National End of Life Care Strategy - Merseyside & Cheshire Cancer ...
National End of Life Care Strategy - Merseyside & Cheshire Cancer ...
National End of Life Care Strategy - Merseyside & Cheshire Cancer ...
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
Welcome toThe Annual Joint ConferenceThe <strong>Merseyside</strong> and <strong>Cheshire</strong> <strong>Cancer</strong> Network<strong>End</strong> <strong>of</strong> <strong>Life</strong> and Palliative <strong>Care</strong> CNGandThe <strong>National</strong> Council for Palliative <strong>Care</strong>Thursday 7th July 2011
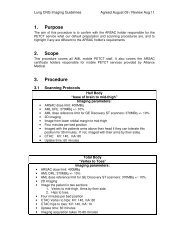
<strong>National</strong> <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> <strong>Strategy</strong>Pre pathwayStep 1Step 2Step 3Step 4Step 5 & 6RaisingAwarenessDiscussionsas the end<strong>of</strong> lifeapproachesAssessment,care planningand reviewCoordination<strong>of</strong> careDelivery <strong>of</strong>high qualityservices indifferentsettings<strong>Care</strong> in thelast days<strong>of</strong> life andcare after deathMeasurement - Intelligence network ,quality markers , VOICESSpirituality, User involvement, Information/support for patients and carersWorkforce – competences, E-learning, methods <strong>of</strong> delivery, facilitators networkCommissioning, currency and pricing, provider development, service improvementCross boundary working/sharing good practice, communications strategy, events ,website
Using the end <strong>of</strong> life care pathway
Six key levers for improving end <strong>of</strong> life carein acute hospitals• Co-ordinated care and discharge planning based on assessed needand by working with community and social care• Senior clinicians making decisions close to the patient andintervening early• Use recognised support tools such as advance care planning and theLiverpool <strong>Care</strong> Pathway <strong>of</strong> the dying• Strong oversight and support from the board and senior management• Training and education appropriate to each team member’s role• Access to a hospital specialist palliative care team
Improved outcomes• Improved patient experience and quality <strong>of</strong> care• Improved the hospital’s reputation• Reduce complaints• Enable people to die in the place they chose• Put control in the hands <strong>of</strong> the hospital with potential cost benefitsfrom reducing unnecessary costly interventions• Skilled workforce with higher morale and improved retention• Access to a hospital specialist palliative care team
Productive Ward - EOLC• Locality registers• Advanced care planning• Amber bundle• LCP(Two tiered approach – executiveengagement)• QIPP
Celebrate whatyou want to seemore <strong>of</strong>’Tom Peters
NCPC & Dying MattersProgress & Prioritiesfor 2011/12
Subscriber Survey: What you toldus• 100% think our publications and DVDs areinformative or very informative• 96% agree or strongly agree that NCPC effectivelycommunicates palliative and end <strong>of</strong> life priorities tonational and regional decision makers• 90% think the subscription is good value for moneyespecially with free Dying Matters membership too
COALITIONGOVERNMENTCoalition politics• Coalition withoutrecent precedent• Aim for a 5-year 5parliament – nextelection 7 May 2015• Andrew Lansley (C) -Sec <strong>of</strong> State forHealth- majorreform/cuts/ pause• Paul Burstow (LD)-<strong>Care</strong> ServicesMinister- cross cuttingLiberal Conservatives
DON’TCHANGE JUSTBECAUSETHERE’S S A NEW• True in May; truetoday:GOVERNMENT• More older people• More dementia andmultiple conditions• More people will dieeach year• Good and badexperiences at home,in care homes andhospitals
Joining up people public experienceswith policy analysis and practicalsupportPublic•• Equip people to tomake choices areality•• Campaign to tomake end end <strong>of</strong> <strong>of</strong> life lifecare care everybody’sbusinessPeople• Developinvolvementtechniques &measurement• Listen and act onwhat people sayPolicy•Develop <strong>End</strong> <strong>of</strong><strong>Life</strong> <strong>Care</strong>intelligence•Build communitycapacity
Our New NCPC Websitewww.ncpc.org.uk
3 Challenges for this Parliament• “Ensuring a good death for everyone”should be a key quality outcome for allcommissioners and providers across health andsocial care• Access to co-ordinatedordinated 24/7 end <strong>of</strong> life careservices to enable people to remain in home andcommunity settings <strong>of</strong> their choice• Empowering people to talk about dying,death and bereavement and to make plans fortheir end <strong>of</strong> life care and support
Our Vision for our 20 th AnniversaryYear People will be aware <strong>of</strong> choices and issues <strong>of</strong>• dying, death and bereavement People will be able to make informed choicesin order to get their needs met People and pr<strong>of</strong>essionals will be equipped tomeet those needs and wishes
2010/11: Involving PeopleAchievementsGrew our work with people with personal experience,involving them in all aspects <strong>of</strong> our workListened to patients and carers and learnt from themLaunched our series <strong>of</strong> ‘how to involve people’ leafletsoutlining a range <strong>of</strong> practical examples <strong>of</strong> involvementLaunched our Difficult Conversations rangeLaunched our ‘Can You See Me?’ DVDWorked with a range <strong>of</strong> communities to test out the DyingMatters leaflets and develop key messages and resources inpartnershipWorked with schools in Hackney and Lewisham
THE DYING MATTERS COALITION• Set up by the <strong>National</strong> Council for Palliative<strong>Care</strong>, the umbrella Charity for all thoseinvolved in palliative care, to support the2008 <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> <strong>Strategy</strong>• It is a broad based, inclusive nationalCoalition, working in partnership, with over15,000 members s from across the NHS andvoluntary and independent health and caresectors, social care and housing, faith,community and retirement organisations,schools, legal, insurance and funeralsectors.19
RESEARCH AND INSIGHT
IMPLICATIONS FORACTIONSCommunicationis the key needed to makeit easier for more peopleto talk about itThe “It’s a long way<strong>of</strong>f” perception:People more likelyto talk to trustedfamily membersand GPsDifferentApproaches/toolsNeeded for differentgroups/audiencestarget groups:55 – 65s65 – 75sGPs
DYING MATTERS SUCCESS• Party for Kath won HC in IVCA Clarion VideoAwards 2010• Awareness Week our second nationalweek saw a step change in activities withnational and local events• Website successful with public facingwebsite pages for the NHS EolC QIPPcampaign• 75,000 leaflets sent out• GP pilots improved confidence & patientexperienceC itit
DYING MATTERS GP PILOTPROJECT• Aim: Support GPs inconversations withpatients & relatives aboutdying & death• 31% <strong>of</strong> public wantinformation about EoLCfrom their GP• 75% <strong>of</strong> GPs agree theyshould encouragepatients to plan for EoLC,yet, only:• 5% <strong>of</strong> GPs have written aOur PilotEvaluationResults• It is possible toincrease GPsconfidence inhaving end <strong>of</strong> lifeconversations• Conversationsbetween GP andpatients, familymembers and
Media Highlightsfrom AwarenessWeek May 2011• Over 200 print and online media coverage – with 10 millionopportunities to see coverage on first day <strong>of</strong> Dying MattersAwareness Week alone• Estimated radio reach <strong>of</strong> 32 million on first day <strong>of</strong> DyingMatters Awareness Week alone plus coverage across the weekincluding major item on BBC Radio 4’s 4 s Midweek Programme• Five different articles in three national newspapers- aneditorial in The Guardian in support <strong>of</strong> palliative care and talkingabout dying and prominent coverage in The Times• Articles online- include Daily Mail website (the most readnews website in the UK, with over 3.5 million daily visitors), TheGuardian (2.4 million daily visitors) and The Mirror (631,000 dailyvisitors)www.dyingmatters.org
Media Highlightsfrom Dying MattersAwareness Week• Articles and coverage across health and care media includingBritish Medical Journal, Nursing Times, Health Service Journal andCommunity <strong>Care</strong>. . Both BMJ and Nursing Times ran polls wesuggested on end <strong>of</strong> life care, which formed the basis <strong>of</strong> additionalnews coverage•• Substantial regional and local media coverage with extensiveprint and broadcast coverage for member-led activities•• Over 20 radio interviews plus interviews across regional radiowith coalition members; adverts from the NHS also ran oncommercial radio in the North West on Smooth Radio and RealRadio
