or</strong> public health fromfiscal year (FY) 2009-2010 to 2010-2011, 30 of these states cut funding f<strong>or</strong> asecond year in a row. Acc<strong>or</strong>ding to the Center on Budget and Policy Pri<strong>or</strong>ities(CBPP), states have experienced overall budgetary sh<strong>or</strong>tfalls of $425 billionsince FY 2009. 53n Local cuts: Since 2008, 34,400 local public health jobs have been lost, andin the past year, close to half of all local public health departments rep<strong>or</strong>tedreducing <strong>or</strong> cutting at least one program altogether; 54n Federal cuts: Between FY 2005 and 2011, federal supp<strong>or</strong>t f<strong>or</strong> state and localpublic health preparedness via the PHEP cooperative agreements was also cutby 27 percent. 55 Additional cuts in the President’s proposed FY 2012 budgetwould mean a 37 percent in the PHEP funds from FY 2005 to 2012.There is already a maj<strong>or</strong> sh<strong>or</strong>tage of trained public health w<strong>or</strong>kers and fundedpositions. There are not enough w<strong>or</strong>kers, particularly experts, to effectivelyrespond during public health emergencies. The United States has 50,000 fewerpublic health w<strong>or</strong>kers than it did 20 years ago, and one-third of public healthw<strong>or</strong>kers will be eligible to retire within five years. 56, 57 As baby boomers beginto retire, there is not a new generation of w<strong>or</strong>kers being trained to fill thevoid. Also, under current policies and, in some cases, public health w<strong>or</strong>kersin one area are not allowed to be shifted to help in other areas, even duringemergencies. The recent budget cuts are intensifying the problem, with areduction of 15 percent of the local public health w<strong>or</strong>kf<strong>or</strong>ce since 2008, and,at the same time, health departments around the country are experiencingfurloughs <strong>or</strong> sh<strong>or</strong>tened w<strong>or</strong>k weeks.28
A Surge CapacityGapA Surveillance GapA Gap in CommunityResiliency Supp<strong>or</strong>tGaps in Vaccineand PharmaceuticalResearch,Development, andManufacturingMAJOR ONGOING GAPSIn the event of a maj<strong>or</strong> disease outbreak <strong>or</strong> attack, the health care system isstretched beyond n<strong>or</strong>mal capabilities. Surge capacity, the ability of the medicalsystem to care f<strong>or</strong> a massive influx of patients, remains one of the most seriouschallenges f<strong>or</strong> emergency preparedness. A large-scale disaster also requireshaving enough equipment and appropriate space to treat patients. There arenumerous ongoing surge capacity issues related to response in primary caresettings beyond just hospitals, including crisis standards of care, alternativecare sites, co<strong>or</strong>dinating volunteers to help and providing them with adequateliability protection and regional co<strong>or</strong>dination among health care facilities.The United States still lacks an integrated, national approach to biosurveillance— which would dramatically improve response capabilities ranging from abioterr<strong>or</strong>ism attack to catastrophic disasters to contamination of the foodsupply. There is not a standardized, interoperable system using up-todatetechnology. Currently, there are maj<strong>or</strong> differences in states’ ability tocollect and rep<strong>or</strong>t data, which hampers bioterr<strong>or</strong>ism and disease outbreakidentification and control eff<strong>or</strong>ts. Timeliness in identifying and emerging healththreats can prevent disease and save lives.The ability of public health to w<strong>or</strong>k with communities to cope and recoverfrom a disaster <strong>or</strong> public health emergency is another maj<strong>or</strong> challenge. Itis particularly difficult to address the needs of at-risk, special needs andvulnerable populations, such as children, the elderly, people with underlyinghealth conditions and lower-income communities. The gaps in day-todaypublic health departments, such as enough staff to engage communitymembers in preparedness and limits in cultural competencies, make itchallenging to build and maintain the relationships needed to identify and w<strong>or</strong>kwith vulnerable Americans who need the most help during emergencies.Research and development of medical countermeasures — including diagnostics,antiviral medications and vaccines — is outdated in the United States, in largepart because it is not a particularly profitable venture f<strong>or</strong> pharmaceuticalinvest<strong>or</strong>s. Project BioShield and BARDA were developed to spur innovation andinvestment in medical countermeasures, but, so far, the result of new, effectiveproducts has been limited. The investments made in vaccine research anddevelopment did help lead to the production of a vaccine f<strong>or</strong> the H1N1 flu strainin rec<strong>or</strong>d time, but manufacturers were only able to produce limited quantitiesby the beginning of the flu season because of insufficient capacity and a relianceon an outdated egg-based production strategy.29
C. Preparedness Hist<strong>or</strong>y Timeline, 2001-2011The September 11, 2001 and anthrax attacks revealedsignificant deficiencies in the country’sdisaster preparedness f<strong>or</strong> health emergencies,and led to a paradigm shift in how the governmentand public view disaster readiness. Thefollowing timeline highlights many of the maj<strong>or</strong>public health emergencies and policy and researchevents from the past decade.2001Maj<strong>or</strong> Public Health Emergenciesn September 11 — Al Qaeda terr<strong>or</strong>ists hijackedfour planes and crashed them into the W<strong>or</strong>ldTrade Center, the Pentagon and a field inShanksville, Pennsylvania, killing nearly 3,000people. In the aftermath, public health officialsactivated a range of responses, includingreadying the SNS and providing services,including mental health counseling.n October — A series of anthrax attacks occurred;five people were killed, 17 weresickened and thousands were potentiallyexposed. Public health officials were at thelead of the anthrax response –diagnosing andtreating victims, running m<strong>or</strong>e than a milliontests on hundreds of thousands of potentiallylife-threatening samples, providing usefulguidance to the public to address their fearsand supp<strong>or</strong>ting eff<strong>or</strong>ts to decontaminatepostal facilities and other properties contaminatedwith anthrax sp<strong>or</strong>es.Maj<strong>or</strong> Policy <strong>or</strong> Research Eventsn March -– CDC released a new rep<strong>or</strong>t, PublicHealth Infrastructure — A Status Rep<strong>or</strong>t, in thewake of the tragedies, that concluded theU.S. public health infrastructure “is still structurallyweak in nearly every area.” 58n September — President Ge<strong>or</strong>ge W. Bush appointedGov. Tom Ridge as the direct<strong>or</strong> ofthe new Office of Homeland Security withinthe White House. 59n October — The USA Patriot Act became law,expanding definitions and discretion of lawenf<strong>or</strong>cement to investigate and prevent domesticand international terr<strong>or</strong>ism.2002Maj<strong>or</strong> Public Health Emergenciesn Spring/Summer — Public health officialsaround the country developed strategies f<strong>or</strong>responding to the continuing spread of theWest Nile Virus (WNV) — in 2002, the virusspread to nearly every state while m<strong>or</strong>e than4,000 Americans developed West Nile Virusand 284 died from the illness. 60 The WNVresponse helped inf<strong>or</strong>m future disease trackingand containment approaches.n Fall — Severe acute respirat<strong>or</strong>y syndrome(SARS) first emerged in Foshan City, GuangdongProvince, China. 61 Chinese officials<strong>or</strong>iginally withheld inf<strong>or</strong>mation about theoutbreak. The disease was later identified tobe a new c<strong>or</strong>onavirus. There were no existingvaccines f<strong>or</strong> the disease and treatmentsdid not offer a clear benefit. The full impactof SARS would not be recognized until 2003.n October -– Pilgrim’s Pride recalled over 27million pounds of frozen and prepared poultryproducts after Listeria was found at a processingplant. Eight people died, 53 becameseriously ill and three women had miscarriages<strong>or</strong>62, 63stillbirths.Maj<strong>or</strong> Policy and Research Eventsn January — HHS announced $1.1 billion infunding f<strong>or</strong> state public health, hospital andmedical preparedness planning f<strong>or</strong> a bioterr<strong>or</strong>istevent. 64n June -– The Public Health Security and Bioterr<strong>or</strong>ismAct became law. It provided guidanceto public health officials, created the AssistantSecretary f<strong>or</strong> Public Health Emergency Preparednessand the National Disaster MedicalSystem and provided cooperative agreementgrant funds to states f<strong>or</strong> public health emergencypreparedness, including:s The HPP, which is designed to help hospitalsrespond m<strong>or</strong>e effectively to bioterr<strong>or</strong>attacks and other public health emergenciessuch as pandemic flu outbreaks. HPPprovides money f<strong>or</strong> hospitals to buy medication,medical supplies, communicationsequipment and other resources that canhelp during an emergency. 65s PHEP, which provides money to states, territ<strong>or</strong>iesand urban areas to improve publichealth lab testing, health surveillance, training,planning and other aspects of disasterresponse. PHEP currently gives out 62 grantsa year to the 50 states, four large metropolitanareas (Chicago, Los Angeles County, NewY<strong>or</strong>k City and Washington, D.C.) and eightU.S. territ<strong>or</strong>ies and freely associated states. 6630
n November -– The Homeland Security Act becamelaw, creating the Department of HomelandSecurity (DHS), which inc<strong>or</strong>p<strong>or</strong>ated anumber of existing federal agencies, includingthe Customs Service, the Coast Guard and67, 68the Secret Service.n November — The MRC was established to helpcommunities respond to disasters. Communitybasedunits made up of volunteers now existacross the country, ready to be activated whennecessary. As of 2011, there are m<strong>or</strong>e than 950units, with m<strong>or</strong>e than 200,000 volunteers. 69n November — Then-U.S. Senate Maj<strong>or</strong>ityLeader Bill Frist, MD, auth<strong>or</strong>ed an analysis inHealth Affairs that concluded that “over thepast two decades, the [nation’s public health]infrastructure has greatly deteri<strong>or</strong>ated.” 702003Maj<strong>or</strong> Public Health Emergenciesn March — The W<strong>or</strong>ld Health Organization(WHO) issued a global alert f<strong>or</strong> SARS and WHOand CDC issued travel alerts f<strong>or</strong> Vietnam, Chinaand Hong Kong. 71 In April, CDC issued a travelalert f<strong>or</strong> T<strong>or</strong>onto, which was the center of theoutbreak in Canada. A week later the agencylifted the T<strong>or</strong>onto alert. 72 CDC issued anothertravel alert f<strong>or</strong> T<strong>or</strong>onto in April that was soonlifted. SARS proved to be highly contagious onlyin hospitals, so the spread of the virus was able tobe controlled by isolation of the sick and otherpublic health interventions. 73 In July, WHOannounced that SARS’ chain of transmissionhad been broken. 74 Overall, m<strong>or</strong>e than 8,400people were infected with SARS, and m<strong>or</strong>e than800 died. The disease spread to 29 countries.In the United States, there were 33 confirmed75, 76cases. None of these patients died.n June — There were 37 confirmed cases of themonkeypox virus in Midwestern states. Therewere no fatalities, but two children were hospitalized,one with encephalitis. The illness isin the same family of viruses as smallpox, althoughits symptoms are generally milder. Investigat<strong>or</strong>straced the outbreak to pet prairiedogs, which had contracted it from rodents77, 78imp<strong>or</strong>ted from Africa.nn October — A Hepatitis A outbreak began,which was linked to contaminated green onionsand caused m<strong>or</strong>e than 600 illnesses andfour deaths. The onions were served in salsaand a cheese dip at a Chi-Chi’s restaurantoutside Pittsburgh. Investigat<strong>or</strong>s traced the79, 80onions to farms in Mexico.December -– The first case of Mad Cow disease(bovine spongif<strong>or</strong>m encephalopathy (BSE)) wasdiscovered in the United States. The UnitedStates Department of Agriculture (USDA)began widespread testing. After detecting veryfew cases, it scaled back testing in 2006. 81Maj<strong>or</strong> Policy and Research Eventsn January — CDC launched a national campaignto vaccinate 500,000 emergency andmedical w<strong>or</strong>kers on a voluntary basis againstsmallpox. The disease was eradicated in the1970s, but officials were concerned that terr<strong>or</strong>istscould get samples and use them as abioweapon. Fewer than 40,000 medical andemergency personnel — less than 10 percentof the campaign’s goal — received the shots.Acc<strong>or</strong>ding to a GAO rep<strong>or</strong>t, many healthw<strong>or</strong>kers were concerned about the healthrisks of vaccination. 82n March — The previously existing NationalPharmaceutical Stockpile was expanded bythe Homeland Security Act to become theSNS, a national reposit<strong>or</strong>y of antibiotics,chemical antidotes and other medicines andmedical supplies f<strong>or</strong> use during a chemical<strong>or</strong> biological terr<strong>or</strong> attack, <strong>or</strong> other publichealth emergency. 83n April — A GAO rep<strong>or</strong>t examining state andlocal preparedness progress found deficienciesin capacity, communication and co<strong>or</strong>dinationelements essential to preparednessand response, including w<strong>or</strong>kf<strong>or</strong>ce sh<strong>or</strong>tages,inadequacies in disease surveillance and lab<strong>or</strong>at<strong>or</strong>iesand a lack of regional co<strong>or</strong>dinationand compatible communications systems. 84n September — CDC launched BioSense, anationwide system to detect early signs of abioterr<strong>or</strong>ism attack <strong>or</strong> infectious disease outbreak.Initially, BioSense focused solely onbioterr<strong>or</strong> attacks, but it expanded over time tocover a range of threats, such as Dengue feverand health problems related to the Gulf OilSpill. The netw<strong>or</strong>k receives inf<strong>or</strong>mation froma wide range of sources across the country:nearly 2,000 government and private hospitalsand healthcare facilities, almost 2,800 lab<strong>or</strong>at<strong>or</strong>iesand m<strong>or</strong>e than 49,00085, 86pharmacies.n October — DHS launched BioWatch, a monit<strong>or</strong>ingsystem that tests air samples f<strong>or</strong> biologicalagents. As of 2011, there are sens<strong>or</strong>sin m<strong>or</strong>e than 30 cities around the country,monit<strong>or</strong>ing six maj<strong>or</strong> biological threats, includinganthrax. 8731
n November — The IOM published the Futureof the Public’s Health in the 21st Centuryrep<strong>or</strong>t, which found that the public healthsystem had: “vulnerable and outdated healthinf<strong>or</strong>mation systems and technologies; aninadequately trained public health w<strong>or</strong>kf<strong>or</strong>ce;antiquated lab<strong>or</strong>at<strong>or</strong>y capacity; a lackof real-time surveillance and epidemiologicalsystems; ineffective and fragmented communicationsnetw<strong>or</strong>ks; incomplete domesticpreparedness and emergency response capabilities;and communities without accessto essential public health services.” Overall,the rep<strong>or</strong>t concluded that, “[t]hese problemsleave the nation’s health vulnerable — andnot only to exotic germs and bioterr<strong>or</strong>ism.” 88n December — The White House issued HomelandSecurity Presidential Directive-8 (HSPD-8), which established new requirements f<strong>or</strong>national preparedness. HSPD-8 assignedDHS the lion’s share of responsibility f<strong>or</strong><strong>or</strong>ganizing the federal preparedness eff<strong>or</strong>t.The directive also established the NationalPreparedness Goal, Universal Task List andTarget Capabilities List (TCL) to serve asbaseline capabilities necessary f<strong>or</strong> all aspectsof preparedness, from prevention to recovery.HSPD-8 was the first in a series of HomelandSecurity Presidential Directives relatedto bioterr<strong>or</strong>ism and public health preparednessissued between 2002 and 2009. 89n December — F<strong>or</strong> the first time, every stateand Washington, D.C. were recognized f<strong>or</strong>having CDC-approved bioterr<strong>or</strong>ism and publichealth emergency plans. 902004Maj<strong>or</strong> Public Health Emergenciesn February — Ricin, a highly toxic protein madefrom the cast<strong>or</strong> bean that is poisonous if inhaled,injected <strong>or</strong> ingested, was detected in aU.S. Senate mailroom serving the office of Maj<strong>or</strong>ityLeader Bill Frist, MD. No illnesses wererep<strong>or</strong>ted in the mailroom <strong>or</strong> in Sen. Frist’s office.91 News rep<strong>or</strong>ts said it was unclear howthe ricin was delivered and approximately 16people underwent decontamination. An investigationinto the incident is still open.n March — The New Y<strong>or</strong>k Times rep<strong>or</strong>ts on a Pentagonrep<strong>or</strong>t, Lessons Learned from the AnthraxAttacks: Implications f<strong>or</strong> U.S. Bioterr<strong>or</strong>ism Preparedness,which was written in 2002 but notpreviously publicly released. The article describedthe rep<strong>or</strong>t as “a sweeping assessment[that] identifies weaknesses in ‘almost every aspectof U.S. biopreparedness and response.’” 92n May — A Salmonella outbreak linked to rawalmonds sickened at least 29 people in 12states, leading to the recall of 13 million93, 94pounds of the nuts.n July — Tomatoes contaminated with Salmonellacaused m<strong>or</strong>e than 400 illnesses in ninestates. Investigat<strong>or</strong>s traced the problem topre-sliced tomatoes served at a chain of convenience95, 96st<strong>or</strong>es.n Fall — A series of powerful hurricanes hitFl<strong>or</strong>ida. In response, the U.S. Public HealthService sent nearly 500 members of the CommissionedC<strong>or</strong>ps, a unif<strong>or</strong>med service of8,500 public health professional who are ableto help during national and internationalhealth emergencies and offer aid. 97n October — The United States faced a flu vaccinesh<strong>or</strong>tage, when the Chiron C<strong>or</strong>p<strong>or</strong>ation announcedit would not be able to meet demandf<strong>or</strong> its flu vaccine after problems at a Britishplant halted production of millions of doses. 98The sh<strong>or</strong>tage highlighted gaps in vaccine researchand development in the United States.n October — the w<strong>or</strong>ldwide death toll fromH5N1 avian influenza reached 32 in Asia, triggeringconcerns of the potential of new pandemicflu outbreak. 99 As of 2011, H5N1 stillposes a potential threat and is being trackedby researchers.Maj<strong>or</strong> Policy and Research Eventsn April — President Bush signed a classified directive,Biodefense f<strong>or</strong> the 21st Century, to improveco<strong>or</strong>dination among the government’sbioterr<strong>or</strong>ism programs and initiatives. 100n July — Project BioShield became law. BioShieldis a $5.6 billion eff<strong>or</strong>t to encourage biotech andpharmaceutical companies to develop productsthat will help treat <strong>or</strong> prevent the effects ofa chemical <strong>or</strong> biological terr<strong>or</strong> attack. In 2007,BioShield became part of BARDA.n September — CRI was created, to help citiesand large metropolitan areas prepare todispense medicine quickly, on a large scale.From 2004 to 2010, CRI expanded from 21 to72 cities and metropolitan areas. 1012005Maj<strong>or</strong> Public Health Emergenciesn July — Tomatoes contaminated with Salmonellasickened 29 people in 16 states. Health officialstraced the problem to a pair of Virginia farms. 10232
n August and September — Two powerful hurricanes,Katrina and Rita, hit the Gulf Coast. Thest<strong>or</strong>ms killed approximately 1,900 people andcaused m<strong>or</strong>e than $100 billion in damage.103In response, the Commissioned C<strong>or</strong>ps carriedout the largest deployment in its hist<strong>or</strong>y, deployingsome 2,119 C<strong>or</strong>ps officers to the regionbetween August 26 and November 7. Ofthese officers, 81 percent served on teams thatprovided healthcare and other services directlyto the affected communities, while 19 percentserved on emergency response teams <strong>or</strong> at104, 105local operations centers.n September — A second maj<strong>or</strong> Salmonella outbreakoccurred — m<strong>or</strong>e than 80 people weresickened after eating tomatoes at a chain restaurant.Investigat<strong>or</strong>s identified the source toa farm in Fl<strong>or</strong>ida. Twenty-six people overallwere hospitalized. 106Maj<strong>or</strong> Policy and Research Eventsn September — As part of HSPD-8, DHS released15 National Planning Scenarios tohelp federal, state and local officials and theprivate sect<strong>or</strong> develop better responses f<strong>or</strong> arange of emergencies. 107The 15 National PlanningScenarios:n Four biological attacks: aerosol anthrax,plague, contamination of ground beef at afact<strong>or</strong>y and Foot and Mouth Disease;n Four chemical attacks: a blister agent, thenerve agent sarin, a toxic industrial chemicalrelease and a chl<strong>or</strong>ine tank explosion;n The detonation of a 10-kiloton nuclear bomb;n A “dirty bomb” that spreads radiationthroughout a city;n The bombing of a sp<strong>or</strong>ts arena;n A cyber attack that damages the nation’sfinancial infrastructure; andn Three natural events: an 8.0 earthquake near amaj<strong>or</strong> city, a Categ<strong>or</strong>y 5 hurricane that strikesa maj<strong>or</strong> city and a pandemic flu outbreak.n November — President Bush released a $7.1billion plan, the National Strategy f<strong>or</strong> PandemicInfluenza, to guide the “nation’s preparednessand response to an influenza pandemic, withthe intent of (1) stopping, slowing <strong>or</strong> otherwiselimiting the spread of a pandemic tothe United States; (2) limiting the domesticspread of a pandemic, and mitigating disease,suffering and death; and (3) sustaininginfrastructure and mitigating impact to theeconomy and the functioning of society.” 1082006Maj<strong>or</strong> Public Health Emergenciesn March — A cow in Alabama tested positivef<strong>or</strong> Mad Cow Disease. 109, 110 The cow was notlinked to a larger outbreak.n Summer and Early Fall — Nearly 200 peoplebecame sick and at least three died due to E.111, 112, 113coli contamination in spinach.n July to November — Two Salmonella outbreaksoccurred, both linked to contaminated tomatoes.The first one took place in 19 states, whilethe second occurred in 21 states and Canada.Overall, m<strong>or</strong>e than 300 people were sickened.Investigat<strong>or</strong>s found that one outbreak was relatedto tomatoes consumed in restaurants, butcould not determine the source of the contamination.In the second case, investigat<strong>or</strong>s tracedthe problem to a single restaurant, which had receivedits tomatoes from an Ohio packinghousethat had been supplied by three growers. 114n August — Between August 1, 2006 and February16, 2007, Salmonella-tainted peanut butterfrom the Peter Pan and Great Value brandssickened 425 people in 44 states. After an investigation,the manufacturer, ConAgra, saidmoisture from leaks and a faulty sprinkler systemlikely led to the115, 116, 117problem.n November and December — M<strong>or</strong>e than 70people who ate at Taco Bell restaurants in theN<strong>or</strong>theast were infected with E.coli bacteria.Three-quarters of these people were hospitalizedand eight developed a type of kidney failureknown as hemolytic-uremic syndrome. Atfirst, Taco Bell traced the problem to greenonions, but FDA investigat<strong>or</strong>s later ruled outthat possibility. Officials eventually determinedthat lettuce was the likely118, 119source.n December — Five school-aged children inRhode Island were diagnosed with encephalitis,an acute inflammation of the brain. Oneof the children died. The health departmentdistributed antibiotics to all students, staff,and family members from the affected school.In early January of 2007, public health auth<strong>or</strong>itiesalso closed three nearby school districtsas a precautionary measure. The Departmentof Health was able to rapidly distribute antibioticsto m<strong>or</strong>e than 1,000120, 121people.33
34Maj<strong>or</strong> Policy and Research Eventsn July — The Unif<strong>or</strong>m Emergency VolunteerHealth Practitioners Act (UEVHPA) is adoptedby the National Conference of Commissionerson Unif<strong>or</strong>m State Laws (NCCUSL) to addressthe lack of unif<strong>or</strong>mity in state laws that wererevealed during the maj<strong>or</strong> hurricanes in 2005,especially focused on the use and efficacy ofvolunteers and licensing and accreditation, liabilityprotection and w<strong>or</strong>kers compensation. 122n December — The Pandemic and All-HazardsPreparedness Act (PAHPA) becamelaw. PAHPA reauth<strong>or</strong>ized several expiringprograms in the Public Health Security andBioterr<strong>or</strong>ism Act, and established some newauth<strong>or</strong>ities. 123 It broadened the government’sfocus from bioterr<strong>or</strong>ism to a m<strong>or</strong>e comprehensive,all-hazards approach that includedinfectious diseases and natural disasters,as well as chemical, nuclear, <strong>or</strong> radiologicalterr<strong>or</strong> attack. It also placed HHS as thelead agency f<strong>or</strong> the public health and medicalresponse to a public health emergencyand created BARDA within HHS to distributefunding f<strong>or</strong> the development of medicalcountermeasures. BARDA has funded about100 projects, including anthrax vaccines andantitoxins, radiation treatments and vaccinesf<strong>or</strong> smallpox and influenza. 124, 125 As part ofPAHPA, Congress also created the Officeof the Assistant Secretary f<strong>or</strong> Preparednessand Response (ASPR), within HHS. ASPRfocuses on preparedness planning and response,federal emergency medical capability,countermeasures research and improvinghospital and health care disaster response. 1262007Maj<strong>or</strong> Public Health Emergenciesn May — CDC announced that a patient with suspectedextensively drug resistant- Tuberculosis(XDR-TB), which is spread through the air traveledto Europe and back, prompting an internationalpublic health scare. The patient didnot turn out to have the disease, but problemsin the response raised concerns among publichealth experts about preparedness f<strong>or</strong> managinga real multidrug resistant TB patient. 127n June — Lead paint was found on a range oftoys made in China, posing a significant publichealth threat. Over several months, millionsof products were recalled. 128n August — The Interstate 35W bridge collapsedin Minneapolis during the evening rush houron August 1, leaving 13 people dead and m<strong>or</strong>ethan 100 injured. 129 Minneapolis May<strong>or</strong> R.T.Rybak attributed a quick emergency responseto the city’s investment of some $50 millionsince 2001 in emergency preparedness, specifically,enhanced communication technology. 130n October — Calif<strong>or</strong>nia saw the largest evacuationin state hist<strong>or</strong>y due to a series of wildfiresthat caused 10 deaths and 139 injuries andf<strong>or</strong>ced evacuation of approximately 350,000homes. The Calif<strong>or</strong>nia Department of PublicHealth deployed 2,000 alternate care sitebeds that had been purchased by the state toimprove the emergency preparedness capabilities.The department also co<strong>or</strong>dinated evacuationsfrom 23 nursing homes, two acute carefacilities and a psychiatric hospital. 131n September — Concerns about the H5N1 birdflu as a potential pandemic threat continued togrow as m<strong>or</strong>e than 200 cumulative human deaths132, 133had been linked to H5N1 at this time.n September — E.coli contamination in frozenhamburger meat prompted the third largesthamburger recall in USDA hist<strong>or</strong>y. Nearly22 million pounds of meat were recalled; the134, 135product caused 40 illnesses in eight states.n October — CDC rep<strong>or</strong>ted that methicillin-resistantStaphylococcus aureus (MRSA), whichcan cause Staph infections, was responsiblef<strong>or</strong> m<strong>or</strong>e than 94,000 serious infections andnearly 19,000 deaths each year. CDC identifiedMRSA as “a maj<strong>or</strong> public health problemprimarily related to health care, but no longerconfined to intensive care units, acute carehospitals, <strong>or</strong> any health care institution.” 136Maj<strong>or</strong> Policy and Research Eventsn October — The White House updated the NationalStrategy f<strong>or</strong> Homeland Security f<strong>or</strong> the firsttime since September 11, 2001 and also issuedthe Homeland Security Presidential Directive21 (HSPD 21), which established a NationalStrategy f<strong>or</strong> Public Health and Medical Preparedness.137 The directive was the most recent ina series of executive <strong>or</strong>ders issued since September11, 2001 to protect the nation in theevent of terr<strong>or</strong>ist attacks <strong>or</strong> other catastrophichealth events. The directive included four keyparts: biosurveillance, countermeasure distribution,mass casualty care and community resilience.138 The strategy included many of therequirements set f<strong>or</strong>th in PAHPA and affirmsthe imp<strong>or</strong>tance of the all-hazards approachto public health emergency preparedness.In addition, it established the Public Healthand Medical Preparedness Task F<strong>or</strong>ce and requiredthe Task F<strong>or</strong>ce to submit yearly statusrep<strong>or</strong>ts on the implementation plan and suggestedchanges to HSPD 21.
“Indeed, certain non-terr<strong>or</strong>ist events that reach catastrophiclevels can have significant implications f<strong>or</strong>homeland security. The resulting national consequencesand possible cascading effects from theseevents might present potential <strong>or</strong> perceived vulnerabilitiesthat could be exploited, possibly eroding citizens’confidence in our nation’s government and ultimatelyincreasing our vulnerability to attack. This strategy,theref<strong>or</strong>e, recognizes that effective preparation f<strong>or</strong> catastrophicnatural disasters and man-made disasters,while not homeland security per se, can neverthelessincrease the security of the homeland.” 139n National Strategy f<strong>or</strong> Homeland Security, October 2007n December — Congress created the NationalCommission on Children and Disasters to addressthe unique needs of children during acrisis. The Commission issued its final rep<strong>or</strong>tin October 2010, which included recommendationsf<strong>or</strong> a National Strategy on Childrenand Disasters, establishing permanent children’sand disaster co<strong>or</strong>dination offices, fundingdisaster planning f<strong>or</strong> schools and childcare facilities and purchasing child-appropriatesupplies f<strong>or</strong> shelters and hospitals. 1402008Maj<strong>or</strong> Public Health Emergenciesn January — A measles outbreak occurred inSan Diego after a seven-year-old who hadnever been vaccinated f<strong>or</strong> measles traveled toSwitzerland and returned with a case of measles.He spread the disease to 11 other children,none of whom had been vaccinated. 141n January to April — The city of Chicago had10 cases of Group C meningococcal invasivedisease, which is best known as a causef<strong>or</strong> meningitis — compared with 13 casesin all of 2007. The Chicago Department ofPublic Health launched a mass vaccinationcampaign focused on the at-risk population— children aged 11 to 18. The city was ableto vaccinate 7,213 children in two weeks. 142n February — In the largest beef recall in hist<strong>or</strong>y,143 million pounds of beef were deemed unfitf<strong>or</strong> human consumption. The recall occurredafter the Humane Society of the United Statesreleased an undercover video showing w<strong>or</strong>kersat a Calif<strong>or</strong>nia meat company kicking sick cowsand using f<strong>or</strong>klifts to f<strong>or</strong>ce them to walk. 143n February — Vials of ricin were found in amotel room in Las Vegas, Nevada after a mansuffering from respirat<strong>or</strong>y distress was taken tothe hospital. 144 Acc<strong>or</strong>ding to news rep<strong>or</strong>ts, theman said he had the ricin f<strong>or</strong> his “self-defense.”n March — Salmonella in cantaloupes imp<strong>or</strong>tedfrom a Honduran grower and packer waslinked to 50 illnesses in 16 states, as well asnine illnesses in Canada. 145n March — A Salmonella outbreak in Col<strong>or</strong>adowas linked to the water supply. 146n March and June — Heavy rains caused severeflooding in the Midwest. In March, 17 peopledied as a result of the flooding, and, by theend of June, st<strong>or</strong>ms and flooding across sixstates caused 24 deaths, 148 injuries and m<strong>or</strong>ethan $1.5 billion in damages to Iowa alone. 147n June — Outbreaks of Salmonella Saintpaulwere linked first to tomatoes, and then,months later, to jalapeño and Serrano peppers.CDC identified m<strong>or</strong>e than 1,442 peoplewho were sickened by the outbreak in 43states, the District of Columbia and Canada. 148n June — Lightning sparked thousands of wildfiresacross n<strong>or</strong>thern Calif<strong>or</strong>nia. M<strong>or</strong>e than2,700 individual fires were rec<strong>or</strong>ded, causingmandat<strong>or</strong>y evacuations and damaging thousandsof acres. 149n September — Hurricane Gustav caused widespreaddestruction in Louisiana, amountingto billions of dollars in damages. Two weeksafter Gustav, Hurricane Ike hit Texas as aCateg<strong>or</strong>y 2 st<strong>or</strong>m, causing extreme damagein the state. Twenty-seven deaths were attributedto the st<strong>or</strong>m, which f<strong>or</strong>ced hundreds ofthousands of residents to evacuate. 150n September — Melamine-contaminated infantf<strong>or</strong>mula and related dairy productsproduced in China were found in countriesacross the globe. 151n November — Federal health officials begantracking cases of Salmonella linked to taintedpeanut butter products. 152 Over the next fourmonths, investigat<strong>or</strong>s tracked the problem totwo peanut butter plants owned by the PeanutC<strong>or</strong>p<strong>or</strong>ation of America. The outbreakkilled eight people and sickened m<strong>or</strong>e than700 in 46 states. 153Maj<strong>or</strong> Policy and Research Eventsn February — CDC released its first rep<strong>or</strong>tfeaturing state-by-state inf<strong>or</strong>mation on theprogress states have made using PHEP grantfunding, Public Health Preparedness: MobilizingState by State. 154 Some key areas of progressincluded increases in the number of epidemiologistsand labs with bio-testing capabilitiesand improvements in the ability to distributevaccines and antiviral medications.35
36n Fall — The w<strong>or</strong>ld economic crisis began,which has led to a continuing wave of publichealth budget cuts and w<strong>or</strong>ker layoffs. Between2008 and 2011, LHDs cut about 34,000jobs — almost a fifth of the entire local publichealth w<strong>or</strong>kf<strong>or</strong>ce. 1552009Maj<strong>or</strong> Public Health Emergenciesn January — A severe ice st<strong>or</strong>m struck Kentucky,and m<strong>or</strong>e than 85 percent of the state’s countieswere declared disaster areas. Immediatelyafter the st<strong>or</strong>m, approximately 800,000residential and commercial units lost power,including numerous hospitals and long-termcare facilities. At the height of the response,m<strong>or</strong>e than 200 shelters in 72 counties providedassistance to m<strong>or</strong>e than 7,800 people.In the largest statewide call-up ever, over 4,100National Guard members helped respond. 156n March — An outbreak of H1N1, a novel fluvirus, is identified in Veracruz, Mexico. OnApril 26, officials from CDC and DHS declareda national public health emergencyas cases of H1N1 began to spread across thecountry. In June, WHO and CDC classifiedthe outbreak as a pandemic. Hundreds ofschools across the United States closed inthe initial weeks of the H1N1 outbreak. Althoughit was viewed as a relatively moderatepandemic, the H1N1 virus had a serious impacton the United States. It infected around20 percent of Americans (approximately60 million people), leading to approximately274,000 hospitalizations and 12,000deaths.157 About 90 percent of the Americanswho died were under the age of 65, includingat least 340 children, as confirmed bylab<strong>or</strong>at<strong>or</strong>y testing. 158 Acc<strong>or</strong>ding to CDC, theactual number of deaths in children could bebetween 910 and 1,880. 159Maj<strong>or</strong> Policy and Research Eventsn June — In response to the H1N1 outbreak,Congress passed and President Obamasigned the Supplemental AppropriationsAct of 2009, appropriating $1.9 billion inemergency supplemental funding and anadditional $5.8 billion in contingency funding.160 These funds helped enhance vaccineproduction capacity, purchase and distributevaccines, upgrade surveillance capabilities,supp<strong>or</strong>t the state and local pandemic responseand meet other needs.n September — The IOM released Guidance f<strong>or</strong>Establishing Crisis Standards of Care f<strong>or</strong> Use inDisaster Situations, which provided guidanceto stakeholders to develop health care protocolswhen resources are scarce, includingtaking into account ethics, community engagement,legal auth<strong>or</strong>ities, clear indicat<strong>or</strong>sand evidence-based clinical processes. 161n December — HHS released the NationalHealth Security Strategy to help galvanize eff<strong>or</strong>tsto minimize the health consequencesassociated with significant health incidents.The strategy is built on a foundation of communityresilience. 1622010Maj<strong>or</strong> Public Health Emergenciesn January and February — M<strong>or</strong>e than 1.3 millionpounds of salami tainted with Salmonellawere recalled after m<strong>or</strong>e than 250 people in44 states became ill. Federal officials said theproblem may have been related to black andred pepper coating the meat. 163n April — The Deepwater H<strong>or</strong>izon oil platf<strong>or</strong>mexploded on the Gulf Coast, resulting in thedeaths of 11 w<strong>or</strong>kers and the release of an estimated205 million barrels of oil into the Gulf. 164,165In response to the oil spill, with fundingfrom the Substance Abuse and Mental HealthServices Agency, CDC designed the Gulf StatesPopulation Survey to collect the data needed toassess the mental and behavi<strong>or</strong>al health needsof the affected population. Data collectionbegan in December 2010 and will conclude inDecember 2011. The complete public healthimpact of the explosion, spill, and dispersantson the safety of seafood, health of recoveryw<strong>or</strong>kers, and psychological wellbeing of GulfCoast residents remains unknown. 166n May — An outbreak of Salmonella linked toeggs caused m<strong>or</strong>e than 1,900 illnesses. Thesource of the problem was traced to two largeegg farms in Iowa. Eventually, m<strong>or</strong>e than 500million eggs were recalled. FDA officials investigatingthe farms found a wide range ofhealth violations, including rodents, maggotsand improperly st<strong>or</strong>ed manure. 167n June — Calif<strong>or</strong>nia public health officials declareda Pertussis, also known as whoopingcough, epidemic in the state. Over the courseof the year, the epidemic caused almost 8,000illnesses and 10 deaths and was the largest epidemicin the state in half a century. 168 Pertussisvaccinations are recommended beginning attwo months old, but infants are not fully protecteduntil they reach six months of age andhave received a series of shots. Officials attributedthe epidemic to gaps in vaccinations.
