Oklahoma Run Report 2002 - NHTSA
Oklahoma Run Report 2002 - NHTSA
Oklahoma Run Report 2002 - NHTSA

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
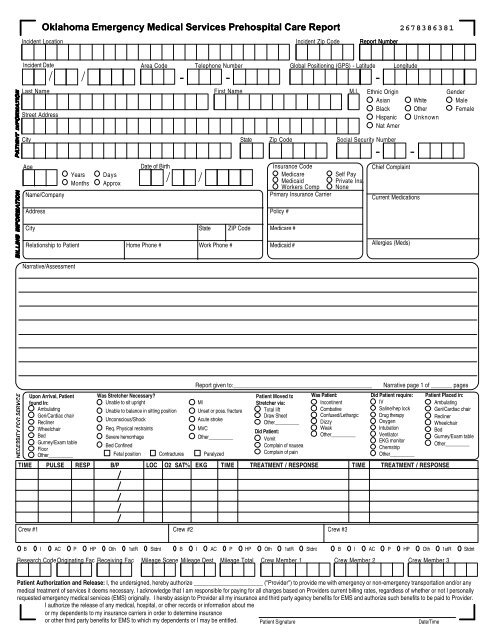
<strong>Oklahoma</strong> Emergency Medical Services Prehospital Care <strong>Report</strong>Incident LocationIncident Zip Code<strong>Report</strong> Number2678386381Incident Date/ /Area Code Telephone Number- -Last NameStreet AddressFirst NameCity State Zip CodeAgeName/CompanyYearsMonthsDaysApproxDate of Birth/ /Insurance CodeMedicareMedicaidGlobal Positioning (GPS) - LatitudeWorkers CompPrimary Insurance CarrierM.I.Ethnic OriginAsianBlackHispanicNat AmerSocial Security Number- -Self PayPrivate Ins.None-LongitudeChief ComplaintCurrent MedicationsWhiteOtherUnknownGenderMaleFemaleAddressCity State ZIP CodeRelationship to Patient Home Phone # Work Phone #Policy #Medicare #Medicaid #Allergies (Meds)Narrative/AssessmentUpon Arrival, Patientfound In:AmbulatingGeri/Cardiac chairReclinerWheelchairBedGurney/Exam tableFloorOther__________Was Stretcher Necessary?Unable to sit uprightUnable to balance in sitting positionUnconscious/ShockReq. Physical restraintsSevere hemorrhageBed ConfinedMIUnset or poss. fractureAcute strokeMVCOther__________Fetal position Contractures Paralyzed<strong>Report</strong> given to:______________________________________________Patient Moved toStretcher via:Total liftDraw SheetOther__________Did Patient:VomitComplain of nauseaComplain of painWas Patient:IncontinentCombativeConfused/LethargicDizzyWeakOther__________Narrative page 1 of _______ pagesDid Patient require:IVSaline/hep lockDrug therapyOxygenIntubationVentilatorEKG monitorChemstripOther__________TIME PULSE RESP B/P LOC O2 SAT% EKG TIME TREATMENT / RESPONSE TIME TREATMENT / RESPONSEPatient Placed in:AmbulatingGeri/Cardiac chairReclinerWheelchairBedGurney/Exam tableOther__________Crew #1 Crew #2 Crew #3B I AC P HP Oth 1stR Stdnt B I AC P HP Oth 1stR Stdnt B I AC P HP Oth 1stR StdntResearch CodeOriginating Fac Receiving Fac Mileage Scene Mileage Dest Mileage Total Crew Member 1 Crew Member 2 Crew Member 3Patient Authorization and Release: I, the undersigned, hereby authorize _______________________ ("Provider") to provide me with emergency or non-emergency transportation and/or anymedical treatment of services it deems necessary. I acknowledge that I am responsible for paying for all charges based on Providers current billing rates, regardless of whether or not I personallyrequested emergency medical services (EMS) originally. I hereby assign to Provider all my insurance and third party agency benefits for EMS and authorize such benefits to be paid to Provider.I authorize the release of any medical, hospital, or other records or information about meor my dependents to my insurance carriers in order to determine insuranceor other third party benefits for EMS to which my dependents or I may be entitled. Patient SignatureDate/Time