Community Group Members• Local Hospices• Funeral Directors & Solicitors, financial advisors• Local Age Concern , NPC & other pensionerorgs• <strong>Care</strong> Homes• Nursing Homes• Housing Associations• Local Authorities• Schools• GPs, <strong>Care</strong>rs• Acute hospitals• Community Champions•Faith &belief Groups• Bereavement groups• PCTs, SHAsOutcomes• More conversationsleading to more planning,including PPC and ACP• More DM members• Greater priority for end <strong>of</strong> life careCommunity DevelopmentProgrammeOutputs• Local network<strong>of</strong> engagedorganisations• Supportingmaterialsencouragefuture planning• Local eventsduring 2011/12• Higher localpr<strong>of</strong>ile for DMImpact• More people’s wishes are met• Improved end <strong>of</strong> life care
Practical resource withinformation and tipsfrom different sectorson how best to worktogether to raiseawareness incommunities
Community Resources• Practical resource pack with tips fromdifferent sectors on how best to work togetherto raise awareness in communities• Volunteer educator Pack - training packprepares volunteers to share information aboutadvance care planning in their local communitiesor workplaces.• A guide for trainers, , handbooks,presentations and handouts, evaluation sheetsand a resource list• Developed with the University <strong>of</strong> Nottingham
COMMUNITYWWW.DYINGMATTERS.ORG/COMMUNITYEasy to use• Simple registration process• Offers forums, blog, share your event/story• Users can post comments in forum and blogYou can:• Register & postcomments• Add links &buttons to yourwebsites• Provide expertcomment/ opinion• Join DM Twitter &Facebook
TWITTER AND YOUTUBEUploads: 6Twitter statsFollowers: 811 (+188%,January 2011)YouTube statsTotal upload views: 2,404 (+210%, January 2011)
HOW DYING MATTERS USERSCURRENTLY ENGAGE WITH USFacebook Key Stats, May 2011• 887 ‘Likes’ (+70% Jan 2011)• 68,887 post views (+265%)• 275 post feedbacks (+145%)GENDER74% women 22% maleAGE45-5454 28%35-4424%25-3421%55+ 10%18-248%13-1717 2%
What You Can Do
Welcome toThe Annual Joint ConferenceThe <strong>Merseyside</strong> and <strong>Cheshire</strong> <strong>Cancer</strong> Network<strong>End</strong> <strong>of</strong> <strong>Life</strong> and Palliative <strong>Care</strong> CNGandThe <strong>National</strong> Council for Palliative <strong>Care</strong>Thursday 7th July 2011
<strong>National</strong> OverviewEND OF LIFE CAREPr<strong>of</strong>essor John EllershawPr<strong>of</strong>essor <strong>of</strong> Palliative Medicine – Marie CuriePalliative <strong>Care</strong> Institute - University <strong>of</strong>Liverpool<strong>National</strong> Deputy Clinical Director for <strong>End</strong> <strong>of</strong><strong>Life</strong> <strong>Care</strong> – Department <strong>of</strong> Health
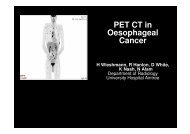
Actual and Projected deaths Englandand WalesSource : Gomes and Higginson; Where people die (1974–2030): past trends, futureprojections and implications for care., Palliative Medicine 2008; 22: 33–41
An ageing populationEngland : The proportion <strong>of</strong> the total population aged 65 and over25Proportion <strong>of</strong> all ages population201510565‐7475‐8485+02006 2010 2020 2030Source :Office <strong>of</strong> <strong>National</strong> Statisticshttp://www.statistics.gov.uk/downloads/theme_population/NPP-2006/NPP06_NSOnline.pdf
Place <strong>of</strong> death by age and sex, percentage <strong>of</strong> deaths in malesand females in each age group in England 2005–070770%60%Percentage <strong>of</strong> deaths in age group50%40%30%20%10%0%Elsewhere Hospice Hospital Nursing home Old people'shomeAge group (years)
The NHS Northwest<strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> ModelUK1 2 3 4 5Advancing diseaseIncreasingDeclineLast Days<strong>of</strong> <strong>Life</strong>First Daysafter DeathBereavement1 year6 monthsDeath1 year
<strong>National</strong> <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> <strong>Strategy</strong>Pre pathwayStep 1Step 2Step 3Step 4Step 5 & 6RaisingAwarenessDiscussionsas the end<strong>of</strong> lifeapproachesAssessment,care planningand reviewCoordination<strong>of</strong> careDelivery <strong>of</strong>high qualityservices indifferentsettings<strong>Care</strong> in thelast days<strong>of</strong> life andcare after deathMeasurement - Intelligence network ,quality markers , VOICESSpirituality, User involvement, Information/support for patients and carersWorkforce – competences, E-learning, methods <strong>of</strong> delivery, facilitators networkCommissioning, currency and pricing, provider development, service improvementCross boundary working/sharing good practice, communications strategy, events ,website
<strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> <strong>Strategy</strong>Key elements:• Societal level:Actions to raiseawareness <strong>of</strong> death andand to change attitudes• Individual level:Integrated servicedelivery based aroundpathway• Infrastructure:measurement,f di ti l t ta caredyingWorkforce development,research,
Measurement & Outcomes• Place <strong>of</strong> death (from death certification)QUIPP• <strong>National</strong> <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> IntelligenceNetwork will bring together differentdatasets e.g. HES, ONS, GPRD andsocial care• VOICES – surveys <strong>of</strong> bereaved relativeswill provide a proxy for quality <strong>of</strong> caregiven to patients at the end <strong>of</strong> life
Treatment and care towards the end <strong>of</strong>life:good practice in decision making
<strong>National</strong> Drivers1. Operational Framework 2011 – <strong>End</strong> <strong>of</strong><strong>Life</strong> <strong>Care</strong>2. Outcomes Framework 20113. QIPP – Stream4. QOFF – Measures5. <strong>National</strong> Tariffs – Summer 20116. NICE Standards – Summer 20117. CQUINS and Proms
<strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> in TheNorth WestPr<strong>of</strong>essor John Ellershaw
<strong>National</strong> <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> <strong>Strategy</strong>Pre pathwayStep 1Step 2Step 3Step 4Step 5 & 6RaisingAwarenessDiscussionsas the end<strong>of</strong> lifeapproachesAssessment,care planningand reviewCoordination<strong>of</strong> careDelivery <strong>of</strong>high qualityservices indifferentsettings<strong>Care</strong> in thelast days<strong>of</strong> life andcare after deathMeasurement - Intelligence network ,quality markers , VOICESSpirituality, User involvement, Information/support for patients and carersWorkforce – competences, E-learning, methods <strong>of</strong> delivery, facilitators networkCommissioning, currency and pricing, provider development, service improvementCross boundary working/sharing good practice, communications strategy, events ,website
Ombudsman's Report2011• Investigation undertaken by the health serviceombudsman into complaints made about the care <strong>of</strong>10 older people.• Each investigation was completed independently butthe report has been pulled together because <strong>of</strong>some common themes and areas <strong>of</strong> concern.• Each investigation highlighted ‘a a stark contrast incare delivered compared to the principles <strong>of</strong> NHSvalues’.• 9 out <strong>of</strong> 10 patients included in the report died
Mr Js Story.• Mr Js wife admitted to hospital from a Nursing home. History <strong>of</strong>Dementia but Mr J and he’s s wife spent time together every daysand enjoyed each others company.• Asked to wait in the waiting room <strong>of</strong> A&E. He was forgottenabout and it was only when Mrs J had died that the staff rangthe nursing home to be reminded that Mr J was actually at thehospital.• Decision made not to resuscitate with no discussion with herhusband.‘They let her slip away under the cloak <strong>of</strong> “quality <strong>of</strong> life”without stopping to think <strong>of</strong> any other involved party’• Mr J felt the hospital had denied them the chance to betogether in the
Mr D’s D s StoryDischarge home described as a shambles:• Daughter arrived to find her fatherin adistressed state behind curtains.• In pain, desperate to go to the toilet.• Buzzer out <strong>of</strong> reach.• Drip bag disconnected and fallen with fluid all over the floor.