Maj<strong>or</strong> Policy and Research Eventsn August — The President’s Council of Advis<strong>or</strong>son Science and Technology (PCAST) issued:Rep<strong>or</strong>t to the President on Reengineering the InfluenzaVaccine Production Enterprise to Meet theChallenges of Pandemic Influenza. The rep<strong>or</strong>tfound that the response to the H1N1 outbreakwas “impeded by unanticipated delays that arosein manufacturing what was supposed to be themost powerful tool f<strong>or</strong> preventing widespreadm<strong>or</strong>bidity and m<strong>or</strong>tality: a vaccine designed toprotect against the 2009 H1N1 virus.” 169 Therep<strong>or</strong>t featured a series of recommendations toenhance the nation’s ability to produce influenzavaccine in a timelier manner.n August — HHS released a Public Health EmergencyMedical Countermeasures Review, PublicHealth Emergency Countermeasures Review:Transf<strong>or</strong>ming the Enterprise to Meet Long-RangeNational Needs, a strategy to modernize the developmentof medical countermeasures acrossthe federal government, including addressingissues related to bureaucracy and profitabilityto help encourage private industry investmentin the development of vaccines and othermedical countermeasures. 1702011Maj<strong>or</strong> Public Health Emergenciesn March — On March 11, 2011, n<strong>or</strong>thern Japansuffered first a magnitude 9.0 earthquake centered130 miles off the eastern coast and thenan ensuing tsunami. At the Fukushima Daiichinuclear react<strong>or</strong> complex, this caused a cascadeof events including loss of electrical power to essentialcooling systems, react<strong>or</strong> overheating andc<strong>or</strong>e meltdown, and radionuclide releases causingwidespread radioactive contamination ofresidential areas, agricultural land, and coastalwaters. The Fukushima nuclear emergencyresponse identified maj<strong>or</strong> public health andmedical challenges in both Japan and in theUnited States; challenges in the U.S., includedthe need to identify potential contaminationin food, water, and on returning travelers andcargo imp<strong>or</strong>ted from Japan, as well as to protectthe health of Americans in Japan.n May — A series of t<strong>or</strong>nadoes in Southern andCentral states resulted in m<strong>or</strong>e than $7 billionin damages and m<strong>or</strong>e than 140 deaths inJoplin, Missouri. 171n July — The first cases of illness associated withListeria-tainted cantaloupes were rep<strong>or</strong>ted.The outbreak has sickened m<strong>or</strong>e than 139people in 28 states, killing 30 of them, as ofDecember 14, 2011, making it the deadliestfoodb<strong>or</strong>ne outbreak since 1924. Investigat<strong>or</strong>straced the outbreak to a Col<strong>or</strong>ado farm. Officialssaid this was the first known outbreakof Listeria in cantaloupe. 172n August — Hurricane Irene lead to 56 deaths,$10 to $25 billion in damages, including massiveflooding in Vermont. The st<strong>or</strong>m resultedin nearly six million Americans losing electricityand maj<strong>or</strong> transp<strong>or</strong>tation shut downs. 173n August — A multistate outbreak of Salmonellawas traced to ground turkey, sickening m<strong>or</strong>ethan 136 people in 31 states and one death. 174n October — A Halloween n<strong>or</strong>’easter becamethe 14th natural multi-billion dollar naturaldisaster in the United States in 2011, causingat least six deaths and transp<strong>or</strong>tation shutdowns and millions to lose electricity on theEast coast. 175n November — A Salmonella outbreak lined toboiled chicken livers sickened m<strong>or</strong>e than 179people in six states. 176Maj<strong>or</strong> Policy and Research Eventsn January — The FDA Food Safety ModernizationAct became law, giving the agency expandedpowers to protect the nation’s food supply.The law, which made the first maj<strong>or</strong> changesto the country’s food safety system in 80 years,included auth<strong>or</strong>ization of $1.4 billion in fundingover five years and a focus on prevention offoodb<strong>or</strong>ne illness, rather than response alone.Among the maj<strong>or</strong> changes, f<strong>or</strong> the first time,FDA could <strong>or</strong>der recalls of contaminated food.Previously, the agency had to w<strong>or</strong>k with companiesto engineer voluntary recalls. 177n March — President Obama issued PresidentialPolicy Directive-8 (PPD-8), the latest in aseries of policy directives since September 11,2001, which laid out the country’s approach topreparing f<strong>or</strong> acts of terr<strong>or</strong>ism, cyber attacks,disease outbreaks and natural disasters. 178 Aspart of PPD-8, DHS released an updated NationalPreparedness Goal (NPG) in September2011 to improve both local and nationaldisaster response. The top level summary ofthe goal is “to have a secure and resilient Nationwith the capabilities required across thewhole community to prevent, protect against,mitigate, respond to, and recover from thethreats and hazards that pose the greatestrisk.” 179 Additional requirements of the directiveinclude: a National Preparedness SystemDescription; a series of National Framew<strong>or</strong>ksand Federal Interagency Operational Plans;a National Preparedness Rep<strong>or</strong>t; and a Campaignto Build and Sustain Preparedness.37
n September — The Public Health AccreditationBoard launched the first nationalaccreditation program f<strong>or</strong> public health departments,initiated and supp<strong>or</strong>ted by theRobert Wood Johnson Foundation (RWJF)and CDC, to protect and improve Americans’health by advancing the quality and perf<strong>or</strong>manceof all of the nation’s public health departments—state,local, territ<strong>or</strong>ial and tribal.n September — CDC released a new 10-year NationalStrategic Plan f<strong>or</strong> Public Health Preparednessand Response. 180 The plan builds on theexperience the agency has had after a decadeof maj<strong>or</strong> public health emergencies, includingthe 2001 terr<strong>or</strong>ist attacks, Hurricane Katrinaand the H1N1 flu pandemic. The planincludes strategies to cooperate with state andlocal emergency management and healthdepartments, the private sect<strong>or</strong> and international<strong>or</strong>ganizations. It also identifies bestpractices f<strong>or</strong> co<strong>or</strong>dination between publichealth departments, emergency managementgroups and the healthcare system. In addition,it proposes methods to strengthen thesurveillance of threats; improve epidemiologyand lab<strong>or</strong>at<strong>or</strong>y science related to disasters;generate m<strong>or</strong>e ideas f<strong>or</strong> improving trainingand efficient use of funds; increase the waysto improve cooperation and co<strong>or</strong>dinationacross the federal government and amongfederal, state and local agencies; and developimprovements f<strong>or</strong> evaluating progress.2011 CDC Strategic Preparedness Plan EightOverarching Objectives:n Objective 1: Prevent and/<strong>or</strong> mitigate threatsto the public’s healthn Objective 2: Integrate public health, the healthcaresystem and emergency managementn Objective 3: Promote resilient individuals andcommunitiesn Objective 4: Advance surveillance, epidemiologyand lab<strong>or</strong>at<strong>or</strong>y science and service practicen Objective 5: Increase the application of scienceto preparedness and response practicen Objective 6: Strengthen public preparednessand response infrastructuren Objective 7: Enhance stewardship of publichealth preparedness fundsn Objective 8: Improve the ability of the publichealth w<strong>or</strong>kf<strong>or</strong>ce to respond to health threats“These are challenging economic times. We must sustain existing public health capabilities and infrastructurewhile developing solutions to build the public health systems of the future. Looking aheadtowards the year 2020, projected pressures on public health include the increase of the U.S. populationfrom 308 million to 336 million, m<strong>or</strong>e diversified age groups (including a 54% increase of citizensover 65, straining the already overburdened health care system), socio-economic tensions, and massmigrations due to adverse weather events. We also know that the advancement and diffusion of scientifictechnologies will pose threats to health security. Improvements in DNA technologies will increaseour vulnerability to attacks from groups who have adapted microbes <strong>or</strong> created entirely new pathogenswith the intent to harm the population. We also face the risk of individuals acting on their own, combiningreadily available chemicals and other materials to create improvised weapons. The increasingease of global mobility means that bio-attacks, pandemics, and other health threats to our citizenscan m<strong>or</strong>e easily travel across b<strong>or</strong>ders. Vigilance and f<strong>or</strong>ecasting are necessary to mitigate these scenariosand can only be done by sustaining and increasing public health capabilities.” 181— Ali S. Khan, M.D., M.P.H., U.S. Assistant Surgeon General (Ret), Direct<strong>or</strong>, Office of PublicHealth Preparedness and Response, DHHS/CDC from the National Strategy38
Maj<strong>or</strong> CDC and ASPR Public Health Preparedness Programs, 2011U.S. Centers f<strong>or</strong> Disease Control andPreventionn Office of Public Health Preparedness andResponse: Leads the agency’s preparednessand response activities by providing strategicdirection, supp<strong>or</strong>t, and co<strong>or</strong>dination f<strong>or</strong>activities across CDC as well as withlocal, state, tribal, national, territ<strong>or</strong>ial andinternational public health partners. 182s The Public Health EmergencyPreparedness (PHEP) cooperativeagreement program awards funds tostates, territ<strong>or</strong>ies and urban areas to buildand sustain public health preparednesscapabilities that enhance their ability t<strong>or</strong>espond to public health emergencies.PHEP awards funds to 62 public healthdepartments nationwide, including the50 states; four large metropolitan areas,Chicago, Los Angeles County, New Y<strong>or</strong>kCity and Washington, D.C.; and eight U.S.territ<strong>or</strong>ies and freely associated states:American Samoa, Guam, U.S. VirginIslands, N<strong>or</strong>thern Mariana Islands, PuertoRico, Federated States of Micronesia,Republic of the Marshall Islands and theRepublic of Palau. 183 The distribution ofPHEP funds is calculated using a f<strong>or</strong>mulathat includes a base amount f<strong>or</strong> eachawardee plus population-based funding.Funding also is awarded f<strong>or</strong> specificpreparedness activities. The fiscal year2011 cooperative agreement includes anew pilot program that provides a yearof funding to 10 urban areas to developassessments of public health and medicalrisks, as well as accelerated developmentof risk reduction strategies that mitigatethe public health risks associated withhigher population areas. 184The 2011 PHEP cooperative agreement focuseson 15 key capability areas, including:n Community Preparednessn Community Recoveryn Emergency Operations Co<strong>or</strong>dinationn Emergency Public Inf<strong>or</strong>mation and Warningn Fatality Managementn Inf<strong>or</strong>mation Sharingn Mass Caren Medical Countermeasure Dispensingn Medical Material Management and Distributionn Medical Surgen Non-pharmaceutical Interventionsn Public Health Lab<strong>or</strong>at<strong>or</strong>y Testingn Public Health Surveillance and EpidemiologicalInvestigationn Responder Safety and Healthn Volunteer Managementn CRI is funded through the PHEP cooperativeagreement to help cities and large metropolitanareas prepare to dispense medicine quickly, ona large scale. 185n The SNS is a national reposit<strong>or</strong>y of antibiotics,chemical antidotes and other medicines andmedical supplies f<strong>or</strong> use during a chemical <strong>or</strong> biologicalterr<strong>or</strong> attack, <strong>or</strong> other public health emergency.Started in 1999, SNS is managed throughOPHPR. The program focuses on respondingquickly to a large-scale bioterr<strong>or</strong> attack in a largecity <strong>or</strong> metropolitan area (where m<strong>or</strong>e than halfof the country’s population lives). The first lineof supp<strong>or</strong>t is “12-hour Push Packages,” whichcontain over 50 tons of medicines, antidotes andmedical supplies designed to provide rapid immediatehelp, even when the cause of an attack<strong>or</strong> event is uncertain. Push Packages are keptin secure warehouses across the country, readyf<strong>or</strong> rapid deployment to a designated city <strong>or</strong> site.SNS also has further supplies, designed to arrivewithin 24 to 26 hours, if necessary. 186Examples of SNS Contents (as of 2009)n Enough smallpox vaccine to protect 300 million people, <strong>or</strong> every man, woman and child in America;n Over 41 million regimens of countermeasures against anthrax;n Therapeutic anthrax antitoxins to treat symptomatic patients; 187n 10 million anthrax vaccine (AVA) doses; andn Countermeasures to address radiation exposure including 475,000 combined doses of Calcium-DTPA(Diethylenetriamine pentaacetate) and Zinc-DTPA. 18839
Office of the Assistant Secretary of Preparedness and Responsen Office of Policy and Planning (OPP) advisesHHS and ASPR leadership through policyoptions and strategic planning initiatives tosupp<strong>or</strong>t domestic and international publichealth emergency preparedness and responseactivities.n Office of Preparedness and Emergency Operationsoversees a range of operational programs,three of which include:s Hospital Preparedness Program, whichprovides leadership and funding throughgrants and cooperative agreements to states,territ<strong>or</strong>ies and eligible municipalities to improvesurge capacity and enhance communityand hospital preparedness f<strong>or</strong> public healthemergencies.189 HPP provides supp<strong>or</strong>t f<strong>or</strong>hospitals to buy medication, medical supplies,communications equipment and otherresources that can help during an emergency.The program helps hospitals improve decontaminationcapabilities and personnel managementand hospital evacuation planning.It also pays f<strong>or</strong> disaster training and helpslocal netw<strong>or</strong>ks of hospitals — as well as localbusinesses and non-profit groups — w<strong>or</strong>ktogether to plan f<strong>or</strong> emergencies.A 2009 HHS evaluation found that m<strong>or</strong>ethan three quarters of hospitals participatingin HPP met at least 90 percent of all measuresf<strong>or</strong> preparedness. 190s National Disaster Medical System(NDMS), a federally co<strong>or</strong>dinated systemthat augments the nation’s medical responsecapability, which consists of m<strong>or</strong>e than 100teams of trained doct<strong>or</strong>s, nurses and othermedical professionals to help respond tomaj<strong>or</strong> emergencies, and co<strong>or</strong>dinates patienttransp<strong>or</strong>t and hospital care.191 M<strong>or</strong>e than1,000 hospitals participate in NDMS. Basedthroughout the country, these teams arebrought to the disaster site to provide arange of services, including medical assessments,primary and emergency medical care,provision of medical equipment and supplies,victim identification and veterinary services. 192s Emergency System f<strong>or</strong> Advance Registrationof Volunteer Health Professionals(ESAR-VHP), a federal program created tosupp<strong>or</strong>t states and territ<strong>or</strong>ies in establishingstandardized volunteer registration programsf<strong>or</strong> disasters and public health and medicalemergencies. The program, administered onthe state level, verifies health professionals’identification and credentials so that they canrespond m<strong>or</strong>e quickly when disaster strikes.By registering through ESAR-VHP, volunteers’identities, licenses, credentials, accreditationsand hospital privileges are all verifiedin advance, saving valuable time in emergencysituations. 193n BARDA encourages the development of vaccines,medicines and diagnostic tools thatcould be used in public health emergencies.Established in 2006 by PAHPA, BARDAw<strong>or</strong>ks to speed up the development of medicalcountermeasures (MCMs) by supp<strong>or</strong>tingadvanced research, development and testing,w<strong>or</strong>king with manufacturers and regulat<strong>or</strong>s,and helping companies devise large-scalemanufacturing strategies. BARDA bridges thefunding gap between early research and commercialproduction.In 2011, BARDA has m<strong>or</strong>e than 100 ongoingprojects, including potential vaccines f<strong>or</strong>smallpox, anthrax, influenza and radiation treatments.194In addition, the program is involvedin helping to open the nation’s first cell-based fluvaccine fact<strong>or</strong>y. 195s Project BioShield, a program within BARDA,was set up to guarantee a market f<strong>or</strong> newlydeveloped vaccines and medicines needed f<strong>or</strong>biodefense that would not otherwise have a196, 197commercial market.40
MEMORANDUM OF UNDERSTANDING FOR EMERGENCY PREPAREDNESSGRANT COORDINATIONSeveral federal departments and agenciesdistribute preparedness funds and/<strong>or</strong> providetechnical assistance and national strategies insupp<strong>or</strong>t of various preparedness activities.ASPR, CDC, the Health Resources and ServicesAdministration (HRSA), the Departmentof Homeland Security’s Federal EmergencyManagement Agency (FEMA), and the Departmentof Transp<strong>or</strong>tation’s (DOT) NationalHighway Transp<strong>or</strong>tation Safety Administration(NHTSA) recently agreed through amem<strong>or</strong>andum of understanding (MOU) tocooperatively assess their current preparednessgrant programs and to engage in collab<strong>or</strong>ativeeff<strong>or</strong>ts to improve interagency grantco<strong>or</strong>dination. The MOU establishes a f<strong>or</strong>malframew<strong>or</strong>k that supp<strong>or</strong>ts joint federal planningdesigned to focus investments, measureand improve preparedness outcomes, reduceduplication, rep<strong>or</strong>t results, and enhance returnon investment. 198Acc<strong>or</strong>ding to the agreement, seni<strong>or</strong> leadersfrom each agency involved will participate inthe Interagency Grant Co<strong>or</strong>dination Committeeas well as the Grant Co<strong>or</strong>dination W<strong>or</strong>kingGroup. The Committee and W<strong>or</strong>kingGroup will w<strong>or</strong>k to co<strong>or</strong>dinate grants in thefollowing areas:1) Grant Program Policies to co<strong>or</strong>dinatepolicy guidance and documents, includingassuring consistency of grant guidance withnational emergency preparedness strategiesand pri<strong>or</strong>ities.2) Grant Cycle/Timeline to align the following:pre-award administration eff<strong>or</strong>ts; programmaticfiscal years; joint application submissions;and application reviews.3) Grant Administration/Management to co<strong>or</strong>dinatethe use of the grant funding f<strong>or</strong>administration activities such as site visits;inf<strong>or</strong>mation sharing; co-presentation at nationalconferences/meetings; and co<strong>or</strong>dinationof programmatic supp<strong>or</strong>t.4) Grant Rep<strong>or</strong>ting Mechanisms and Evaluationto develop tools and resources to co<strong>or</strong>dinategrant program perf<strong>or</strong>mance measures. 199CDC and ASPR have made significant progressin grant alignment, including improvingco<strong>or</strong>dination between HPP and PHEP cooperativeagreements. The HPP-PHEP collab<strong>or</strong>ationis w<strong>or</strong>king to improve capabilities,evaluation, framew<strong>or</strong>k, IT systems, trainingand technical assistance, grants administrationand policy and guidance development. Goalsf<strong>or</strong> the HPP-PHEP collab<strong>or</strong>ation are to:n Have a joint HPP-PHEP funding opp<strong>or</strong>tunityannouncement in 2012;n Reduce awardee burden, including duringthe application process;n Increase programmatic impact of state andlocal preparedness programs; andn Improve federal efficiencies to better supp<strong>or</strong>tstate and local preparedness programs.41
ALL-HAZARDS APPROACH TO EMERGENCY PUBLIC HEALTH THREATSThe U.S. public health system is responsible f<strong>or</strong> protecting the American people from a range ofpotential health threats.EXAMPLES OF MAJOR EMERGENCY PUBLIC HEALTH THREATSAgroterr<strong>or</strong>ism: The “…deliberate introductionof an animal <strong>or</strong> plant disease with the goalof generating fear, causing economic losses, and/<strong>or</strong> undermining stability.” 200 Agroterr<strong>or</strong>ism canbe considered a subcateg<strong>or</strong>y of “bioterr<strong>or</strong>ism”and foodb<strong>or</strong>ne diseases.Bioterr<strong>or</strong>ism: The intentional <strong>or</strong> deliberate useof germs, biotoxins, <strong>or</strong> other biological agentsthat cause disease <strong>or</strong> death in people, animals,<strong>or</strong> plants. Examples include anthrax, smallpox,botulism, Salmonella, and E. coli.Blast Injuries: Explosions, whether deliberate <strong>or</strong>accidental, can cause multi-system, life threateninginjuries among individuals and within crowds. Inaddition, blunt and penetrating injuries to multiple<strong>or</strong>gan systems are likely when an explosion occursand unique injuries to the lungs and central nervoussystem occur during explosions.Chemical terr<strong>or</strong>ism: The deliberate use ofchemical agents, such as poisonous gases, arsenic,<strong>or</strong> pesticides that have toxic effects on people, animals,<strong>or</strong> plants in <strong>or</strong>der to cause illness <strong>or</strong> death.Examples include ricin, sarin, and mustard gas.Chemical incidents and accidents: Thenon-deliberate exposure of humans to harmfulchemical agents, with similar outcomes tochemical terr<strong>or</strong>ism.Foodb<strong>or</strong>ne diseases: Food-b<strong>or</strong>ne illness iscaused by harmful bacteria, viruses, parasites <strong>or</strong>chemicals that are found in food and beveragesand enter the body through the gastrointestinaltract. CDC estimates there are approximately76 million pathogen-induced cases of food-b<strong>or</strong>nediseases each year in the United States, causingapproximately 127,000 hospitalizations and3,000 deaths. Examples include botulism, Salmonella,E.coli 0157:H7, shigella, and n<strong>or</strong>ovirus.Natural disasters: Harm can be inflicted duringand after natural disasters, which can lead to contaminatedwater, sh<strong>or</strong>tages of food and water,loss of shelter, and the disruption of regularhealth care. Examples include hurricanes, earthquakes,t<strong>or</strong>nados, mudslides, fires, and tsunamis.Pandemic flu: A novel, potentially lethal strainof the influenza against which humans have nonatural immunity. The H1N1 flu was the firstpandemic flu of the 21st century. Hist<strong>or</strong>ically,pandemic flu occurs two to three times everyhundred years <strong>or</strong> so. In the 20th century thew<strong>or</strong>ld experienced the 1918, 1957/58, and 1968pandemic flu, although the severity of the diseasevaried greatly among them.Radiological threats: Intentional <strong>or</strong> accidentalexposure to radiological material. F<strong>or</strong> example,a terr<strong>or</strong>ist attack could involve the scattering ofradioactive materials through the use of explosives(“dirty bomb”), the destruction of a nuclearfacility, the introduction of radioactive materialinto a food <strong>or</strong> water supply, <strong>or</strong> the explosion of anuclear device near a population center.Vect<strong>or</strong>-b<strong>or</strong>ne diseases: Diseases spread byvect<strong>or</strong>s, such as insects. Examples include RockyMountain spotted fever and malaria.Water-b<strong>or</strong>ne diseases: Diseases spread bycontaminated drinking water <strong>or</strong> recreationalwater, such as typhoid fever and cholera. Acc<strong>or</strong>dingto CDC, m<strong>or</strong>e than 4,100 personsbecome ill from contaminated drinking waterand m<strong>or</strong>e than 13,000 persons become ill fromrecreational water disease outbreaks annually in201, 202the United States.Zoonotic/Animal-b<strong>or</strong>ne diseases: Animaldiseases that can spread to humans and, in somecases, become contagious from human to human.Examples include Avian flu, West Nile virus, andSARS. In 2000, WHO identified m<strong>or</strong>e than 200diseases occurring in humans that were known tobe transmitted through animals. 203 Experts believethat the increased emergence of zoonotic diseasesw<strong>or</strong>ldwide can be attributed to population displacement,urbanization and crowding, def<strong>or</strong>estation,and globalization of the food supply.42
ECONOMICS AND PUBLIC HEALTH PREPAREDNESSIn addition to the health toll that diseases, disasters andbioterr<strong>or</strong>ism can take, they also have maj<strong>or</strong> economicimplications. F<strong>or</strong> example:n September 11, 2001 Tragedies: The total economicloss has been estimated at roughly $80 billion, of which$32.5 billion was insurable. 204 The insurance industrypaid the $32.5 billion in insured losses from businessinterruption, property, w<strong>or</strong>kers’ compensation, aviationliability and other liability costs. 205 In addition, W<strong>or</strong>ldTrade Center w<strong>or</strong>kers received a $625 million settlementf<strong>or</strong> their exposure to toxic dust. 206n Anthrax Attacks: Acc<strong>or</strong>ding to an article in the WashingtonPost, the clean up from the 2001 anthrax attacksexceeded $1 billion. 207 A rep<strong>or</strong>ted $42 million was spent todecontaminate the Hart Senate Office Building and otherCapitol Hill offices and it cost in excess of $200 million todecontaminate the postal facilities at Brentwood in Washington,D.C. and in Hamilton Township, New Jersey. 208This does not include the cost of the public health responseand lab<strong>or</strong>at<strong>or</strong>y testing of specimens around the country.s Acc<strong>or</strong>ding to a rep<strong>or</strong>t in the New Y<strong>or</strong>k Times, under ahypothetical scenario developed by DHS involving ananthrax attack, if terr<strong>or</strong>ists were to spray aerosolizedanthrax from a van in three cities initially, followed bytwo m<strong>or</strong>e cities sh<strong>or</strong>tly afterward, casualties could wellexceed 13,000, and result in a loss of billions of dollars. 209Other estimates are that anthrax could result in m<strong>or</strong>ethan 13,000 deaths in a single city.s Acc<strong>or</strong>ding to a study by Towers Perrin Consulting,one anthrax attack in New Y<strong>or</strong>k City could lead to $90billion in w<strong>or</strong>kers’ compensation losses, which would bethree times greater than the entire $30 billion w<strong>or</strong>kers’compensation industry. 210s Risk Management Solutions (RMS), a leading risk consultingfirm, believes an attack on downtown New Y<strong>or</strong>kCity could result in 173,000 casualties. In this scenario,anthrax is weaponized and dispersed in aerosol f<strong>or</strong>m,resulting in inhalation of anthrax by approximately onemillion people. RMS estimates economic losses of $91billion from w<strong>or</strong>kers compensation alone. 211n Nuclear, Biologic, <strong>or</strong> Chemical Attacks and the InsuranceIndustry: In 2005, the CEO of Allstate C<strong>or</strong>p, a leadinginsurance company, stated that nuclear, biological <strong>or</strong>chemical terr<strong>or</strong>ist attacks “could literally destroy the entirecapital base of the insurance industry.” 212 In 2003, the capitalbase f<strong>or</strong> the insurance industry was $347 billion. 213n Foodb<strong>or</strong>ne Illness and Agroterr<strong>or</strong>ism: Agriculturerepresents 1.2 percent of the U.S. gross domestic product(GDP), <strong>or</strong> $173 billion a year. 214 Agriculture and the foodsect<strong>or</strong> employed approximately 12.5 million w<strong>or</strong>kers in2008, <strong>or</strong> nearly nine percent of the total U.S. w<strong>or</strong>kf<strong>or</strong>ce. 215s In 2001, a foot-and-mouth disease outbreak in Britain ledto an estimated economic loss of $6 billion to $18 billion,and led to the destruction of four million animals. 216 A1999 rep<strong>or</strong>t estimated that an outbreak of foot-and-mouthin Calif<strong>or</strong>nia would lead to economic losses of $6 billion. 217s Over the last few decades, the United Kingdom has battledbovine spongif<strong>or</strong>m encephalopathy (BSE), better known as“mad cow” disease. As of March 2005, 149 people whowere infected with the disease have died, and nearly fourmillion cows have been slaughtered. 218 If a significant outbreakof BSE occurred in the United States, FDA estimatesthat there would be a loss of $15 billion, resulting from a 24percent decline in domestic beef sales and an 80 percentdecline in beef and live cattle exp<strong>or</strong>ts. Slaughter and disposalcosts of at-risk cattle could be additional $12 billion. 219s In 1978, the Arab Revolutionary Council engaged in bioterr<strong>or</strong>ism,using mercury to poison Israeli <strong>or</strong>anges. A dozenchildren in Holland and West Germany were hospitalizedas a result. Ultimately, this act helped sabotage the Israelieconomy, resulting in a 40 percent reduction in <strong>or</strong>ange exp<strong>or</strong>ts.220 At the time, <strong>or</strong>anges accounted f<strong>or</strong> about a tenthof all Israeli exp<strong>or</strong>ts. 221 The United States produces over 20percent of the w<strong>or</strong>ld’s citrus, <strong>or</strong> approximately 15.6 milliontons in 2004. 222 U.S. citrus exp<strong>or</strong>ts are roughly $1 billion,while U.S. consumers spend m<strong>or</strong>e than $3 billion on citrusproducts (<strong>or</strong>ange and grapefruit juice and fresh fruit). 223n New Infectious Disease Outbreak: In 2003, SARS sweptthrough Southeast Asia, infecting over 8,000 people andleaving 774 dead. 224 Its reach demonstrates the tremendousspeed in which disease can spread. Originating in China, theSARS outbreak eventually infected individuals from 29 nationsaround the w<strong>or</strong>ld. Overall, the economic losses, dueto deaths, quarantines and lost tourism dollars, may havebeen $30 to $50 billion, acc<strong>or</strong>ding to some estimates. 225 InT<strong>or</strong>onto alone (many thousands of miles away from the initialoutbreak), m<strong>or</strong>e than 27,000 people in and around the citywere f<strong>or</strong>ced into quarantine during two outbreaks, which ledto an estimated economic loss of nearly $1 billion. 226n Severe Pandemic Flu Outbreak: A severe pandemicflu similar to the 1918 pandemic could lead to a significantdrop in the U.S. Gross Domestic Product (GDP).227n Gulf Coast Oil Spill: There was a loss of an estimated$1.2 billion in economic output and 17,000 jobs in 2010 acc<strong>or</strong>dingto an analysis from Moody’s Analytics. 22843
D. SPECIAL TOPICS — A DECADE AFTER 9/11 AND ANTHRAXThe following expert commentaries feature aset of topics that are essential components ofpreparedness, including: bringing a range ofcommunity leaders together to prepare togetherf<strong>or</strong> potential health emergencies through Meta-Leadership eff<strong>or</strong>ts; defining the research agendato further preparedness systems and services; ensuringthat laws are in place to protect the publicand health officials during emergencies; and focusingon injuries, which is often an overlookedcomponent of preparedness.EXPERT PERSPECTIVEMeta-Leadership Empowers Community Leadersto Act Together in Times of CrisisBy Charles Stokes, president and chief executive officer of the CDC Foundation, an independent, nonprofit <strong>or</strong>ganization established byCongress to help CDC do m<strong>or</strong>e, faster.The events surrounding 9/11, Hurricane Katrina and H1N1should be a wakeup call f<strong>or</strong> America. From my perspective,these emergencies undersc<strong>or</strong>e the urgent need f<strong>or</strong> leadersto act collab<strong>or</strong>atively across public and private sect<strong>or</strong>s in timesof crisis. As ongoing public health budget cuts strain the capacityof CDC and state and local health agencies across the country, itis critical f<strong>or</strong> communities to find ways to close the gaps to keepAmerica healthy, safe and secure.The Meta-Leadership Summit f<strong>or</strong> Preparedness, a five-yearinitiative funded by the Robert Wood Johnson Foundation(RWJF), is a model approach f<strong>or</strong> bringing communities togetherto respond to crises. Since 2006, the initiative has connectedclose to 5,000 business, government and nonprofit leaders in 36communities representing approximately 139 million Americans.The CDC Foundation partnered with CDC, the Robert WoodJohnson Foundation and the National Preparedness LeadershipInitiative-Harvard School of Public Health to host the successfulnetw<strong>or</strong>king and training events.What makes the Meta-Leadership Summit f<strong>or</strong> Preparednessprogram unique is its focus on cross-sect<strong>or</strong> collab<strong>or</strong>ation andcommunity action. As Summits took place across the country,local host committees were crucial to end<strong>or</strong>sing the Summitand getting the right leaders in the room. Local spons<strong>or</strong>ssupplemented the Robert Wood Johnson Foundation’s nationalsupp<strong>or</strong>t, covering local event expenses so that participantscould attend at no cost. Frontline meta-leaders from CDC andother federal agencies joined with Harvard faculty to providereal-w<strong>or</strong>ld perspectives on leading in emergencies. High profilespeakers — including govern<strong>or</strong>s, may<strong>or</strong>s and CEOs — elevatedthe profile of the initiative and attracted local media coverage.Realistic scenarios, developed by Harvard faculty in collab<strong>or</strong>ationwith local leaders, helped participants envision the seriousconsequences that could emerge in their own communities followinga terr<strong>or</strong>ist attack <strong>or</strong> natural disaster.Sometimes connections among Summit participants were notimmediately obvious. F<strong>or</strong> example, at the Boston Meta-LeadershipSummit, a leader from the Boston Ballet attended theevent. Some wondered what role the arts could possibly playin community preparedness. However, when leaders identifiedgaps in preparedness — and how they might contribute theirown resources and capabilities to fill those gaps — the BostonBallet offered its space as a shelter f<strong>or</strong> disaster victims. A synergyoccurs when leaders connect face-to-face to create betterprepared, m<strong>or</strong>e resilient communities.Although the final Meta-Leadership Summit took place in Long Island,New Y<strong>or</strong>k, in June 2011, the initiative is far from over. A CDCpost-Summit team reconvenes leaders approximately six monthsafter each Summit to continue building cross-sect<strong>or</strong> connectivityand applying meta-leadership concepts to preparedness planning.Through post-Summit activities unique to each community, CDCcasts a wider net, encouraging participants to address preparednessgaps identified at the Summit and through evaluation results. Todate, m<strong>or</strong>e than 2,000 leaders have participated in post-Summitpresentations and discussions related to cross-sect<strong>or</strong> preparedness.Topics include addressing the needs of vulnerable populations, engagingfaith-based <strong>or</strong>ganizations in preparedness planning, enhancingc<strong>or</strong>p<strong>or</strong>ate security and leveraging virtual communities.Summit participants are also invited to join a Meta-Leadership OnlineCommunity (www.meta-leadershipcommunity.<strong>or</strong>g) that extendstheir collab<strong>or</strong>ation. With thoughtful cultivation and ongoingsupp<strong>or</strong>t from the Robert Wood Johnson Foundation, the onlinecommunity continues to thrive. M<strong>or</strong>e than 2,800 members havejoined to share resources, discuss topics of interest and connectwith other Summit participants, locally and nationally.Throughout the initiative, all partners and stakeholders soughtclear evidence of Summit outcomes and continuous improvementin the program’s design and implementation. Cumulativeevaluation results are extremely positive: 94 percent of respon-44
