TO ALL RPN EMPLOYERS - Registered Practical Nurses ...
TO ALL RPN EMPLOYERS - Registered Practical Nurses ...
TO ALL RPN EMPLOYERS - Registered Practical Nurses ...
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
<strong>TO</strong> <strong>ALL</strong> <strong>RPN</strong> <strong>EMPLOYERS</strong>:Please take the time to read this valuable information. With today’s everincreasing scope of practice and a public that is more knowledgeable, any nursecould face misconduct allegations.As an employer, please encourage your <strong>RPN</strong>s to continue investing in the manybenefits derived from membership in <strong>RPN</strong>AO.More employers are beginning to ask <strong>RPN</strong>s to belong to their association becauseit enhances their professionalism and protects their employees with the bestprofessional liability insurance, legal and criminal defense fund. All nurses needthis type of coverage, a simple complaint to CNO can cost potential financial loss,and most employers and/or unions do not cover this.As a member of <strong>RPN</strong>AO they will also receive the quarterly magazine The <strong>RPN</strong>Journal to keep them informed of the developments in nursing and specialdiscounted rates for workshops, seminars and conference to enhance their nursingknowledge and many more.If you need more information regarding <strong>RPN</strong>AO membership and payrolldeduction plan, please:• Visit: www.rpnao.org/membership.asp• Contact:Rocio Lock, CMPManager, Membership & AdministrationE-mail: rlock@rpnao.org
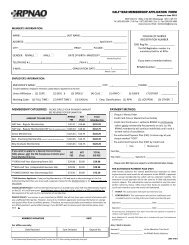
MEMBERSHIP - PAYROLL DEDUCTION PLANThe <strong>RPN</strong>AO membership year is July 1 st to June 30 th , and the payrolldeduction plan is made in the preceding year so the full amount is sent to<strong>RPN</strong>AO before the new membership starts every July 1 st .For example, they have monthly deductions in July 2012 to June 2013 andthe total membership of $256.39 payment must reach <strong>RPN</strong>AO before June15 th 2013, this is to ensure their membership benefits and professionalliability insurance coverage remains uninterrupted.<strong>RPN</strong>AO MEMBERSHIP FEE: JULY 2013 - JUNE 2014$226.89 + HST$ 29.50 <strong>TO</strong>TAL $ 256.39Please find enclosed the Membership Application Form for payrolldeduction participants. Employer must submit all completed membershipapplication forms to <strong>RPN</strong>AO with payment by June 15 th of the previousmembership year.Thank you for supporting the professional association for <strong>RPN</strong>s in Ontario.Regards,Rocio Lock, CMPMembership & AdministrationManager
Applicant’s Information:Last Name First Name CNO Registration No.
Last Name First Name CNO Registration No.Mail to:<strong>RPN</strong>AO - MembershipRocio Lock, CMPManager, Membership & Administration5025 Orbitor Drive, Building 4, Suite 200Mississauga, ON L4W 4Y5Or by e-mail: membership@rpnao.org
Payroll Deduction Plan2013-2014 Membership Year5025 Orbitor Drive, Bldg 4, Suite 200, Mississauga, ON L4W 4Y5Tel: (905)602-4664 - Toll Free #: 1(877)602-4664 - Fax: (905)602-4666E-mail: membership@rpnao.org website: www.rpnao.orgMEMBER’S INFORMATION:(Please feel free to make photocopies of this form if needed)NAME:________________________________ LAST NAME:_________________________________________________ADDRESS: _______________________________________________________________________ Apt/Unit #_________CITY: _____________________ PROV._____ P/CODE: _____________ TEL: (_________)_______________________FAX (_______)______________________ E-mail: ______________________________________________________Please print your fax number and/or e-mail clearly to receive important information from <strong>RPN</strong>AOGENDER: FEMALE MALE DATE OF BIRTH: MM/DD/YY ________________________TRAINING CENTRE: _________________________________________ YEAR OF GRADUATION: ________________COLLEGE OF NURSESREGISTRATION NUMBER:Reg No.:( if you do not submit your CNO #, we won’t beable to process your membership)<strong>RPN</strong>AO MEMBERSHIPNUMBER:__________________________EMPLOYER’S INFORMATION:EMPLOYER’S NAME: ________________________________________________________________ CITY: ________________________ PHONE:_____________________EMPLOYER’S NAME: ________________________________________________________________ CITY: ________________________ PHONE:_____________________UNION AFFILIATION: (1 )CUPE (2) SEIU 3 ) OPSEU (4) CLAC (5) PNFO (6) CAW (7) OTHER: _______________________WORKING CODE: (1) FULL-TIME (2) PART-TIME (3) CASUAL EMPLOYMENT CLASS: (1) <strong>RPN</strong> (2)UCP/PSW (3)OTHER: _____________MEMBERSHIP CATEGORY: (SELECT ONE )PAYMENT METHOD:Membership Payment Plans ANNUAL FEE AMOUNT PAIDRegular MembershipPayroll Deduction Plan $ 256.39Regular Membership1 payment (by cheque, $ 256.39visa, mastercard)Regular MembershpPre-authorized Payment Plan $ 269.94VOID cheque is required (19.91monthly + $31.06 HST)Pre-Authorized Payment Plan:I/We hereby authorize the named bank/financial institution to debit my/our accounteach month for all payments to the <strong>RPN</strong>AO in payment of my annual membership feewhich will be collected monthly. The treatment of each payment will be the sameas if I/We had personally issued a cheque. This authorization may be cancelled atany time upon written notice by me/us. I/We ensure that funds are available on the1st business day of each month to cover the amount of withdrawal. Please note,additional $1 monthly PAP Admin fee is included with your pre-authorized paymentplan. Cancellations prior to the <strong>RPN</strong>AO membership expiry date are subjectto a $35 cancellation fee.Continous: This authorization will continue indefinitelyuntil cancelled by me in writing.<strong>RPN</strong>AO Collects personal information for the purposes of verifying membership eligibility and type, malpractice insurance coverage and abilityto communicate assocition information (PIPEDA)PRIVATE POLICY: Your privacy is very important to <strong>RPN</strong>AO. We will not share your contact information with any unaffiliated third parties.However, many of our members appreciate receiving information on savings and special offers from our affinity partners. Therefore, we mayoccasionally send members information on our affinity partners' special offers/savings. If you DO NOT wish to receive such informationplease mark here.Member’s Signature:______________________________________FOR OFFICE USE ONLY:Date: ___________________Signature: ________________________ Date: __________Signature: _________________________Date: __________Note: For a joint account, all depositors must sign if more than onesignature is required on cheques issued against the accountFOR PRE-AUTHORIZED PAYMENT PLANPLEASE ENCLOSE A COPYOF YOUR CHEQUE MARKED “VOID”Date Received Sum Enclosed Deposit # Also, I wish to donate:Amount: $_________________ To the Education Trust FundAmount: $_________________For <strong>RPN</strong>AO Public Relations