Mr D’s D s StoryDischarge home described as a shambles:• Daughter arrived to find her fatherin adistressed state behind curtains.• In pain, desperate to go to the toilet.• Buzzer out <strong>of</strong> reach.• Drip bag disconnected and fallen with fluid all over the floor.• Ambulance did not arrive until 2.30pm. Familytook father home.• Not enough pain killers were provided.• Family spent weekend trying to get painkillersprescribed.• Father died 3 days later.‘Family felt they were deprived <strong>of</strong> spending
‘The investigations reveal an attitude –both personal and institutional – which failsto recognize the humanity and individuality<strong>of</strong> the people concerned and to respond tothem with sensitivity, compassion andpr<strong>of</strong>essionalism’
Using the end <strong>of</strong> life care pathway
Six key levers for improving end <strong>of</strong> life carein acute hospitals• Co-ordinated care and discharge planning based on assessed needand by working with community and social care• Senior clinicians making decisions close to the patient andintervening early• Use recognised support tools such as advance care planning and theLiverpool <strong>Care</strong> Pathway <strong>of</strong> the dying• Strong oversight and support from the board and senior management• Training and education appropriate to each team member’s role• Access to a hospital specialist palliative care team
Improved outcomes• Improved patient experience and quality <strong>of</strong> care• Improved the hospital’s reputation• Reduce complaints• Enable people to die in the place they chose• Put control in the hands <strong>of</strong> the hospital with potential cost benefitsfrom reducing unnecessary costly interventions• Skilled workforce with higher morale and improved retention• Access to a hospital specialist palliative care team
Productive Ward - EOLC• Locality registers• Advanced care planning• Amber bundle• LCP(Two tiered approach – executiveengagement)
Implementing the Renal <strong>End</strong> <strong>of</strong><strong>Life</strong> <strong>Care</strong> <strong>Strategy</strong>:The impact <strong>of</strong> a practice educator on end<strong>of</strong> life care for renal patients.Joan DevereuxMacmillan Nurse
Chronic Kidney Disease (CKD)• Estimated 10-15% 15% <strong>of</strong> population• Affects people <strong>of</strong> all ages• Is classified into 5 stages according to estimatedGlomerular Filtration Rate (eGFR)• Stage 1 is the mildest form• Stage 5 is the most severe (advanced kidney disease)• Patients with eGFR less than 15 (
Why do people with advanced kidneydisease need end <strong>of</strong> life care?Advanced Kidney DiseasePatients whose CKD progresses to end stagekidney disease will die without interventionPatients can choose:• Renal Replacement Therapy (RRT)• Conservative kidney management(everything but dialysis)
<strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> in Advanced KidneyDisease: A Framework forImplementation (June 2009)• <strong>End</strong> <strong>of</strong> life care important for everyone withadvanced kidney disease but especially for thosewho:• decide not to undergo dialysis• choose to withdraw from dialysis after a period <strong>of</strong>treatment• are coming to the end <strong>of</strong> their lives while already onlong term dialysis• have a failing transplant and decide not to return todialysis
Aims <strong>of</strong> Project• <strong>End</strong> <strong>of</strong> life care education for renal staff• Increase in the use <strong>of</strong> the EOLC tools• Gold Standard Framework• Advance care planning / PPC• Liverpool <strong>Care</strong> Pathway• Supportive <strong>Care</strong> Register• Improve the end <strong>of</strong> life care for renalpatients
The Project:• Introductions• Steering group development• Education strategy development• Experiential learning• Delivery <strong>of</strong> education• Data collection• Audit• Resource
Renal Palliative <strong>Care</strong>• Greater insight into the “life” <strong>of</strong> the renalpatient• Need for high quality end <strong>of</strong> life care• Stopping, failing on dialysis• Conservative Management• Failed transplant• Collaborative approach to care• Advice & support• Complex cases• Symptom management• Out <strong>of</strong> hospital EOLC
What We Learned• Engage staff to see that EOLC was relevantto their practice• Taking on a large geographical area as 1person• Keep their engagement in the provision <strong>of</strong>education & motivation• Encourage change in attitudes & practice• Releasing staff for education, time formedical education• Understanding the process <strong>of</strong> advancingdisease & symptom management in ESRF
Success Factors• Being there – part <strong>of</strong> the team, showing byexample• Ongoing & supporting experiential learning• Identifying champions & clinical leaders• Clear goals to give to staff• Data collection• Staff being released for education• Team approach, concurrent education <strong>of</strong>medical & nursing staff• Congruence in attitudes & approach
Audit OutcomesThe project has demonstrated:• Increased Use <strong>of</strong> the Liverpool <strong>Care</strong> Pathway onthe ward.• Increased Use <strong>of</strong> the Liverpool <strong>Care</strong> Pathway<strong>Care</strong> after Death section• Increased number <strong>of</strong> Preferred Priority for <strong>Care</strong>discussions• Increased number <strong>of</strong> discharges for care outsidehospital at end <strong>of</strong> life.• Increased staff knowledge and confidence inend <strong>of</strong> life care.
Take Home Message• Renal patients require end <strong>of</strong> life care• Urgency with CM patients• High quality symptom management• Partnership working• two way learning• Engaging with ‘local’ palliative care services• Specialist renal advice available (hub/spoke)• Prescribing guidance & support leaflets (MCCC)• Communication and outcomes
Conclusions• Renal failure is common• <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> <strong>Strategy</strong> is for all• Patients have a right to good care• Changes in attitude and practice• Collaborative working & shared learning• across teams & boundaries• Education is key to good end <strong>of</strong> life care• Communication pivotal
Questions?
Workshop QuestionsQuestion 1• What end <strong>of</strong> life care education needs tobe provided?• What are the gaps in skills/knowledge <strong>of</strong>staff?• Where do you start?
Workshop QuestionsQuestion 2• What are the challenges to end <strong>of</strong> life careeducation provision?
Workshop QuestionsQuestion 3• Why is data collection important?• What data do we need to collect?• How can we build-in in a data collection system?
Workshop QuestionsQuestion 4• How do you motivate staff to improve end<strong>of</strong> life care?