dents agreed that attendance at the Summit was a valuable use oftheir time, 91 percent rated the overall quality of the Summit as“good” <strong>or</strong> “outstanding” and 91 percent would recommend theSummit to their colleagues.Practical examples of meta-leadership are evident across thecountry. F<strong>or</strong> example, in San Diego, a public-private coalitionestablished by the San Diego County Office of Emergency Servicesexperienced a significant boost in nonprofit and businessparticipation after the Summit. In Boston, May<strong>or</strong> Menino held across-sect<strong>or</strong> Boston Influenza Preparedness Summit, building onthe meta-leadership model. Eight Illinois meta-leaders who participatedin a University of Illinois at Chicago (UIC) School of PublicHealth fellowship program made the case f<strong>or</strong> the nation’s firstMeta-Leadership Institute and applied meta-leadership to communityissues beyond preparedness, including school violence, fluvaccination and faith-based outreach. Following the Gulf oil spill,Southeast Louisiana meta-leaders developed a proposal templateand process f<strong>or</strong> BP-funded emotional supp<strong>or</strong>t services that areessential to long-term community supp<strong>or</strong>t. Kay Wilkins, CEO,American Red Cross Southeast Louisiana Chapter said, “What theMeta-Leadership Summit did was open avenues to other peopleand groups we might not have thought about.”As others learn about meta-leadership, interest continues tobuild. In September 2011, the CDC Foundation was invited tohelp the Federal Emergency Management Agency (FEMA) developand implement a “Whole Community” approach to emergencymanagement. The eff<strong>or</strong>t includes methods to build on thelessons learned through the Meta-Leadership Initiative — fromSummits to post-Summit activities to the online community —to help FEMA identify and test ways to better engage with communities,and to integrate preparedness into community andcivic <strong>or</strong>ganizations that serve those communities.CDC and public health leaders across the nation shoulder the considerableand singular duty to protect the nation from maj<strong>or</strong> healththreats 24/7, including catastrophic events. In light of the ongoingbudget cuts, and at a time when the United States and the w<strong>or</strong>ldfaces increasing threats from nature, technology and human action,helping leaders understand their counterparts’ interests and establishingconnectivity bef<strong>or</strong>e disaster strikes is imperative.San FranciscoCalif<strong>or</strong>niaMeta-Leadership Summit f<strong>or</strong> Preparedness ImpactLos AngelesSan DiegoPhoenixDenverNew MexicoNebraskaKansasDallasMinneapolisHoustonMilwaukeeBostonLongCleveland Pittsburgh IslandIllinoisCentral Indiana CincinnatiNew JerseyColumbusDelaware ValleyLouisville Maryland NationalSt. Louis LexingtonSouthwest VirginiaCapital RegionN<strong>or</strong>th CarolinaLousianaAtlantaColumbus Coastal Ge<strong>or</strong>giaFl<strong>or</strong>ida CapitalTampaFrom 2006-2011, the Meta-Leadership Summit f<strong>or</strong> Preparedness connectedclose to 5,000 business, government and nonprofit leaders in 36 communitiesrepresenting approximately 139 million Americans.What is a Meta-Leader? A meta-leader is aleader of leaders, who mobilizes people and<strong>or</strong>ganizations to collab<strong>or</strong>ate in times of crisis.When disaster strikes, meta-leaders reachacross <strong>or</strong>ganizations and sect<strong>or</strong>s to buildcross-cutting strategies to protect the safetyof their families, businesses and communities.They exchange inf<strong>or</strong>mation, share resourcesand co<strong>or</strong>dinate systems and personnel. Theyuse their influence and connections to guide acooperative course of action.Being a meta-leader requires a unique mindsetand skill set, which often goes beyond thescope of an individual’s previous experiences.And it requires building strong alliances with adiverse array of leaders bef<strong>or</strong>e an event occurs.The Meta-Leadership Summit f<strong>or</strong> Preparednesscultivates the critical problem-solving skills andconnectivity that leaders need to be effectivemeta-leaders during times of crisis.45
EXPERT PERSPECTIVEPreparedness and Public HealthSystems and Services ResearchBy F. Douglas Scutchfield, M.D., principal investigat<strong>or</strong>, Center f<strong>or</strong> Public Health Systems and ServicesResearch at the University of Kentucky College of Public HealthThe 10th anniversary of 9/11 and the Anthraxscare give us an occasion to pause and considera vital question. We moved, as a nation, toassure that we were protected from bioterr<strong>or</strong>ismand were prepared f<strong>or</strong> the natural and unnaturaldisasters that we will likely experience. We havehad other reminders of the imp<strong>or</strong>tance of thatcapacity, Hurricane Katrina being a classic example.One of the key components of our abilityto respond to either of these s<strong>or</strong>ts of events is ourpublic health system and its backbone, the localhealth department.Unf<strong>or</strong>tunately, as a nation we have a tendency to“fight the last war” and to gear up in response to amaj<strong>or</strong> event, but as those problems fade into time,we tend to neglect the lessons, and allow those eff<strong>or</strong>tswe invested in preparedness to deteri<strong>or</strong>ateand return to the status quo that existed bef<strong>or</strong>e theevent. Recently, a colleague and I were w<strong>or</strong>king ona public health book, in which there was a chapteron the hist<strong>or</strong>y of public health. We were both struckby the hist<strong>or</strong>y of public health, gearing up to respondto a maj<strong>or</strong> public health event and then watching aspublic health gains that were achieved diminish withtime and a loss of supp<strong>or</strong>t and interest.Unf<strong>or</strong>tunately, that is the current state of publichealth. We don’t learn our hist<strong>or</strong>y lessons, so followingthe build-up of public health in 2001, weare now allowing the system we established to deteri<strong>or</strong>ate— two steps f<strong>or</strong>ward, three steps back.As certain as the sun will rise in the east, we willexperience another event that will demonstrateour inability to cope, as the resources f<strong>or</strong> publichealth are scarce, and it will prompt the cycle ofbuild-up, neglect, event, build-up, etc.Following 9/11 we created, in our nation’s schoolsof public health, preparedness centers that wereresponsible f<strong>or</strong> developing training f<strong>or</strong> preparednesscapacity in our nation’s public health system. Thesecenters quickly realized that there was inf<strong>or</strong>mationthat they needed in their training eff<strong>or</strong>ts, inf<strong>or</strong>mationthat wasn’t available in the lexicon of public healthand where they needed research and investigationto respond to this need. This need prompted Congressto establish auth<strong>or</strong>ity to empower preparednesscenters, previously created by CDC as theresult of congressional action, to answer some ofthe most difficult questions in how best to addresspublic health preparedness. With this auth<strong>or</strong>ity, theCDC created a few select preparedness centersto help find and make this inf<strong>or</strong>mation available tothose who are and were training the individuals thatwe needed f<strong>or</strong> preparedness. As an example of thew<strong>or</strong>k of these research centers, the University ofN<strong>or</strong>th Carolina at Chapel Hill demonstrated that, inN<strong>or</strong>th Carolina, which has a state public health departmentaccreditation program, accredited healthdepartments were m<strong>or</strong>e likely to sc<strong>or</strong>e higher ontheir preparedness profiles than health departmentsthat were not accredited. With the advent of nationalpublic health accreditation, this inf<strong>or</strong>mation is apowerful tool to encourage and supp<strong>or</strong>t those healthdepartments seeking and obtaining accreditation, asthere is the assurance that they are m<strong>or</strong>e likely to beprepared f<strong>or</strong> dealing with disasters. These centers,Preparedness and Emergency Response Research46
Centers, unf<strong>or</strong>tunately lost their funding two yearsago. That left a maj<strong>or</strong> hole in the capacity to helpdevelop and train the individuals and <strong>or</strong>ganizations,as critical gaps exist in knowledge that would impactour ability to cope with disasters.This is not an uncommon problem. One of the firstcuts made in tight budget times is the activities thatproduce new data and knowledge. Often the assumptionis made that we can move on programs,including preparedness, without understandingwhat’s necessary to develop, implement and evaluatehealth <strong>or</strong> public health programs. The requiredknowledge and skills come as the result of eff<strong>or</strong>tsto examine the questions and find answers thathave utility and can be used to deal with whateverthe problem is that presents itself. In fact, one ofthe most useful things we can engage in, duringtight budget times, is the questions of efficiencyand effectiveness of our programs. We need to uselimited resources as best we can — and research iskey to knowing how best to accomplish our goals.As with other public health programs, successfulimplementation depends on the infrastructure todeliver the program. The w<strong>or</strong>kf<strong>or</strong>ce, technology,finances and <strong>or</strong>ganization influence tremendouslythe capacity of the public health system and itsunits to respond to any eventuality. It is imperativethat we have the best knowledge possible onthe infrastructure that allows us to be successfulin our eff<strong>or</strong>ts to implement any public health program,including preparedness.Recently, the Robert Wood Johnson Foundation andCDC led an eff<strong>or</strong>t to establish an agenda of the researchquestions we need to know in <strong>or</strong>der to mosteffectively develop and implement public health programs.The list of research questions that coveredw<strong>or</strong>kf<strong>or</strong>ce, structure, finance and other infrastructureissues was several pages long, and reflectedthe questions and concerns of practitioners, policymakers,and public health academicians alike. Theagenda is rich with issues that stand in the way ofour being able to carry out the programs and projectsthat include not only preparedness, but also themyriad of public health problems that face America,from childhood obesity to the increased concernswith chronic diseases, such as cancer and heartdisease. Questions from that agenda include issuessuch as how should state health departments be<strong>or</strong>ganized, independent entities <strong>or</strong> part of a healthand social services umbrella <strong>or</strong>ganization? How canlocal health departments develop and sustain sharingagreements across jurisdictional boundaries toassure that the capacity f<strong>or</strong> emergency responseexists f<strong>or</strong> the communities they serve? How arebroad categ<strong>or</strong>ical areas of public health, includingpreparedness, funded? How do decisions about thisfunding impact other areas of public health responsibility?Does, f<strong>or</strong> example, an emphasis on preparednessdetract from the community’s immunizationeff<strong>or</strong>ts and lead to the increase in whooping coughcases we are experiencing in the U.S.?These are not trivial questions; in fact the latterissue has prompted a study by GAO and one in theDepartment of Health and Human Services AssistantSecretary of Planning and Evaluation’s office.Over the past century, public health has played avital role in eff<strong>or</strong>ts to address these issues. Strongpublic health programs are a critical componentto our nation’s ability to thrive, even in trying economictimes. In <strong>or</strong>der to have those programs, itis imperative that we have the knowledge that laysthe groundw<strong>or</strong>k f<strong>or</strong> that success. W<strong>or</strong>king withall segments of the health community in a timeof economic instability and tremendous change inour health care system, we can and must have theinf<strong>or</strong>mation and knowledge that allows f<strong>or</strong> successfulpublic health programs and assures that weare prepared f<strong>or</strong> either natural <strong>or</strong> unnatural disasters.As Gandhi observed, “It is health that is realwealth and not pieces of gold and silver.”47
EXPERT PERSPECTIVEPublic Health Legal Preparedness in the United StatesAn Interview with James G. Hodge, Jr., J.D., LL.M., Lincoln Profess<strong>or</strong> of Health Law and Ethics and direct<strong>or</strong> of the Public Health Law& Policy Program and direct<strong>or</strong> of the Netw<strong>or</strong>k f<strong>or</strong> Public Health Law-Western Region at the ASU Sandra Day O’Conn<strong>or</strong> College of LawOn September 27, 2011, the Trust f<strong>or</strong> America’s Healthconducted an interview with Profess<strong>or</strong> James G. Hodge,Jr. regarding the nature, scope and challenges of emergencylegal preparedness. Edited f<strong>or</strong> content, questions and responsesare as follows:What is the role of law in emergency preparedness fromyour point of view?Law is an essential component of emergency preparedness. Lawsdefine what constitutes an emergency, disaster, <strong>or</strong> public healthemergency. They auth<strong>or</strong>ize (and at times prohibit) specific actions.Laws set roles, responsibilities, and liabilities f<strong>or</strong> public and privatesect<strong>or</strong> responders and entities. Ultimately, it is law that helps toprovide guidance f<strong>or</strong> emergency responses, and, when practicedappropriately in real-time, laws can contribute to declinations inpreventable m<strong>or</strong>bidity and m<strong>or</strong>tality in declared emergencies.What types of legal challenges do states and other governmentsface in emergency preparedness?Legal preparedness challenges across jurisdictions are immense.One central challenge of public health legal preparedness relatesto meeting surge capacity (i.e., the ability of public health andmedical systems to care f<strong>or</strong> a massive influx of patients duringpublic health emergencies). Meeting surge capacity is key to savinglives and preventing the spread of communicable diseasesin emergencies. Maj<strong>or</strong> concerns surrounding surge capacityinclude distributing and dispensing antivirals, vaccines, <strong>or</strong> othermedicines; increasing health care staffing; and securing adequateand safe spaces f<strong>or</strong> the influx of patients. None of these objectivesis possible without real-time legal assistance and supp<strong>or</strong>t.F<strong>or</strong> example, personnel required in a crisis (including out-of-statephysicians, nurses, and assistants, as well as mental health providers)must be capable of adapting quickly to implementing a crisisstandard of care under potentially changing rules regarding scopeof practice. These adaptations necessitate legal changes, as well,inherent in declarations of public health emergency that may typicallyprecede maj<strong>or</strong> jurisdictional shifts in health care personnel.How can law specifically facilitate health care voluntarismduring emergencies?There are many legal paths to ensuring adequate and skillednumbers of volunteer health practitioners in declared emergencies.Whether coming through state-based ESAR-VHP programs,locally-run MRC units, <strong>or</strong> other routes, civilian volunteersstrengthen public health and emergency response eff<strong>or</strong>ts byproviding essential personnel f<strong>or</strong> overrun medical systems duringa crisis. Thousands of skilled, vetted volunteers streamed toLouisiana and surrounding states post-Katrina in 2005. Their eff<strong>or</strong>tswere greatly facilitated through legal interventions designedto supp<strong>or</strong>t trained volunteers and encourage their participation.N<strong>or</strong>mally, you cannot just bring in out-of-state practitionersand let them practice medicine in any given state. In non-emergencies,state-based licensing laws and other legal liability issueswould stop the deployment and use of out-of-state volunteers.The emergency legal environment has to evolve quickly to allowskilled volunteers to step in seamlessly and aid in the response.Legal techniques that provide licensure reciprocity and liabilitycoverage f<strong>or</strong> volunteers make their contributions possible. Eachof these and many other legal tools have been crafted in the lastdecade following the terr<strong>or</strong>ist acts of September 11, 2001, andthe ensuing anthrax exposures that fall. My ESAR-VHP Legaland Regulat<strong>or</strong>y Issues Rep<strong>or</strong>t, prepared f<strong>or</strong> DHHS’ AssistantSecretary f<strong>or</strong> Preparedness and Response, provides some helpfultables and analyses across the 50 states related to these issues.The rep<strong>or</strong>t and other helpful documents are available online athttp://www.publichealthlaw.net/Projects/ESAR-VHP.php.Are there any maj<strong>or</strong> gaps in state <strong>or</strong> local public healthpreparedness laws?Over the last decade, there have been systematic, wholesale changesto emergency response laws and policies at all levels of government.Despite solid models introduced to help policymakers consideringref<strong>or</strong>ms, many of the legal changes are not unif<strong>or</strong>m across states.While most emergency laws are written broadly enough to allow extensiveand flexible responses, sometimes the breadth of these lawsleads to confusion, debate, and delay in actual emergencies.In addition, there are extensive variances in the legal framew<strong>or</strong>ksrelated to surge capacity, especially in licensing and reciprocity.Lacking unif<strong>or</strong>m protections concerning common negligenceclaims, f<strong>or</strong> example, it is empirically shown that volunteers mighthesitate to help during a crisis. Volunteers and entities thatdeploy <strong>or</strong> host them seek strong protections from liability, butsometimes find divergent standards across jurisdictions.What can jurisdictions do to address these gaps?Active, advance eff<strong>or</strong>ts to assess and address legal preparednessgaps are key. There are several excellent models that provide48
unif<strong>or</strong>m approaches to key legal preparedness issues. TheModel State Emergency Health Powers Act, drafted in 2001 bythe Centers f<strong>or</strong> Law and the Public’s Health at Ge<strong>or</strong>getown andJohns Hopkins Universities, provides a comprehensive seriesof legislative and regulat<strong>or</strong>y provisions f<strong>or</strong> state and local publichealth emergency responses. Nearly every state legislature hasconsidered its provisions in whole <strong>or</strong> part, and 38 states, as wellas the District of Columbia, have passed related bills, acc<strong>or</strong>dingto the Center’s legislative tracking available at http://www.publichealthlaw.net/ModelLaws/MSEHPA.php.The Emergency Management Assistance Compact (EMAC), executednow by all states, provides licensure reciprocity automaticallyf<strong>or</strong> all “state <strong>or</strong> local agents” serving across state b<strong>or</strong>dersduring declared emergencies. It also provides clear limitations onliability. Of course, not all volunteers are state <strong>or</strong> local agents.Private sect<strong>or</strong> volunteers through ESAR-VHP <strong>or</strong> MRC systemsmay garner similar protections under the Unif<strong>or</strong>m EmergencyVolunteer Health Practitioners Act of 2007, but only if stateshave adopted its provisions. Presently, only 12 states, the Districtof Columbia, and the Virgin Islands have done so acc<strong>or</strong>ding tothe Unif<strong>or</strong>m Law Commission (available at http://www.nccusl.<strong>or</strong>g/Act.aspx?title=Emergency Volunteer Health Practitioners).How do federal, state and local preparedness laws differ?Federal, state and local governments have very different legalauth<strong>or</strong>ities. States possess the broadest auth<strong>or</strong>ity to addresspublic health threats, which they may share in part with localgovernments depending on the degree of “home rule” thatis assigned to these local governments. This varies considerablyacross states. Hist<strong>or</strong>ically, the federal government’s publichealth emergency law responsibilities are m<strong>or</strong>e limited to providingsignificant guidance, resources and expertise, except asrelated to emergencies implicating national security interests f<strong>or</strong>which federal jurisdiction is extensive.While the federal government has re<strong>or</strong>ganized itself since 2001to better handle national response eff<strong>or</strong>ts during emergencies,state and local governments ultimately remain on the frontlines.The federal government defers to state and local agencies inmany cases, subject to some prominent exceptions.How can these differences in federal, state, and local powerscomplicate <strong>or</strong> impede emergency response eff<strong>or</strong>ts?One example concerns the distribution of antivirals, vaccines,and other medicines <strong>or</strong> supplies. To alleviate the potential f<strong>or</strong>national sh<strong>or</strong>tages in public health emergencies, Congress hasauth<strong>or</strong>ized the creation of stockpiles of antivirals and vaccineskept by the SNS, controlled by CDC. These assets are availableto supplement state and local response eff<strong>or</strong>ts at the discretionof CDC. Legally, CDC may be positioned not only to distributeSNS supplies, but also determine the pri<strong>or</strong>ities through whichthe supplies may be dispensed across states.During the 2009/2010 H1N1 pandemic, CDC dispensed availablevaccines to states together with its policy outlining whoshould be first in line to receive them. Many state and localact<strong>or</strong>s adhered to CDC’s guidance; others did not, however.Once these supplies get to points of dispensing, CDC ultimatelymay lose control over how they are provided to local populations,although legally it can set a pri<strong>or</strong>itization plan.What steps can be taken to improve public health legalpreparedness across all jurisdictions?While emergency legal preparedness has improved immenselyover the pri<strong>or</strong> decade since 9/11, there are still imp<strong>or</strong>tant gapsto be filled at every level of government, but most notably atthe state level given their prominence in protecting the public’shealth. States seeking to improve preparedness through lawmight consider actions to:1. Assess critical legal and policy issues that need to be addressedin advance of the next emergency. Events like Katrina,the H1N1 pandemic and regional emergencies provide ample illustrationsof potential gaps in law and policy. So do specific observationsamong emergency and public health responders waryof key dilemmas bef<strong>or</strong>e they arise. Policymakers must routinelystudy and seek to address these issues affirmatively.2. Address the gaps. Identifying gaps is one thing; solving themis another. Hoping f<strong>or</strong> real-time solutions during an emergencyis counter-productive. Lives may be lost while legal issues arehammered out. This is unacceptable and yet easily c<strong>or</strong>rected.Using existing models, practice guidance, <strong>or</strong> comparisons to policyfixes that w<strong>or</strong>k in other jurisdictions, states can legislatively<strong>or</strong> via regulation address gaps without waiting f<strong>or</strong> inevitablecomplications during the next emergency.3. Practice legal preparedness. Like other preparedness skillsand capacities, legal preparedness must be practiced to be effective.Everyone involved in law and policy responses duringemergencies should w<strong>or</strong>k through legal scenarios in “real-time”during training exercises. Practicing what I like to call “legal triage”through actual exercises <strong>or</strong> education eff<strong>or</strong>ts helps to identify andremedy gaps — it is an investment that will facilitate future emergencyresponses in real-time. CDC and NACCHO have w<strong>or</strong>kedrecently with the Netw<strong>or</strong>k f<strong>or</strong> Public Health Law to develop abrief public health legal preparedness curriculum of particular valuef<strong>or</strong> state and local officials (which is still under federal review).49
EXPERT PERSPECTIVEDisaster Preparedness f<strong>or</strong> Mass Casualties fromExplosive Devices—the Role of Injury Preventionand ControlBy Richard W. Sattin, M.D., F.A.C.P., president-elect, Society f<strong>or</strong> Advancement of Violence and Injury Research and profess<strong>or</strong> and researchdirect<strong>or</strong> at the Department of Emergency Medicine at Ge<strong>or</strong>gia Health Sciences UniversityT<strong>or</strong>nadoes,earthquakes, hurricanes, tsunamis and terr<strong>or</strong>istbombings have one maj<strong>or</strong> health outcome in common—most deaths during these disasters occur due to injury. Drowning,being crushed by a collapsing building <strong>or</strong> other structure,being struck by a moving object, being thrown against a structure<strong>or</strong> an object are common outcomes and are predictable.Many non-medical types of preparedness exist that reduce injuriesand deaths from natural disasters, including building codes(retrofits f<strong>or</strong> earthquakes, construction of safe rooms in t<strong>or</strong>nadoareas, use of hurricane shutters and elevated construction inhurricane/typhoon areas), and improved planning and regulationf<strong>or</strong> land use and building of homes and businesses. Better andm<strong>or</strong>e effective preparedness and evacuation plans could lessenthe impact of these injuries on individuals, families and society.As we remember 10 years later the events of 9/11, it is clear thatthere remain critical issues on how to prevent and lessen thecomplications of injuries, including death, disability and emotionalstress during catastrophic events. Much of the preparednessf<strong>or</strong> mass casualty events in the United States has focused on thethreat of biological, chemical, radiation and nuclear incident.As events in Oklahoma City, New Y<strong>or</strong>k City, Madrid, London,Mumbai, Bali and elsewhere have shown, the use of conventionalweapons and explosive devices is a far m<strong>or</strong>e likely scenario,and the resultant injuries present unique triage, diagnostic andmanagement challenges to health care providers. Injuries fromexplosive materials due to terr<strong>or</strong>ism <strong>or</strong> other causes are a constantthreat that happens w<strong>or</strong>ldwide. The remainder of thiscommentary will primarily use mass casualties from conventionalexplosive devices to explain current injury prevention and controlprinciples and ways to strengthen policies and procedures.Few physicians in the United States, other than those whohave served in combat areas, have been trained in the care ofthe injured blast victim <strong>or</strong> have taken care of a patient whohas sustained injuries from an explosion. Persons injured froman explosion often have a much greater number of penetratingwounds compared with the routine trauma patient. Mosthospitals have emergency response plans and do have regularexercises, but exercises do not approach the chaos which accompaniesa mass casualty event. Identifying weak points inthose plans and testing alternative strategies are critical to ensurethe care f<strong>or</strong> those injured from explosive devices duringa real episode is optimal, especially if a large explosion-relatedmass casualty event occurs on our already fragile and overburdenedresponse system. The ability to push out key inf<strong>or</strong>mationon best practices quickly and efficiently to health professionalswho are suddenly faced with a situation with which they are notfamiliar will be essential to optimizing care.During a mass casualty event, health professionals use triageprotocols to identify those persons needing immediate, lifesavingcare and transp<strong>or</strong>t to critical care hospitals while avoidingovercrowding at those hospitals. Due to the potential extensivenature of a mass casualty event, outcomes are dependent ona broad continuum and rapid co<strong>or</strong>dination of multidisciplinarycare together with the availability of hospital resources (e.g.,operating theaters, radiology suites, number of intensive-carebeds and respirat<strong>or</strong>s, medical specialty care). The number ofvictims can quickly overwhelm the capacity of the health caresystem. Health care providers can expect casualties to arrivewithin 20 minutes of the bombing, with most of the total victimspresenting f<strong>or</strong> care within two hours. Most current planning f<strong>or</strong>mass casualty events assumes that the emergency medical responsewill function n<strong>or</strong>mally. Auf der Heide provided a reviewof the literature regarding disaster planning (The imp<strong>or</strong>tance ofevidence-based disaster planning Annals of Emergency Medicine2006;47, 34–49) indicating, however, that the actual responsediffers considerably from these planning assumptions; there isunco<strong>or</strong>dinated emergency dispatch, lack of hospital notificationand communication, significant bystander involvement andrescue, absent <strong>or</strong> ineffective scene triage, self-referral and thetransp<strong>or</strong>t of many, if not most, patients to the nearest healthcarefacility. What occurs is, theref<strong>or</strong>e, reverse triage, that is,the least-injured patients arrive at the nearest hospitals bef<strong>or</strong>ethe critically injured patients do. The extent of this reverse triagehas been shown to c<strong>or</strong>relate directly with the m<strong>or</strong>tality ofthose patients who were critically injured in the event.Injury has been described, until recently, as the “neglected disease”since it occurs in such great numbers, but has been tacitlyaccepted as a n<strong>or</strong>mal occurrence of living in a modern society.50
The 1985 rep<strong>or</strong>t, Injury in America, noted, however, that a publichealth approach similar to that used f<strong>or</strong> other diseases couldlead to significant reduction in injuries. To understand the conceptsof injuries from explosions, one must also understand thebasic paradigm of injury control. Injury can affect any person’sbody part, <strong>or</strong>gan, <strong>or</strong> system and its functioning and can haveboth sh<strong>or</strong>t-term and long-term effects. It is not merely survivalafter an explosion-related injury that is imp<strong>or</strong>tant, but rather theability of the individual to attain maximum physical recovery, tosurvive financially, and to enable secure, productive lives regardlessof functional status. As with other diseases, injuries can beviewed as a relationship between a person (the host), an agentand the environment. Unlike other diseases, the underlyingagent of injury is not a microbe <strong>or</strong> carcinogen, but is energy,most often in the f<strong>or</strong>m of mechanical f<strong>or</strong>ce. The dose of energyreceived, the dose’s distribution, duration and rapidity, and theindividual’s response to the transfer of the energy can determineif a physical injury occurs <strong>or</strong> is prevented. F<strong>or</strong> example, a largemechanical energy load quickly transmitted to a hip during a fallinvolving an older person may lead to a fracture. If that sameenergy load could be dissipated through use of energy-abs<strong>or</strong>bingflo<strong>or</strong>ing <strong>or</strong> mats <strong>or</strong> through hip pads <strong>or</strong> other new technologies,fewer persons would sustain hip fractures. Similarly, the designof safer buildings (e.g., the use of blast-resistant materials such astempered glass and window coverings) dissipates the energy loadand reduces the numbers of persons injured from an explosion.The basic injury paradigm of host, agent and environment alsoneeds to include the effect of the social environment. Victimsof explosions can also experience adverse mental health consequencesincluding depression, anxiety and low self-esteem, andharmful physical health consequences such as suicide attempts,cardiovascular disease and substance abuse. The emotional,financial, and psychosocial effects of an acute injury may beeven m<strong>or</strong>e debilitating than the actual physical injury. An acuteinjury has not just an immediate effect on the injured person,but also a long-term “ripple effect” on that person’s life and thelives of others in his <strong>or</strong> her family and community. Temp<strong>or</strong>ary<strong>or</strong> permanent loss of income, changes in personal relationshipsincluding income responsibilities, and difficulty in care and financialsupp<strong>or</strong>t f<strong>or</strong> one’s children <strong>or</strong> parents may be a significantsocial outcome from the injury. Health care providers may alsobe subject to psychosocial problems resulting from caring f<strong>or</strong>so many injured persons in such a sh<strong>or</strong>t time period. A community’ssocietal and functional infrastructure may be affectedextensively during a mass casualty event.An understanding of the epidemiology of explosion-relatedinjuries also requires surveillance data to help identify ways toprevent <strong>or</strong> reduce vulnerability to these types of events. Surveillancedata are analyzed to determine the magnitude, scope andcharacteristics of a health problem; to study the fact<strong>or</strong>s thatincrease the risk of disease, injury, <strong>or</strong> disability; to determinewhich risks are potentially modifiable; to assess what can bedone to prevent the problem using the inf<strong>or</strong>mation about causesand risk fact<strong>or</strong>s; to design, pilot test and evaluate interventions,and to then implement the most promising interventions on abroad scale. Much data during a mass casualty event are perishablesince there are no active plans to collect these data. Thisis unf<strong>or</strong>tunate since determining ways to prevent and improveoutcomes from injuries are dependent on understanding whattook place and how patients were managed. Standardized minimumdata collection instruments and definitions are essentialto generate reliable intra- and inter-country comparisons ofinjuries from explosions. Data collected through this integratedapproach can be used to make the case f<strong>or</strong> the design of saferbuildings, improve evacuation plans and plan the allocation ofmedical and rescue resources and operations (e.g., ambulances,blood supply). These enhanced surveillance systems can helppublic health professionals link the findings to the managementdecision process and disseminate the data collected to improvethe level of preparedness nation-wide.Over the last decade, we have made significant strides in caringf<strong>or</strong> the explosion-related victim but further progress in learninghow to maximize care and protect the public is needed.Further integration of trauma systems and evaluation of thatintegration with law enf<strong>or</strong>cement, fire prevention, power supplyand other infrastructure issues should take place to improve thecare of the acutely injured. As communication can be difficultduring the chaos following a mass casualty event, it is imp<strong>or</strong>tantto continue to improve communication systems’ interoperability.Accurate and reliable data systems are critical to determinehow best to prevent injury and care f<strong>or</strong> the injured so identifyingand improving ways of collecting data, making full use ofexisting data systems and having access to the real-time use ofdata during an event would be maj<strong>or</strong> steps f<strong>or</strong>ward. Educationalprograms f<strong>or</strong> health care providers are currently available,but the exact type and extent of education and the need f<strong>or</strong> andamount of refresher courses f<strong>or</strong> various providers (pre-hospitaland hospital) to ensure an appropriate level of knowledge andexpertise is not precisely known. Many serious secondary injuriesoccur after a disaster so further co<strong>or</strong>dination between disasterpreparedness and acute injury care management of thesedifficult environments and situations is necessary. By integratingfurther injury prevention and control into disaster preparedness,we will continue to make maj<strong>or</strong> strides in preventing injury andin providing improved medical, mental health and rehabilitativeservices to surviv<strong>or</strong>s of disaster events.51
Federal Policy Issues andRecommendations4SectionIn the coming year, implementation of the reauth<strong>or</strong>ized public health preparednesslegislation provides a new opp<strong>or</strong>tunity to address ongoing challenges that publichealth preparedness faces while the field considers how to allocate increasingly scarceresources during budget cutbacks.TFAH has identified some top areas of concern,including:A. Assuring dedicated and ongoing funding f<strong>or</strong>emergency preparedness and strengthening thec<strong>or</strong>e public health infrastructure nationwide;n Commentary: Improving Collab<strong>or</strong>ation betweenFederal, State and Local agencies in Planning f<strong>or</strong> aW<strong>or</strong>st Case Scenario: A Broad Aerosolized Dispersal ofWeaponized Anthrax in a Maj<strong>or</strong> Metropolitan Area.By Alonzo Plough, PhD, MPH, Direct<strong>or</strong>, EmergencyPreparedness and Response of the Los Angeles CountyDepartment of Public Health and Member of theBoard of Direct<strong>or</strong>s of the Trust f<strong>or</strong> America’s HealthB. Modernizing biosurveillance to rapidly andaccurately detect outbreaks and threats;C. Improving the research, development andavailability of vaccines and medications;n Commentary: Surveillance: Essential f<strong>or</strong> Public HealthPreparedness and Response, By, Jeffrey Engel, M.D.,State Health Direct<strong>or</strong>, Division of Public Health, N<strong>or</strong>thCarolina Department of Health and Human ServicesD. Increasing the ability of the public healthand health care systems to provide mass careduring emergencies;E. W<strong>or</strong>king with communities to cope withand recover from emergencies, particularlyf<strong>or</strong> the m<strong>or</strong>e vulnerable members of communitiesincluding children, seni<strong>or</strong>s, people withunderlying health conditions, racial and ethnicmin<strong>or</strong>ities and lower-income individuals;n Commentary: Vulnerability, Resilience and MentalHealth Considerations in Disaster Planning and Response:Do Resources Match the Rhet<strong>or</strong>ic? By DavidAbramson, PhD, MPH and Irwin Redlener, MD, ColumbiaUniversity Mailman School of Public HealthF. Co<strong>or</strong>dinating public health preparednesswith strategic implementation of the FDA FoodSafety Modernization Act of 2011.n Commentary: Food Safety: New Law Takes a BigBite Out of the Problem, but Leaves Much on thePlate. By Erik D. Olson, Direct<strong>or</strong> of Food Programsat The Pew Charitable TrustsA. Assuring Dedicated Funding and StrengtheningPublic Health Preparedness InfrastructureThe United States made a significant investmentto improve public health preparedness after theSeptember 11, 2001 and the anthrax tragedies.The main funding streams have included bolsteringbasic federal capabilities; improving nationalvaccine and medication development, stockpilingand distribution; improving state, local andhospital preparedness; and a one-time fundinginflux to supp<strong>or</strong>t pandemic flu preparedness.While the funding has resulted in significantprogress in the past decade, the <strong>Ready</strong> <strong>or</strong> <strong>Not</strong>?rep<strong>or</strong>ts have documented a number of maj<strong>or</strong>gaps that still remain, particularly in maintaininga fully-staffed and trained w<strong>or</strong>kf<strong>or</strong>ce, vaccineand medical countermeasure research andproduction, biosurveillance programs, medicalsurge capacity and providing supp<strong>or</strong>t f<strong>or</strong> communitiesto cope with and respond to crises.Hist<strong>or</strong>ically, the federal approach to preparednesshas not provided a stable <strong>or</strong> sustained levelof supp<strong>or</strong>t f<strong>or</strong> federal, state <strong>or</strong> localities. Themost consistent pattern in U.S. preparednessfunding is inconsistency. These inconsistenciesmake it difficult f<strong>or</strong> states to maintain programs,capabilities and enough employees, particularlytrained scientific experts, f<strong>or</strong> emergencies.53