Call ReceivedInjury Site/TypeNoneHeadFaceEyeNeckChestBackAbdomenPelv/GenitUpper ExtLower Ext<strong>Oklahoma</strong> Emergency Medical Services Prehospital Care <strong>Report</strong>EnrouteArrive SceneDepart SceneArrive Dest.Return ServiceCalled ByPatient/FamilyBystanderFirePoliceNursing FacAcute Care FacUse Military TimeUsed 911YesNoBLS TREATMENTCM1 CM2 CM3AssessmentAirway AdjunctOxygenIV MonitorAbdom. ThrustBack blowsAuto-Defib.CPRWound MgmtCervical CollarBack BoardExtricationSplint ExtremitiesMASTOB DeliveryRestraintsSuctionVentilationGlucometerOther BLSProceduresIV-CentralIV-PeripheralDefibrillationIntubation1 2 3+ UPre-hospital Trauma MechanismAssaultExplosionATVFire/BurnBicycleMotorcycleBite/StingMVCEjectionOccupant (Death)ElectricalVehicle RolloverResponse ModeTo SceneEmergencyNon Emerg.In CityOutsideFrom SceneEmergencyNon Emerg.Response OutcomeTransportedCare TransferCancelledRefusedTreat, No Tran.False CallP.O.V.No Pt. FoundD.O.A.AssistanceNone BystanderResp Fire Police1stFirst AidAEDBLSALSALS TREATMENTCM1AssessmentCM2 CM3Blood DrawIV-CentralIV-Ext. JugularIV-IntraosseousIV-PeripheralCardiac MonitorCardioversionManual Defib.PacingPTLNasal Intub.Oral Intub.Drug Admin.CricothyrotomyNeedle Thorac.Glucometer12 LeadOther ALSIV Type/RateGAUGE TKO BOLUS OPEN OTHERD5WNSLROther# Lines 1 2 3 4Near/DrownPedestrianShootingSignificant FallStabbingOther TraumaPT ProtectionShoulder/Lap BeltShoulder BeltLap BeltAirbag (Deployed)Child Safety SeatHelmetPersonal Flotation DevNoneInfo Not AvailableUnknownType of CallPrehospitalThis is to certify that I am refusing treatment/transport. I have been informed ofthe risk(s) involved, and hereby release the ambulance service, its attendants,and its affiliates, from all responsibility which may result from this action.Pre-hospitalMedical IllnessTraumaSuspected Medical IllnessPrimary SecondaryMark 1 Mark All that applyAbdominal PainAirway ObstructionAllergic ReactionBehavioralBreathing DifficultyCardiac ArrestCardiac SymptomsChest PainCVADehydrationDizzinessGynecologicalHypertensionHypo/HyperglycemiaHypo/HyperthermiaNausea/VomitingObstetricalPainParalysisPoisoning/IngestionRespiratory ArrestSeizureShockUnconsciousWeaknessOtherAirwaySizePatentOral/NasalIntubationPatient SignatureTransfer TypeAdmission TransferDischarge (Hosp.)Inter Fac. (Hosp.)Additional InfoScheduledMedical HistoryAllergiesAsthmaBehavioralCancerCardiacCHFCOPDCVADiabetesDrug/ETOHEmphysemaHTNCom DiseaseRecent SurgeryRenal FailureSeizuresNon-PertinentOtherNoneAnatomical Trauma CriteriaPenetratingFlail chestBurns (>20%) FractureAmputationFracture SkullParalysisPelvisPT LocationDriverPass. FrontPass. Left RearPass. Right RearTruck BedOtherUnknownPupilsMedical ControlProtocolOn LineD.N.R.LeftNormalConstrictedDilatedNon-ReactiveStandbyTransfer-InterfacilityRSIPTLCricothyrotomyRightSpecial SituationMutual AidALS AssistMedical HistoryVerifiedSuctionVentilationOxygenRescue/ExtricationYesNoTotal Extrication TimeSkinWarmCoolDryMoistCyanoticEKGI LDiaphoreticPalePink<strong>Report</strong> NumberIncident LocationResidenceHighwayOther Traffic WayWaterOffice/BusinessEducation FacilityFarm/RanchPublic AreaNursing FacilityClinic/Dr OfficeHospitalOtherWas Incident Work-Related? Y NPEANSRSin. Tach.Sin. BradyAsystoleAV BlockAtrial Fib.Atrial Flut.Vent. Tach.Vent. Fib.SV Tach.Pace RhythmPVC'sMedication Treatment CategoryAllergic ReactionBradycardiaChest PainCardiac ArrestDysrhythmiaHypotensionOverdosePain ControlSeizuresThrombolyticsWitnessed Arrest?Pulse Restored?ByStander CPRPossible Contributing FactorAlcoholSubstanceExtrication >15 min.Self-InflictionPatient abusedEquipmentGlasgow Coma ScaleEyesVerbal4 Spontan. 5 Oriented3 To Speech 4 Confused2 To Pain 3 Inapp.1 None 2 GarbledScore______ 1 NonePediatric Trauma ScoreWeight>20 kg (+2)10-20 kg (+1)90 (+2)90-50 (+1)