Today ‘Leadership’ concerns• A guiding vision• Shared values• Influence – not command& control• Personal & organisationalintegrity• Building respect &understanding across oldboundaries to achievecommon purpose• Genuine enthusiasm andbelief about what you wantto achieve• SHARED RESPONSIBILITYNOT ONE PERSON’S S JOB
The Leadership Impact Programme• Designed to strengthen leadership capability inPalliative and <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> across<strong>Merseyside</strong> and <strong>Cheshire</strong> and the North West• Participants will be in key roles in palliative andend <strong>of</strong> life care
KEY IDEAS FOR DESIGN1. Strengthening the network2. Following the pioneers3. Safety first4. Personal to collective5. Getting uncomfortable6. Maximising strengths7. Making a difference at work
1.Strengthening the Network
2. Following thepioneers
3. SafetyFirst
4. Personal to collective4. Individual to Collective
5. GettingUncomfortable
6. DiscoveringandMaximising Strengths
Key Features <strong>of</strong> the Programme• Stepping outside your day to day work to reflect on yourstyle and leadership challenge• Opportunity to work with and learn from others in similarroles, facing similar challenges• Feedback from a range <strong>of</strong> sources on your leadershipstyle and behaviour and its potential impact on yourworkgroup and effectiveness• Individual coaching and group work providing supportand challenge aimed at designing and implementing apersonal leadership development action plan
Programme Elements• Launch & Briefing• Leadership Impact Workshop 24 th May• Coaching Session & Buddy Meeting June• Two-day Development Centre 13 th and 14 thJune• Coaching Session and Buddy MeetingJune/July• Leading in Context Workshop 6 th July• Buddy Meetings• Leading Change Workshop 14 th September
Building links with partners inlong term conditionsKim Wrigley<strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> Lead&Joanne LangtonQuality Improvement Manager
Joint Working• Representation on GM cross cutting group• Sharing information, knowledge and skills• Adding value to end <strong>of</strong> life in heart failure discussions• Collaboratively supporting education and development• Increased opportunities to network
• Input to GM heart failure nurses group• Case studyJoint Working• Provision <strong>of</strong> peer support and advice• Advance care planning• Improved communication <strong>of</strong> local & national issues• Evolving to include other non malignant diseases• Workforce developmentAccess to advanced communication skills training
Annual Collaborative <strong>End</strong> <strong>of</strong> <strong>Life</strong> Event• ICD Deactivation2010(Implantable Cardioverter Defibrillator)• Many issues• No infrastructure – adhoc basis• Working group established• Developing a GM network operational policy
Annual Collaborative <strong>End</strong> <strong>of</strong> <strong>Life</strong> Event2011 Good mix <strong>of</strong> specialities made the day interesting.Common themes emerged in all presentationshighlighting that palliative care principles can beapplied to any speciality. This was an excellent day,lots <strong>of</strong> diversity and very thought provoking.Palliative <strong>Care</strong> Community Nurse SpecialistAnAnenjoyable,enjoyable,informative,informative,wellwellstructuredstructuredandandwellwellbalancedbalancedevent.event.Didn’tDidn’tfeelfeeltalkedtalkedat,at,sessionssessionswerewereengagingengagingbothbothintellectuallyintellectuallyandandemotionally,emotionally,andandthoughtthoughtprovokingprovokingbothbothpr<strong>of</strong>essionallypr<strong>of</strong>essionallyandandpersonally.personally.ThankThankyouyouforforaasupersuperdayday:):)SocialSocialWorker VeryWorker Verygoodgoodinformativeinformativeday.day.GladGladIIattendedattendedititandandbookedbookedtimetime<strong>of</strong>f.<strong>of</strong>f.WillWilltaketakethisthisbackbackwithwithmemetotowork.work.WouldWouldsuggestsuggestthatthatusersuserscommentscommentsononscreenscreenarearenotnotspokenspokenoveroverbybythethespeakers.speakers.DifficultDifficulttotoreadreadandandlistenlistenatatthethesamesametime.time.SocialSocialWorkerWorkerIIfoundfoundthisthistotobebeaaveryveryenjoyableenjoyabledaydaywithwithlotslots<strong>of</strong><strong>of</strong>valuablevaluableinformationinformationwhichwhichIIwillwillcarrycarrywithwithmemeintointomymyjobjobrole.role.TonyTonyBonserBonserwaswasaarealrealassetassettotothetheconferenceconferencehishispassionpassionandandcommitmentcommitmentisisinfectious.infectious.DeputyDeputyManagerManagerThis was the best day <strong>of</strong> training I can remember.I would only say a greater involvement by socialcare may be a good thing in the future. Reducedstaffing budgets and resources are making it sodifficult to deliver good practice which events likethis inspire. Team Manager
Future Plans• 6 monthly post event review• Continued representation <strong>of</strong> groups• Peer support meetings & updates• Inclusion <strong>of</strong> other non malignant diseases/long term conditions• Maintenance <strong>of</strong> good communication links• Continued dissemination <strong>of</strong> information,national/local updates & educationalsupport
Thank youAny Questions?
Implementing the Renal <strong>End</strong> <strong>of</strong><strong>Life</strong> <strong>Care</strong> <strong>Strategy</strong>:The impact <strong>of</strong> a practice educator on end<strong>of</strong> life care for renal patients.Joan DevereuxMacmillan Nurse
Chronic Kidney Disease (CKD)• Estimated 10-15% 15% <strong>of</strong> population• Affects people <strong>of</strong> all ages• Is classified into 5 stages according to estimatedGlomerular Filtration Rate (eGFR)• Stage 1 is the mildest form• Stage 5 is the most severe (advanced kidney disease)• Patients with eGFR less than 15 (
Why do people with advanced kidneydisease need end <strong>of</strong> life care?Advanced Kidney DiseasePatients whose CKD progresses to end stagekidney disease will die without interventionPatients can choose:• Renal Replacement Therapy (RRT)• Conservative kidney management(everything but dialysis)
<strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> in Advanced KidneyDisease: A Framework forImplementation (June 2009)• <strong>End</strong> <strong>of</strong> life care important for everyone withadvanced kidney disease but especially for thosewho:• decide not to undergo dialysis• choose to withdraw from dialysis after a period <strong>of</strong>treatment• are coming to the end <strong>of</strong> their lives while already onlong term dialysis• have a failing transplant and decide not to return todialysis
Aims <strong>of</strong> Project• <strong>End</strong> <strong>of</strong> life care education for renal staff• Increase in the use <strong>of</strong> the EOLC tools• Gold Standard Framework• Advance care planning / PPC• Liverpool <strong>Care</strong> Pathway• Supportive <strong>Care</strong> Register• Improve the end <strong>of</strong> life care for renalpatients
The Project:• Introductions• Steering group development• Education strategy development• Experiential learning• Delivery <strong>of</strong> education• Data collection• Audit• Resource
Renal Palliative <strong>Care</strong>• Greater insight into the “life” <strong>of</strong> the renalpatient• Need for high quality end <strong>of</strong> life care• Stopping, failing on dialysis• Conservative Management• Failed transplant• Collaborative approach to care• Advice & support• Complex cases• Symptom management• Out <strong>of</strong> hospital EOLC
What We Learned• Engage staff to see that EOLC was relevantto their practice• Taking on a large geographical area as 1person• Keep their engagement in the provision <strong>of</strong>education & motivation• Encourage change in attitudes & practice• Releasing staff for education, time formedical education• Understanding the process <strong>of</strong> advancingdisease & symptom management in ESRF
Success Factors• Being there – part <strong>of</strong> the team, showing byexample• Ongoing & supporting experiential learning• Identifying champions & clinical leaders• Clear goals to give to staff• Data collection• Staff being released for education• Team approach, concurrent education <strong>of</strong>medical & nursing staff• Congruence in attitudes & approach
Audit OutcomesThe project has demonstrated:• Increased Use <strong>of</strong> the Liverpool <strong>Care</strong> Pathway onthe ward.• Increased Use <strong>of</strong> the Liverpool <strong>Care</strong> Pathway<strong>Care</strong> after Death section• Increased number <strong>of</strong> Preferred Priority for <strong>Care</strong>discussions• Increased number <strong>of</strong> discharges for care outsidehospital at end <strong>of</strong> life.• Increased staff knowledge and confidence inend <strong>of</strong> life care.