Preparedness requires ongoing funding dedicatedto ensure that basic capabilities are inplace and that experts have the training and systemsto quickly act in the face of emergencies.Ten years ago, the nation was caught off-guardwhen the public health system was unpreparedf<strong>or</strong> emergencies. Many c<strong>or</strong>e public health functions,including epidemiology, lab<strong>or</strong>at<strong>or</strong>ies andoutbreak surveillance were lacking. Reviews bythe IOM, CDC, GAO and other experts foundthe country’s public health “infrastructure hadgreatly deteri<strong>or</strong>ated.” 229, 230, 231 On top of that,little groundw<strong>or</strong>k was in place f<strong>or</strong> hospitalsand public health departments to respond tothe massive influx of potential anthrax samplesand there was a lack of co<strong>or</strong>dination, training,leadership and communication within the fieldand f<strong>or</strong> public health departments to w<strong>or</strong>k withother first responders.The United States has learned several lessonsfrom the September 11, 2001 and anthrax tragedies,Hurricane Katrina, the H1N1 pandemicflu and other emergencies, most notably thatbeing prepared means having:n Functional c<strong>or</strong>e public health systems in place,including epidemiology, lab<strong>or</strong>at<strong>or</strong>ies, communicationand outbreak surveillance; andn Emergency-specific training and systemsacross a variety of threats. Similar to militaryreadiness,public health emergency readinessnecessitates ongoing planning, training andupgrading of systems and technology.Basic preparedness involves:n Rapid detection of and response to emergencydisease threats, including those causedby bioterr<strong>or</strong>ism.n Intensive investigative capabilities to quicklydiagnose an infectious disease outbreak <strong>or</strong> toidentify the biological <strong>or</strong> chemical agent usedin an attack.n Surge capacity f<strong>or</strong> mass events, includingadequate facilities, equipment, supplies andtrained health professionals.n Mass containment strategies, including pharmaceuticalsneeded f<strong>or</strong> antibiotic <strong>or</strong> antidoteadministration and isolation and quarantiningwhen necessary.n Streamlined and effective communicationchannels so health w<strong>or</strong>kers can swiftly and accuratelycommunicate with each other, otherfront line w<strong>or</strong>kers, and the public about 1)the nature of an emergency <strong>or</strong> attack, 2) therisk of exposure and how to seek treatmentwhen needed, and 3) any actions they <strong>or</strong> theirfamilies should take to protect themselves.n Communication that is able to reach and takeinto consideration at-risk populations.n Streamlined and effective evacuation of atriskpopulations with special medical needs.n An inf<strong>or</strong>med and involved public that can providematerial and m<strong>or</strong>al supp<strong>or</strong>t to professionalresponders, and can render aid when necessaryto friends, family, neighb<strong>or</strong>s and associates.Dedicated funding is needed to supp<strong>or</strong>t theunique capabilities and training required tomaintain adequate levels of emergency preparedness,including:n Leadership, planning and co<strong>or</strong>dination: Anestablished chain-of-command and well definedroles and responsibilities f<strong>or</strong> seamlessoperation across different medical and logisticalfunctions and among federal, stateand local auth<strong>or</strong>ities during crisis situations,including police, public safety officials andother first responders.n C<strong>or</strong>e public health capabilities: Basic publichealth systems and equipment, including lab<strong>or</strong>at<strong>or</strong>ytesting and communications that keeppace with advances in science and technology.n An expert and fully-staffed w<strong>or</strong>kf<strong>or</strong>ce: Highlytrained and adequate numbers of publichealth professionals, including epidemiologists,lab scientists, public health nurses anddoct<strong>or</strong>s, and other experts, in addition toback-up w<strong>or</strong>kers f<strong>or</strong> surge capacity needs.n Modernized technology: State-of-the-art lab<strong>or</strong>at<strong>or</strong>yequipment, inf<strong>or</strong>mation collection andhealth tracking systems.n Rapid development and ability to manufacturevaccines and medications: A streamlined,safe, effective system to ensure rapid researchand production of medical countermeasuresto protect people from emerging threats.n Pre-planned, safety-first rapid emergency responsecapabilities and precautions: Testedplans and safety precautions to mitigate potentialharm to communities, public healthprofessionals and first responders.n Immediate, streamlined communications capabilities:Co<strong>or</strong>dinated, integrated communicationsamong all parts of the public healthsystem, frontline responders and the public.Communications capabilities must includeback-up systems in the event of power loss <strong>or</strong>overloaded wireless channels.54
It is also essential to consider the costs of respondingto disasters and the toll it takes onhealth departments — to find mechanisms toprovide supp<strong>or</strong>t f<strong>or</strong> rebuilding after an incidentand response have happened.The current economic situation is compoundingthe problems created by the hist<strong>or</strong>ic inconsistentfunding f<strong>or</strong> emergency preparedness.Combined federal, state and local budget cutsare resulting in the loss of c<strong>or</strong>e programs andfunctions and maj<strong>or</strong> staff losses. Even bef<strong>or</strong>ethe recession, federal supp<strong>or</strong>t f<strong>or</strong> preparednessbegan to decline. From FY 2005 to the proposedbudget in FY 2011, federal supp<strong>or</strong>t f<strong>or</strong>state and local activities via the PHEP grants hasdecreased by 27 percent, adjusted f<strong>or</strong> inflation.A decade of progress in preparedness is at risk dueto the cuts. Federal, state and local health departmentswill no longer be able to maintain basicfunctions needed to respond to emergencies.F<strong>or</strong> the future, this is likely to mean a relianceon emergency supplemental funding to try toquickly ramp up response eff<strong>or</strong>ts after an eventhas happened.This puts states and localities in the positionof trying to respond without c<strong>or</strong>e capabilities— and trying to build capacity during anemergency response. In these situations, as wasevident during the anthrax attacks and H1N1outbreak, states and localities have to deal withcontracting and bureaucratic restrictions, whichoften limit the ability to spend funds quickly <strong>or</strong>to enter into fast, sh<strong>or</strong>t-term contracts. Developingemergency capacity as an event is unfoldingis particularly challenging when health departmentsdo not know how long they will have resourcesto sustain their capabilities <strong>or</strong> needs.States and localities have rep<strong>or</strong>ted it will takethem longer to achieve the 15 national capabilitiesf<strong>or</strong> public health preparedness due to limitedresources. 232Many states and localities have taken creativeapproaches to budget and spending restrictions,such as making flexible use of their publichealth employees during disasters, to reassignindividuals to other duties f<strong>or</strong> the time of emergencies.But in some cases, federal grants restrictthis ability if the personnel are funded tosupp<strong>or</strong>t other specific programs, such as maternaland child health. CDC and ASPR are currentlyw<strong>or</strong>king with the states and localities tofind ways to be able to make quick use of emergencysupplemental funds easier, but emergencysupp<strong>or</strong>t cannot fill ongoing gaps.RECOMMENDATIONSIn addition to dedicated and sustained supp<strong>or</strong>tf<strong>or</strong> preparedness, TFAH also recommends a seriesof actions to ensure preparedness fundingis m<strong>or</strong>e predictable, to cut down on federal bureaucraticred tape and to ensure flexibility sothat when emergencies happen, resources andemergency supplemental supp<strong>or</strong>t can be usedquickly and effectively. This eff<strong>or</strong>t requires:n Establishing multi-year grant cycles withgreater flexibility in states’ retention and useof carry f<strong>or</strong>ward and unexpended funds;n Creating a mechanism to fast track the awardingand programming of emergency supplementalfunds into existing grant mechanismswithout additional requirements;n Granting auth<strong>or</strong>ity to the U.S. Secretary ofHHS to allow states to also use personnelthat are part of other federal programs in responseto a public health emergency; andn Improving co<strong>or</strong>dination among emergency preparednessgrant programs, including PHEP,HPP, FEMA and CDC grants, through increasedleadership and direction and by encouragingunif<strong>or</strong>mity of guidelines and requirements tomaximize efficiency, carrying out the MOUagreements that the agencies have entered into.55
Overview of Federal Funding f<strong>or</strong> Preparedness Since 2001In early 2002, HHS announced $1.1 billion infunding f<strong>or</strong> state public health, hospital andmedical preparedness planning f<strong>or</strong> a bioterr<strong>or</strong>istevent. 233 In June 2002, Congress passed thePublic Health Security and Bioterr<strong>or</strong>ism Act andappropriated new federal funds to fill gaps andhelp modernize the public health system to beable to respond to bioterr<strong>or</strong> and health threats.The funds were devoted to:n Improving national capabilities and policies atCDC and other areas within HHS;n Expanding the SNS, which is a federal reposit<strong>or</strong>yof vaccines, medications and other medicalequipment f<strong>or</strong> use in emergencies;n Creating a medical reserve c<strong>or</strong>ps and volunteernetw<strong>or</strong>ks f<strong>or</strong> supp<strong>or</strong>t; andn Developing two grant new programs, PHEP,which supp<strong>or</strong>ts state and local public healthpreparedness, was initially funded just under$1 billion annually in FY 2003 — and theHospital Preparedness Program (HPP) wasfunded at around $400 million annually.In 2004, Congress passed the BioShield Actand appropriated $5.6 billion to help fill a maj<strong>or</strong>gap in the country’s ability to quickly developand procure vaccines and other medicationsthat could be needed to prevent <strong>or</strong> respond tohealth threats.In 2005 and 2006, following Hurricanes Katrinaand Rita, national awareness of the implicationsof a potential pandemic flu outbreak made itclear that while initial progress had been madeto begin to improve federal, state and localpublic health preparedness, maj<strong>or</strong> areas of vulnerabilitycould not be addressed with the levelof resources provided. In 2005, President Bushannounced the National Strategy f<strong>or</strong> PandemicInfluenza and in FY 2006, Congress appropriatedm<strong>or</strong>e than $5.6 billion in one-time funds tosupp<strong>or</strong>t pandemic flu preparedness activities,particularly to supp<strong>or</strong>t vaccine research, productionand delivery and surveillance, and included$600 million in grants to state and local healthdepartments.In 2006, Congress passed PAPHA, reauth<strong>or</strong>izingthe 2002 bill to expand the focus towardm<strong>or</strong>e of an “all-hazards” approach to improvereadiness f<strong>or</strong> a wider range of potential threats.The bill created ASPR to better co<strong>or</strong>dinate anddevelop policy at HHS, which included BARDAto provide an integrated, systematic approach tothe development and purchase of the necessaryvaccines, drugs, therapies and diagnostic toolsf<strong>or</strong> public health medical emergencies, whichincludes overseeing Project BioShield, as well astaking over management of the medical reservec<strong>or</strong>ps and volunteer programs, the HPP grantsand other programs.When the H1N1 pandemic flu began, Congressallocated m<strong>or</strong>e than $8 billion in one-time fundsin FY 2009 to fill immediate needs and gaps to234, 235respond to the outbreak.CDC Office of Public Health Preparedness and Response Funding Totalsand Select ProgramsFY 2002 FY 2003 FY 2004 FY 2005 FY 2006 FY 2007 FY 2008 FY 2009 FY 2010 FY 2011 TOTALFY 2012(Requested)CDC Total $1,747,023,000 $1,533,474,000 $1,507,211,000 $1,622,757,000 $1,631,173,000 $1,472,553,000 $1,479,455,000 $1,514,657,000 $1,522,339,000 $1,415,416,000 $13,460,863,000 $1,452,618,000State andLocalPreparedness $940,174,000 $1,038,858,000 $918,454,000 $919,148,000 $823,099,000 $766,660,000 $746,039,000 $746,596,000 $760,986,000 $664,294,000 $8,324,308,000 $651,048,000and ResponseCapability*SNS $645,000,000 $298,050,000 $397,640,000 $466,700,000 $524,339,000 $496,348,000 $551,509,000 $570,307,000 $595,661,000 $591,001,000 $5,136,555,000 $655,000,000*Includes Public Health Emergency Preparedness (PHEP) cooperative agreements, Centers f<strong>or</strong> Public Health Preparedness, Advanced Practice Centers (FY2004-09),Cities Readiness Initiative, U.S. Postal Service Costs (FY 2004), All Other State and Local Capacity, and Smallpox Supplement (FY 2003)CDC FundingSource: FY 2002-09: http://www.cdc.gov/phpr/publications/2010/Appendix3.pdfSource: FY 2010-11: U.S. Centers f<strong>or</strong> Disease Control and Prevention. 2011 Operating Plan. http://www.hhs.gov/asfr/ob/docbudget/2011operatingplan_cdc.pdf.Source: FY 2012: http://www.cdc.gov/fmo/topic/Budget%20Inf<strong>or</strong>mation/appropriations_budget_f<strong>or</strong>m_pdf/FY2012_CDC_CJ_Final.pdf, p. 25556
Office of Assistant Secretary f<strong>or</strong> Prepardness and Response FundingTotals and Select ProgramsFY 2002 FY 2003 FY 2004 FY 2005 FY 2006 FY 2007 FY 2008 FY 2009 FY 2010 FY 2011 TOTAL FY 2012(Requested)ASPR Totals -- -- -- -- $632,000,000 $694,280,000 $632,703,000 $788,191,000 $891,446,000 $891,000,000 $4,529,620,000HPP^ $135,000,000 $514,000,000 $515,000,000 $487,000,000 $474,000,000 $474,030,000 $423,399,000 $393,585,000 $425,928,000 $383,858,000 $4,225,800,000BARDA -- -- -- $5,000,000 $54,000,000 $103,921,000 $101,544,000 $275,000,000 $304,948,000 $415,000,000 $1,259,413,000Bioshield Special-- -- $5,600,000,000* -- -- -- -- -- -- -- -Reserve Fund* One-time Funding^HPP moved from HRSA to ASPR in 2007Source: HPP FY 2002: http://archive.hhs.gov/budget/04budget/fy2004bib.pdf, p. 14Source: HPP FY 2003: http://archive.hhs.gov/budget/05budget/fy2005bibfinal.pdf, p. 16Source HPP FY 2004:http://archive.hhs.gov/budget/06budget/FY2006BudgetinBrief.pdf, p. 16Source: HPP FY 2005: http://archive.hhs.gov/budget/07budget/2007BudgetInBrief.pdf, p. 20Source: BARDA FY 2005-06: http://www.hhs.gov/asrt/ob/docbudget/2010phssef.pdf, p. 45.Source: FY 2006: http://www.hhs.gov/asfr/ob/docbudget/2008budgetinbrief.pdf, p. 109Source: FY 2007: http://www.hhs.gov/budget/09budget/budgetfy09cj.pdf, p. 288Source: FY 2008-09: http://www.hhs.gov/asfr/ob/docbudget/2010phssef.pdf, p. 8Source: FY 2010-11: http://www.hhs.gov/asfr/ob/docbudget/2011operatingplan_phssef.pdfSource: FY 2012: http://www.hhs.gov/about/FY2012budget/phssef_cj_fy2012.pdf, p. 11Flu Funding Totals and Select ProgramsFY 2004 FY 2005 FY 2006 FY 2007 FY 2008 FY 2009 FY 2010 FY 2011 TOTALFY 2012(Requested)Flu Tota1 $50,000,000 $183,000,000 $5,590,000,000* $138,000,000 $299,000,000 $8,456,000,000 $572,000,000 $300,525,000 $9,998,525,000State and LocalPandemic GrantsVaccineDevelopment andPurchase-- -- $600,000,000^ -- -- $1,444,000,000 -- -- $1,444,000,000$50,000,000 $183,000,000 $2,963,000,000 -- -- $1,944,000,000 $158,000,000 -- $5,298,000,0001 May include HHS agency budgets, Office of the Secretary and one-time funding.^ Appropriated in FY2006 to be used over the following three years* Obligated over three yearsFlu FundingSource: FY 2004-05: http://www.fas.<strong>or</strong>g/sgp/crs/misc/RS22576.pdf, p. 2-3Source: FY 2006: http://www.hhs.gov/asfr/ob/docbudget/2008budgetinbrief.pdf, p. 105Source: FY 2007: http://www.hhs.gov/budget/09budget/2009BudgetInBrief.pdf p. 107Source: FY 2008: http://dhhs.gov/asfr/ob/docbudget/2010budgetinbrief.pdf p. 107Source: FY 2009: http://dhhs.gov/asfr/ob/docbudget/2011budgetinbrief.pdf, p. 9Source: FY 2010: http://dhhs.gov/asfr/ob/docbudget/2011budgetinbrief.pdf p. 104Source: FY 2011: C<strong>or</strong>respondence with Liz DeVoss at HHS November 4, 2011Source: FY 2012: http://www.hhs.gov/about/FY2012budget/fy2012bib.pdf, p. 757
Prevention and Public Health Fund: BuildingPrepared CommunitiesThe Aff<strong>or</strong>dable Care Act (ACA) included thecreation of a Prevention and Public Health Fund(Fund) to provide communities around thecountry $16.5 billion over the next 10 years toinvest in effective, proven prevention eff<strong>or</strong>tsand to build the public health infrastructure. TheFund is being used to supp<strong>or</strong>t community andclinical prevention eff<strong>or</strong>ts, strengthen state andlocal health departments and the public healthw<strong>or</strong>kf<strong>or</strong>ce, and supp<strong>or</strong>t science and research.The Fund has the potential to have a tremendousimpact on the nation’s preparedness. The Fundis helping to build resilient communities throughinvestments in:n Lab<strong>or</strong>at<strong>or</strong>y and epidemiology capacity — PreventionFund money has been used to hireand train epidemiologists and lab<strong>or</strong>at<strong>or</strong>y scientistsand expand the number of public healthlab<strong>or</strong>at<strong>or</strong>ies using electronic lab<strong>or</strong>at<strong>or</strong>y inf<strong>or</strong>mationsystems. 236, 237 As part of public healthinfrastructure grants, HHS is also promotingthe capacity of health departments to useelectronic health rec<strong>or</strong>ds through participationin electronic lab<strong>or</strong>at<strong>or</strong>y rep<strong>or</strong>ting and traininghealth inf<strong>or</strong>mation specialists. These specializedsystems are critical to the public healthsystem’s ability to quickly detect, pinpoint andrespond to an emergency such as an emerginginfectious disease <strong>or</strong> foodb<strong>or</strong>ne outbreak.n W<strong>or</strong>kf<strong>or</strong>ce training and fellowships — Grantsmay help mitigate the devastating impact ofbudget cuts on the public health w<strong>or</strong>kf<strong>or</strong>ce,allowing m<strong>or</strong>e trained personnel to engage inpreparedness and response activities.n Immunizations — Grants have been allocatedto improve the Immunization Inf<strong>or</strong>mationSystems (registries) and other immunizationinf<strong>or</strong>mation technologies and to expand adultimmunization programs and vaccination capacityin schools. 238 Growing the ability to quicklyand accurately vaccinate the population andimproving vaccine access and acceptance willbe vital during an infectious pandemic that requiresmass vaccination of the public.n Community prevention — In addition to accessto vaccines and clinical prevention, theFund is supp<strong>or</strong>ting chronic disease preventionthrough community-level eff<strong>or</strong>ts to combatobesity, tobacco use, and po<strong>or</strong> nutrition. Individualswith chronic conditions are particularlyvulnerable during a disaster because of theneed f<strong>or</strong> specialized equipment and medicinesand difficulty with evacuation and sheltering.Healthy communities, with an inf<strong>or</strong>med populationand strong connections between thepublic, healthcare system, and public health,are better able to weather a disaster.58
EXPERT COMMENTARYA Decade of Public Health Preparedness:A Focus on OregonBy Mel Kohn, M.D., MPH, State Health Officer and Public Health Direct<strong>or</strong>, Oregon Health Auth<strong>or</strong>ityImust be getting old because I remember the days bef<strong>or</strong>e wehad a public health preparedness program. Outbreak investigationswere handled almost exclusively by our communicable diseaseepidemiologists. Even in Oregon, which witnessed the onlybioterr<strong>or</strong>ist incident on US soil in recent mem<strong>or</strong>y pri<strong>or</strong> to 2001— the salmonella outbreak engineered by followers of BhagwanShree Rajneesh in a small town near the Dalles, Oregon — preparednesswas not a c<strong>or</strong>e public health activity. It almost seemsquaint in retrospect, but I remember when we got our first federalpreparedness grant, and used it to hire a single staff person.But everything changed with the 9/11 and anthrax attacksof 2001. These events, together with the SARS outbreak of2003 and Hurricane Katrina in New Orleans in 2005, spurreda dramatic federal investment in public health preparednessat the state and local level. After many years of neglect of thepublic health infrastructure, preparedness dollars were usedto plug holes in our fraying epidemiologic and lab<strong>or</strong>at<strong>or</strong>y infrastructure,as well as to build new capacity in incident commandstructures, agency operations centers, and communications.In Oregon, here’s a list of some of the most imp<strong>or</strong>tant thingsthat these investments have bought f<strong>or</strong> us:n Capacity f<strong>or</strong> lab<strong>or</strong>at<strong>or</strong>y testing that enables us to investigateand respond to threats in a m<strong>or</strong>e timely way (think the spateof white powder incidents in the wake of the anthrax attacks,<strong>or</strong> the rapid testing in-state of flu samples during theH1N1 influenza pandemic);n 24-7 responsiveness of the public health system so whensomeone calls the health department f<strong>or</strong> an emergencythere is someone to answer the phone and provide help;n Communications hardware, software and training that enable us toprovide accurate and timely inf<strong>or</strong>mation to the public — the bestantidote to the fear and anxiety that are a maj<strong>or</strong> part of any disaster;n The ability to use incident command methodology so thatwe can quickly and effectively communicate with partnersin other agencies and utilize the state and local emergencymanagement system including our National Guard; andn The capacity to monit<strong>or</strong> healthcare system capacity andneeds so that life-saving resources in sh<strong>or</strong>t supply during anemergency can be targeted to where they are most needed.These investments have yielded substantial returns numerous timesin recent years. Without our preparedness program, our responseto the (hopefully) once-in-a-lifetime H1N1 influenza pandemicwould have been impossible to mount; we could not have effectivelyco<strong>or</strong>dinated vaccine distribution, provided inf<strong>or</strong>mation to the publicand monit<strong>or</strong>ed and helped manage our health care systems’ needs.Because Oregon is on the Pacific rim, there was a very high level ofconcern about how the nuclear accident in Japan would affect thesafety of our food and water. Our Agency Operations Center andour communications skills and infrastructure made it possible f<strong>or</strong> usto provide reliable inf<strong>or</strong>mation to a fearful public on these issues.While by definition none of us can predict what the next maj<strong>or</strong>emergency will be, climate change, regardless of one’s beliefsabout its causes, is likely to be a maj<strong>or</strong> fact<strong>or</strong>. Climate change-relatedextreme weather events such as floods, f<strong>or</strong>est fires, droughtsand heat waves, are already becoming m<strong>or</strong>e common, and each ofthese will bring the potential f<strong>or</strong> serious health effects that a robustpublic health preparedness system can do a great deal to mitigate.Today there is no doubt that the public expect the public health systemto have the capability to competently protect their health duringemergencies. This is not an optional service. So in the face ofmaj<strong>or</strong> budget cuts, how will we be able to meet those expectations?We should use this budget crisis to look f<strong>or</strong> efficiencies and newways of w<strong>or</strong>king that will enable us to stretch our dollars further.F<strong>or</strong> example, integration of healthcare and community-basedpreparedness activities could yield some efficiencies, and shouldbe done whether <strong>or</strong> not there is a budget crisis. But it’s fantasy tothink that we will be able to abs<strong>or</strong>b reductions of this magnitudesimply by finding efficiencies. Next year we are expecting additionalreductions in federal preparedness funding. Should theycome to pass, public health in Oregon will be f<strong>or</strong>ced to reduce ourcapacity in some serious ways that will not be overcome by findingefficiencies. We have reached the point where we will lose groundon the investments we’ve made, and our ability to do this w<strong>or</strong>k willbe seriously compromised, with life and death consequences.It’s difficult to predict how <strong>or</strong> where the funding-induced deficienciesin our preparedness system will manifest themselves. New Orleanssurvived f<strong>or</strong> many years, despite design defects and insufficientmaintenance of its levee system. Funds that would have been spenton the levees were used f<strong>or</strong> other pri<strong>or</strong>ities that probably seemedm<strong>or</strong>e urgent at the time. Those funding decisions either went unnoticed,<strong>or</strong> perhaps were even applauded as good stewardship ofpublic funds. And each individual decision about funding may haveappeared at the time as if it could be abs<strong>or</strong>bed with little impact.But in the hindsight of Hurricane Katrina, it’s clear that over timethe net effect of all those decisions was disastrous and tragic.We should think of our public health preparedness system as a leveesystem that protects us at times of critical need and cannot be fixedon the spur of the moment. Can we really aff<strong>or</strong>d to let that erode?59
Training and Exercises: Maj<strong>or</strong> Component of ReadinessTraining and exercises are essential f<strong>or</strong> public healthw<strong>or</strong>kers to be ready f<strong>or</strong> emergencies. Training isimp<strong>or</strong>tant so public health w<strong>or</strong>kers have the skillsto perf<strong>or</strong>m in situations that are outside of day-todayactivities, so they are prepared ahead of time todeal with unexpected issues that arise during crises.Exercises provide public health w<strong>or</strong>kers the opp<strong>or</strong>tunityto test out their plans and capabilitiesbef<strong>or</strong>e an actual event arises, and are an imp<strong>or</strong>tantaspect of training, to understand roles andresponsibilities during crises and to understandhow to co<strong>or</strong>dinate with other first responders.These are often the only time and mechanismf<strong>or</strong> understanding the roles and responsibilities ofother first responders — and often the only wayother first responders, ranging from fire and policedepartments, gain an understanding of the capabilitiesand limits that public health departmentshave. They are essential f<strong>or</strong> minimizing confusionand maximizing efficiency during emergencies.Acc<strong>or</strong>ding to a June 2011 paper, The Impact ofState and Local Budget Cuts on Public HealthPreparedness, by PRTM, commissioned by theIOM, “from table-top exercises to m<strong>or</strong>e realisticevent simulations, exercises provide a chance toanalyze the strengths, weaknesses, and areas ofimprovement in public health response.” 239The paper found that training “has been one ofthe first areas to be de-pri<strong>or</strong>itized during budgetcuts. In general, state and local health departmentsare running low funding, human resourcesand time necessary to train staff…. Eff<strong>or</strong>ts tostandardize and align training throughout thestates, such as by integrating c<strong>or</strong>e curricula andstandardizing c<strong>or</strong>e competencies, have also suffered.”240 In addition, acc<strong>or</strong>ding to the paper,exercises are being cut back, particularly in scopeand sophistication.60
EXPERT PerSPECTIVEImproving Collab<strong>or</strong>ation between Federal, Stateand Local agencies in Planning f<strong>or</strong> a W<strong>or</strong>st CaseScenario: A Broad Aerosolized Dispersal ofWeaponized Anthrax in a Maj<strong>or</strong> Metropolitan AreaBy Alonzo Plough, PhD, MPH, Direct<strong>or</strong>, Emergency Preparedness and Response of the Los Angeles County Department of Public Healthand Member of the Board of Direct<strong>or</strong>s of the Trust f<strong>or</strong> America’s HealthOnSeptember 8, 2011, the Los Angeles County Departmentof Public Health hosted a tabletop exerciserequested by FEMA’s National Exercise Division’s. Goals wereto review and discuss emergency response plans, policies,and procedures f<strong>or</strong> rapid MCM dispensing. The exercise wasprompted by Presidential Executive Order 13527 to establishthe federal capability f<strong>or</strong> the timely provision of MCM followinga biological attack, and involved several federal agenciesincluding DHS, FEMA, HHS, CDC, DoD, and others.Even though Los Angeles County and other large urban areashave w<strong>or</strong>ked extensively with the CDC, especially under theCities Readiness Initiative (CRI) — which is directly responsiblef<strong>or</strong> enhancing our ability to distribute MCMs through the SNS— this w<strong>or</strong>k was not well known by many other federal agencies,including those who could play an integral role in WMDresponse. The exercise expanded the list of federal agenciesparticipating in this planning, and aligned them on how theycould best supp<strong>or</strong>t local and state eff<strong>or</strong>ts to provide prophylaxisto at-risk populations within 48-hours of a decision to dispenseif aerosolized weaponized anthrax was broadly dispersed usingthe newly drafted Federal Interagency Concept of Operations(CONOPS)—Rapid Medical Countermeasures Dispensing.Months bef<strong>or</strong>e we began planning f<strong>or</strong> the exercise, Los AngelesCounty had begun w<strong>or</strong>king with the Department ofDefense N<strong>or</strong>thern Command to develop interagency plans f<strong>or</strong>rapid medical countermeasure dispensing in an anthrax-typeevent (the w<strong>or</strong>st case scenario f<strong>or</strong> a widespread weapons ofmass destruction (WMD) type event). At the request of theNational Security Council and White House, we welcomedthe opp<strong>or</strong>tunity to show how ready large jurisdictions are t<strong>or</strong>espond to such an event, and how willing we are to partnerwith federal agencies to further improve timely response.The goal during those meetings was to develop DoD’s conceptof operations and to establish requirements f<strong>or</strong> a federal rapidresponse to dispense MCM to an affected population followinga large-scale biological attack. In sh<strong>or</strong>t, the DoD wanted to learnfrom us how we would respond to a WMD situation, what resourcesand plans we had in place and how best they could supp<strong>or</strong>tour eff<strong>or</strong>ts to <strong>or</strong>ganize and distribute federal resources.The DoD came to Los Angeles in December of 2009, andwent through our anthrax response plans in detail. Theyquickly learned that we had been doing this planning, trainingand testing f<strong>or</strong> nearly a decade under CRI, and that these planshad been strengthened and honed by experiences during theH1N1 pandemic. The agency began to digest what supp<strong>or</strong>tingroles they could play to improve response to a WMD event.In March of 2011, we met in Col<strong>or</strong>ado Springs at N<strong>or</strong>thern Commandheadquarters with representatives from DoD, DHS, HHS,CDC, and the City of Chicago and District of Columbia healthdepartments to develop the Commander’s estimate f<strong>or</strong> deployingDoD assets (f<strong>or</strong> example, the National Guard) in this kind of scenario.The focus was on what kind of supp<strong>or</strong>ts could be deliveredto large urban areas such as Los Angeles County in 24 hours. At thispoint, this project showed the wonderful interaction between publichealth and DoD — something that had not previously existed. Asa result, DoD realized the agency had to adopt and adapt strategiesto what public health had already built up and put in place. Thesefindings, plans and outcomes were taken to the Pentagon.Following this planning project, this summer, we received arequest from the White House to host a national level anthraxexercise, with an eye toward the 10th anniversaries of the 9/11and anthrax tragedies. The objectives of the exercise were to:n Examine the approach and mechanisms f<strong>or</strong> <strong>or</strong>ganizing andmanaging the federal response to supp<strong>or</strong>t medical countermeasuredispensing operations in a large urban area as outlinedin the draft the Federal Interagency CONOPS–MCMRapid Dispensing;n Assess the viability of the Federal Interagency CONOPS–MCM Rapid Dispensing; andn Identify policy and operational issues associated with the effectivenessand timeliness of the federal capability to supp<strong>or</strong>tinitial State and local dispensing of MCM.In addition to the federal agencies mentioned above, state andnational guards, local, county and state health departments,city, county and state emergency management agencies andlocal/first responders (fire, police, etc.) took part.61
EXPERT PerSPECTIVE continuedImproving Collab<strong>or</strong>ation between Federal, State andLocal agencies in Planning f<strong>or</strong> a W<strong>or</strong>st Case ScenarioThe exercise was based on a massive anthraxattack that was identified by multiple Biowatchmonit<strong>or</strong>s across the county. It was designed f<strong>or</strong>a “w<strong>or</strong>st case” type scenario: broad aerosolizeddispersal of weaponized anthrax. We did notdesign the exercise to test capabilities beyonddispensing to focus the play (i.e., what happensonce an attack is identified and whether 10 millionpeople could receive prophylaxes in 48hours). Hopefully, at the end, we would have theframew<strong>or</strong>k of how the federal family could assiststate and local government in improving timelyresponse during such a situation.The exercise went extremely well. Planning f<strong>or</strong>it opened a dialogue between federal responseagencies and public health. Pri<strong>or</strong> to this exercise,there had not really been a deep knowledgeat DHS, FEMA <strong>or</strong> DoD of all that was accomplishedby the CDC investments, especially indirectly funded cities like LA. Federal agenciescame out of the exercise with a much cleareridea of what local and state capabilities had beenbuilt up through CDC funding. Specifically, opp<strong>or</strong>tunitiesf<strong>or</strong> federal MCM supp<strong>or</strong>t in the first48-hours were identified in the area of logistics(drivers and vehicles, <strong>or</strong> access to federal logisticscontract<strong>or</strong>s to move supplies to dispensingsites), and less so on access to federal personnelto assist with dispensing because of planning eff<strong>or</strong>tswith DoD. The exercise also provided thebackdrop f<strong>or</strong> a good discussion of what types ofnearby federal resources can be put into place(postal trucks, military bases, people etc.) in the48 hour dispensing window.Basically, the participating federal agencies learnedabout the return on investment from the CDCdollars and saw that local MCM distribution planswere solid and had been tested both throughannual exercises and actual response during theH1N1 pandemic. Bef<strong>or</strong>e the exercise, there justwasn’t a lot of knowledge about the planning,training, exercises and perf<strong>or</strong>mance measure requirementsthat go with the CRI — there wasn’twidespread understanding of the accountabilitymechanisms that have been in place f<strong>or</strong> years.While the exercise was successful, it did exposesome gaps in a unified federal-state-local responseto a WMD. There is clearly still confusion and lackof widespread inf<strong>or</strong>mation on the capabilities oflarge urban areas (especially if you look the WMDCenter Bio-Response Rep<strong>or</strong>t Card which wasreleased on October 12, 2011). The exercise andthat rep<strong>or</strong>t card reflects a lack of engagement andunderstanding of the great successes and advancesthat have been made in high threat areas as a resultof CDC funding, particularly f<strong>or</strong> MCMs.As a result of these meetings and the exercise,we were able to show how federal investmenthas improved local response to WMDs, andhow closer interagency planning can improveresponse even further. This w<strong>or</strong>k is not finished;if these resources don’t continue <strong>or</strong> are cut,we’re in trouble. The public health emergencypreparedness budget should be protected thesame way other national security budgets areprotected.Over the last ten years, through the CDC fundingand CRI, large urban areas have built up atremendous capacity to respond to and stave offa WMD attack. CDC should be applauded f<strong>or</strong>what they have put on the ground, especially inhighly populated high threat large urban areas.Quite simply, there is a logic of preparedness andresponse that operates inside the Beltway that issometimes div<strong>or</strong>ced from what has been accomplishedby and what would happen in the rest ofthe country during a WMD attack. It is encouragingthat federal agencies are reaching out to localand state governments to see what has beenbuilt, and to develop interagency plans to improvereadiness to response. This enhanced partnershipwill allow us to save lives, reduce human suffering,and speed recovery after a WMD attack.62
B. Improving Biosurveillance:The United States lacks an integrated, nationalapproach to biosurveillance — which hampersthe country’s ability to rapidly detect and trackbioterr<strong>or</strong>ism attacks <strong>or</strong> disease outbreaks.In a 2009 review, the National BiosurveillanceAdvis<strong>or</strong>y Subcommittee (NBAS) found that there“are m<strong>or</strong>e than 300 separate biosurveillance eff<strong>or</strong>tsunderway in various federal, state and localgovernment agencies. These eff<strong>or</strong>ts are, f<strong>or</strong> themost part, neither integrated n<strong>or</strong> interoperable,and propose to serve an array of purposes. Theeffectiveness of many of these systems remainsuntested and, in some cases, undefined.” 241The existing structure is an ass<strong>or</strong>tment of manydifferent systems that were built one disease <strong>or</strong>crisis at a time, and the result is a set of fragmented,unco<strong>or</strong>dinated systems that cannotshare inf<strong>or</strong>mation effectively <strong>or</strong> quickly.Remaining constantly aware of surroundingthreats and our capacity to respond is critical todealing with emergencies. The U.S. disease surveillancesystem has been built one disease <strong>or</strong> crisisat a time, resulting in archaic and static silosof inf<strong>or</strong>mation rather than as an interoperablesystem with a focus on prevention. Fixing thesystem will require that the nation fundamentallyrethinks how to do biosurveillance — f<strong>or</strong> bothemergencies and routine public health issues.The particular challenge in the field of preparednessis that officials don’t necessarily know in advancewhat they will need to know, and thus themost comprehensive approach to data collectionis needed. Right now, the fragmented system ofdata rep<strong>or</strong>ting drastically weakens our nation’sdefense against emergency outbreaks.Improving the system means harnessing the opp<strong>or</strong>tunitiesaff<strong>or</strong>ded by the nation’s transitionto an integrated health inf<strong>or</strong>mation technology(HIT) system with electronic health rec<strong>or</strong>ds atthe c<strong>or</strong>e. This could create economies of scaleand provide m<strong>or</strong>e useful inf<strong>or</strong>mation to publichealth and national security officials. Currently,the White House is examining the national biosurveillancesystem. TFAH believes that anynew national strategy should examine means toachieve interoperability, efficiency, and transparencyamong various surveillance systems in<strong>or</strong>der to create an integrated biosurveillanceoperation. In particular, HIT must strengthenmeaningful use requirements, which currentlycontain weak public health rep<strong>or</strong>ting requirements.Building the capacity of health departmentsto receive this data started through grantsfrom the Recovery Act and Prevention and PublicHealth Fund, but these investments need tocontinue and grow. TFAH also urges ongoing,enhanced communication between Congress,CDC and the Office of the National Co<strong>or</strong>dinat<strong>or</strong>f<strong>or</strong> Health IT (ONC) to ensure that ONC considersthe preparedness implications of EHRs.RECOMMENDATIONSTFAH recommends modernizing and co<strong>or</strong>dinatingthe biosurveillance system — using up-to-datehealth inf<strong>or</strong>mation technology (HIT) to be ableto receive, compile and analyze data in a m<strong>or</strong>erapid and accessible fashion. This requires:n Implementing a new national strategy thatexamines means to achieve interoperability,efficiency and transparency among varioussurveillance systems in <strong>or</strong>der to create an integratedbiosurveillance operation;n Leveraging new epidemiological data thatresults from health IT developments andelectronic health rec<strong>or</strong>ds (EHRs) throughenhanced communication between CDC andthe Office of the National Co<strong>or</strong>dinat<strong>or</strong> f<strong>or</strong>Health Inf<strong>or</strong>mation Technology (ONC);n Ensuring the system includes electronic rep<strong>or</strong>tingof lab<strong>or</strong>at<strong>or</strong>y test requests and results; andn Allowing Poison Control Centers to be eligible f<strong>or</strong>grants to establish surveillance netw<strong>or</strong>ks, alongwith hospitals, public health and other facilities.63
The Current State of BiosurveillanceBiosurveillance is complicated by the fact that:n Different data is required f<strong>or</strong> detecting andmanaging different types of emergencies;n Health departments rely on receiving inf<strong>or</strong>mationfrom hospitals and doct<strong>or</strong>s — and thereis often a lag time in the transmission of thatinf<strong>or</strong>mation and another lag in the types oftechnologies used (phone rep<strong>or</strong>ts, faxes, emailsthat are not linked directly to databases).Currently, only a small number of health departmentshave agreements with hospitals toobtain direct access to a hospital’s electronicmedical rec<strong>or</strong>ds f<strong>or</strong> investigations; andn Many health departments lack the capacityto receive and analyze data from electronichealth rec<strong>or</strong>ds.Recent developments in HIT — both from thestandpoint of technologies and standardization —are providing new opp<strong>or</strong>tunities to rethink and harnessnew capabilities f<strong>or</strong> biosurveillance. Issues ofhow to quickly and effectively standardize, transfer,s<strong>or</strong>t, analyze and st<strong>or</strong>e data are keys f<strong>or</strong> building aneffective system. Maj<strong>or</strong> retail chains, which rapidlytrack invent<strong>or</strong>ies and customer patterns, and insurancecompanies, could serve as models f<strong>or</strong> developingsuch a system that tracks health patterns,claims and billings, among other fact<strong>or</strong>s. .Acc<strong>or</strong>ding to a recent study from Harvard Universityresearchers, allowing practitioners (hospitals, doct<strong>or</strong>sand clinicians) access to data on infections in theircommunity as diagnoses occur would greatly improvepatient care. While hospitals, clinics and doct<strong>or</strong>srep<strong>or</strong>t symptoms to public health departments,the inf<strong>or</strong>mation typically stops there. If two doct<strong>or</strong>sin different hospitals rep<strong>or</strong>t the same symptoms,it is unlikely they will ever know there are similarcases in a neighb<strong>or</strong>ing hospital. However, based onthe Harvard study, if there were real-time relays ofinf<strong>or</strong>mation, m<strong>or</strong>e than 166,000 patients would beprevented from receiving unnecessary antibiotics totreat suspected strep throat, f<strong>or</strong> example. 242Moving from the current system, which is comprisedof a range of different systems in each stateand f<strong>or</strong> different diseases and health conditions,to a standardized, interoperable, rapid system willrequire a full modernization of U.S. biosurveillance.F<strong>or</strong> instance, a recent rep<strong>or</strong>t from GAOoutlined a set of common challenges state andcity official identified as obstacles to developingand maintaining their biosurveillance capabilities:“(1) state policies that restrict hiring, travel,and training in response to budget constraints;(2) ensuring adequate w<strong>or</strong>kf<strong>or</strong>ce, training, andsystems; and (3) the lack of strategic planning andleadership to supp<strong>or</strong>t long-term investment incross-cutting c<strong>or</strong>e capabilities, integrated biosurveillance,and effective partnerships.” 243Key findings from a November 2011 article examiningthe state of biosurviellance in the UnitedStates today in Biosecurity and Bioterr<strong>or</strong>ism:Biodefense Strategy, Practice, and Science by theCenter f<strong>or</strong> Biosecurity of UMPC included that: 2441. A single comprehensive biosurveillance systemis probably not possible, and many systemswould be needed.2. Rapid lab<strong>or</strong>at<strong>or</strong>y rep<strong>or</strong>ting <strong>or</strong> clinical carerep<strong>or</strong>ting are the most imp<strong>or</strong>tant means bywhich health departments detect outbreaks.3. Public health departments have systems toanswer a number of the key outbreak questions,but this takes time.4. Private sect<strong>or</strong> medical resource and logisticalinf<strong>or</strong>mation is often not readily available topublic health departments.5. State and local health agencies do not havesufficient numbers of professionals with thespecial skills needed to build <strong>or</strong> run biosurveillancesystems.6. Federal grant language may prevent healthdepartments from reassigning staff during apublic health crisis.7. Exchange of electronic health inf<strong>or</strong>mationbetween clinical and public health communitieshas the potential to substantially improvebiosurveillance.8. State and local public health inf<strong>or</strong>mation technologyinfrastructure has improved over time, butbudget cuts threaten to erode this infrastructure.The auth<strong>or</strong>s provided a series of recommendations,including to:1. Provide appropriate levels of funding and explicitgrant guidance f<strong>or</strong> state and local publichealth surveillance.2. Improve public health agencies’ ability to accessand use electronic health inf<strong>or</strong>mation.3. Promote the integration of electronic lab<strong>or</strong>at<strong>or</strong>yrep<strong>or</strong>ting and electronic death registries.4. Address key gaps in biosurveillance f<strong>or</strong> respondingto public health emergencies: advanced epidemiologyand supply/logistical inf<strong>or</strong>mation.64
EXPERT COMMENTARYSurveillance: Essential f<strong>or</strong> Public HealthPreparedness and ResponseBy, Jeffrey Engel, M.D.; State Health Direct<strong>or</strong>, Division of Public Health, N<strong>or</strong>th Carolina Department of Health and Human ServicesSurveillance, the Science of GatheringData on PopulationsSurveillance has always been a c<strong>or</strong>e public health function andit is essential to effectively monit<strong>or</strong> the health of a community.Over the last 60 years, the science of surveillance has beenrefined and is the c<strong>or</strong>nerstone on which we base every publichealth intervention. As public health practice is largely perf<strong>or</strong>medat the state and local level, so it is f<strong>or</strong> surveillance.The U.S. Constitution leaves this responsibility up to states intheir police powers. The maj<strong>or</strong> role of the federal government,largely through CDC, lies in co<strong>or</strong>dinating and standardizingsurveillance across jurisdictions to ensure rep<strong>or</strong>ts can be comparedand to provide a national profile.After the 9/11 and anthrax attacks, gaps in surveillance systemsbecame apparent: most notably there was no f<strong>or</strong>mal p<strong>or</strong>talinto the hospitals (anthrax disease was best tracked in emergencydepartments). This was just a decade ago, yet, basically,our surveillance system was a handful of epidemiologists onthe phone calling hospitals to obtain inf<strong>or</strong>mation and ask if theyhad seen patients with particular symptoms. Out of this experience,public health and the hospitals recognized that they hadto build a m<strong>or</strong>e robust and real time system — which is whatN<strong>or</strong>th Carolina has now.Implementation of Surveillance: InfluenzaDuring 2009 pandemic influenza A (H1N1), surveillance wasessential f<strong>or</strong> understanding the activity and severity of the pandemic.To monit<strong>or</strong> seasonal flu and potential flu pandemics,public health departments rely on non-specific case definitionsbecause of the common nature of flu.With pandemic H1N1, public health had to quickly understandthe activity of the strain, in particular the prop<strong>or</strong>tion of thepopulation that would be affected and the subsequent severitymeasured by hospitalizations and m<strong>or</strong>tality. In the early days ofthe pandemic, states needed to understand rapidly what wasgoing on since there was no available vaccine. Antiviral stockpilesneeded to be deployed to providers in a way that madesense based on the surveillance. Community isolation andquarantine decisions relied on timely and accurate estimates ofdisease activity and severity.Because pandemic H1N1 had its <strong>or</strong>igins in N<strong>or</strong>th America,international p<strong>or</strong>t plans were already out of play: the firststep in disease prevention is to keep it off sh<strong>or</strong>e as long aspossible. Instead, public health had to shift and rely on rapidassessments of community disease, which was based onexisting biosurveillance systems.At the local and state level, surveillance begins with clinicianand lab rep<strong>or</strong>ting. Public health relies heavily on the medicalcare system to be the “boots on the ground” f<strong>or</strong> initiatingrep<strong>or</strong>ts and intelligence. N<strong>or</strong>th Carolina has two systems f<strong>or</strong>influenza rep<strong>or</strong>ting.The first is the CDC’s sentinel provider netw<strong>or</strong>k which includesvolunteer clinics/private care providers that file rep<strong>or</strong>tsto CDC on a weekly basis. Our State Lab<strong>or</strong>at<strong>or</strong>y of PublicHealth uses the sentinel sites (we have 70 in N<strong>or</strong>th Carolinaserving our population of 9.5 million people) to requestthat approximately one of every ten patients presenting withinfluenza-like illness (fever and respirat<strong>or</strong>y symptoms) submita nasal swab f<strong>or</strong> inoculation. The samples are then transp<strong>or</strong>tedto the state lab f<strong>or</strong> isolation and characterization of flu viruses.The second system is a syndromic surveillance system operatedthrough the emergency departments across the state.The emergency departments gather data elements f<strong>or</strong> everyhospital emergency department visit and state law mandatesrep<strong>or</strong>ting all visits electronically. To my knowledge, we are theonly state that has mandated emergency department rep<strong>or</strong>ting.F<strong>or</strong> every visit, we collect 18 data elements and use naturallanguage alg<strong>or</strong>ithms from the chief complaint and nurses notesto categ<strong>or</strong>ize a human illness into various syndromes. F<strong>or</strong> flu,the surveillance system looks f<strong>or</strong> temperature (if it is greaterthan 100.5 degrees) and respirat<strong>or</strong>y symptoms.This syndromic surveillance system is much timelier because itis rep<strong>or</strong>ted to the state every 12 hours via an automated transferto our analytical partner, the University of N<strong>or</strong>th CarolinaSchool of Medicine. They then analyze the data and provideaggregated summaries to state public health officials and to theCDC’s BioSense system.Consequently, we rely on our two parallel systems to trackand understand the development of pandemics and other seriouspublic health threats.65
EXPERT COMMENTARY continuedSurveillance: Essential f<strong>or</strong> Public Health Preparedness and ResponseN<strong>or</strong>th Carolina also has a third system that focuses on m<strong>or</strong>bidityand m<strong>or</strong>tality of unusual events. This system revolvesaround public health epidemiologists which are stationed in 10of the largest hospital systems in the state. The epidemiologistsrep<strong>or</strong>t on patients admitted to the hospital with suspectedrep<strong>or</strong>table community acquired infections. While the othersystems are centered m<strong>or</strong>e on population dynamics, this lastsurveillance system would be the most imp<strong>or</strong>tant one early onin the event of an anthrax attack <strong>or</strong> other bioterr<strong>or</strong> event.The hospital emergency department syndromic surveillancesystem and hospital-based epidemiologist positions were madepossible by the CDC’s emergency preparedness funding to thestates after 9/11 and the anthrax attacks. Unf<strong>or</strong>tunately, thesefunds have been dwindling f<strong>or</strong> the past two years and we havelost some hospital positions.The Ideal Surveillance SystemEnhanced electronic health rec<strong>or</strong>ds (EHRs) and rep<strong>or</strong>ting has thepotential to be, at least on the data collection side, completelyautomated from the second a patient has an encounter with thehealth system. Ideally, if a person presents with an illness and goesto a “doc in a box”, emergency department <strong>or</strong> any other provider,all symptoms and inf<strong>or</strong>mation are entered into the EHR and keydata elements are automatically rep<strong>or</strong>ted to a reposit<strong>or</strong>y wherethey are analyzed and translated into actionable inf<strong>or</strong>mation.The steps would be synchronous and automated: a patient hasthe clinical encounter, then a specimen is obtained, then the labisolates an <strong>or</strong>ganism on the specimen and health data and rep<strong>or</strong>tsare sent to the relevant parts of the public health system.The lab rep<strong>or</strong>ting is actually the easiest to automate first and weare beginning to do this. In N<strong>or</strong>th Carolina, we have implementedthe CDC’s National Electronic Disease Surveillance System(NEDSS) that can capture lab rep<strong>or</strong>ts through a health inf<strong>or</strong>mationexchange interface. F<strong>or</strong> example, a patient has diarrhea: a specimenis transferred to lab, toxin-producing E. coli is identified andthe inf<strong>or</strong>mation is electronically transferred to the local and statehealth department. The local health department contacts thepatient and begins an investigation as to where the E. coli camefrom. Electronic lab rep<strong>or</strong>ting is beginning to w<strong>or</strong>k; the problem isevery lab needs its own interface to NEDSS, and this is costly.Barriers to Building the FutureSurveillance SystemsA completely seamless, ideal surveillance system faces severalbarriers at the moment.The barrier to building the electronic lab rep<strong>or</strong>ting mentionedabove is finding the money to create the interfaces: each labwould need to communicate via standard messaging to NEDSSand this function can cost up to $50,000 per lab.When it comes to fully optimizing EHRs, a larger barrier isgoing to be confidentiality and permissions f<strong>or</strong> health inf<strong>or</strong>mationexchanges and proper governance of the exchanges. Whilein public health we have certain exemptions (HIPAA exemptionsf<strong>or</strong> rep<strong>or</strong>table diseases and conditions within state laws,f<strong>or</strong> example), public health and state law has to s<strong>or</strong>t what fallsunder these exemptions and then how the inf<strong>or</strong>mation can betransferred securely.Lastly, sustainability is a huge piece. Currently, we are buildingsystems largely on federal dollars via health inf<strong>or</strong>mationtechnology grants and others. However, there is a big questionof where sustained funding will come from. Ultimately is thisgoing to be funded by the health care financing system? Or willit be the duty of government to pay f<strong>or</strong>? This remains an unansweredissue because we do know that funding f<strong>or</strong> health carefinancing is getting less and less and state governments don’thave money to invest in these systems.The Future of SurveillanceWe are now on the cusp of modernization of our state andfederal public health surveillance system. That said, the systemwill always rely on the standardization and epidemiologic sciencethat was established and promulgated over the last 60years by the CDC and state and local public health departments.Regardless of the technological advancements, accurateand timely surveillance will always need the human element todetermine national case definitions f<strong>or</strong> rep<strong>or</strong>ting, data collectiontools, analysis and communication of actionable inf<strong>or</strong>mationto the agencies and people that need to know.There are two possible, realistic scenarios f<strong>or</strong> the developmentof automated surveillance systems:Surveillance systems will be built steadily and slowly one brickat a time, i.e., one hospital system will agree to submit EHR labrep<strong>or</strong>ts and pay f<strong>or</strong> it and set up the interface, then others willfollow as they see fit. This is, mostly, what is happening now.Occasionally we will find federal dollars to assist, but mostlymodernization is b<strong>or</strong>n from public-private partnerships withprivate entities taking on a large burden. Here, modernizationof surveillance will be an iterative accomplishment. This is slowand not strategic, because progress will involve whether it isfinancially advantageous f<strong>or</strong> a system to come on board. Thisis, likely, the best case scenario.The w<strong>or</strong>st case scenario would be a h<strong>or</strong>rible event that is exacerbatedby weaknesses in the system. The public and policymakerswill be appalled and there will finally be the political will to dosomething and modernize the surveillance systems. That eventwill likely be an act of bioterr<strong>or</strong>ism — the biggest and most plausiblefear that everyone is concerned about in public health.66
Hist<strong>or</strong>y of Biosurveillance in the United StatesA modern biosurveillance system would allow public healthdepartments to quickly detect a catastrophic biological eventand then rapidly share pertinent and accurate inf<strong>or</strong>mationacross jurisdictions, counties and states.How Federal Policies and Biosurveillance havedeveloped over time:n July 2002: Public Health Security and Bioterr<strong>or</strong>ism Preparednessand Response Act of 2002 requires the establishmentof a system of public health alerts and surveillance.n January 2004: Homeland Security Presidential Directive-9(HSPD): Defense of United States Agriculture and Fooddirects several federal agencies to create surveillancesystems co<strong>or</strong>dinated across agencies f<strong>or</strong> animals, plants,wildlife, food, human health and water.n April 2004: HSPD-10: Biodefense f<strong>or</strong> the 21st Century beginsthe process of developing a system capable of quicklyrecognizing and analyzing potential biological attacks.n December 2006: Pandemic and All-Hazards PreparednessAct of 2006 calls f<strong>or</strong> the creation of a nationwide, interconnected,electronic surveillance system.n August 2007: Implementing Recommendations of the 9/11Commission Act of 2007 requires the creation of the NationalBiosurveillance Integration Center.n October 2007: HSPD-21: Public Health and Medical Preparednesscalls f<strong>or</strong> establishing an operational national epidemiologicsurveillance system f<strong>or</strong> human health, with international connectivitywhere appropriate and created the National BiosurveillanceAdvis<strong>or</strong>y Subcommittee (NBAS) and requires theUnited States to develop biosurveillance capabilities across thecountry that can link with international systems.Homeland Security Presidential Directive-21 (HSPD-21) waslargely focused on surveillance. Dr. Engel was co-chair of the NationalBiosurveillance Advis<strong>or</strong>y Subcommittee to the Advis<strong>or</strong>y Committeeto the Direct<strong>or</strong> of CDC sanctioned under HSPD-21.The directive, which began under President Bush, was extendedby President Obama to allow the committee to publish thesecond rep<strong>or</strong>t in April 2011 (www.cdc.gov/osels/pdf/NBAS_Final_Rep<strong>or</strong>t_2011.pdf).The rep<strong>or</strong>t identified four maj<strong>or</strong> areas f<strong>or</strong> recommendation f<strong>or</strong> improvementf<strong>or</strong> national biosurveillance:1. Governance: co<strong>or</strong>dinate under the Executive Office of the Presidentthe federal agencies that oversee biosurveillance, includingCDC, Homeland Security, Department of Defense, USDA and othersthat have a hand in surveillance.2. Inf<strong>or</strong>mation exchange: methods used in acquiring biosurveillancedata are highly variable; efficient and comprehensive aggregationof these data must occur among the human health, animal, food,vect<strong>or</strong> and environmental sect<strong>or</strong>s.3. W<strong>or</strong>kf<strong>or</strong>ce development: need m<strong>or</strong>e skilled w<strong>or</strong>kers, particularlyin the area of public health inf<strong>or</strong>matics and social and behavi<strong>or</strong>alepidemiology (community resiliency).4. Research and development: the federal government needs toinvest in new areas including inf<strong>or</strong>mation technology, molecular andcellular sciences and communication.“Biosurveillance in the context of human health is a new term f<strong>or</strong> the science and practice of managing health-related data andinf<strong>or</strong>mation f<strong>or</strong> early warning of threats and hazards, early detection of events, and rapid characterization of the event so that effectiveactions can be taken to mitigate adverse health effects. It represents a new health inf<strong>or</strong>mation paradigm that seeks to integrate andefficiently manage health-related data and inf<strong>or</strong>mation across a range of inf<strong>or</strong>mation systems toward timely and accurate populationhealth situation awareness.” 245 — National Biosurveillance Strategy f<strong>or</strong> Human Health“Biosurveillance is the process of active data-gathering with appropriate analysis and interpretation of biosphere data that might relate to disease activityand threats to human <strong>or</strong> animal health — whether infectious, toxic, metabolic, <strong>or</strong> otherwise, and regardless of intentional <strong>or</strong> natural <strong>or</strong>igin — in<strong>or</strong>der to achieve early warning of health threats, early detection of health events, and overall situational awareness of disease activity.” 246 – HSPD-21BioSense 2.0BioSense 2.0, launched in November 2011, is the first HHSprogram to move to a distributed computing platf<strong>or</strong>m (Internetcloud) which allows f<strong>or</strong> rapid sharing of data across jurisdictionsand with CDC. It is also designed to supp<strong>or</strong>t enhancedinterchange of critical public health inf<strong>or</strong>mation necessary f<strong>or</strong>accurate early notification of outbreaks, pandemics, and terr<strong>or</strong>istevents. By integrating local and state-level inf<strong>or</strong>mation, it isexpected that BioSense will be able to provide a m<strong>or</strong>e timelyand cohesive picture at regional and national levels by:n Having a health monit<strong>or</strong>ing infrastructure and w<strong>or</strong>kf<strong>or</strong>ce capacitywhere needed at the state, local, tribal, and territ<strong>or</strong>ial(SLTT) levels;n Having a user-centered approach to increase local andstate jurisdictions’ participation in BioSense;n Supp<strong>or</strong>ting Meaningful Use adoption at the SLTT levels; andn Supp<strong>or</strong>ting state and local capability to conduct syndromicsurveillance is key in helping to implement Meaningful Use.67
C. Improving Medical Countermeasure Research,Development and ManufacturingAnthrax vaccine, botulinim antitoxin and smallpoxvaccine all have something in common: thegovernment is the only real customer f<strong>or</strong> theseproducts. As a result of the lack of a naturalmarketplace, the U.S. government has investedin the research, development and stockpilingof emergency MCM f<strong>or</strong> a pandemic, bioterr<strong>or</strong>attack <strong>or</strong> emerging infectious disease outbreak.Development of medical products f<strong>or</strong> the nation’sbiodefense is a key piece of any publichealth emergency response. By preparing f<strong>or</strong>a bioterr<strong>or</strong> attack with adequate supplies ofcountermeasures, the nation can effectivelyneutralize that threat. A successful domesticMCM enterprise will prepare the nation f<strong>or</strong>new threats, expected <strong>or</strong> unexpected, by buildingthe science, policy and production capacityin advance of an outbreak.Congress created Project BioShield in 2003 tospur development and procurement of MCM andauth<strong>or</strong>ized the Biomedical Advanced Researchand Development Auth<strong>or</strong>ity (BARDA) in 2006to supp<strong>or</strong>t the development of domestic manufacturingcapacity. However, industry was still reluctantto invest in vaccine and countermeasuredevelopment in large part due to limited profitincentives and slow bureaucratic processes.In August 2010, the Secretary of HHS releasedThe Public Health Emergency Medical CountermeasuresEnterprise Review, which laid out strategiesf<strong>or</strong> addressing chokepoints in research andadvanced development, improvements in domesticmanufacturing capacity and enhancing public-privatepartnerships. 247 The review concludedthat new strategies were needed to creative incentivesf<strong>or</strong> private industry while protecting thepublic’s interest and safety, including:n Enhancing regulat<strong>or</strong>y innovation, scienceand capacity;n Improving domestic manufacturing capacity;n Providing c<strong>or</strong>e advanced development and manufacturingservices to development partners;n Creating novel ways f<strong>or</strong> the enterprise to w<strong>or</strong>kwith partners;n Developing financial incentives;n Addressing roadblocks from concept developmentto advanced development; andn Improving management and administrationwithin the enterprise.Since release of the Review, the national countermeasureenterprise has made progress insome notable ways:n BARDA has issued a request f<strong>or</strong> proposals f<strong>or</strong>Centers f<strong>or</strong> Innovation in Advanced Developmentand Manufacturing (CIADM), a strategyfrom the Review which would create flexiblefacilities to produce MCM on a routine basisf<strong>or</strong> CBRN threats as well as a manufacturingprocess f<strong>or</strong> emergency <strong>or</strong> pandemic conditions.248 The proposals are currently beingreviewed, with awards expected in FY2012.HHS is using $478 million in unspent H1N1funds f<strong>or</strong> these facilities.n FDA launched the Medical CountermeasuresInitiative (MCMi) to establish regulat<strong>or</strong>ypathways to accelerate MCM development,including modernizing the review processand updating the legal and policy framew<strong>or</strong>kf<strong>or</strong> regulating these products. 249 FDA has allocated$170 million from H1N1 emergencyfunds f<strong>or</strong> this initiative.n The National Institute f<strong>or</strong> Allergy and InfectiousDiseases (NIAID) has introducedthe Concept Acceleration Program, whichenables co<strong>or</strong>dination of teams of scientific,medical and product development expertsto guide MCM researchers with the goal ofnurturing promising concepts that mightotherwise not be pursued. 250 NIH has begunstaffing the program. 251n ASPR has convened interagency co<strong>or</strong>dination,including an Enterprise Seni<strong>or</strong> Council,which meets regularly to discuss lifecyclemanagement of biodefense products. Participantsinclude representatives from ASPR,CDC, FDA, NIAID, DHS, Veterans Affairs(VA), USDA and DOD.n BARDA has issued significant new contracts,including f<strong>or</strong> recombinant vaccine technology,which could significantly sh<strong>or</strong>ten theproduction timeline f<strong>or</strong> seasonal and pandemicflu vaccine; 252 and new contracts underthe Broad Spectrum Antimicrobial Program,including what would be the first new classof antibacterial agents to treat Gram-negativeinfections in 30 years. 253n HHS has begun to develop a five-year budgetplanning process to help project fundingneeds f<strong>or</strong> development and stockpilingthroughout the countermeasure lifecycle. 25468
The national countermeasure enterprise stillfaces challenges in fully implementing the strategieslaid out in the Review, including:n BARDA has requested congressional auth<strong>or</strong>izationas well as $100 million to launch a MCMStrategic Invest<strong>or</strong>, which would be an independent501(c)(3) venture capital firm thatwould provide both investment and businessmanagement to biotechnology companies tobring commercially-viable platf<strong>or</strong>ms to fruition.Although the Strategic Invest<strong>or</strong> wouldbe independent, BARDA would house an InterfaceCenter to communicate with the firm.n Funding f<strong>or</strong> research and development is stillfar below recommended levels. 255 The Presidentrequested $655 million f<strong>or</strong> BARDA f<strong>or</strong>FY2012, in addition to funding f<strong>or</strong> the StrategicInvest<strong>or</strong>, but Senate appropriat<strong>or</strong>s (the onlyCommittee that had passed an HHS appropriationsbill as of publication of this rep<strong>or</strong>t) onlyapproved $415 million. The Committee’s rep<strong>or</strong>tobjected to HHS’ request that this fundingcome from BioShield’s Special Reserve Fund. 256n After its initial investment, future funding f<strong>or</strong>FDA’s MCM Initiative is uncertain, and proposedcuts to that agency could significantlyhamper the program’s potential.n Cuts to the public health w<strong>or</strong>kf<strong>or</strong>ce could hinderthe success of any dispensing plans. ASPRhas begun outreach to the public health communityto discuss these plans, but these conversationsneed to be m<strong>or</strong>e extensive and takeinto account drastic w<strong>or</strong>kf<strong>or</strong>ce reductions.n The Bipartisan WMD Terr<strong>or</strong>ism ResearchCenter recently issued a “D” grade f<strong>or</strong> the nation’sMCM development and approval process,based on failure to meet criteria suchas clearly defined requirements, a commonset of pri<strong>or</strong>itized research and developmentgoals, co<strong>or</strong>dinated budget requests and sufficient,sustained funding. 257 69RECOMMENDATIONSTFAH recommends that the United States mustplace a higher pri<strong>or</strong>ity on research and developmentof MCM, including vaccines, medicines andtechnology. Policymakers must ensure that thepublic health system is involved in this process,from initial investment through distribution anddispensing. The nation’s MCM enterprise couldbe advanced through the following activities:n Auth<strong>or</strong>izing the President’s requests f<strong>or</strong> MCMadvancement: building an MCM Strategic Invest<strong>or</strong>to leverage capital f<strong>or</strong> new technologies; anddeveloping end-to-end leadership to overseeproducts from initial research to dispensing;n Improving oversight and management ofnational stockpiles through ongoing replacementof expiring products and expansion ofthe Shelf-Life Extension Program (SLEP) tostate stockpiles to maintain supplies in a costeffectivemanner;n Building increased flexibility f<strong>or</strong> FDA to issueEmergency Use Auth<strong>or</strong>ity of medical productsnecessary to respond to an emergency; andn Increased focus on special pediatric needs,including in the development, testing anddosages of MCMs.In September 2010, BARDA awarded contracts,w<strong>or</strong>th up to $100 million over three years, toeight biotech and pharmaceutical companiesresearching a range of innovative countermeasures.One company, Pfenex, is w<strong>or</strong>king todevelop a faster way to make anthrax vaccine;others, including Novartis and Rapid Micro Biosystems,are looking into methods to speed upflu vaccine manufacturing. 258Examples of BARDA ActivitiesIn September 2011, BARDA awarded $153 millionto Cellerant Therapeutics, a biotech firmw<strong>or</strong>king on a new drug that may protect humansfrom nuclear radiation and awarded up to $94 millionto GlaxoSmithKlein f<strong>or</strong> a dual-purpose broadspectrum antibiotic with potential to treat illnessescaused by bioterr<strong>or</strong>ism threats such as plague andtularemia, as well as certain life-threatening infections,known as Gram-negative infections, associatedwith prolonged259, 260hospitalization.