Take Home Message• Renal patients require end <strong>of</strong> life care• Urgency with CM patients• High quality symptom management• Partnership working• two way learning• Engaging with ‘local’ palliative care services• Specialist renal advice available (hub/spoke)• Prescribing guidance & support leaflets (MCCC)• Communication and outcomes
Conclusions• Renal failure is common• <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> <strong>Strategy</strong> is for all• Patients have a right to good care• Changes in attitude and practice• Collaborative working & shared learning• across teams & boundaries• Education is key to good end <strong>of</strong> life care• Communication pivotal
Questions?
Workshop QuestionsQuestion 1• What end <strong>of</strong> life care education needs tobe provided?• What are the gaps in skills/knowledge <strong>of</strong>staff?• Where do you start?
Workshop QuestionsQuestion 2• What are the challenges to end <strong>of</strong> life careeducation provision?
Workshop QuestionsQuestion 3• Why is data collection important?• What data do we need to collect?• How can we build-in in a data collection system?
Workshop QuestionsQuestion 4• How do you motivate staff to improve end<strong>of</strong> life care?
Implementing the Renal <strong>End</strong> <strong>of</strong><strong>Life</strong> <strong>Care</strong> <strong>Strategy</strong>:The impact <strong>of</strong> a practice educator on end<strong>of</strong> life care for renal patients.Joan DevereuxMacmillan Nurse
Chronic Kidney Disease (CKD)• Estimated 10-15% 15% <strong>of</strong> population• Affects people <strong>of</strong> all ages• Is classified into 5 stages according to estimatedGlomerular Filtration Rate (eGFR)• Stage 1 is the mildest form• Stage 5 is the most severe (advanced kidney disease)• Patients with eGFR less than 15 (
Why do people with advanced kidneydisease need end <strong>of</strong> life care?Advanced Kidney DiseasePatients whose CKD progresses to end stagekidney disease will die without interventionPatients can choose:• Renal Replacement Therapy (RRT)• Conservative kidney management(everything but dialysis)
<strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> in Advanced KidneyDisease: A Framework forImplementation (June 2009)• <strong>End</strong> <strong>of</strong> life care important for everyone withadvanced kidney disease but especially for thosewho:• decide not to undergo dialysis• choose to withdraw from dialysis after a period <strong>of</strong>treatment• are coming to the end <strong>of</strong> their lives while already onlong term dialysis• have a failing transplant and decide not to return todialysis
Aims <strong>of</strong> Project• <strong>End</strong> <strong>of</strong> life care education for renal staff• Increase in the use <strong>of</strong> the EOLC tools• Gold Standard Framework• Advance care planning / PPC• Liverpool <strong>Care</strong> Pathway• Supportive <strong>Care</strong> Register• Improve the end <strong>of</strong> life care for renalpatients
The Project:• Introductions• Steering group development• Education strategy development• Experiential learning• Delivery <strong>of</strong> education• Data collection• Audit• Resource
Renal Palliative <strong>Care</strong>• Greater insight into the “life” <strong>of</strong> the renalpatient• Need for high quality end <strong>of</strong> life care• Stopping, failing on dialysis• Conservative Management• Failed transplant• Collaborative approach to care• Advice & support• Complex cases• Symptom management• Out <strong>of</strong> hospital EOLC
What We Learned• Engage staff to see that EOLC was relevantto their practice• Taking on a large geographical area as 1person• Keep their engagement in the provision <strong>of</strong>education & motivation• Encourage change in attitudes & practice• Releasing staff for education, time formedical education• Understanding the process <strong>of</strong> advancingdisease & symptom management in ESRF
Success Factors• Being there – part <strong>of</strong> the team, showing byexample• Ongoing & supporting experiential learning• Identifying champions & clinical leaders• Clear goals to give to staff• Data collection• Staff being released for education• Team approach, concurrent education <strong>of</strong>medical & nursing staff• Congruence in attitudes & approach
Audit OutcomesThe project has demonstrated:• Increased Use <strong>of</strong> the Liverpool <strong>Care</strong> Pathway onthe ward.• Increased Use <strong>of</strong> the Liverpool <strong>Care</strong> Pathway<strong>Care</strong> after Death section• Increased number <strong>of</strong> Preferred Priority for <strong>Care</strong>discussions• Increased number <strong>of</strong> discharges for care outsidehospital at end <strong>of</strong> life.• Increased staff knowledge and confidence inend <strong>of</strong> life care.
Take Home Message• Renal patients require end <strong>of</strong> life care• Urgency with CM patients• High quality symptom management• Partnership working• two way learning• Engaging with ‘local’ palliative care services• Specialist renal advice available (hub/spoke)• Prescribing guidance & support leaflets (MCCC)• Communication and outcomes
Conclusions• Renal failure is common• <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> <strong>Strategy</strong> is for all• Patients have a right to good care• Changes in attitude and practice• Collaborative working & shared learning• across teams & boundaries• Education is key to good end <strong>of</strong> life care• Communication pivotal
Questions?
Workshop QuestionsQuestion 1• What end <strong>of</strong> life care education needs tobe provided?• What are the gaps in skills/knowledge <strong>of</strong>staff?• Where do you start?
Workshop QuestionsQuestion 2• What are the challenges to end <strong>of</strong> life careeducation provision?
Workshop QuestionsQuestion 3• Why is data collection important?• What data do we need to collect?• How can we build-in in a data collection system?
Workshop QuestionsQuestion 4• How do you motivate staff to improve end<strong>of</strong> life care?