Innovations f<strong>or</strong> FDA and Medical CountermeasuresFDA is responsible f<strong>or</strong> getting lifesaving drugsand devices to market as quickly as possiblewhile ensuring safety. The spectrum of the medicalcountermeasure (MCM) enterprise includesvaccines, antiviral and other lifesaving drugs anddevices such as diagnostics that are used to determineif someone has been exposed to a biologic,chemical, nuclear <strong>or</strong> radiologic threat.MCMs pose unique challenges, since it is often impossible<strong>or</strong> unethical to safely test these products onhumans. F<strong>or</strong> instance, while it is possible to test aproduct f<strong>or</strong> safety in humans, it is not feasible to exposepeople to the threat itself to test whether thevaccine <strong>or</strong> the treatment w<strong>or</strong>ks. It is essential thatnew vaccines, antiviral medications and devices intendedto save lives do not cause unintentional harmand endanger the health of Americans — but it isalso essential to have effective countermeasures inplace to respond to man-made and natural threats.FDA must take steps to minimize red tape, maximizeinnovation and maintain safety when it comesto reviews and standards f<strong>or</strong> medical countermeasures.Additional co<strong>or</strong>dination with BARDA andprivate industry is essential to understand pri<strong>or</strong>itiesand to find ways to improve processes to makethem less burdensome on companies.The agency is developing new scientific andanalytic tools to speed the approval of lifesavingdrugs and devices. Innovative approaches can beused to m<strong>or</strong>e efficiently manage the movementof potential treatments from idea to reality.In August 2010, the agency launched a newMedical Countermeasures Initiative (MCMi),which was first limited to preparing f<strong>or</strong> respondingto a flu pandemic. 261 In April 2011, Congressenacted legislation to allow the project to alsoaddress chemical, biological, radiological andnuclear (CBRN) threats. 262Examples of the eff<strong>or</strong>ts FDA is taking to expandand be m<strong>or</strong>e flexible in testing and review ofproducts include:n Developing genetically modified animals f<strong>or</strong> testing,such as an engineered modified mouse to testthe smallpox vaccine and potential side effects;n Expanding testing on cell cultures created inlabs combined with m<strong>or</strong>e research into howhumans are likely to react differently than testanimals conducted lab-created materials <strong>or</strong>rodents;n Implementing supercomputing and IT enhancementsto better simulate the effect ofMCMs on humans;n Creating research models, such as biomimetrics,which create artificial models natural biology;n Researching adjuvants to maximize theamount of vaccine available during crises;n Advancing treatment f<strong>or</strong> acute radiationsyndrome;n Enhancing the ability to test f<strong>or</strong> multiplepathogens simultaneously;n Improving the ability to rapidly and accuratelytest f<strong>or</strong> new potential threats; andn Focusing significant research on the impact ofMCMs on children and other at risk patients.Examples of FDA eff<strong>or</strong>ts to expand and be m<strong>or</strong>eflexible to ensure life-saving drugs and devicesare sped to market and available f<strong>or</strong> use in crisesinclude:n Enhancing clarity and flexibility f<strong>or</strong> emergency useauth<strong>or</strong>ization (EUA), which permits FDA to approvethe emergency use of drugs, devices, andmedical products (including diagnostics) that werenot previously approved, cleared, <strong>or</strong> licensed bythe agency <strong>or</strong> the off-label use of approved productsin certain well-defined emergency situations;n Issuing an EUA so doxycycline can be used asa prophylaxis f<strong>or</strong> people exposed to anthrax;n Expanding the shelf-life extension program touse drug stockpiles beyond f<strong>or</strong>mal expirationdates when safe;n Improving risk-benefit analyses; andn Developing models f<strong>or</strong> predicting and mitigatingthe potential f<strong>or</strong> sh<strong>or</strong>tages of MCM drugs,biologics and devices during emergencies.“The mission of the FDA should continue to ensure that new devices and drugs reaching the publicin the U.S. are safe and effective. We encourage fostering innovation, without lowering evidencestandards <strong>or</strong> putting the public at risk.” 263—Testimony from America’s Health Insurance Plans (AHIP) to the House Oversight andGovernment Ref<strong>or</strong>m Committee in June 201170
D. Enhancing Surge CapacityThe ability of our health care system to quicklyprovide care f<strong>or</strong> an influx of patients during anemergency is critical.During a severe health emergency, the health caresystem would be stretched beyond n<strong>or</strong>mal limits.Patients would quickly fill emergency rooms anddoct<strong>or</strong>s’ offices, exceed the existing number ofavailable hospital beds, and cause a surge in demandf<strong>or</strong> critical medicines and equipment.The challenge of how to equip hospitals and trainhealth care staff to handle the large influx of criticallyinjured <strong>or</strong> ill patients who show up f<strong>or</strong> treatmentafter <strong>or</strong> during a public health emergencyremains the single, most challenging issue f<strong>or</strong>public health and medical preparedness. 264In public health emergencies, such as a new diseaseoutbreak, a bioterr<strong>or</strong> attack, <strong>or</strong> catastrophicnatural disaster, U.S. hospitals and health carefacilities are on the front lines providing triageand medical treatment to individuals. In thebest of times, however, most emergency roomsand intensive care units (ICUs) must confrontbed sh<strong>or</strong>tages and staffing issues; in a mass casualtyevent — particularly a pandemic influenza<strong>or</strong> mass bioterr<strong>or</strong> attack — the situation couldquickly spiral out of control.RECOMMENDATIONSTFAH recommends:n Enhancing the Hospital Preparedness Program(HPP) to create coalitions among hospitalsto share surge burdens within a region withemphasis on developing creative strategies, intensivetraining and providing additional funding,particularly in large urban centers;n Clarifying crisis standards of care via creation ofa national framew<strong>or</strong>k to guide states and localentities in the event of a mass casualty <strong>or</strong> crisis;n Eliminating the need f<strong>or</strong> dual declarations tobe made by the President and U.S. Secretaryof HHS to implement Section 1135 waivers toallow rapid availability of healthcare servicesf<strong>or</strong> individuals affected by a disaster; andn Clarifying federal laws to implement a broadliability protection that applies to all volunteerhealth professionals during a nationallydeclaredpublic health emergency, creating aFederal T<strong>or</strong>t Claims Act protection f<strong>or</strong> MedicalReserve C<strong>or</strong>ps volunteers year-round, as thesepersonnel participate in public health drills andtraining during times of non-disaster, and mechanismsf<strong>or</strong> ensuring hospital and provider costsincurred during disaster response are covered.71
E. Improving Community Resilience: HelpingCommunities Cope and RecoverEnsuring communities can cope with and recoverfrom emergencies is a significant challengeto public health preparedness.The most vulnerable members of a community,such as children, the elderly, people with underlyinghealth conditions and racial and ethnicmin<strong>or</strong>ities, face special challenges that must beplanned f<strong>or</strong> pri<strong>or</strong> to emergencies happening.Building community resilience is one of thetwo overarching goals identified by HHS in therelease of the draft Biennial ImplementationPlan f<strong>or</strong> the National Health Security Strategy.It calls f<strong>or</strong> fostering inf<strong>or</strong>med, empowered individualsand communities.Improving relationships with the communityand the health of the community are bothstrongly tied to resiliency. The aftermath ofHurricane Katrina provides a strong reminderof the imp<strong>or</strong>tance of engaging all membersof a community to be prepared f<strong>or</strong> emergencies.F<strong>or</strong> instance, acc<strong>or</strong>ding to one study inthe Annals of Emergency Medicine, 55.6 percentof individuals displaced in the aftermath ofHurricane Katrina had a chronic disease, suchas hypertension, hypercholesterolemia, diabetes<strong>or</strong> pulmonary disease, which compoundedthe challenges of evacuation and supp<strong>or</strong>t.265Similarly, during Hurricanes Gustav and Ike, 40percent of evacuees were obese and many wereunable to stay in local shelters because they werem<strong>or</strong>bidly obese <strong>or</strong> on oxygen. 266 Currently, twothirdsof Americans are overweight <strong>or</strong> obese.Experts recommend that improving resiliency, particularlyamong vulnerable populations, requires:n Improving the overall health status of communities,so they are in better condition toweather and respond to emergencies, such asthrough initiatives and programs supp<strong>or</strong>tedby the Public Health and Prevention Fund’sCommunity Transf<strong>or</strong>mation Grants (CTGs);n Providing clear, honest, straightf<strong>or</strong>ward guidanceto the public;n Health officials developing ongoing relationshipswith members of the community, so,when emergencies arise, they are trusted andunderstood; andn Engaging members of the community directlyin emergency planning eff<strong>or</strong>ts.To reach diverse communities, experts als<strong>or</strong>ecommend inf<strong>or</strong>mation must be provided inchannels beyond the Internet, such as radio andracial and ethnic publications and television, andin languages other than English. In addition,idiomatic translations are imp<strong>or</strong>tant to reachspecific cultural perspectives effectively, andmessages should be delivered by trusted sources,such as religious and community leaders.RECOMMENDATIONSTFAH recommends leveraging new opp<strong>or</strong>tunitiescreated by the Aff<strong>or</strong>dable Care Act (ACA),which includes several provisions to improveoverall health of communities that supp<strong>or</strong>t communityresiliency, including:n The Prevention and Public Health Fund providesa $16.5 billion investment over the next10 years f<strong>or</strong> communities around the countryto use f<strong>or</strong> proven, effective ways to keepAmericans healthier and m<strong>or</strong>e productive;n A National Prevention Strategy which aims toimprove health and reduce disease rates by ensuringhealth departments w<strong>or</strong>k with other sect<strong>or</strong>s,such as housing, transp<strong>or</strong>tation, educationand businesses, to ensure healthy choices arem<strong>or</strong>e widely available and accessible to Americansin their daily lives and during emergencies;n As part of the Prevention Fund, CommunityTransf<strong>or</strong>mation Grants (CTGs), in particular,supp<strong>or</strong>t building community coalitions to addressobesity, tobacco and other public healthproblems, which also help f<strong>or</strong>ge ongoing relationshipsbetween the community and publichealth professionals, particularly with underservedcommunities. Outreach to individualswith underlying health conditions serves a dualpurpose, since they are often particularly vulnerableduring emergencies, and people dependenton prescription drugs medical treatments encounterunique challenges during emergencies.72
Prevention, Preparedness, the Armed F<strong>or</strong>ces andTotal F<strong>or</strong>ce Fitness“Total F<strong>or</strong>ce Fitness is m<strong>or</strong>e than a physical fitness. It is the sum total of the many facets of individuals,their families, and the <strong>or</strong>ganizations to which they serve. It is not something someone achieves twicea year f<strong>or</strong> a test. It is a state of being.” 267— ADM Michael Mullen, (f<strong>or</strong>mer) Chairman of the Joint Chiefs of StaffIn 2009, the Chairman of the Joint Chiefs ofStaff (JCS), ADM Michael Mullen asked the Cons<strong>or</strong>tiumf<strong>or</strong> Human and Military Perf<strong>or</strong>mance(CHAMP) to develop what has become knownas Total F<strong>or</strong>ce Fitness (TFF) to ensure servicemembers and their families are prepared f<strong>or</strong> therig<strong>or</strong>s of war and a constant state of readiness.Lessons learned from the Total F<strong>or</strong>ce Fitnessinitiative can be used to help inf<strong>or</strong>m engagementand resiliency planning f<strong>or</strong> communities aroundthe country.During wartime, service members are trained andf<strong>or</strong>ced to adapt to chaotic and life-threatening situations.When they return home, service membersmust maintain a state of preparedness while, at thesame time, living acc<strong>or</strong>ding to the n<strong>or</strong>ms of a civilsociety. Consequently, the fitness of service membersis not merely physical, it has to be holistic.Per the Chairman’s directive, CHAMP co<strong>or</strong>dinatedwith the Samueli Institute, the Institute of AlternativeFutures and members of the JCS to create anew fitness doctrine that took a holistic approach tomilitary preparedness and the fitness and resiliencyof service members. The project sought to expandthe definition of health promotion and preventionand create a different model from the typical medicalapproach, i.e. one that is m<strong>or</strong>e comprehensive.The group w<strong>or</strong>ked with over 70 scientists, health,social, community and spiritual leaders to define,evaluate and measure everything involved in keepingservice members fit, resilient and prepared.Ultimately, the group created a framew<strong>or</strong>k focusedon the mind, body and the communitiesand environments supp<strong>or</strong>ting a service member.The final structure depicts the service membersurrounded by family, community and environmentas these impact health and resiliency. Inaddition, the framew<strong>or</strong>k found eight domains ofTotal F<strong>or</strong>ce Fitness: 1) Physical, 2) Nutritional,3) Medical, 4) Environmental, 5) Behavi<strong>or</strong>al, 6)Psychological, 7) Spiritual and 8) Social.As the military views it, total fitness is a statewhere mind and body are one: the perfect balancebetween readiness and well-being, whereeach condition supp<strong>or</strong>ts the other. A servicemember who achieves total fitness is healthy,ready and resilient. Under TFF, to supp<strong>or</strong>t servicemembers, the military takes the preventive stepsto ensure health across all fronts. F<strong>or</strong> example,diet and nutrition are just as imp<strong>or</strong>tant as mentalacuity and physical strength. To be completely fit,a service member must go beyond maintaining anideal body weight to instead combine diet, nutritionand physical and mental training.Consequently, TFF provides the foundationf<strong>or</strong> how any military fitness program could beevaluated and measured. The framew<strong>or</strong>k includesmetrics that could be used f<strong>or</strong> monit<strong>or</strong>ingprogram effectiveness and f<strong>or</strong> improving andcomparing programs that already exist. TFF hasbecome a new military doctrine that builds adialogue and strategy among everyone involvedwith health.73
EXPERT PerSPECTIVEVulnerability, Resilience and Mental HealthConsiderations in Disaster Planning and Response:Do Resources Match the Rhet<strong>or</strong>ic?By David Abramson, PhD, MPH and Irwin Redlener, MD, Columbia University Mailman School of Public HealthOver the past decade, policymakers, leading publichealth officials and scientists have acknowledged theimp<strong>or</strong>tance of addressing mental health issues in the wake ofa disaster, but the practice of disaster mental health has yet tomatch the rhet<strong>or</strong>ic. This rhet<strong>or</strong>ic, embodied in such recentpolicy documents as the President’s policy directive on nationalpreparedness (PPD-8, released March 30, 2011) 268 and theCDC’s Public Health Emergency Preparedness Capabilities(March 2011), 269 appropriately links mental health with disasterresilience. The capacity of individuals and communities towithstand, adapt <strong>or</strong> recover quickly from emergency eventsand disasters is clearly related to their mental welfare bothbef<strong>or</strong>e and after a disaster. And yet the practice of disastermental health is mired in old and generally untested thinking,still mainly focused on the identification and treatment of Post-Traumatic Stress Dis<strong>or</strong>der (PTSD), using practices that areonly minimally-related to an evidence base. M<strong>or</strong>eover, publichealth practice is often overseen by public health systems generallyill-equipped and under-funded to co<strong>or</strong>dinate <strong>or</strong> providecomplex mental and behavi<strong>or</strong>al health services.Mental health effectsDisasters and complex emergencies leave their mark on thoseexposed to them, although perhaps in ways contrary to popularbelief. Responders to a disaster can certainly suffer psychologicalconsequences, as can the populations affected by them.But in one recent comprehensive review of the disaster mentalhealth research, the auth<strong>or</strong>s pointed out that severe casesof PTSD, in which surviv<strong>or</strong>s “re-experience” the event, mayoccur at most in 30 percent <strong>or</strong> fewer of the exposed population,and that generally within one to two years people havereturned to a psychological “equilibrium”. 270 The bigger issuesnoted in this seminal review are those pre-disposing fact<strong>or</strong>s ofrisk and resilience which protect individuals and communities<strong>or</strong> make them m<strong>or</strong>e vulnerable.Nearly a decade ago, N<strong>or</strong>ris and colleagues reviewed the researchliterature regarding the individual-level risk fact<strong>or</strong>s complicitin po<strong>or</strong> mental health outcomes following a disaster. 271One very imp<strong>or</strong>tant finding was that the exposure to the devastatingeffects of a disaster were compounded by pre-disasterstress<strong>or</strong>s in people’s lives, such as living in blighted communitiesand dealing with the stresses of poverty. A household’s compositionmade a difference as well: regardless of income, womenwere m<strong>or</strong>e susceptible to po<strong>or</strong> mental health outcomes, particularlyif they were married and had children in the home.Furtherm<strong>or</strong>e, those individuals who had lost confidence in theirability to cope <strong>or</strong> control outcomes, <strong>or</strong> who had few social resources,were highly susceptible to mental health problems.Community-level fact<strong>or</strong>s make a difference in surviv<strong>or</strong>s’ mentalhealth as well. Disasters can sever social netw<strong>or</strong>ks, particularlywhen populations are evacuated <strong>or</strong> displaced. Disasters also underminethe capability of civic institutions to supp<strong>or</strong>t the physicaland social welfare of people in the community — hospitals andhealth systems, as well as social services and systems of justice.International disaster mental health providers have witnessed thistime and again. When the social supp<strong>or</strong>ts and institutions in acommunity unravel, the mental health of its residents plummets. 272Our own studies of the mental health of individuals affectedby the 2005 Hurricane Katrina and the 2010 Deepwater H<strong>or</strong>izonOil Spill have certainly reinf<strong>or</strong>ced these findings. OurGulf Coast Child & Family Health Study, which followed 1,079randomly sampled households in Louisiana and Mississippi f<strong>or</strong>five years after the hurricane, revealed the long tail of mentalhealth distress, and how much of it was due to neighb<strong>or</strong>hoodconditions, chronic uncertainty, and pre-disposing economicrisk fact<strong>or</strong>s. When we first interviewed parents in 2006, over60 percent were suffering mental health distress and disability.By the fourth time we spoke to them in 2010, things had improved— although 40 percent of them were still experiencinglingering mental health effects. And among their children, evenyears after the hurricane they were five times as likely as similar“non-exposed” children to be experiencing serious emotionaldisturbance. Over one in three children was still experiencingdepression, anxiety <strong>or</strong> behavi<strong>or</strong>al effects. 273 These mental healtheffects were far subtler than PTSD, since they reflected depression,anxiety, and complicated grief, and interfered with people’sability to recover and return to stable and productive lives.Sh<strong>or</strong>tly after the rupture of the Deepwater H<strong>or</strong>izon Macandowell in the Mississippi Gulf last year, we conducted town hallmeetings and focus groups in communities along the GulfCoast. Residents were clearly distressed by the environmentaldisaster, and even children expressed concerns f<strong>or</strong> theirfutures and f<strong>or</strong> their way of life. When we followed this witha random survey of 1,203 residents living within ten miles ofthe coast in Louisiana and Mississippi, we found that slightly74
less than 20 percent of parents rep<strong>or</strong>ted that their childrenhad emotional <strong>or</strong> behavi<strong>or</strong>al problems since the Oil Spill, andamong those families who thought they might have to moveas a result of the oil spill, over a third rep<strong>or</strong>ted mental healthproblems among their children. 274These studies, and many others, serve to illustrate the complexityof the problem. Communities are m<strong>or</strong>e resilient to a disasterwhen they are psychologically stronger bef<strong>or</strong>e the event occurs,yet there is little political impetus to recognize this link. After theevent, mental health problems are not restricted to PTSD, canlast f<strong>or</strong> years after an event, and are often the consequence ofhousehold, neighb<strong>or</strong>hood, and larger political f<strong>or</strong>ces. The solutionhas to extend beyond “Psychological First Aid” (PFA), the“intervention du jour” in most disaster response circles.The disaster mental health practice environmentAlthough not the sole mental health intervention, PFA is oneof the federal government’s primary tools. Under provisionsof the Staff<strong>or</strong>d Act, FEMA employs the Crisis Counseling Assistanceand Training Program, in consultation with SAMHSA,to fund states and localities to deliver PFA, often through theuse of community health w<strong>or</strong>kers. As noted in a recent rep<strong>or</strong>tto the National Biodefense Science Board, the administrativerules and constraints imposed by this program are so restrictivethat some states have decided not to even apply f<strong>or</strong> thefunds after a disaster. 275 When deployed, these communityhealth w<strong>or</strong>kers serve a critical community outreach function,although once cases have been identified there are meager <strong>or</strong>no resources available f<strong>or</strong> addressing complex psychologicalproblems. The case-finding may be good, but the followthroughtreatment is often non-existent; furtherm<strong>or</strong>e, the Staff<strong>or</strong>dAct cannot adequately pay f<strong>or</strong> the treatment needed. 276Perhaps most imp<strong>or</strong>tantly, the “treatment” needs to be able toaddress the larger household and community fact<strong>or</strong>s that haveled to the mental health problems. This requires a systemsviewentirely absent from most recovery eff<strong>or</strong>ts — not becauseit’s not valued, but because it’s not funded.Organizationally, the responsibility f<strong>or</strong> disaster mental healtheff<strong>or</strong>ts falls within Emergency Supp<strong>or</strong>t Function 8, as articulatedin the National Response Framew<strong>or</strong>k, and is squarely withinthe public health domain, although crisis counseling is a taskdesignated to Emergency Supp<strong>or</strong>t Function 6 (Mass Care, ledby FEMA and the American Red Cross). Compounding theproblem is that local public health has little experience overseeing<strong>or</strong> assuring netw<strong>or</strong>ks of mental health services. Acc<strong>or</strong>dingto a 2010 profile of 2,033 local health departments conductedby the National Association of City and County Health Officials(NACCHO), over 84 percent of all health departments do notoffer mental health <strong>or</strong> behavi<strong>or</strong>al services, n<strong>or</strong> do they overseethem. 277 And, as noted in the rep<strong>or</strong>t to the National BiodefenseScience Board, “Responders often do not know what mentaland behavi<strong>or</strong>al health resources and interventions are available,useful, and effective, and do not have training in principles of disasterbehavi<strong>or</strong>al health” (p. 6). 278 The source of the problem,the auth<strong>or</strong>s conclude, is that, “Federal Agencies do not havea clear understanding of State and local capabilities in disastermental and behavi<strong>or</strong>al health response (p. 10).”The responsibility sits with public health, but it is essentially anunfunded mandate. As the country’s economic crisis deepens,public health and emergency preparedness have abs<strong>or</strong>beden<strong>or</strong>mous funding cuts. Over one year’s time, preparednessand response funding within DHHS and DHS dropped by nearly$900 million, from $5.3 billion in FY10 to $4.4 billion in FY11,a 17 percent overall reduction. Acc<strong>or</strong>ding to the NACCCHO2010 health department survey, the average local health departmentreceives $2 per capita within its catchment f<strong>or</strong> emergencypreparedness activities, and even that meager amount is beingeroded. With that money, smaller health departments fund a .5FTE to do their emergency preparedness, and the largest agenciesfund an average of 4 FTE. As often occurs in public health,its mandate increases even as its budget shrinks.ConclusionMany challenges remain with respect to meeting the complexmental health needs of individuals and communities exposedto disasters. Perhaps most challenging — and most demandingof resources — is the capacity to reduce vulnerability andincrease resilience pri<strong>or</strong> to a maj<strong>or</strong> catastrophic event. This, ofcourse, speaks to broader public policy issues such as povertyreduction, improved access to health care and early, effectiveintervention f<strong>or</strong> mental health concerns long bef<strong>or</strong>e the disasterexposure. In the current economic environment, wherepublic spending on discretionary programs is on a clearlydownward traject<strong>or</strong>y, the likelihood of substantive investmentsin these critical areas is virtually inconceivable.Where does this leave us?At the very least, we have to develop strategies that:• maximize existing resources;• reverse the cuts which have left the nation’s public healthw<strong>or</strong>kf<strong>or</strong>ce dangerously depleted and underfunded;• ensure that interventions deployed in post-disaster publichealth practice are based on data-driven, evidence-influencedrecommendations; and,• remove bureaucratic barriers which have been mem<strong>or</strong>ializedin existing regulations <strong>or</strong> legislation (a poignantexample being the service restrictions imposed by currentStaff<strong>or</strong>d Act provisions).Failure to provide pro-active improvements in U.S. capacityto prevent and intervene effectively with respect to themental health consequences of disasters will leave the nationincreasingly vulnerable to the catastrophic events which aresure to appear with regularity in the years to come.75
Public Communication and Social Media Usage during H1N1Reaching diverse communities during a publichealth emergency requires providing inf<strong>or</strong>mationto the public via multiple channels includingthe Internet, social media and traditional, racialand ethnic publications and broadcast outlets.Acc<strong>or</strong>ding to the Pew Internet & American LifeProject, 93 percent of 12-17 year-olds go onlineand 65 percent utilize a social netw<strong>or</strong>king platf<strong>or</strong>m;87 percent of 18-32 year-olds go onlineand 67 percent use social media. 279 Meanwhile,older generations prefer traditional media: 56percent of 64-72 year-olds are online and 31percent of those older than 73 go online. 280During the 2009 outbreak of H1N1, while traditionalmedia was utilized, social media playeda special role in the government’s response,especially because of that medium’s ability t<strong>or</strong>each younger populations. 281 CDC focused onsocial media to ensure messages about the outbreakreached younger populations which weremost at-risk during H1N1. 282 The agency alsocontinues to use Twitter and Facebook to communicateabout H1N1 and other public healthinf<strong>or</strong>mation programs, and their Facebook pagehas m<strong>or</strong>e than 20,000 “fans.” 283Going beyond communication and education,the National Institutes of Health (NIH) usedTwitter ® to monit<strong>or</strong> the spread of the H1N1outbreak. 284Increased outreach on social media and via theInternet may be necessary to reach a younger audienceduring a pandemic. In addition, traditionalmedia is imp<strong>or</strong>tant when trying to reach older andpo<strong>or</strong>er populations that typically do not engage incomparable rates of Internet communication.F. Co<strong>or</strong>dinating Overall Preparedness and FoodSafety Prevention: Strategic Implementation ofthe FDA Food Safety Modernization Act of 2011In addition to the reauth<strong>or</strong>ization of overallpublic health emergency preparedness, theFDA Food Safety Modernization Act was signedinto law in 2011. The law contained many provisionsto help re<strong>or</strong>ient the nation’s food safetysystem to prevent outbreaks instead of detectingproblems after they already occurred.TFAH recommends that sufficient resourcesand administration actions be taken to fullyimplement the law.TFAH asked Erik Olson, Direct<strong>or</strong> of Food Programsf<strong>or</strong> The Pew Charitable Trusts to providean overview of the opp<strong>or</strong>tunities and challengesf<strong>or</strong> implementing the new act.76
EXPERT perspectiveFood Safety: New Law Takes a Big Bite Out of theProblem, but Leaves Much on the Plate 285By Erik D. Olson, Direct<strong>or</strong> of Food Programs at The Pew Charitable TrustsThe Promise of the Food Safety Modernization ActThe FDA Food Safety Modernization Act (FSMA), a landmarklaw passed with broad bipartisan supp<strong>or</strong>t in December 2010and signed into law by President Obama on January 4, 2011,will help tackle foodb<strong>or</strong>ne illness by setting up a new, prevention-basedsafety system f<strong>or</strong> the 80 percent of our food supplythat is regulated by FDA. This was the first significant overhaulof FDA’s food safety auth<strong>or</strong>ities since the Great Depressionwhen President Franklin Roosevelt signed an update of the lawin 1938. Maj<strong>or</strong> advances anticipated under this imp<strong>or</strong>tant newlaw include new national standards f<strong>or</strong> the safety of produceand processed foods, stronger inspection requirements, stricterimp<strong>or</strong>ts controls, and m<strong>or</strong>e muscular FDA auth<strong>or</strong>ities to helpthe agency deter practices that can cause foodb<strong>or</strong>ne illnesses.However, as the late-summer 2011 outbreak of Listeria monocytogenesinfections from Col<strong>or</strong>ado cantaloupe that killed atleast 28 people (with a staggering fatality rate of over 20 percent)has reminded us, substantial challenges lie ahead. F<strong>or</strong> allof the crucial steps f<strong>or</strong>ward included in the new FSMA law, itwill take many years to reverse over 100 years of accumulatedneglect of the food safety system’s basic infrastructure, whichwas designed primarily to track down the causes of illnessesand contamination problems after they have occurred. Theseproblems have gradually manifested themselves since the <strong>or</strong>iginalPure Food and Drug Act of 1906 was enacted.Remaining Concerns with Foodb<strong>or</strong>ne IllnessAcc<strong>or</strong>ding to CDC, each year, an estimated 47 million Americanssuffer from foodb<strong>or</strong>ne illnesses caused by pathogens — diseasecausingmicrobes such as bacteria <strong>or</strong> viruses. These illnesses send127,000 people to the hospital and kill approximately 3,000, CDCestimates.286,287 In addition, acc<strong>or</strong>ding to CDC, about two tothree percent of those who are stricken with the illnesses will sufferfrom long-term chronic complications — approximately onemillion Americans, many of whom were not <strong>or</strong>iginally hospitalizedf<strong>or</strong> their infection. These complications can include reactive arthritis,autoimmune thyroid disease, kidney disease, neural and neuromusculardysfunctions, and heart and vascular disease. 288To m<strong>or</strong>e effectively reduce foodb<strong>or</strong>ne illnesses, FDA needssubstantial additional human, scientific, and financial resourcesand quite honestly needs to reinvent itself — to make the shiftto a prevention-based approach in <strong>or</strong>der to give real life to theambitious new food safety law. The President identified FDA’soverhaul of its food safety program as a top pri<strong>or</strong>ity, recommendingan increase of $118 million dollars f<strong>or</strong> Fiscal Year(FY) 2012 above the previous year’s budget; these additionalfunds would help the agency beef up its scientific staff, expandits inspection eff<strong>or</strong>ts, strengthen its ability to check up on imp<strong>or</strong>ts,and take other key steps to improve the safety of thefood supply. The House of Representatives disagreed with theproposed increase, and, instead, passed an austere budget f<strong>or</strong>FDA, slashing its food safety budget by $87 million comparedto the previous year (FY 2011). The Senate approved a modest$40 million increase, and the House-Senate disagreement hadnot been resolved as of the time of this writing.A wide range of stakeholders — the food industry(includingthe Grocery Manufacturers Association, which represents foodprocessing companies), consumer and public health groups (includingPew and the Trust f<strong>or</strong> America’s Health), <strong>or</strong>ganizationsrepresenting the victims of foodb<strong>or</strong>ne illness and their families,and others — have been urging Congress to provide FDA withthe resources it needs to carry out the critical components ofthe food safety law to enable the agency to protect the Americanpublic and reduce the scourge of foodb<strong>or</strong>ne illness.Concerns with Heavy Non-Therapeutic Use ofAntibiotics in Animal AgricultureEven if the FSMA were to be fully funded, however, key foodsafety issues untouched by the 2011 statute include the lack ofeffective restrictions on antibiotic use in animal agriculture, andaging laws governing meat and poultry safety, and the use ofchemicals in food. These laws should be reviewed and updatedas necessary — using the latest science — to tighten the focuson preventing disease.Of particular continuing concern is the extensive non-therapeuticuse of antibiotics in animal agriculture — that is, antibioticuse to promote the animal’s growth <strong>or</strong> to compensate f<strong>or</strong> theeffects of overcrowding <strong>or</strong> unsanitary conditions, not to treatclinically ill animals with curative doses. Such practices carry thepotential to breed antibiotic-resistant bacteria, which can causehuman illnesses that do not respond to the most commonly usedantibiotics. 289 In one example of a serious public health problemthat some experts have been warning about f<strong>or</strong> years therewas a large outbreak of multi-drug resistant Salmonella infectionslinked to consumption of ground turkey; as of September29, 2011 CDC confirmed that 129 people were sickened by aSalmonella strain a strain that is resistant to many f<strong>or</strong>ms of commonly-prescribedantibiotics. 290 CDC noted that this “antibioticresistance may be associated with an increased risk of hospitalization<strong>or</strong> possible treatment failure in infected individuals.” 677
EXPERT perspective continuedNew Law Takes a Big Bite Out of the ProblemFDA data show that 29.2 million pounds of antimicrobialactive ingredients were sold f<strong>or</strong> use infood-producing animals in 2010, an increase ofnearly 1.3 percent from the previous year. 291 Becausethe agency does not publicly track comparabledata f<strong>or</strong> human use, it currently is not possibleto determine with certainty the exact percentageof antibiotics sold f<strong>or</strong> use in food animals. However,recent estimates are that approximately 70percent of all antibiotics in the United States areused non-therapeutically in food animal production;earlier estimates were292, 293, 294lower.The CDC, FDA, U.S. Department of Agriculture,W<strong>or</strong>ld Health Organization, and others havenoted the link between the use of non-therapeuticantibiotics in animal agriculture and antibioticresistantpathogens that can impair the usefulnessof antibiotics prescribed to treat humandisease. 295, 296, 297, 298 Some representatives of themeat and poultry industry, however, contend thatthe problem of antibiotic resistance in humans is“overwhelmingly an issue related to human antibioticuse,” rather than from the consumption ofantibiotics in food animals. 299Concerns with Chemicals Added to FoodIn addition to pathogen-related illnesses attributableto food production, processing, handling,<strong>or</strong> preparation, there are other risks posed bychemicals that are added, intentionally <strong>or</strong> not, tothe food supply. Often these chemical hazards areless well characterized than the microbiologicalrisks, which have been studied f<strong>or</strong> decades.Acc<strong>or</strong>ding to a review published in a peer-reviewedjournal by experts from the Pew HealthGroup’s food additives program, m<strong>or</strong>e than10,000 chemicals were allowed to be added tohuman food in the United States as of January2011. 300 Of particular concern, the study foundthat the safety of m<strong>or</strong>e than 3,000 chemicalsadded to food has not been reviewed <strong>or</strong> evaluatedby FDA. This is because under the currentoutdated system, food companies <strong>or</strong> trade associationsare allowed to make their own determinationthat a chemical they want to add tothe food supply is “generally recognized as safe,”<strong>or</strong> “GRAS,” and they need not inf<strong>or</strong>m FDA <strong>or</strong>the public of this determination. M<strong>or</strong>eover, thisanalysis found that in <strong>or</strong>der to encourage foodcompanies to voluntarily ask FDA to examine thesafety of chemicals they want to add to food, FDAhas moved almost exclusively to a system in whichit evaluates chemicals without notifying the public<strong>or</strong> providing an opp<strong>or</strong>tunity f<strong>or</strong> the public to commenton the chemical’s safety.In sum, under the current system, FDA is unawareof a large number of chemical uses in food and,theref<strong>or</strong>e, cannot ensure that safety decisions regardingthese uses were properly made.Additionally, food manufacturers are not requiredto notify FDA of relevant health and safety studies,thereby placing the agency in the difficultposition of tracking safety inf<strong>or</strong>mation f<strong>or</strong> m<strong>or</strong>ethan 10,000 chemicals with limited resources andinf<strong>or</strong>mation. M<strong>or</strong>eover, the agency’s expeditedapproach to reviewing safety decisions in the pastdecade and a half occurs with little public engagement.Finally, Pew’s research concluded FDA lacksthe resources and inf<strong>or</strong>mation needed to identifyand prevent potential health problems <strong>or</strong> to setpri<strong>or</strong>ities f<strong>or</strong> systematic reevaluation of safetydecisions made during the past half-century. Thisis a troublesome set of findings, and Pew expectsto look at carefully at potential policy solutions tothese and other concerns identified in its ongoingscrutiny of the FDA food additives program, and t<strong>or</strong>ecommend changes as needed in 2012.The Need f<strong>or</strong> Additional Ref<strong>or</strong>msThe FDA Food Safety Modernization Act of 2011and the pesticide residue provisions in the FoodQuality Protection Act of 1996 have addressedsome of the m<strong>or</strong>e serious risks posed by contaminantsin food.78
The newly enacted food safety law will not fulfillits promise, however, if the FDA lacks theresources to carry out its new responsibilities.The House of Representatives’ <strong>or</strong>iginally-passedversion of the food safety legislation included ameasure, which did not make it into the final act,that would have established a registration fee f<strong>or</strong>food facilities to help fund the FDA’s food-safetyactivities. 301 Congress should consider establishinga similar fee through another appropriate act, toensure that the FDA has a stable source of fundingf<strong>or</strong> its food safety program.It also is imp<strong>or</strong>tant to note that the new foodsafetylaw does not address the sh<strong>or</strong>tcomings inthe U.S. Department of Agriculture’s powers toprevent <strong>or</strong> address meat and poultry contamination.F<strong>or</strong> example, a court decision handeddown under the decades-old meat safety lawhas blocked the department from closing downmeat processing plants where repeated tests havefound Salmonella contamination. 302 Additionally,there is continued discussion about consolidatingall federal food safety activities into a singleagency: a Government Accountability Office rep<strong>or</strong>tissued in 2011 has reiterated its previous recommendationthat serious consideration be givento consolidating <strong>or</strong> restructuring the fragmentedfood safety system, which they found is splinteredamong 15 federal agencies, including USDA andFDA, implementing 30 laws. 303M<strong>or</strong>eover, the FDA’s science and risk analysis arein need of modernization and additional resources;FDA’s Science Board found that the “agency suffersfrom serious scientific deficiencies and is notpositioned to meet current <strong>or</strong> emerging regulat<strong>or</strong>yresponsibilities” because the demands onthe FDA have soared in recent years, and theresources have not increased in prop<strong>or</strong>tion to thedemands. 304 The agency’s oversight of food additives—especiallythe procedures f<strong>or</strong> substancesthat are generally recognized as safe—in particularneeds closer scrutiny, as the GovernmentAccountability Office recommended. 305 Issuesthat have been proposed f<strong>or</strong> evaluation includewhether there is a need f<strong>or</strong> regular reevaluationsof current research on the risks posed by all substancesadded to food, and f<strong>or</strong> establishing a anopen and publicly transparent system to evaluateall risks in assessing the safety of these compounds.Legislative <strong>or</strong> administrative actions should be consideredto prevent problematic nontherapeutic usesof antibiotics in animal agriculture, to reduce therisk of creating and spreading antibiotic-resistant“superbugs.” Bills to mandate such ref<strong>or</strong>m wereintroduced in Congress in 2009 and reintroduced in2011, but they have not moved beyond the hearingstage. 306, 307, 308 FDA has proposed a voluntary guidancedocument intended to encourage the judicioususe of antibiotics in food-producing animals, but hasnot yet finalized it. 309 Completion of a strong guidancecould be a helpful first step, but ultimately,mandat<strong>or</strong>y requirements are needed.Finally, measures that prevent the tainting offood by environmental contaminants, such as untreatedsewage <strong>or</strong> manure that enter waters andpollute crops downstream, and requirements tostrengthen controls on air and water dischargesof mercury and other common pollutants that arewidely found in the food supply would help to reducethe health risks to the American public.In the end, while the new 2011 food safety lawwill update and strengthen p<strong>or</strong>tions of the nation’sfood- safety net, there remain significant gaps.America’s food safety infrastructure must takeadvantage of rapidly-developing scientific knowledge,meet the ever-growing needs f<strong>or</strong> scientificcapacity and other resources at FDA, addressemerging pathogens and other newly-recognizedhealth risks, and keep up with the constantlym<strong>or</strong>phingglobal food industry. We must reviewand, as necessary, update our mid-20th Centuryfood laws and programs, to ensure that they arepreventing 21st Century threats to public health.79
All-Hazards Preparedness Funding by Source and YearFY 2010 FY 2011 % ChangeFY 10 - FY 11State CDC ASPR Total State CDC ASPR TotalAlabama $10,048,584 $5,959,171 $16,007,755 Alabama $8,633,983 $5,386,508 $14,020,491 -12.4%Alaska $5,165,000 $1,295,371 $6,460,371 Alaska $5,177,600 $1,211,937 $6,389,537 -1.1%Arizona $14,047,671 $7,819,583 $21,867,254 Arizona $11,894,861 $7,051,765 $18,946,626 -13.4%Arkansas $7,393,805 $3,836,580 $11,230,385 Arkansas $6,469,981 $3,486,575 $9,956,556 -11.3%Calif<strong>or</strong>nia $49,301,738 $31,967,442 $81,269,180 Calif<strong>or</strong>nia $41,661,534 $28,666,533 $70,328,067 -13.5%Col<strong>or</strong>ado $10,875,195 $6,142,385 $17,017,580 Col<strong>or</strong>ado $9,397,930 $5,550,503 $14,948,433 -12.2%Connecticut $8,719,806 $4,660,301 $13,380,107 Connecticut $7,553,479 $4,223,889 $11,777,368 -12.0%Delaware $5,150,000 $1,513,099 $6,663,099 Delaware $5,422,932 $1,406,825 $6,829,757 2.5%D.C. $6,616,482 $1,682,835 $8,299,317 D.C. $6,730,903 $1,558,756 $8,289,659 -0.1%Fl<strong>or</strong>ida $33,481,834 $21,973,177 $55,455,011 Fl<strong>or</strong>ida $27,687,829 $19,720,658 $47,408,487 -14.5%Ge<strong>or</strong>gia $18,481,819 $11,615,246 $30,097,065 Ge<strong>or</strong>gia $15,653,814 $10,449,266 $26,103,080 -13.3%Hawaii $5,249,782 $2,025,920 $7,275,702 Hawaii $5,260,290 $1,865,852 $7,126,142 -2.1%Idaho $5,495,096 $2,240,733 $7,735,829 Idaho $5,181,907 $2,058,131 $7,240,038 -6.4%Illinois $19,496,622 $12,357,745 $31,854,367 Illinois $16,845,953 $11,113,877 $27,959,830 -12.2%Indiana $12,995,857 $7,994,316 $20,990,173 Indiana $11,146,909 $7,208,168 $18,355,077 -12.6%Iowa $7,565,448 $4,039,814 $11,605,262 Iowa $6,595,869 $3,668,490 $10,264,359 -11.6%Kansas $7,530,021 $3,781,030 $11,311,051 Kansas $6,595,020 $3,436,853 $10,031,873 -11.3%Kentucky $9,455,848 $5,492,721 $14,948,569 Kentucky $8,275,695 $4,968,989 $13,244,684 -11.4%Louisiana $9,999,458 $5,589,694 $15,589,152 Louisiana $8,632,297 $5,055,790 $13,688,087 -12.2%Maine $5,259,067 $2,068,743 $7,327,810 Maine $5,206,160 $1,904,184 $7,110,344 -3.0%Maryland $12,720,551 $7,166,017 $19,886,568 Maryland $11,057,196 $6,466,757 $17,523,953 -11.9%Massachusetts $15,229,770 $8,141,119 $23,370,889 Massachusetts $13,459,602 $7,339,572 $20,799,174 -11.0%Michigan $20,143,034 $12,483,796 $32,626,830 Michigan $16,543,509 $11,226,706 $27,770,215 -14.9%Minnesota $12,911,644 $6,633,486 $19,545,130 Minnesota $10,842,711 $5,990,088 $16,832,799 -13.9%Mississippi $7,527,286 $3,954,888 $11,482,174 Mississippi $6,565,242 $3,592,473 $10,157,715 -11.5%Missouri $12,572,343 $7,435,455 $20,007,798 Missouri $10,717,722 $6,707,932 $17,425,654 -12.9%Montana $5,166,198 $1,621,303 $6,787,501 Montana $5,178,911 $1,503,679 $6,682,590 -1.5%Nebraska $5,876,388 $2,599,056 $8,475,444 Nebraska $5,234,954 $2,378,867 $7,613,821 -10.2%Nevada $7,511,623 $3,462,259 $10,973,882 Nevada $6,585,802 $3,151,521 $9,737,323 -11.3%New Hampshire $5,349,356 $2,060,815 $7,410,171 New Hampshire $5,398,877 $1,897,087 $7,295,964 -1.5%New Jersey $18,015,661 $10,856,284 $28,871,945 New Jersey $16,184,853 $9,769,919 $25,954,772 -10.1%New Mexico $7,643,606 $2,820,161 $10,463,767 New Mexico $6,526,120 $2,576,778 $9,102,898 -13.0%New Y<strong>or</strong>k $22,932,149 $13,666,210 $36,598,359 New Y<strong>or</strong>k $19,284,669 $12,285,085 $31,569,754 -13.7%N<strong>or</strong>th Carolina $16,552,440 $11,012,906 $27,565,346 N<strong>or</strong>th Carolina $14,020,450 $9,910,111 $23,930,561 -13.2%N<strong>or</strong>th Dakota $5,021,860 $1,254,791 $6,276,651 N<strong>or</strong>th Dakota $5,180,405 $1,175,614 $6,356,019 1.3%Ohio $20,947,527 $14,124,698 $35,072,225 Ohio $17,618,925 $12,695,478 $30,314,403 -13.6%Oklahoma $8,487,239 $4,748,620 $13,235,859 Oklahoma $7,509,542 $4,302,943 $11,812,485 -10.8%Oregon $8,871,324 $4,892,898 $13,764,222 Oregon $7,829,790 $4,432,087 $12,261,877 -10.9%Pennsylvania $22,808,671 $15,267,347 $38,076,018 Pennsylvania $19,774,638 $13,718,265 $33,492,903 -12.0%Rhode Island $5,150,000 $1,767,281 $6,917,281 Rhode Island $5,302,058 $1,634,345 $6,936,403 0.3%South Carolina $11,034,653 $5,629,437 $16,664,090 South Carolina $9,308,851 $5,091,363 $14,400,214 -13.6%South Dakota $5,150,000 $1,428,159 $6,578,159 South Dakota $5,169,600 $1,330,796 $6,500,396 -1.2%Tennessee $12,711,428 $7,668,219 $20,379,647 Tennessee $10,845,628 $6,916,279 $17,761,907 -12.8%Texas $43,194,539 $28,404,362 $71,598,901 Texas $37,545,665 $25,477,218 $63,022,883 -12.0%Utah $7,328,511 $3,526,992 $10,855,503 Utah $6,464,082 $3,209,463 $9,673,545 -10.9%Vermont $5,193,078 $1,240,595 $6,433,673 Vermont $5,192,031 $1,162,908 $6,354,939 -1.2%Virginia $17,063,098 $9,572,306 $26,635,404 Virginia $14,483,987 $8,620,629 $23,104,616 -13.3%Washington $13,731,541 $8,091,982 $21,823,523 Washington $11,711,066 $7,295,589 $19,006,655 -12.9%West Virginia $5,898,188 $2,658,572 $8,556,760 West Virginia $5,336,731 $2,432,140 $7,768,871 -9.2%Wisconsin $13,276,438 $7,095,720 $20,372,158 Wisconsin $11,235,615 $6,403,834 $17,639,449 -13.4%Wyoming $5,000,000 $1,111,323 $6,111,323 Wyoming $5,169,600 $1,047,196 $6,216,796 1.7%80CDC TotalFY 10**APPENDIX A: CDC AND ASPR PREPAREDNESS GRANTS BY STATEASPR* TotalFY 10**Grand TotalFY 10**CDC TotalFY 11**ASPR* TotalFY 11**Grand TotalFY 11**Grand TotalPercent ChangeFY 10 - FY 11$633,349,277 $356,452,963 $989,802,240 $553,303,778 $321,736,271 $875,040,049 -11.6%* <strong>Not</strong>e that state CDC total funding include funding f<strong>or</strong> Cities Readiness Initiative funding, Level 1 chemical lab<strong>or</strong>at<strong>or</strong>y funding, EWIDS funding and Risk funding although notevery state receives funding in all of these supplemental categ<strong>or</strong>ies.**<strong>Not</strong>e that totals do not include funds f<strong>or</strong> three maj<strong>or</strong> U.S. metropolitan areas, Chicago, L.A. County,and New Y<strong>or</strong>k City, U.S. Territ<strong>or</strong>ies, such as Puerto Rico and Guam, and Freely Associated States of the Pacific, such as the Marshall Islands.Source: FY2011 Funding 1) CDC. Public Health Emergency Preparedness Cooperative Agreement Budget Period 11 (FY 2011) Funding. (accessed September 8, 2011). 2) HHS.gov. HHS Grants Boost Disaster Preparedness in Hospitals, Health Care Systems.News Release, July 1, 2011. FY2010 Funding 1) CDC. Public Health Emergency Preparedness CooperativeAgreement Budget Period 10 Extension (FY 2010) Funding. (accessed October 14, 2010). 2) HHS.gov. HHS Provides $390.5 Million to Improve Hospital Preparedness and Emergency Response. NewsRelease, July 7, 2010. (accessed July 8, 2010.)
APPENDIX B: Data and Methodology f<strong>or</strong> State PublicHealth BudgetsTFAH conducted an analysis of state spendingon public health f<strong>or</strong> the last budget cycle, fiscalyear 2010-2011. F<strong>or</strong> those states that only rep<strong>or</strong>ttheir budgets in biennium cycles, the 2009-2011period (<strong>or</strong> the 2010-2012 and 2010-2011 f<strong>or</strong> Virginiaand Wyoming respectively) was used, andthe percent change was calculated from the lastbiennium, 2007-2009 (<strong>or</strong> 2008-2010 and 2009-2010 f<strong>or</strong> Virginia and Wyoming respectively).This analysis was conducted from August toOctober of 2011 using publicly available budgetdocuments through state government websites. Based on what was made publicly available,budget documents used included eitherexecutive budget document that listed actualexpenditures, estimated expenditures, <strong>or</strong> finalappropriations; appropriations bills enacted bythe state’s legislature; <strong>or</strong> documents from legislativeanalysis offices.“Public health” is defined to broadly include allhealth spending with the exception of Medicaid,CHIP, <strong>or</strong> comparable health coverage programsf<strong>or</strong> low-income residents. Federal funds,mental health funds, addiction <strong>or</strong> substanceabuse-related funds, WIC funds, services relatedto developmental disabilities <strong>or</strong> severely disabledpersons, and state-spons<strong>or</strong>ed pharmaceuticalprograms also were not included in <strong>or</strong>derto make the state-by-state comparison m<strong>or</strong>e accuratesince many states receive federal moneyf<strong>or</strong> these particular programs. In a few cases,state budget documents did not allow these programs,<strong>or</strong> other similar human services, to bedisaggregated; these exceptions are noted. F<strong>or</strong>most states, all state funding, regardless of generalrevenue <strong>or</strong> other state funds (e.g. dedicatedrevenue, fee revenue, etc.), was used. In somecases, only general revenue funds were used in<strong>or</strong>der to separate out federal funds; these exceptionsare also noted.Because each state allocates and rep<strong>or</strong>ts itsbudget in a unique way, comparisons acrossstates are difficult. This methodology may includeprograms that, in come cases, the statemay consider a public health function, but themethodology used was selected to maximize theability to be consistent across states. As a result,there may be programs <strong>or</strong> items states may wishto be considered “public health” that may notbe included in <strong>or</strong>der to maintain the comparativevalue of the data.Finally, to improve the comparability of thebudget data between FY 2009-2010 and FY2010-2011 (<strong>or</strong> between biennium), TFAH adjustedthe FY 2009-2010 numbers f<strong>or</strong> inflation(using a 0.9652 conversion fact<strong>or</strong> based on theU.S. Dept. of Lab<strong>or</strong> Bureau of Lab<strong>or</strong> Statistics;Consumer Price Index Inflation Calculat<strong>or</strong> athttp://www.bls.gov/cpi/).After compiling the results from this onlinereview of state budget documents, TFAH co<strong>or</strong>dinatedwith the Association of State and Territ<strong>or</strong>ialHealth Officials (ASTHO) to confirm thefindings with each state health official. ASTHOsent out emails on October 26, 2011 and statehealth officials were asked to confirm <strong>or</strong> c<strong>or</strong>rectthe data with TFAH staff by November 11, 2011.ASTHO followed up via email with those statehealth officials who did not respond by the November11, 2011 deadline and were given untilNovember 18, 2011 to respond. The states thatdid not reply by that date were assumed to be inacc<strong>or</strong>dance with the findings.81
82Endnotes1 Public Health Infrastructure — A Status Rep<strong>or</strong>t. Atlanta,Ge<strong>or</strong>gia: Centers f<strong>or</strong> Disease Control and Prevention,2001.2 The Future of the Public’s Health in the 21st Century. Washington,D.C.: Institute of Medicine, 20033 HHS Bioterr<strong>or</strong>ism Preparedness Programs: States Rep<strong>or</strong>tedProgress But Fell Sh<strong>or</strong>t of Program Goals in 2002. Washington,D.C.: Government Accountability Office, 2004.4 Budget Cuts Continue to Affect the Health of Americans: UpdateNovember 2011. Washington, D.C.: Association ofState and Territ<strong>or</strong>ial Health Officials, November 2011.5 Local Health Department Job Losses and Program Cuts:Findings from July 2011 Survey. Washington, D.C.: NationalAssociation of County and City Health Officials,September 2011; and Budget Cuts Continue to Affect theHealth of Americans: Update November 2011. Washington,D.C.: Association of State and Territ<strong>or</strong>ial HealthOfficials, November 2011.6 Adjusting f<strong>or</strong> inflation.7 Institute of Medicine (IOM). The Future of the Public’sHealth in the 21st Century. Washington, D.C.: NationalAcademies Press, 2002.8 Cities Readiness Initiative. In U.S. Centers f<strong>or</strong> DiseaseControl and Prevention. http://www.bt.cdc.gov/cri/ (accessedSeptember 2011).9 Cities Readiness Initiative. In Washington County, Oregon,Department of Health and Human Services. http://www.co.washington.<strong>or</strong>.us/HHS/EmergencyPreparedness/cities-readiness-initiative.cfm(accessed September2011)10 Alternative Methods of Dispensing: Model Highlights.Washington, D.C.: National Association of Countyand City Health Officials, 2008, http://www.naccho.<strong>or</strong>g/topics/emergency/SNS/upload/POD-Article-2_utilizing-school-busses.pdf (accessed September 2011)11 Public Health Preparedness: 2011 State-by-State Update onLab<strong>or</strong>at<strong>or</strong>y Capabilities and Response Readiness Planning.12 U.S. Centers f<strong>or</strong> Disease Control and Prevention. Cities andMetropolitan Areas That Receive CRI Funding. Atlanta,GA: U.S. Centers f<strong>or</strong> Disease Control and Prevention,2011, http://www.cdc.gov/phpr/documents/PHEP_FY_2011.pdf (accessed September 2011).14 U.S. Centers f<strong>or</strong> Disease Control and Prevention.“Facts About the Lab<strong>or</strong>at<strong>or</strong>y Response Netw<strong>or</strong>k.”http://www.bt.cdc.gov/lrn/factsheet.asp. (accessedSeptember 8, 2011).15 Public Health Preparedness: 2011 State-by-State Update onLab<strong>or</strong>at<strong>or</strong>y Capabilities and Response Readiness Planning.Washington, D.C.: U.S. Centers f<strong>or</strong> Disease Control andPrevention, 2011. http://www.cdc.gov/phpr/pubs-links/2011/documents/SEPT_UPDATE_REPORT_9-13-2011-Final.pdf (accessed September 2011)16 U.S. Centers f<strong>or</strong> Disease Control and Prevention.“Facts About the Lab<strong>or</strong>at<strong>or</strong>y Response Netw<strong>or</strong>k.”http://www.bt.cdc.gov/lrn/factsheet.asp. (accessedSeptember 8, 2011).17 http://thomas.loc.gov/cgi-bin/query/z?c107:H.R.3448.ENR:18 http://www.whitehouse.gov/the-press-office/executive-<strong>or</strong>der-optimizing-security-biological-selectagents-and-toxins-united-stat19 http://www.selectagents.gov/resources/HHS%20Federal%20Register.pdf20 http://blog.aphl.<strong>or</strong>g/2010/09/aphl-briefs-expertson-biosecurity-in-public-health-lab<strong>or</strong>at<strong>or</strong>ies/21 http://blog.aphl.<strong>or</strong>g/2011/08/nods-of-agreementin-a-federal-w<strong>or</strong>kgroup-meeting/22 http://www.phe.gov/Preparedness/legal/boards/fesap/Documents/fesap-recommendations-101102.pdf23 U.S. Centers f<strong>or</strong> Disease Control and Prevention.Career Epidemiology Field Officer Program. http://www.cdc.gov/phpr/science/cefo.htm (accessed September2011).24 U.S. Centers f<strong>or</strong> Disease Control and Prevention, PublicHealth Matters Blog: Battling Disease Outbreaksin the Big Apple. http://blogs.cdc.gov/publichealthmatters/2011/02/battling-disease-outbreaks-in-thebig-apple-2/(accessed September 2011).25 U.S. Centers f<strong>or</strong> Disease Control and Prevention.CEFO Field Locations. http://www.cdc.gov/phpr/science/cefomap.htm (accessed September 2011).26. CDC Awards $13 Million f<strong>or</strong> Preparedness and ResponseLearning Centers. In U.S. Centers f<strong>or</strong> Disease Control andPrevention. http://www.cdc.gov/media/pressrel/2010/r100914.htm (accessed September 2011).27 Crowley C. “School Receives $7.9 Million BirthdayGift.” The Albany Times-Union September 25, 2010.28. Preparedness and Emergency Response LearningCenter, Hist<strong>or</strong>y. In Harvard University School of PublicHealth. http://www.hsph.harvard.edu/hperlc/hist<strong>or</strong>y/(accessed September 2011).29 Redlener I. “America Unprepared: Are Budget CutsUndermining National Disaster Readiness?” PoliticalMachine July 19, 201130 Domestic Preparedness Cuts in the Current FederalBudget Threaten Infrastructure Gains and Public HealthPreparedness. In Columbia University Mailman School ofPublic Health. http://www.ncdp.mailman.columbia.edu/files/911memo.pdf (accessed September 2011).31 Redlener I. “America Unprepared: Are Budget CutsUndermining National Disaster Readiness?”32. Preparedness and Emergency Response LearningCenters (PERLC) Factsheet. In U.S. Centers f<strong>or</strong> DiseaseControl and Prevention. http://www.cdc.gov/phpr/perlc_factsheet.htm (accessed September 2011).33.ERP Preparedness and Emergency Response ResearchCenters (PERRCs) — Program Updates. InU.S. Centers f<strong>or</strong> Disease Control and Prevention. http://www.cdc.gov/phpr/science/updates.htm (accessedSeptember 2011).34 Ibid.35 ASPH email.36 Fiscal Year 2012 Justification of Estimates f<strong>or</strong> AppropriationCommittees. Atlanta, GA: U.S. Centers f<strong>or</strong> DiseaseControl and Prevention, 2011, http://www.cdc.gov/fmo/topic/Budget%20Inf<strong>or</strong>mation/appropriations_budget_f<strong>or</strong>m_pdf/FY2012_CDC_CJ_Final.pdf(accessed September 2011). (NB: on p. 261)37 National Planning Scenarios: Created f<strong>or</strong> Use in National,Federal, State and Local Homeland Security Activities.April 2005. Achieved copy: http://media.washingtonpost.com/wp-srv/nation/nationalsecurity/earlywarning/NationalPlanningScenariosApril2005.pdf(accessed October 5, 2011).38 National Planning Scenarios: Created f<strong>or</strong> Use in National,Federal, State and Local Homeland Security Activities.April 2005. Achieved copy: http://media.washingtonpost.com/wp-srv/nation/nationalsecurity/earlywarning/NationalPlanningScenariosApril2005.pdf(accessed October 5, 2011).
39 Khan AS. Public health preparedness and responsein the USA since 9/11: a national health security imperative.The Lancet, 378(9794): 953-6, 2011.40 Ibid.41 2009 National Assessment of Epidemiology Capacity: Findingsand Recommendations. Atlanta, GA: Council of Stateand Territ<strong>or</strong>ial Epidemiologists, 2009, http://www.cste.<strong>or</strong>g/dnn/P<strong>or</strong>tals/0/2009EpidemiologyCapacityAssessmentRep<strong>or</strong>t.pdf (accessed September 2011)42 Farley TA and Weisfuse I. Redefining of public healthpreparedness after 9/11. The Lancet, 378(9794): 957-9, 2011.43 Ibid.44 Inglesby TV. Progress in Disaster Planning and PreparednessSince 2001. Journal of the American MedicalAssociation, 2011;306(12):1372-1373, 2011..45 Franco C and Sell TK. Federal Agency biodefensefunding, FY2011-FY2012. Biosecurity and Bioterr<strong>or</strong>ism,9(2): 117-137, 2011.46 Inglesby TV, 1372-1373.47 “Public Health Accreditation Board Launches NationalAccreditation f<strong>or</strong> Health Departments.” Public HealthAccreditation Board. September 16, 2011. http://www.phaboard.<strong>or</strong>g/wp-content/uploads/PHAB-Press-Release-09.14.112.pdf (accessed November 2011).48 Ibid.49 Budget Cuts Continue to Affect the Health of Americans: UpdateNovember 2011. Washington, D.C.: Association ofState and Territ<strong>or</strong>ial Health Officials, November 2011.50 Ibid.51 Local Leaders Discuss Emergency Preparedness.In International City/County Management Association.http://icma.<strong>or</strong>g/en/icma/newsroom/highlights/Article/101480/Local_Leaders_Discuss_How_Jurisdictions_Prepare_f<strong>or</strong>_Emergencies(accessed September2011)52 Bio-Response Rep<strong>or</strong>t Card. Washington, D.C.: BipartisanWMD Terr<strong>or</strong>ism Research Center, 2011, http://www.wmdcenter.<strong>or</strong>g/wp-content/uploads/2011/10/bio-response-rep<strong>or</strong>t-card-2011.pdf (accessed October2011).53 McNichol E et al. States Continue to Feel Recession’s Impact.Washington, D.C.: Center on Budget and PolicyPri<strong>or</strong>ities, October 2010, http://www.cbpp.<strong>or</strong>g/files/9-8-08sfp.pdf (accessed November 15, 2010).54 Local Health Department Job Losses and Program Cuts:Findings from July 2011 Survey. Washington, D.C.:National Association of County and City Health Officials,September 201155 Adjusting f<strong>or</strong> inflation.56 Confronting the Public Health W<strong>or</strong>kf<strong>or</strong>ce Crisis: ASPHStatement on the Public Health W<strong>or</strong>kf<strong>or</strong>ce. Washington,D.C.: Association of Schools of Public Health, 2008.57 2007 State Public Health W<strong>or</strong>kf<strong>or</strong>ce Survey Results. Arlington,VA: Association of State and Territ<strong>or</strong>ialHealth Officers, 2007.58 Public Health’s Infrastructure — A Status Rep<strong>or</strong>t. Atlanta,Ge<strong>or</strong>gia: U.S. Centers f<strong>or</strong> Disease Control and Prevention,2001.59 Creation of the Department of Homeland Security.In U.S. Department of Homeland Security. http://www.dhs.gov/xabout/hist<strong>or</strong>y/gc_1297963906741.shtm(accessed October 2011).60 “West Nile Virus 2002 Case Count,” Centers f<strong>or</strong> DiseaseControl and Prevention. (accessed July2003).61 SARS and Its Implications f<strong>or</strong> U.S. Public Health Policy.Washington, D.C.: Trust f<strong>or</strong> America’s Health, 2008,http://healthyamericans.<strong>or</strong>g/rep<strong>or</strong>ts/files/SARSrep<strong>or</strong>t.pdf(accessed October 2011).62 Rubinkam M. “Listeria outbreak traced to meat processingplant outside Philadelphia.” The AssociatedPress October 16, 2002.63 U.S. Centers f<strong>or</strong> Disease Control and Prevention,(2002). Update: Listeriosis Outbreak Investigation. [PressRelease]. http://www.cdc.gov/media/pressrel/r021121.htm (accessed October 2011).64 U.S. Department of Health and Human Services.(2002). HHS Announces $1.1 Billion in Funding to Statesf<strong>or</strong> Bioterr<strong>or</strong>ism Preparedness. [Press Release]. http://archive.hhs.gov/news/press/2002pres/20020131b.html (accessed October 2011).65 Hospitals Rising to the Challenge: The First Five Yearsof the U.S. Hospital Preparedness Program and Pri<strong>or</strong>itiesGoing F<strong>or</strong>ward. Pittsburgh, PA: Center F<strong>or</strong> Biosecurity,2009, http://www.upmc-biosecurity.<strong>or</strong>g/website/resources/publications/2009/2009-04-16-hpprep<strong>or</strong>t.html (accessed September 2011).66 Funding, Guidance, and Technical Assistance toStates, Localities, and Territ<strong>or</strong>ies. In U.S. Centers f<strong>or</strong>Disease Control and Prevention, Office of Public HealthPreparedness and Response. http://www.cdc.gov/phpr/coopagreement.htm (accessed September 2011).67 Creation of the Department of Homeland Security.In U.S. Department of Homeland Security. http://www.dhs.gov/xabout/hist<strong>or</strong>y/gc_1297963906741.shtm(accessed October 2011).68 Who Became Part of the Department? In U.S. Departmentof Homeland Security. http://www.dhs.gov/xabout/hist<strong>or</strong>y/edit<strong>or</strong>ial_0133.shtm (accessed October 2011).69 National <strong>Not</strong>es. MRC In Focus, 5(3): 1-7, Summer2011, http://www.medicalreservec<strong>or</strong>ps.gov/File/NationalNewsletters/MRCInFocus-Summer2011.pdf(accessed October 2011).70 Frist, B. Public health and national security: the criticalrole of increased federal supp<strong>or</strong>t. Health Affairs,21(6): 117-30, 2002.71 Stockman LJ, Bellamy R, Garner P, et al. SARS: systematicreview of treatment effects. PLoS Medicine,3(9): 1525-31, 2006.72. Update 95 — SARS: Chronology of a serial killer. InW<strong>or</strong>ld Health Organization. http://www.who.int/csr/don/2003_07_04/en/index.html (accessed October2011).73 SARS and Its Implications f<strong>or</strong> U.S. Public Health Policy.Washington, D.C.: Trust f<strong>or</strong> America’s Health, 2008,http://healthyamericans.<strong>or</strong>g/rep<strong>or</strong>ts/files/SARSrep<strong>or</strong>t.pdf(accessed October 2011).74 Brown D. “The SARS Triumph, And What It Promises.”The Washington Post July 20, 2003.75 Summary table of SARS cases by country, 1 November2002 — 7 August 2003. In W<strong>or</strong>ld Health Organization.http://www.who.int/csr/sars/country/country2003_08_15.pdf (accessed October 2011).76 U.S. Centers f<strong>or</strong> Disease Control and Prevention. Update:Severe Acute Respirat<strong>or</strong>y Syndrome — United States,2003. M<strong>or</strong>bidity and M<strong>or</strong>tality WeeklyRep<strong>or</strong>t,, 52(18);411-413,2003, http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5218a2.htm (accessed October 2011).77 U.S. Centers f<strong>or</strong> Disease Control and Prevention.Update: Multistate Outbreak of Monkeypox — Illinois,Indiana, Kansas, Missouri, Ohio, and Wisconsin,2003. M<strong>or</strong>bidity and M<strong>or</strong>tality Weekly Rep<strong>or</strong>t, 52(25);589-590, 2003,. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5225a4.htm (accessed October 2011).83
78 Yates J. “African rodents had monkeypox; Virus’ U.S.spread is traced to pets.” Chicago Tribune July 3, 2003.79 Mandak J. “Fourth person dies as result of 2003 hepatitisA outbreak at Pa. restaurant.” The Associated PressApril 3, 2004.80 U.S. Centers f<strong>or</strong> Disease Control and Prevention.Hepatitis A Outbreak Associated with Green Onions ata Restaurant — Monaca, Pennsylvania, 2003. M<strong>or</strong>bidityand M<strong>or</strong>tality Weekly Rep<strong>or</strong>t, 52(47);1155-1157, 2003,http://www.cdc.gov/mmwR/preview/mmwrhtml/mm5247a5.htm (accessed October 2011).81 McNeil D. “U.S. Reduces Testing f<strong>or</strong> Mad Cow Disease,Citing Few Infections.” The New Y<strong>or</strong>k Times July21, 200682 Smallpox Vaccination: Implementation of National ProgramFaces Challenges. Washington, D.C.: U.S. GeneralAccounting Office, 2003. http://www.gao.gov/new.items/d03578.pdf (accessed October 2011).83 Strategic National Stockpile (SNS). In U.S. Centers f<strong>or</strong> DiseaseControl and Prevention. http://www.cdc.gov/phpr/stockpile/stockpile.htm. (accessed October 2011).84 Bioterr<strong>or</strong>ism: Preparedness Varied across State and LocalJurisdictions. Washington, D.C.: U.S. General AccountingOffice, 2003.85 Biosense. In U.S. Centers f<strong>or</strong> Disease Control and Prevention.http://www.cdc.gov/biosense/ (accessed September2011).86. Updates on the BioSense Program Redesign: 2011Public Health Preparedness Summit. In Slideshow.http://www.slideshare.net/kasshout/kass-hout-phps(accessed September 2011).87 Effectiveness of National Biosurveillance Systems: Bio-Watch and the Public Health System: Interim Rep<strong>or</strong>t.Washington, D.C.: National Academies of Science,2009, http://www.nap.edu/openbook.php?rec<strong>or</strong>d_id=12599&page=1 (accessed October 2011).88 The Future of the Public’s Health in the 21st Century.Washington, DC: Institute of Medicine, 2003.89 Homeland Security Presidential Directives. In U.S. Departmentof Homeland Security. http://www.dhs.gov/xabout/laws/edit<strong>or</strong>ial_0607.shtm (accessed October 2011).90 <strong>Ready</strong> <strong>or</strong> <strong>Not</strong>? 2003: Protecting the Public’s Health in theAge of Bioterr<strong>or</strong>ism. Washington, D.C.: Trust f<strong>or</strong> America’sHealth, 2003.91 Starr B, Carroll J,Feig C, et al. “Frist: Ricin Confirmedbut No Illness Rep<strong>or</strong>ted.” CNN.com February4, 2004. http://www.cnn.com/2004/US/02/03/senate.hazardous/(accessed November 4, 2004).92 Miller J. “Cens<strong>or</strong>ed Study on Bioterr<strong>or</strong> Doubts U.S.Preparedness.” New Y<strong>or</strong>k Times March 3, 2004.93 Gentile G. “Salmonella scare prompts nationwide almondrecall.” The Associated Press May 28, 2004.94 U.S. Centers f<strong>or</strong> Disease Control and Prevention.Outbreak of Salmonella Serotype Enteritidis InfectionsAssociated with Raw Almonds --- United Statesand Canada, 2003--2004. M<strong>or</strong>bidity and M<strong>or</strong>tality WeeklyRep<strong>or</strong>t, 53(22);484-487, 2004, http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5322a8.htm (accessedOctober 2011).95 Murphy J. “FDA: Sheetz tomatoes may have beentainted on the farm.” Food Chemical News August 9, 2004.96 U.S. Centers f<strong>or</strong> Disease Control and Prevention.Outbreaks of Salmonella Infections Associated withEating Roma Tomatoes ---United States and Canada,2004. M<strong>or</strong>bidity and M<strong>or</strong>tality Weekly Rep<strong>or</strong>t, 54(13);325-328, 2005, http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5413a1.htm (accessed October 2011).97 U.S. Department of Health and Human Services,(2004). PHS Commissioned C<strong>or</strong>ps Deploys PublicHealth Professionals to Provide Hurricane Relief.[Press Release].98 “Health Secretary: No Flu Vaccine Crisis.” CNN.com October 18, 2004. http://www.cnn.com/2004/HEALTH/10/18/flu/ (accessed November 16, 2004).99 Cage S. “WHO: Apparently healthy ducks may beinfecting humans with bird flu.” The Associated PressOctober 30, 2004.100 Homeland Security.. In The White House. http://www.whitehouse.gov/homeland/20040430.html(accessed October 26, 2004).101 Cities Readiness Initiative. In U.S. Centers f<strong>or</strong> DiseaseControl and Prevention. http://www.bt.cdc.gov/cri/(accessed September 2011).102 U.S. Centers f<strong>or</strong> Disease Control and Prevention.Multistate Outbreaks of Salmonella Infections Associatedwith Raw Tomatoes Eaten in Restaurants--- United States, 2005--2006. M<strong>or</strong>bidity and M<strong>or</strong>talityWeekly Rep<strong>or</strong>t, 56(35);909-911, 2007, http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5635a3.htm (accessed October 2011).103 The Commissioned C<strong>or</strong>ps’ Response to Hurricanes Katrinaand Rita. Washington, D.C.: Office of the Inspect<strong>or</strong>General, U.S. Department of Health and HumanServices, 2007, http://oig.hhs.gov/oei/rep<strong>or</strong>ts/oei-09-06-00030.pdf (accessed October 4, 2007).104 Ibid.105 About the Commissioned C<strong>or</strong>ps. In U.S. PublicHealth Service. http://www.usphs.gov/AboutUs/ (accessedOctober 4, 2007).106 U.S. Centers f<strong>or</strong> Disease Control and Prevention.Multistate Outbreaks of Salmonella Infections Associatedwith Raw Tomatoes Eaten in Restaurants— United States, 2005--2006. M<strong>or</strong>bidity and M<strong>or</strong>talityWeekly, 56(35);909-911, 2007, http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5635a3.htm (accessedOctober 2011).107 Federal Emergency Management Agency. NationalPlanning Scenarios Fact Sheet. http://www.fema.gov/pdf/media/factsheets/2009/npd_natl_plan_scenario.pdf(accessed September 2011).108 Freeman A. “U.S. to spend $7.1-billion battling avianflu; Plan includes help f<strong>or</strong> other countries, drugstockpiles and new vaccines.” The Globe and Mail November2, 2005109 Knickerbocker B. “Third Mad Cow Case in USRaises Questions about Testing.” Christian ScienceMonit<strong>or</strong> March 15, 2006.110 “First Apparent U.S. Case of Mad Cow Disease Discovered.”CNN.com December 24, 2003, http://www.cnn.com/2003/US/12/23/mad.cow/ (accessedOctober 16, 2006).111 Sander L. “Nebraska Woman’s Death Brings to 3Those Attributed to Spinach.” The New Y<strong>or</strong>k TimesOctober 7, 2006.112 Ibid.113 Shin A. “E. Coli Detected Near Spinach.” The WashingtonPost October 13, 2006.114 U.S. Centers f<strong>or</strong> Disease Control and Prevention.Multistate Outbreaks of Salmonella Infections Associatedwith Raw Tomatoes Eaten in Restaurants--- United States, 2005--2006. M<strong>or</strong>bidity and M<strong>or</strong>talityWeekly Rep<strong>or</strong>t, 56(35);909-911, 2007, http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5635a3.htm (accessed October 2011).84
115 Salmonellosis — Outbreak Investigation, February2007. In U.S. Centers f<strong>or</strong> Disease Control and Prevention.http://www.cdc.gov/ncidod/dbmd/diseaseinfo/salmonellosis_2007/outbreak_notice.htm (accessedOctober 2011).116 Stobbe M. “CDC Tracks Peanut Butter Contamination.”The Associated Press February 16, 2007.117 Funk J. “Moisture Led to Salmonella Outbreak.” TheAssociated Press April 5, 2007.118 Multistate Outbreak of E. coli O157 Infections, November-December2006. In U.S. Centers f<strong>or</strong> Disease Controland Prevention. http://www.cdc.gov/ecoli/2006/december/121406.htm (accessed October 2011).119 Bridges A. “Lettuce Implicated in Taco Bell Outbreak.”The Associated Press December 14, 2006.120 Snapshots of Public Health Preparedness in Statesand Directly Funded Localities: Rhode Island. InU.S. Centers f<strong>or</strong> Disease Control and Prevention. http://www.bt.cdc.gov/publications/feb08phprep/section2/RhodeIsland.asp(accessed October 2011).121 Vernon-Sparks L. “Probe into encephalitis outbreakwill continue.” The Providence Journal January 10, 2007.122 National Conference of Commissioners on Unif<strong>or</strong>mState Laws. “Unif<strong>or</strong>m Volunteer Emergency HealthPractitioners Act — A Summary.” NCCUSL.123 The Pandemic and All-Hazards Preparedness Act (P.L.109-417): Provisions and Changes to PreexistingLaw. Washington, D.C.: Congressional ResearchService, 2007.124 Khan AS. Public health preparedness and responsein the USA since 9/11: a national health securityimperative. The Lancet, 378(9794): 953-6, 2011.125 Hodge JG and Gostin LO. The Pandemic and All-Hazards Preparedness Act: Improving Public HealthEmergency Response. Journal of the American MedicalAssociation, 297(15): 1708-11, 2007.126 Pandemic and All Hazards Preparedness Act. InU.S. Department of Health and Human Services. http://www.phe.gov/preparedness/legal/pahpa/pages/default.aspx (accessed October 2011).127 U.S. Centers f<strong>or</strong> Disease Control and Prevention.(2007). Media Update: XDR TB Public Health Investigation.[Press Release]. http://www.cdc.gov/media/pressrel/2007/r070602.htm (accessed October 2011).128 Simmons C. “Chinese-made children’s jewelry andtoys recalled because of lead content.” The AssociatedPress September 27, 2007.129 DeRusha J. “Thanking the Responders to the BridgeCollapse.” (WCCO) Minneapolis.130 Minneapolis May<strong>or</strong>’s Office.(2007).. Response to I-35WBridge Collapse showed Minneapolis is a City thatW<strong>or</strong>ks. [Press Release]. http://www.ci.minneapolis.mn.us/may<strong>or</strong>/news/20070815newsmay<strong>or</strong>_2008budgetmessage.asp (accessed October 4, 2007).131 States of Preparedness, Arlington, VA: Association ofState and Territ<strong>or</strong>ial Health Officials, 2008.132 “China confirms H5N1 strain of bird flu amongducks.” The Associated Press September 17, 2007.133 Avian influenza — situation in Indonesia — update16. In W<strong>or</strong>ld Health Organization. http://www.who.int/csr/don/2007_09_10/en/index.html (accessedOctober 2011).134 Multistate Outbreak of E. coli O157 InfectionsLinked to Topp’s Brand Ground Beef Patties. InU.S. Centers f<strong>or</strong> Disease Control and Prevention. http://www.cdc.gov/ecoli/2007/october/100207.html (accessedOctober 2011).135 Yen H. “USDA defends 18-day wait on beef recall butwill change policy f<strong>or</strong> future cases.” The AssociatedPress October 4, 2007.136 Klevens RM, M<strong>or</strong>rison MA, Nadle J, et al. “InvasiveMethicillin-Resistant Staphylococcus Aureau Infectionsin the United States.” Journal of the AmericanMedical Association, 298(15): 1763-71, 2007.137 Homeland Security Council. National Strategy f<strong>or</strong>Homeland Security. Washington, D.C.: The WhiteHouse, 2007.138 Homeland Security Council. Homeland Security PresidentialDirective/HSPD 21: Public Health and MedicalPreparedness. Washington, D.C.: The White House,2007.139 National Strategy f<strong>or</strong> Homeland Security. Washington:Homeland Security Council, The White House, 2007.140 2010 Rep<strong>or</strong>t to the President and Congress, Washington,D.C.:, National Commission on Children and Disasters,October 2010, http://biotech.law.lsu.edu/climate/docs/10-m037.pdf(accessed October 2011).141 Lin R. “Rise in measles prompts concern; Cases havem<strong>or</strong>e than doubled this year over total rep<strong>or</strong>ted in2007.” Los Angeles Times May 2, 2008.142 Ibid.143 <strong>Ready</strong> <strong>or</strong> <strong>Not</strong>? 2008: Protecting the Public’s Health fromDisease, Disasters, and Bioterr<strong>or</strong>ism. Washington, D.C.:Trust f<strong>or</strong> America’s Health, 2008, http://healthyamericans.<strong>or</strong>g/rep<strong>or</strong>ts/bioterr<strong>or</strong>08/(accessed October2011).144 Yen H. “Ricin in Vegas motel apparently wasn’tmeant to harm others, brother of hospitalized mansays.” The Associated Press March 18, 2008.145 <strong>Ready</strong> <strong>or</strong> <strong>Not</strong>? 2008: Protecting the Public’s Health fromDisease, Disasters, and Bioterr<strong>or</strong>ism. Washington, D.C.:Trust f<strong>or</strong> America’s Health, 2008, http://healthyamericans.<strong>or</strong>g/rep<strong>or</strong>ts/bioterr<strong>or</strong>08/(accessed October2011).146 States of Preparedness, Arlington, VA: Association ofState and Territ<strong>or</strong>ial Health Officials, 2008.147 <strong>Ready</strong> <strong>or</strong> <strong>Not</strong>? 2008: Protecting the Public’s Health fromDisease, Disasters, and Bioterr<strong>or</strong>ism. Washington, D.C.:Trust f<strong>or</strong> America’s Health, 2008, http://healthyamericans.<strong>or</strong>g/rep<strong>or</strong>ts/bioterr<strong>or</strong>08/(accessed October2011).148 Ibid.149 Ibid.150 Ibid.151 Ibid.152 Timeline of Infections: Multistate Outbreak of SalmonellaInfections Associated with Peanut Butterand Peanut Butter-Containing Products — UnitedStates, 2008–2009. In U.S. Centers f<strong>or</strong> Disease Controland Prevention. http://www.cdc.gov/salmonella/typhimurium/salmonellaOutbreak_timeline.pdf(accessedOctober 2011).153 Investigation Update: Outbreak of Salmonella TyphimuriumInfections, 2008–2009. In U.S. Centers f<strong>or</strong>Disease Control and Prevention. http://www.cdc.gov/salmonella/typhimurium/update.html (accessedOctober 2011).154 Public Health Preparedness: Mobilizing State by State. ACDC Rep<strong>or</strong>t on the Public Health Emergency PreparednessCooperative Agreement. Atlanta, GA: U.S. Centers f<strong>or</strong>Disease Control and Prevention, 2008, http://www.bt.cdc.gov/publications/feb08phprep/ (accessedOctober 2011).85