QIPP – Demand and ThresholdManagement workstream - EOLC
• Brief re-cap <strong>of</strong> the QIPP (Quality, Innovation,Productivity & Prevention) challenge• NHS structure in response• Accountability framework• Overview <strong>of</strong> demand and threshold managementworkstream• Brief focus on demand• And then EoLC:‣ Size <strong>of</strong> the challenge‣ Why – we should do it‣ How – we can do it (better)
QIPP challenge• Limited financial growth for the NHS from2011/12• The NHS needs to identify £15– 20 billion<strong>of</strong> efficiency savings by the end <strong>of</strong>2013/14 to meet the healthcare demands<strong>of</strong> a growing and ageing population for re-investment to continue to deliver year onyear quality improvements
<strong>National</strong> and regional response..<strong>National</strong> workstreamsNW workstreams• Safe <strong>Care</strong>• Right <strong>Care</strong>• Long Term Conditions• Urgent <strong>Care</strong>• <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong>• Procurement• Productive <strong>Care</strong>• Medicine use and procurement• Primary <strong>Care</strong>• Technology and digital vision• Demand and ThresholdManagement• Estates• Informatics• Prescribing and MedicinesManagement• Primary care contracting• Procurement and supply chain• Provider productivity• Transforming CommunityServices• Workforce and Leadership
Accountability Framework“Each level does what only it can do”L1 – Individuals &Individual Organisations•Efficiency•Clinical Quality Imp•Sale <strong>of</strong> Assets•Level <strong>of</strong> reserve•Int pathwaymanagement•LA / NHS Efficiency•Primary careL4– Region wide / SHA Level•Economies <strong>of</strong> Scale•Standardisation <strong>of</strong> pathways•Regional Commissioning•Residual workstreams•I Manage IT / Education spend•Set direction / rules (intervention)•Manage UpL3 – Footprint Group•Acute Configuration•Distribution <strong>of</strong> specialist business•Collective Commissioning•Piloting innovation•Standardisation <strong>of</strong> Pathways•R & DL2 –Health EconomyPCT & Preferred Supplier•<strong>Care</strong> Pathway•Community services•Level <strong>of</strong> reserve•Civic Leadership•Demand MngtL5 –<strong>National</strong> Work•Pay•Tariff•Financial Planning•Central budgets•Policy change
Demand and Threshold Management• What’s s been happening to demand across the NorthWest?• Approach• The QIPP Steering Group Work Programme• <strong>Care</strong> Pathway Group Reports• North West Case Studies• Long Term Conditions• Shared Decision Making• <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong>• Procedures <strong>of</strong> Limited Clinical Value• Dental <strong>Care</strong>• Utilisation Management Data Deep Dives Reviews
MonthDifference from previous yearMar-11 YTD Difference 2from planMarch 11Difference from previous yearGP Referrals Other Referrals All Referrals OP Attendances Elective Ordinary Elective Daycase Total Elective Non-electivePCTs Difference % Difference % Difference % Difference % Difference % Difference % Difference % Difference %5HG Ashton, Leigh & Wigan 4382 6.37% 3723 9.25% 8105 7.43% 8274 8.56% 172 1.64% 4191 12.16% 4363 9.70% 1184 3.40%TAP Blackburn with Darwen 2236 6.78% -860 -7.72% 1376 3.12% 2175 4.95% -771 -12.30% 1706 10.69% 935 4.21% 308 1.59%5HP Blackpool 2870 9.33% 2539 11.07% 5409 10.07% 13923 32.86% -90 -2.12% 668 3.19% 578 2.30% 834 3.93%5HQ Bolton 4828 7.77% 1183 3.30% 6011 6.13% 8097 9.40% -104 -1.13% 1605 7.08% 1501 4.72% 967 3.40%5JX Bury 1923 5.14% 102 0.41% 2025 3.24% 5107 8.91% -626 -8.04% -1606 -6.37% -2232 -6.76% 954 4.60%5NP Central & Eastern <strong>Cheshire</strong> 3587 4.32% -6267 -10.60% -2680 -1.89% -1700 -1.26% -1026 -7.67% 1677 3.96% 651 1.17% 2460 4.82%5NG Central Lancashire 3319 3.14% 2831 5.48% 6150 3.91% 1086 0.73% -735 -4.51% 2242 3.73% 1507 1.97% 1493 3.02%5NE Cumbria 689 0.61% 1267 3.75% 1956 1.34% 2061 1.51% -692 -3.58% 2044 3.83% 1352 1.86% 1187 2.26%5NH East Lancashire 126 0.14% -4020 -12.79% -3894 -3.29% 526 0.45% -1702 -10.95% 2204 4.89% 502 0.83% 1715 4.19%5NM Halton & St Helens 271 0.38% 3494 11.14% 3765 3.64% 8377 9.20% -118 -1.18% 904 2.73% 786 1.82% 1770 4.51%5NQ Heywood, M'ton & Rochdale 4248 10.22% 881 3.03% 5129 7.27% 6067 9.05% -609 -7.08% -728 -2.59% -1337 -3.64% 915 3.43%5J4 Knowsley -1019 -2.20% 1759 7.66% 740 1.07% 763 1.26% -191 -3.70% 506 2.78% 315 1.35% 10 0.04%5NL Liverpool 7026 6.02% 2352 2.26% 9378 4.25% 3578 1.72% -804 -5.64% 937 1.89% 133 0.21% -1088 -1.58%5NT Manchester -5748 -4.55% -1327 -1.30% -7075 -3.10% 21018 13.16% -2381 -12.56% 2303 4.81% -78 -0.12% 4816 7.16%5NF North Lancashire 2923 4.27% 16007 57.56% 18930 19.67% 10309 11.65% -114 -1.06% 618 1.39% 504 0.91% 1437 3.89%5J5 Oldham 1919 4.49% -966 -3.13% 953 1.29% 2363 3.43% -510 -6.35% 943 4.08% 433 1.39% 3592 13.28%5F5 Salford -893 -1.69% 490 1.31% -403 -0.45% 2648 3.92% -514 -6.19% 1554 7.10% 1040 3.45% 5250 17.93%5NJ Sefton -956 -1.40% 563 1.39% -393 -0.36% -2034 -2.04% -494 -5.22% -1094 -2.99% -1588 -3.45% 949 2.85%5F7 Stockport 1121 1.74% 623 1.34% 1744 1.57% -886 -1.00% -1688 -14.24% 2149 7.97% 461 1.19% 1168 3.31%5LH Tameside & Glossop 496 0.92% 4921 13.91% 5417 6.07% 3650 4.45% -660 -7.82% 178 0.74% -482 -1.49% 1600 6.20%5NR Trafford 59 0.09% 410 1.29% 469 0.49% -1906 -2.37% -185 -2.29% 834 3.14% 649 1.87% 2204 10.53%5J2 Warrington -1067 -3.13% 381 1.72% -686 -1.22% -202 -0.38% 113 1.95% 66 0.35% 179 0.72% 548 2.30%5NN Western <strong>Cheshire</strong> -1344 -2.59% -568 -1.14% -1912 -1.88% -1864 -2.32% -126 -1.45% 2142 7.59% 2016 5.47% -1187 -4.09%5NK Wirral 3270 5.31% 7559 19.92% 10829 10.89% -1235 -1.27% -479 -4.35% 832 2.33% 353 0.76% 1088 2.56%Q31 NHS North West 43674 2.77% 57437 6.10% 101111 4.02% 90195 4.00% -10643 -4.32% 30113 3.86% 19470 1.90% 41346 4.92%Note:Data Source:Orange cells denote PCTs where actual activity was greater than planned 85 Plan data - Vital Signs data submissions March 2008 and Vital Signs refreshes March 2009 / March 2010Blue cells denote PCTs where actual activity was less than planned -85 Actual data - monthly MARCOMM returns submitted to DH via Unify systemGreen cells denote PCTs where actual activity was greater than same period previous year 85Blue cells denote PCTs where actual activity was less than same period previous year -85
What has been happening to demand in 2010/11?• Referrals have gone up in 2/3 <strong>of</strong> PCTs• Trends in referrals and out patient activity are notalways correlated!• Almost universal shift from elective IPs to Day Cases• Only 5 PCTs have reduced total elective activity• Only 2 PCTs have reduced non elective activity• The North West has a sizeable gap between our “plans”and actual delivery
Some Important Principles• “Managing Demand” should mean meeting needs in the mosteffective, efficient and patient centred way… not denying access• Existing incentives (in particular PbR) encourage growth in activity–we need to test new approaches• Better ‘integration”• between sectors• between commissioners and providers• Between providers and patientsis key to a more effective management <strong>of</strong> demand• Reduction in demand needs to result in reductions in capacity andconsequent reductions in cost for both commissioners and providersrs
<strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong>• Estimated that hospital admissions in the lastyear <strong>of</strong> life for adults cost the NHS £1.3 billion• By delivering improved recognition <strong>of</strong> palliativecare needs, as well as optimised provision <strong>of</strong>hospital services outside hospital setting couldreduce hospital deaths by approx. 60,000 perannum by 2021.• Using the QIPP estimate <strong>of</strong> £3,000 per hospitaldeath translates to a potential reduction inhospital costs <strong>of</strong> £180 million per annum.