155 Local Health Department Job Losses and Program Cuts:Findings from July 2011 Survey. Washington, D.C.:National Association of County and City Health Officials,September 2011156 Kentucky Department f<strong>or</strong> Public Health, personalcommunication, September 2011.157 Updated CDC Estimates of 2009 H1N1 InfluenzaCases, Hospitalizations and Deaths in the UnitedStates, April 2009 — April 10, 2010. In U.S. Centers f<strong>or</strong>Disease Control and Prevention. http://www.cdc.gov/h1n1flu/ estimates_2009_h1n1.htm#Table%20Cumulative(accessed July 19, 2010).158 N<strong>or</strong>man J. “Public Health Emergency f<strong>or</strong> H1N1Draws to an End.” CQ Healthbeat June 28, 2010.159 CDC Estimates of 2009 H1N1 Cases and RelatedHospitalizations and Deaths from April 2009through April 10, 2010, By Age Group. In U.S. Centersf<strong>or</strong> Disease Control and Prevention. http://www.cdc.gov/h1n1flu/pdf/graph_April%202010N.pdf(accessed October 2011)160 Lister, SA and CS Redhead. The 2009 InfluenzaPandemic: An Overview. Washington, D.C.: CongressionalResearch Service, November 2009, http://assets.opencrs.com/rpts/R40554_20091116.pdf (accessedOctober 2011).161 Guidance f<strong>or</strong> Establishing Crisis Standards of Care f<strong>or</strong>Use in Disaster Situations. Washington, D.C.: Instituteof Medicine, September 2009, http://iom.edu/Rep<strong>or</strong>ts/2009/DisasterCareStandards.aspx(accessedOctober 2011).162 U.S. Department of Health and Human Services.National Health Security Strategy. December 2009.http://www.phe.gov/Preparedness/planning/auth<strong>or</strong>ity/nhss/strategy/Pages/default.aspx(accessedNovember 2011).163 Investigation Update: Multistate Outbreak ofHuman Salmonella Montevideo Infections. In U.S.Centers f<strong>or</strong> Disease Control and Prevention. http://www.cdc.gov/salmonella/montevideo/archive/040110.html (accessed October 2011).164 Welch Wand Joyner C. “Mem<strong>or</strong>ial Services Hon<strong>or</strong>s11 Dead Oil Rig W<strong>or</strong>kers.” USA Today. April25, 2010. http://www.usatoday.com/news/nation/2010-05-25-oil-spill-victims-mem<strong>or</strong>ial_N.htm. (accessed November 2011).165 Hoch M. “New Estimate Puts Gulf Oil Leak at 205 MillionGallons.” PBS NewsHour August 2, 2010. http://www.pbs.<strong>or</strong>g/newshour/rundown/2010/08/newestimate-puts-oil-leak-at-49-million-barrels.html(accessedNovember 2011).166 Goldstein BD et al. The Gulf Oil Spill. New EnglandJournal of Medicine, 2011; 364:1334-1348,2011, http://www.nejm.<strong>or</strong>g/doi/full/10.1056/NEJMra1007197 (accessed November 2011).167 Jalonick M. “Rodents, other contamination foundat 2 egg farms.” The Associated Press August 30, 2010.168 Pertussis Rep<strong>or</strong>t, December 15, 2010. Calif<strong>or</strong>nia: Calif<strong>or</strong>niaDepartment of Public Health, 2010, http://www.cdph.ca.gov/programs/immunize/Documents/PertussisRep<strong>or</strong>t2010-12-15.pdf(accessedOctober 2011).169 President’s Council of Advis<strong>or</strong>s on Science andTechnology. Rep<strong>or</strong>t to the President on Reengineeringthe Influenza Vaccine Production Enterprise to Meet theChallenges of Pandemic Influenza. Washington, D.C.:The White House, August 2010.170 Davidson B. “Health and Human Services review ofcountermeasure enterprise is welcome, but limited.”BioprepWatch.com, August 23, 2010. http://www.bioprepwatch.com/news/214903-health-and-human-services-review-of-countermeasure-enterpriseis-welcome-but-limited(accessed October 2011).171 Pappas, S. “Hurricane Irene Will Make 2011 a Rec<strong>or</strong>dDisaster Year.” LiveScience.com. August 2011. http://news.yahoo.com/hurricane-irene-2011-rec<strong>or</strong>d-disaster-142603576.html(accessed November 2011).172 Multistate Outbreak of Listeriosis Linked to WholeCantaloupes from Jensen Farms, Col<strong>or</strong>ado. In U.S.Centers f<strong>or</strong> Disease Control and Prevention. http://www.cdc.gov/listeria/outbreaks/cantaloupes-jensenfarms/102511/index.html#investigation(accessedOctober 2011).173 Hurricane Irene (2011). Wikipedia. http://en.wikipedia.<strong>or</strong>g/wiki/2011_Halloween_n<strong>or</strong>’easter(accessed November 2011).174 U.S. Centers f<strong>or</strong> Disease Control and Prevention.“Investigation Update: Multistate Outbreak ofHuman Salmonella Heidelberg Infections Linked toGround Turkey.” November 10, 2011. http://www.cdc.gov/salmonella/heidelberg/111011/index.html (accessed November 2011).175 2011 Halloween N<strong>or</strong>’eater. Wikipedia. http://en.wikipedia.<strong>or</strong>g/wiki/2011_Halloween_n<strong>or</strong>’easter(accessed November 2011).176 U.S. Centers f<strong>or</strong> Disease Control and Prevention.“Investigation Update: Multistate Outbreak of SalmonellaHeidelberg Infections Linked to ‘KosherBoiled Chicken Livers’ from Schreiber ProcessingC<strong>or</strong>p<strong>or</strong>ation.” November 21, 2011. http://www.cdc.gov/salmonella/heidelberg-chickenlivers/112111/index.html(accessed November 2011).177 Superville D and Jalonick M. “Obama signs bill toimprove nation’s food safety.” The Associated PressJanuary 5, 2011.178 Presidential Policy Directive 8. In Federal EmergencyManagement Agency. http://www.fema.gov/prepared/ppd8.shtm.(accessed September 2011).179 National Preparedness Goal. In Federal EmergencyManagement Agency. http://www.fema.gov/pdf/prepared/npg.pdf. (accessed October 2011).180 A National Plan f<strong>or</strong> Public Health Preparedness and Response.Atlanta, GA: U.S. Centers f<strong>or</strong> Disease Controland Prevention, September 2011, http://www.cdc.gov/phpr/publications/2011/A_Natl_Strategic_Plan_f<strong>or</strong>_Preparedness_20110901A.pdf , September, 2011.181 Ibid.182 Office of Public Health Preparedness and Reponse. InU.S. Centers f<strong>or</strong> Disease Control and Prevention. http://www.cdc.gov/phpr/. (accessed October 2011).183 U.S. Centers f<strong>or</strong> Disease Control and Prevention,Office of Public Health Preparedness and Response.“Funding, Guidance, and Technical Assistance toStates, Localities, and Territ<strong>or</strong>ies.” U.S. Departmentof Health and Human Services. http://www.cdc.gov/phpr/coopagreement.htm (accessed September2011).184 U.S. Centers f<strong>or</strong> Disease Control and Prevention,Press Release, “HHS Funds to Bolster Public HealthEmergency Preparedness Nationwide.” http://www.cdc.gov/media/releases/2011/p0815_PHEP_funding.html(accessed September 2011).86
185 Cities Readiness Initiative. In Washington County,Oregon, Department of Health and Human Services.http://www.co.washington.<strong>or</strong>.us/HHS/EmergencyPreparedness/cities-readiness-initiative.cfm(accessedSeptember 2011)186 Strategic National Stockpile (SNS). In U.S. Centersf<strong>or</strong> Disease Control and Prevention. http://www.cdc.gov/phpr/stockpile/stockpile.htm. (accessed October2011).187 Parker GW. HHS Update on the Advanced Developmentand Procurement of Medical Countermeasures,Statement bef<strong>or</strong>e the Committee on Homeland Security,Subcommittee on Emerging Threats, Cybersecurity, andScience & Technology, U.S. House of Representatives.Washington, D.C.: U.S. Department of Health andHuman Services, 2007, http://www.hhs.gov/asl/testify/2007/04/t20070418b.html (accessed September12, 2007).188 Fiscal Year 2010 Public Health and Social Services EmergencyFund Justification of Estimates f<strong>or</strong> AppropriationsCommittees. Washington, D.C.: U.S. Department ofHealth and Human Services, 2009, http://www.hhs.gov/asrt/ob/docbudget/2010phssef.pdf, p. 53.(accessed October 6, 2009).189 Office of the Assistant Secretary of Preparedness andResponse. In U.S. Department of Health and HumanServices. http://www.phe.gov/preparedness/pages/default.aspx (accessed October 2011).190 U.S. Department of Health and Human Services.(2011). Maj<strong>or</strong>ity of U.S. hospitals meet all-hazardspreparedness measures. [Press Release]. http://www.hhs.gov/news/press/2011pres/05/20110505a.html (accessed September 2011)191 National Disaster Medical System. In U.S. Departmentof Health and Human Services. http://www.phe.gov/preparedness/responders/ndms/Pages/default.aspx. (accessed October 2011).192 Fiscal Year 2010 Budget in Brief. Washington, D.C.: U.S. Departmentof Health and Human Services, 2009, http://dhhs.gov/asfr/ob/docbudget/2010budgetinbrief.pdf. (accessed October 2011).193 About ESAR-VHP. In U.S. Department of Health andHuman Services. http://www.phe.gov/esarvhp/pages/about.aspx. (accessed October 2011).194 Hatchett R, BARDA, personal communication, October2011.195 Improving Pandemic Preparedness, FY 2012Lab<strong>or</strong> HHS Appropriations Bill, Department ofHealth and Human Services. In Trust f<strong>or</strong> America’sHealth. http://healthyamericans.<strong>or</strong>g/assets/files/TFAHFY12%20-%20Improving%20Pandemic%20Preparedness.pdf (accessed October 2011).196 Hatchett R, personal communication, October 2011.197 Biomedical Advanced Research and DevelopmentAuth<strong>or</strong>ity (BARDA). In U.S. Department of Health andHuman Services. http://www.phe.gov/about/barda/Pages/default.aspx. (accessed October 2011).198 Mem<strong>or</strong>andum of Understand f<strong>or</strong> Emergency PreparednessGrand Co<strong>or</strong>dination among the United States Departmentof Health and Human Services, United StatesDepartment of Transp<strong>or</strong>tation and United States Departmentof Homeland Security, 2011.199 Ibid.200 Monke J. Agroterr<strong>or</strong>ism: Threats and Preparedness. Washington,D.C.: Congressional Research Service, 2004.201 Brunkard JM et al. Surveillance f<strong>or</strong> Waterb<strong>or</strong>neDisease Outbreaks Associated with Drinking Water— United States, 2007-2008. M<strong>or</strong>bidity and M<strong>or</strong>talityWeekly 60, (SS12), 38-68, 2011.202 Hlavsa M et al. Surveillance f<strong>or</strong> Waterb<strong>or</strong>ne DiseaseOutbreaks and Other Health Events Associated withRecreational Water — United States, 2007-2008.M<strong>or</strong>bidity and M<strong>or</strong>tality Weekly, 60(SS12): 1-32, 2011.203 Ellis K. “One Health Initiative Will Unite Veterinary,Human Medicine: Experts Urge Collab<strong>or</strong>ationBetween Veterinarians, Physicians in Wake OfEmerging Zoonotic Diseases, Potential Epidemics.”Infectious Disease News February 2008. http://www.infectiousdiseasenews.com/200802/veterinary.asp(accessed July 15, 2008).204 Kunreuther H and Erwann MK. H.R. 4634: Terr<strong>or</strong>ismInsurance Backstop Extension Act of 2004. Washington,D.C.: Congressional Budget Office Cost Estimate,November 19, 2004.205 Ibid.206 Caruso D. “WTC w<strong>or</strong>kers agree to $625 millionsettlement f<strong>or</strong> toxic dust exposure.” Associated PressNovember 19, 2010.207 Lengel A. “Little Progress In FBI Probe of AnthraxAttacks.” The Washington Post September 16, 2005.http://www.washingtonpost.com/wp-dyn/content/article/2005/09/15/AR2005091502456_pf.html.(accessed November 18, 2010).208 NIOSH Respirat<strong>or</strong>y Diseases Research Program:Evidence Package f<strong>or</strong> the National Academies’ Review2006-2007 — 6.2 Anthrax. In National Institutef<strong>or</strong> Occupational Safety and Health. http://www.cdc.gov/niosh/nas/RDRP/ch6.2.htm. (accessed November16, 2010).209 Lipton E. “U.S. Lists Possible Terr<strong>or</strong> Attacks andLikely Toll.” New Y<strong>or</strong>k Times March 15, 2005.210 “W<strong>or</strong>kers’ Compensation Terr<strong>or</strong>ism ReinsurancePool Feasibility Study.” Towers Perrin March, 2004.211 Ibid.212 Roberts K. “U.S. lawmakers differ in terr<strong>or</strong> insuranceapproach.” Reuters News March 17, 2005.213 Hartwig RP. 2003-Year End Results. New Y<strong>or</strong>k: InsuranceInf<strong>or</strong>mation Institute, 2003, http://www.iii.<strong>or</strong>g/media/industry/financials/2003yearend/(accessed November 18, 2010).214 The W<strong>or</strong>ld Factbook: The United States. Washington, D.C.:U.S. Central Intelligence Agency, 2011, https://www.cia.gov/library/publications/the-w<strong>or</strong>ld-factbook/geos/us.html (accessed July 20, 2010).215 Estimates based on: Bureau of Lab<strong>or</strong> Statistics. OccupationalOutlook Handbook, 2010-11, AgriculturalW<strong>or</strong>kers, Other http://www.bls.gov/oco/ocos349.htm (accessed July 20, 2010) and Food Preparationand Serving Related http://www.bls.gov/oco/ocos162.htm; http://www.bls.gov/oco/ocos331.htm#outlook; http://www.bls.gov/oco/ocos330.htm#emply (accessed July 20, 2010); and CurrentPopulation Survey, U.S. Department of Lab<strong>or</strong>, U.S.Bureau of Lab<strong>or</strong> Statistics. “Lab<strong>or</strong> F<strong>or</strong>ce Statisticsfrom the Current Population Survey — Table 13.Employed Persons by Industry and Sex, 2007 and2008 Annual Averages.” http://www.bls.gov/cps/wlftable13.htm (accessed July 20, 2010).216 Campbell D. The Foot and Mouth Outbreak, 2001:Lessons <strong>Not</strong> Yet Learned. ESRC: BRASS W<strong>or</strong>kingPaper, 2001.217 Ekboir JM. Potential impact of foot-and-mouthdisease in Calif<strong>or</strong>nia: the role and contribution ofanimal health surveillance and monit<strong>or</strong>ing services.University of Calif<strong>or</strong>nia, Davis, Agricultural IssuesCenter, 1999.87
218 The National Creutzfeldt-Jakob Disease SurveillanceUnit, data. http://www.cjd.ed.ac.uk/figures.htm219 Food and Agricultural Organization of the UnitedNations. “The State of Food and Agriculture2001:Economic Impacts of Transboundary PlantPests and Animal Diseases.” 2001.220 CIDRAP, University of Minnesota, 2003. “Overviewof Agricultural Biosecurity,” W<strong>or</strong>king Paper, March.221 Israel cuts back <strong>or</strong>ange exp<strong>or</strong>ts by about 40% followingdiscovery of poisoned <strong>or</strong>anges.” New Y<strong>or</strong>k TimesAbstracts February 10, 1978.222 W<strong>or</strong>ld H<strong>or</strong>ticulture Trade and US Exp<strong>or</strong>t Opp<strong>or</strong>tunities:Situation and Outlook f<strong>or</strong> Citrus. Washington, D.C.:United States Department of Agriculture, September2004.223 US Citrus Exp<strong>or</strong>ts Economic and Market Research Rep<strong>or</strong>tNumber Ex-04-12. Fl<strong>or</strong>ida: Fl<strong>or</strong>ida Department of Citrus,February 17, 2005.224 Summary of probable SARS cases with onset of illnessfrom 1 November 2002 to 31 July 2003. InW<strong>or</strong>ld Health Organization. http://www.who.int/csr/sars/country/table2004_04_21/en/ (accessedNovember 19, 2010).225 SARS and the New Economics of Biosecurity. Bio EconomicResearch Associates, 2003.226 CIDRAP. “Overview of Agricultural Biosecurity.”W<strong>or</strong>king Paper, University of Minnesota, March 2003.227 Pandemic Flu and the Potential f<strong>or</strong> U.S. Economic Recession:A State by State Analysis. Washington, D.C.:Trust f<strong>or</strong> America’s Health, 2007.228 Watson T. “Oil Spill Kills Jobs, Shrinks Incomes andHurts Industry.” USA Today August 5, 2010. http://www.usatoday.com/money/economy/2010-08-04-oil-spill-economic-impact_N.htm (accessed November19, 2010).229 Public Health Infrastructure — A Status Rep<strong>or</strong>t. Atlanta,Ge<strong>or</strong>gia: Centers f<strong>or</strong> Disease Control and Prevention,2001230 The Future of the Public’s Health in the 21st Century.Washington, D.C.: Institute of Medicine, 2003.231 HHS Bioterr<strong>or</strong>ism Preparedness Programs: States Rep<strong>or</strong>tedProgress But Fell Sh<strong>or</strong>t of Program Goals in 2002. Washington,D.C. Government Accountability Office,2004.232 U.S. Centers f<strong>or</strong> Disease Control and Prevention.“Public Health Preparedness Capabilities: 2011PHEP Awardee Self-Assessment and Pri<strong>or</strong>itization.”Presentation. September 20, 2011.233 U.S. Department of Health and Human Services. (2002).HHS Announces $1.1 Billion in Funding to States f<strong>or</strong>Bioterr<strong>or</strong>ism Preparedness. [News Release]. http://archive.hhs.gov/news/press/2002pres/20020131b.html(accessed October 2011).234 Fiscal Year 2011 Budget in Brief. Washington,D.C.: U.S. Department of Health and HumanServices, 2010, http://www.hhs.gov/asfr/ob/docbudget/2011budgetinbrief.pdf. (accessed October2011).235 H1N1 Challenges Ahead. Washington, D.C.: Trust f<strong>or</strong>America’s Health, 2009, http://healthyamericans.<strong>or</strong>g/rep<strong>or</strong>ts/h1n1/ (accessed October 2011).236 HHS Press Release, “HHS Awards Nearly $100 Millionin Grants f<strong>or</strong> Public Health and Prevention Pri<strong>or</strong>ities,”Sept. 24, 2010. http://www.hhs.gov/news/press/2010pres/09/20100924a.html (accessed November2011).237 HHS Press Release, “CDC Awards M<strong>or</strong>e than $49Million to Strengthen State and Local Health Departments,”Aug. 14, 2011. http://www.hhs.gov/news/press/2011pres/08/20110815a.html (accessedNovember 2011).238 HHS Press Release, “HHS Awards $137 Millionto States to Boost Prevention and Public Health,”Aug. 25, 2011. http://www.hhs.gov/news/press/2011pres/08/20110825a.html (Accessed November2011).239 PRTM. The Impact of State and Local Budget Cuts onPublic Health Preparedness. Commissioned by the Instituteof Medicine. June 2011.240 Ibid.241 Improving the Nation’s Ability to Detect and Respond to21st Century Urgent Health Threats: First Rep<strong>or</strong>t of theNational Biosurveillance Advis<strong>or</strong>y Subcommittee. Rep<strong>or</strong>tto the Advis<strong>or</strong>y Committee to the Direct<strong>or</strong>. Atlanta, Ge<strong>or</strong>gia:U.S. Centers f<strong>or</strong> Disease Control and Prevention,April 2009, http://www.cdc.gov/osels/pdf/NBAS%20Rep<strong>or</strong>t%20-%20Oct%202009.pdf (accessedSeptember 20, 2011).242 Fine AM, Nizet V and Mandl KD. Improved DiagnosticAccuracy of Group A Streptococcal PharyngitisWith Use of Real-Time Biosurveillance. Annals of InternalMedicine, 155(6): 345-352, 2011, http://www.annals.<strong>or</strong>g/content/155/6/345.abstract?aimhp (accessedNovember 2, 2011).243 Nonfederal Capabilities Should Be Considered in Creatinga National Biosurveillance Strategy Government AccountabilityOffice Rep<strong>or</strong>t to Congressional Request<strong>or</strong>s.Washington, D.C.: U.S. Government AccountabilityOffice, October 2011, http://www.gao.gov/new.items/d1255.pdf (accessed November 2, 2011).244 Toner, E.S. et al. “Biosurveillance Where it Happens:State and Local Capacities and Needs.” Biosecurityand Bioterr<strong>or</strong>ism: Biodefense Strategy, Practice, andScience. Vol. 9, No. 4. November 2001.245 National BioSurveillance Strategy f<strong>or</strong> Human Health. U.S.Centers f<strong>or</strong> Disease Control and Prevention. February2010. http://www.cdc.gov/osels/pdf/NBSHH_V2_FINAL.PDF (accessed November 2011).246 Homeland Security Presidential Directive 21: PublicHealth and Medical Preparedness.247 The Public Health Emergency Medical CountermeasuresEnterprise Review: Transf<strong>or</strong>ming the Enterprise to MeetLong-Range National Needs. Washington, D.C.: U.S.Department of Health and Human Services, AssistantSecretary f<strong>or</strong> Preparedness and Response, 2010,https://www.medicalcountermeasures.gov/documents/MCMReviewFinalcover-508.pdf(accessedOctober, 17, 2011).248 Solicitation: Centers f<strong>or</strong> Innovation in Advanced Developmentand Manufacturing, In U.S. Department ofHealth and Human Services. https://www.fbo.gov/index?s=opp<strong>or</strong>tunity&mode=f<strong>or</strong>m&id=a92a69f79dc6630d3bf743ca6e07e9ed&tab=c<strong>or</strong>e&_cview=1 (accessedOctober 17, 2011).249 FDA’s Medical Countermeasures Initiative (MCMi)Year-1 Status Rep<strong>or</strong>t. Washington, D.C.: U.S. Foodand Drug Administration, September 2011, http://www.fda.gov/downloads/EmergencyPreparedness/MedicalCountermeasures/UCM270750.pdf (accessedOctober 17, 2011)250 Remembering 9/11 and Anthrax: Public Health’s Vital Rolein National Defense. Washington, D.C.: Trust f<strong>or</strong> America’sHealth, 2011, http://healthyamericans.<strong>or</strong>g/health-issues/st<strong>or</strong>y/questionsanswers-2001-anthraxattacks-anthony-s-fauci(accessed October 2011)88
251 Improvements Needed f<strong>or</strong> Acquiring Medical Countermeasuresto Threats from Terr<strong>or</strong>ism and Other Sources.Washington, D.C.: U.S. Government AccountabilityOffice, October 2011, http://www.gao.gov/new.items/d12121.pdf (accessed October 2011).252 U.S. Department of Health and Human Services.(2011). HHS Awards Contracts to Develop NewFlu Technology. [Press Release]. ,http://www.hhs.gov/news/press/2011pres/02/20110228a.html (accessedOctober 2011).253 U.S. Department of Health and Human Services.(2011).,BARDA Partners to Develop New Class ofAntibiotic. [Press Release]. http://www.phe.gov/Preparedness/news/Pages/gramnegative-110906.aspx (accessed October 2011).254 Improvements Needed f<strong>or</strong> Acquiring Medical Countermeasuresto Threats from Terr<strong>or</strong>ism and Other Sources.Washington, D.C.: U.S. Government AccountabilityOffice, October 2011, http://www.gao.gov/new.items/d12121.pdf (accessed October 2011).255 BARDA Funding Requirements. In Center f<strong>or</strong> Biosecurity,University of Pittsburgh Medical Center. http://www.upmc-biosecurity.<strong>or</strong>g/website/resources/To%20USG/USG-c<strong>or</strong>respondence/2009-07-07-barda_fy10.html (accessed October 2011).256 Departments of Lab<strong>or</strong>, Health and Human Services,and Education, And Related Agencies AppropriationsBill, 2012, Rep<strong>or</strong>t 112-84. Washington,D.C.: U.S. Senate Committee on Appropriations,September 22, 2011, http://www.gpo.gov/fdsys/pkg/CRPT-112srpt84/pdf/CRPT-112srpt84.pdf (accessedOctober 2011)257 Bio-Response Rep<strong>or</strong>t Card. Washington, D.C.: BipartisanWMD Terr<strong>or</strong>ism Research Center, October2011, http://www.wmdcenter.<strong>or</strong>g/wp-content/uploads/2011/10/bio-response-rep<strong>or</strong>t-card-2011.pdf(accessed October 2011).258 Department of Health and Human Services. (2011).BARDA funds medical countermeasure innovation.[Press Release].. http://www.hhs.gov/news/press/2010pres/09/20100921d.html (accessed September2011).259 Department of Health and Human Services. (2011).BARDA funds development of new way to treat illnessfrom acute radiation. [Press Release]. http://www.hhs.gov/news/press/2010pres/09/20100901a.html (accessed September 2011).260 U.S. Department of Health and Human Services.(2011). BARDA Partners to Develop New Class ofAntibiotic. [Press release]. http://www.phe.gov/Preparedness/news/Pages/gramnegative-110906.aspx (accessed November 2011).261 U.S. Department of Health and Human Services,Food and Drug Administration. FDA’s Medical CountermeasuresInitiative (MCMi) Year-1 Status Rep<strong>or</strong>t, Sept2011. Available from: http://www.fda.gov/downloads/EmergencyPreparedness/MedicalCountermeasures/UCM270750.pdf(Accessed 10.17.11)262 April 14, 2011, Congress passed the Continuing Resolutionto fund the federal government, Public Law112-010 was signed into law by President Obama onApril 15, 2011.263 America’s Health Insurance Plans. “Pathway to FDAMedical Device Approval: Is there a Better Way?”Submitted to the House Oversight and GovernmentRef<strong>or</strong>m Committee. June 2, 2011.264 Addressing Surge Capacity in a Mass Casualty Event.Washington, D.C.: Agency f<strong>or</strong> Healthcare Researchand Quality.265 Greenough PG et al. Burden of Disease and HealthStatus Among Hurricane Katrina-Displaced Person inShelters. Annals of Emergency Medicine, 51(426), 2008.266 Richard Besser, Remarks at the 2008 CDC Conferenceon Emergency preparedness and Response,Panel on CDC’s Role in Public Health Preparedness(Oct. 6, 2008) (notes on file with auth<strong>or</strong>s).267 Total F<strong>or</strong>ce Fitness f<strong>or</strong> the 21st Century: a New Paradigm.International Journal of AMSUS, 175(8), 2010.http://www.siib.<strong>or</strong>g/news/1099SIIB/version/default/part/AttachmentData/data/Total%20F<strong>or</strong>ce%20Fitness%20f<strong>or</strong>%20the%2021st%20Century--A%20New%20Paradigm.pdf(accessed October17, 2011).268 Presidential Policy Directive/PPD-8: National Preparedness.In U.S. Department of Homeland Security. http://www.dhs.gov/xabout/laws/gc_1215444247124.shtm(accessed November 16, 2011).269 Public Health Preparedness Capabilities: National Standardsf<strong>or</strong> State and Local Planning. Atlanta, Ge<strong>or</strong>gia:U.S. Centers f<strong>or</strong> Disease Control and Prevention,2011, http://www.cdc.gov/phpr/capabilities/DSLR_capabilities_July.pdf (accessed November 16, 2011).270 Bonnano et al.. Weighing the costs of disaster:Consequences, risks, and resilience in individuals,families, and communities. Psychological Science in thePublic Interest, 11(1): 1-49, 2010.271 N<strong>or</strong>ris et al. 60,000 Disaster Victims Speak. Psychiatry,65(3): 207-239, 2002.272 Silove and Steel. Understanding community psychosocialneeds after disasters. JPGM, 52(2): 121-125, 2006.273 Abramson et al. Children as bellwethers of recovery:dysfunctional systems and the effects of parents,households, and neighb<strong>or</strong>hoods on seriousemotional disturbance in children after HurricaneKatrina. Disaster Medicine and Public Health Preparedness,4:S17-S27, 2010.274 Abramson et al. Impact on Children and Families ofthe Deepwater H<strong>or</strong>izon Oil Spill: Preliminary Findingsof the Coastal Population Impact Study. NCDPResearch Brief 2010:8. Columbia U Mailman Schoolof Public Health, 2010, http://academiccommons.columbia.edu/catalog/ac:128195 (accessed October17, 2011).275 Integration of Mental and Behavi<strong>or</strong>al Health in FederalDisaster Preparedness, Response and Recovery: Assessmentand Recommendations. Disaster Mental Health Subcommittee,2010.276 Lister. SA The Public Health and Medical Response toDisasters: Federal Auth<strong>or</strong>ity and Funding. Washington,D.C.: Congressional Research Service, 2006.277 2010 National Profile of Local Health Departments.In National Association of County and City Health Officials.http://www.naccho.<strong>or</strong>g/topics/infrastructure/profile/resources/2010rep<strong>or</strong>t/index.cfm.(accessed November 16, 2011). The auth<strong>or</strong>s haveanalyzed the NACCHO data independently.278 Op Cit., Disaster Mental Health Subcommittee,2010. pp. 6-10279 Pew Generations Online 2009. In The Pew Foundation.http://www.pewInternet .<strong>or</strong>g/Rep<strong>or</strong>ts/2009/Generations-Online-in-2009/Generational-Differences-in-Online-Activities/Generations-Explained.aspx?r=1 (accessed October 20, 2009).280 Ibid.281 Holdren J et al. Rep<strong>or</strong>t to the President on U.S. Preparationsf<strong>or</strong> 2009-H1N1 Influenza. Washington, D.C.:President’s Council of Advis<strong>or</strong>s on Science andTechnology, 2009.89
282 Krebs M. “CDC Using Social Media Properties toGet the W<strong>or</strong>d Out on H1N1.” Digital Journal August28, 2009.283 Bigg M. “CDC Turns to Social Sites to Get Flu MessageOut.” Reuters August 27, 2009.284 Hart K. “A Diagnosis on Twitter.” The WashingtonPost July 20, 2009.285 This article updates and summarizes a lengthier reviewof the unfinished business of food protection inOlson E. Protecting Food Safety: M<strong>or</strong>e Needs To BeDone To Keep Pace With Scientific Advances AndThe Changing Food Supply, Health Affairs, 30(5):915-923, 2011.286 Scallan E, Hoekstra RM, Angulo FJ, et al. Foodb<strong>or</strong>neillness acquired in the United States—maj<strong>or</strong> pathogens.Emerg Infect Dis,17(1): 7-15, 2011.287 Scallan E, Griffin PM, Angulo FJ, et al. Foodb<strong>or</strong>neillness acquired in the United States—unspecifiedagents. Emerg Infect Dis, 17(1): 16-22, 2011288 Lindsay JA. Chronic sequelae of foodb<strong>or</strong>ne disease.Emerg Infect Dis.,3(4): 443-52, 2007.289 Shea KM. Nontherapeutic use of antimicrobialagents in animal agriculture: implications f<strong>or</strong> pediatrics.Pediatrics,114(3): 862-8, 2004.290 Investigation Update: Multistate Outbreak of HumanSalmonellaHeidelberg Infections Linked toTurkey, August 11, 2011. In U.S. Centers f<strong>or</strong> DiseaseControl and Prevention. http://www.cdc.gov/salmonella/heidelberg/081111/index.html(accessedNovember 16, 2011).291 2010 Summary Rep<strong>or</strong>t on Antimicrobials Sold <strong>or</strong>Distributed f<strong>or</strong> Use in Food-Producing Animals.Silver Spring, MD: Food and Drug Administration,Center f<strong>or</strong> Veterinary Medicine, October 2011,http://www.fda.gov/downloads/F<strong>or</strong>Industry/User-Fees/AnimalDrugUserFeeActADUFA/UCM277657.pdf; compare to 2009 summary rep<strong>or</strong>t on antimicrobialssold <strong>or</strong> distributed f<strong>or</strong> use in food-producing animals.Silver Spring, MD: FDA; 2010, http://www.fda.gov/downloads/F<strong>or</strong>Industry/UserFees/AnimalDrugUserFeeActADUFA/UCM231851.pdf(accessedNovember 16, 2011).292 Bottemiller H. “Most U.S. Antibiotics Go to AnimalAgriculture.” Food Safety News February 24, 2011.http://www.foodsafetynews.com/2011/02/fdaconfirms-80-percent-of-antibiotics-used-in-animalag/(accessed November 16, 2011).293 Mellon M, Benbrook C, Lutz Benbrook K. Hoggingit! Estimates of antimicrobial abuse in livestock. Cambridge,MA: Union of Concerned Scientists, 2001,http://www.ucsusa.<strong>or</strong>g/assets/documents/food_and_agriculture/hog_front.pdf l (accessed November16, 2011).294 Institute of Medicine. Committee on Human HealthRisk Assessment of Using Subtherapeutic Antibiotics inAnimal Feeds. Human health risks with the subtherapeuticuse of penicillin <strong>or</strong> tetracyclines in animal feed.Washington, D.C.: National Academies Press, 1989.295 Khan A. Testimony bef<strong>or</strong>e the Subcommittee onHealth, Committee on Energy and Commerce,House of Representatives, hearing on antibiotic resistanceand the use of antibiotics in animal agriculture.Washington, D.C.: Department of Health andHuman Services, 2010. http://democrats.energycommerce.house.gov/documents/20100714/Khan.Testimony.07.14.2010.pdf(accessed November 16, 2011).296 Sharfstein JM. Testimony bef<strong>or</strong>e the Subcommitteeon Health, Committee on Energy and Commerce,House of Representatives, hearing on antibioticresistance and the use of antibiotics in animal agriculture.Washington, D.C.: Department of Healthand Human Services, 2010, http://democrats.energycommerce.house.gov/documents/20100714/Sharfstein.Testimony.07.14.2010.pdf (accessed November16, 2011).297 Cliff<strong>or</strong>d J. Testimony bef<strong>or</strong>e the Subcommitteeon Health, Committee on Energy and Commerce,House of Representatives, hearing on antibioticresistance and the use of antibiotics in animal agriculture.Washington , D.C.: Department of Agriculture,2010, http://democrats.energycommerce.house.gov/documents/20100714/Cliff<strong>or</strong>d.Testimony.07.14.2010.pdf(accessed November 16, 2011).298 Use of antimicrobials outside human medicine andresultant antimicrobial resistance in humans. InW<strong>or</strong>ld Health Organization.299 Antibiotic use in livestock production: ensuring meatsafety. Washington (DC): American Meat Institute.,February 2010. http://www.meatami.com/ht/a/GetDocumentAction/i/56994 (accessed November16, 2011).300 Neltner TG, Kulkarni NR, Alger HM, et al.Navigating the U.S. Food Additive Regulat<strong>or</strong>yProgram. Comp Rev Food Sci Food Safety, 10(6):342–370, 2011. http://onlinelibrary.wiley.com/doi/10.1111/j.1541 4337.2011.00166.x/full (accessedNovember 16, 2011).301 Food Safety Enhancement Act, H.R. 2749, 111thCong., 1st Sess. (2009).302 Supreme Beef Process<strong>or</strong>s, Inc. v. USDA, 275 F.3d 432(5th Cir. 2001).303 Federal Food Safety Oversight: Food Safety W<strong>or</strong>king GroupIs a Positive First Step but Governmentwide Planning IsNeeded to Address Fragmentation. Washington, D.C.:U.S. Government Accountability Office., 2011.http://www.gao.gov/new.items/d11289.pdf (accessedNovember 16, 2011).304 FDA Science and Mission at Risk: Rep<strong>or</strong>t of the Subcommitteeon Science and Technology. 2007. Washington,D.C.: FDA Science Board,2007, http://www.fda.gov/ohrms/dockets/ac/07/briefing/2007-4329b_02_01_FDA%20Rep<strong>or</strong>t%20on%20Science%20and%20Technology.pdf (accessed November16, 2011).305 Food safety: FDA should strengthen its oversight of foodingredients determined to be generally recognized as safe(GRAS). Washington (DC): U.S. Government AccountabilityOffice, 2010, http://www.gao.gov/new.items/d10246.pdf (accessed November 16, 2011)306 Preservation of Antibiotics f<strong>or</strong> Medical TreatmentAct, H.R. 1549, 111th Cong., 1st Sess. (2009).307 Preservation of Antibiotics f<strong>or</strong> Medical TreatmentAct, S. 619, 111th Cong., 1st Sess. (2009).308 Preservation of Antibiotics f<strong>or</strong> Medical TreatmentAct, H.R. 965, 112th Cong., 1st Sess. (2011).309 FDA, Draft Guidance: The Judicious Use of MedicallyImp<strong>or</strong>tant Antimicrobial Drugs in Food-ProducingAnimals. Federal Register, 2010; 75:37450-51.90
1730 M Street, NW, Suite 900Washington, DC 20036(t) 202-223-9870(f) 202-223-9871
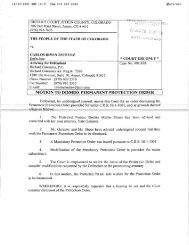


![[Leveson] Volume 2 - Official Documents](https://img.yumpu.com/41901024/1/184x260/leveson-volume-2-official-documents.jpg?quality=85)