• NHS Operating Framework (England) 2011/12 –“the NHS should continue to ensureimplementation <strong>of</strong> the <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> <strong>Strategy</strong>,working to <strong>of</strong>fer patients the choice <strong>of</strong> where tobe cared for as they approach the end <strong>of</strong> life,and where to die, regardless <strong>of</strong> their condition”.Focus on % deaths at home.• NW quality vision – aim for a 10% reduction inhospital deaths through better EoLC planning;reducing emergency admissions in the lastmonth <strong>of</strong> life
How?• Locality registers• Six steps to success – programme for carehomes• GP practices – GSF• Routes to success – in end <strong>of</strong> life care –achieving quality in acute hospitals
ThankyouSusan SummersAssistant Director Quality Assurance and Self <strong>Care</strong>NHS North West SHASusan.summers@northwest.nhs.uk
INFLUENCING THE REFORMAGENDA: KEEPING END OF LIFECARE A PRIORITYJuly 2011SIMON CHAPMANDIRECTOR OF POLICY& PARLIAMENTARY AFFAIRSwww.dyingmatters.org
OMBUDSMAN• “Poor communication & thoughtless action• Discharge can be shambolic and ill-prepared• The NHS must close the gap between the promise<strong>of</strong> care and compassion in its Constitution and theinjustice many older people experience• Inattention to the suffering <strong>of</strong> older people ischaracteristic <strong>of</strong> the stories in this report• <strong>Care</strong> should be shaped not just by their illness,but by the wider context <strong>of</strong> their lives andrelationships”www.dyingmatters.org
REFORM: getting from here...www.dyingmatters.org
...to here?• Patients at the centre• ClinicalCommissioning• Advisory senates• Greater choice &control• Integration &collaboration• Health & well-beingboards• Outcomes frameworks• Funding Review &Dilnotwww.dyingmatters.org
EDDY & MYRLE• EDDY• 86 years old• Lived in shelteredhousing for 5 years.Wants to stay there• In pain; breathless; inbed much <strong>of</strong> the time;not eating much;depressed• Doesn’t t want CPR orantiobiotics for a chestinfection• MYRLE• Eddy’s s daughter, livesnearby; visits daily• Helps Eddy on personalbudgets (health & socialcare)• Eddy is on theGP’s s end <strong>of</strong> liferegister. Quarterlymeeting in 7 weekstime.www.ncpc.org.uk
www.ncpc.org.uk
Policy priorities 11/12• Making end <strong>of</strong> life care a priority at everylevel• Supporting commissioners and providers• Strategic partnership with DH• Building community capacity• Focus on 24/7 care: “all hours” not “out <strong>of</strong> hours”• Developing end <strong>of</strong> life care intelligence• NEoLCIN and Funding Review• Conferences on dementia and heart failure
WHAT WILL WE BE DOING?• Equipping• A+E or A&E?: earlycommissioning actionsfor consortia• Key relationships andquestions: how toinfluence & drive changeat every level• Developing & applyingintelligencewww.dyingmatters.org
24/7• Manifesto call• In white paper• Funding Reviewrecommendation• 49% <strong>of</strong> surveyrespondentsconcerned about painrelief in their area• Conference;publicationwww.dyingmatters.org
HEALTH & SOCIAL CARE BILL• “Pause” aka “NHS Future Forum”• Strong commitments to Eolc• Over 180 amendments to Bill• New local commissioning remains• “Shadow commissioning” by central NCB• Monitor to promote integration and involve public• Operating Framework to be replaced by multi-yearministerial mandate• Health & wellbeing boards to have right to refer backcommissioning planswww.ncpc.org.uk
Palliative <strong>Care</strong>Funding Review• “Stunning inequities”• Range <strong>of</strong> PCT (exc. vol sector) spending on spc/death £168- £6213• 61% spend
Palliative <strong>Care</strong> Funding Review (2)• Looking at phases <strong>of</strong> illness• Stable• Deteriorating• Unstable• Dying• System refined within those categories by needand setting, and packages <strong>of</strong> care providedaccordinglywww.dyingmatters.org
GOVT RESPONSE• “We want to see integrated, responsive andhigh-quality health and care services for those atthe end <strong>of</strong> life. We will now consider the reviewteam’s s proposals in detail before consultingstakeholders on the way forward later thissummer. We will also consider how best toundertake substantial piloting, , as recommendedin the report, in order to gather information onhow best to deliver palliative care services.”• Hansard 3 July 2011www.dyingmatters.org
NICE• Draft Quality Standard: consulting until22/7• 20 statements• Can they be reduced to 15?• Status at present: non-mandatory. But....• Service specifications• Local contractingwww.dyingmatters.org
DILNOT PROPOSALS• Cap on care costs c £35-£50K50K• “Hotel” costs capped at £7-10K/year• Will enable insurance• Not compulsory• Supports Funding Review’s s proposal <strong>of</strong>non- means tested social care at EoLwww.dyingmatters.org
JOINING EVERYTHING UP• Patients at the centre• ClinicalCommissioning• Advisory senates• Greater choice &control• Integration &collaboration• Health & well-beingboards• Outcomes frameworks• Funding Review &Dilnotwww.dyingmatters.org
PEOPLE’S S NEEDS ARETHE SAME• True in 2010; truetoday:• More older people• More dementia andmultiple conditions• More people will dieeach year• Numbers <strong>of</strong> homedeaths below 20%
OPPORTUNITIES &CHALLENGES• Who are your local budget holders & decisionmakers at any given time?• Identifying & working with emergent consortia• How do you fit into local health & social care?• What needs can you help meet?• Working with new partners• Integrating care• New levers to build capacity in the communitywww.dyingmatters.org
LOOKING TO THE FUTURE• Build capacity in the community• Training and education• Equip leaders & champions• Campaign & mobilise for end <strong>of</strong> life care tobe a priority• What can we do together to makeend <strong>of</strong> life care a priority in yourarea?www.dyingmatters.org
www.dyingmatters.org
Caroline Flynn, Elaine Horgan and Christine Taylor
Living well and dying well
<strong>National</strong> Facts And FiguresThere is a major discrepancy between people’s preferences for where they should die and theirplace <strong>of</strong> death• 500,000 people die in England each year.•This will rise to around 530,000 by 2030•Most would prefer to die at home•Only around 18% do so with a further 17% in care homes•Acute hospitals accounting for 58% <strong>of</strong> all deaths•Around 4% in hospices•Only around one third <strong>of</strong> general public have discussed death and dying withanyone• 700,000 people have dementia and 1/3 live in a care home
<strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> <strong>Strategy</strong> 20084.39“GoodPCT’s working with local authorities will wish to commission services from carehomes which:• Residents approaching the end <strong>of</strong> life are on an end <strong>of</strong> life care register• Each resident is <strong>of</strong>fered a care plan, which clearly identifies their tneeds andpreferences for care• Staff receive the training and support they need to provide end <strong>of</strong> life care• There is a appropriate access to GP, District nursing and specialist palliative careadvice”DOH, 2008, <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> <strong>Strategy</strong> p95
Reduction ininappropriatehospitaladmissionsPatient achievingtheir wishes andpreferences at end<strong>of</strong> life <strong>of</strong> where theywant to dieKey Leversfor improved <strong>Care</strong>Equity andaccess to end<strong>of</strong> life care
Challenges for care homesdelivering end <strong>of</strong> life care• Leadership• Staff turnover• Culture <strong>of</strong> the care home• MDT working (sharing information)• Advance <strong>Care</strong> Planning; Starting the conversation with long termresidents• Recognition <strong>of</strong> residents in the last 12 months <strong>of</strong> life• Diagnosing dying
Do care homes have thesupport they need?A 2009 study into the provision <strong>of</strong> goodend <strong>of</strong> life care in care homesdemonstrated that delivery <strong>of</strong> good qualityend-<strong>of</strong>-life care in care homes requires aneffective balance <strong>of</strong> external support, andinternal resources.
more work is needed to enable integration<strong>of</strong> nursing homes into the wider systems <strong>of</strong>end <strong>of</strong> life care and to enablecollaboration across organizational,institutional and funding boundaries sothat patients receive a better quality <strong>of</strong> end<strong>of</strong> life care regardless <strong>of</strong> the care setting inwhich they are located. ‘Jane E Seymour, Arun Kumar andKatherine Froggatt (2009)
Why support care homes• Fits with the <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> <strong>Strategy</strong> identifying the need fora cultural shift in attitude & behaviour across the health &social care workforce.• 10% reduction in inappropriate hospital deaths ( North WestHealthier Horizons 2008)• Provide stronger partnerships between the NHS and theindependent care sector• Address the key components <strong>of</strong> <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> education tosupport care homes in providing end <strong>of</strong> life care i.e ACP,communication skills & LCP• Improving equity <strong>of</strong> quality end <strong>of</strong> life care for allirrespective <strong>of</strong> care setting
“ It should not be down to ’luck’ and wherewe live in the country as to how we die,we all know death happens and we shouldbe more prepared, human and caring”Comment posted on the Patient Opinionwebsite www.patientopinion.org.uk
<strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> Training Matrix
ConceptTo develop a low cost, consistent end <strong>of</strong> life care programme,available to all care homes. It will support the development <strong>of</strong>nominated staff in residential and/or nursing homes tobecome <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> Home Representatives (champions)implementing organisational change utilising the Route toSuccess for care homes.Allow areas supporting the programme to include localpolicies, guidance & literature to promote somestandardisation across settings.
The story so far….NetworkNumber <strong>of</strong>care homesNumber <strong>of</strong>PCTsPCTs inagreementMCCN60076GMCCN651116CLEOLCN80066
QIPPQuality Innovation Productivity Prevention •Improve the resident and family experience <strong>of</strong> end <strong>of</strong> life care in acare home setting•Enhance care delivery within the care home at end <strong>of</strong> life•A A skilled workforce•A A low cost Network EOL programme providing a consistentapproach across PCT’s with a wide access to all care homes•Can support care homes who currently have high recordedadmissions to the acute sector for end <strong>of</strong> life care•Develop a care home representative to take responsibility for thefuture development <strong>of</strong> end <strong>of</strong> life care provision in their care homeh•Enhanced end <strong>of</strong> life care•Enhanced MDT working•Deliver choice at end <strong>of</strong> life•Wider awareness and implementation <strong>of</strong> <strong>End</strong> <strong>of</strong> life care•Development <strong>of</strong> PCT <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> home representativeGroups•Address equity•Reduction in hospital admissions at end <strong>of</strong> life from <strong>Care</strong> homes•Reduction <strong>of</strong> isolated working
Local Recruitment• Local awareness raising session• Participation criteria agreement to be signed• Registration
Expectations <strong>of</strong> an <strong>End</strong> <strong>of</strong> <strong>Life</strong><strong>Care</strong> Home Representative• Regularly meet with other <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> Home Representatives• Develop other learners in end <strong>of</strong> life care• Build resource files within the care home• Produce a portfolio to evidence the implementation <strong>of</strong> the programmethat could be shared with regulatory bodies (CQC), commissioners,social services• To be a link with the local <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> Facilitator• Initiate change management within the home
Overview <strong>of</strong> the Six Steps toSuccess Programme• Induction workshop• Six Steps to Success workshops‣ Step 1 - Discussions as the end <strong>of</strong> life approaches‣ Step 2 - Assessment, care planning and review‣ Step 3 - Co-ordination ordination <strong>of</strong> care‣ Step 4 - Delivery <strong>of</strong> high quality care in care homes‣ Step 5 - <strong>Care</strong> in the last days <strong>of</strong> life‣ Step 6 - <strong>Care</strong> after death• Conclusion workshop• Supporting education: communication skills, Advance <strong>Care</strong>Planning and Liverpool <strong>Care</strong> Pathway for the dying patient (LCP)• Continuation <strong>of</strong> care home forum
Celebration• On Completion <strong>of</strong> the Six Step to SuccessProgramme the <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> Representative willbecome the <strong>Care</strong> Home <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong>‘Champion’• The <strong>Care</strong> Home Representative will receive acertificate <strong>of</strong> attendance• <strong>Care</strong> home will receive a dated certificate oncompletion <strong>of</strong> portfolio
Evaluation/SustainabilityEvaluationSustainability•Ongoing evaluation throughout thecourse•<strong>Care</strong> home forums continue on aregular basis•Pre and post course audits•<strong>Care</strong> homes set agenda•Audit <strong>of</strong> ACP/LCP•External speakers•<strong>National</strong> roll out <strong>of</strong> the Six Steps toSuccess Programme•Continuing access to education andsupport•<strong>National</strong> evaluation through the<strong>National</strong> <strong>End</strong> <strong>of</strong> <strong>Life</strong> care Programme•Local area to decide how they willensure sustainability depending onresources<strong>End</strong> <strong>of</strong> life care home forum will be a valuable resource group to drive and trial newinitiatives in end <strong>of</strong> life care for the care home sector i.e. E-Learning
How will the resident &family/commissioner/care home know it hasworked• Residents receive their wishes and preferences at end <strong>of</strong> life• Family feel supported• Use <strong>of</strong> Liverpool <strong>Care</strong> pathway/Six Steps to Success programmedemonstrates quality care given• Fewer <strong>End</strong> Of <strong>Life</strong> <strong>Care</strong> complaints• Reduction in inappropriate hospital admissions• Staff are trained and competent to deliver the care• Equity and equal access to quality end <strong>of</strong> life care to all
ContactsElaine Horgan - <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong>, <strong>Care</strong> Home CoordinatorGreater Manchester and <strong>Cheshire</strong> <strong>Cancer</strong> NetworkElaine.horgan@manchester.nhs.uk0161 920 9723Caroline Flynn – <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> Lead, <strong>Merseyside</strong> and <strong>Cheshire</strong> <strong>Cancer</strong>NetworkCaroline.flynn@mccn.nhs.uk0151 201 4150Charlotte Pilkington - <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> Home Service Improvement FacilitatorCumbria and Lancashire <strong>End</strong> <strong>of</strong> <strong>Life</strong> <strong>Care</strong> NetworkEmail: charlotte.pilkington@lsccn.nhs.ukTel: 01772 647058/647147Access the Six Steps to Success Programme for <strong>Care</strong> Homes at:Access the Six Steps to Success Programme for <strong>Care</strong> Homes at:http://www.end<strong>of</strong>lifecareforadults.nhs.uk/caresettings/carehomes/route-to-success-in-care-homes-package