ACCIDENT, INCIDENT & NEAR MISS REPORT - eRiding
ACCIDENT, INCIDENT & NEAR MISS REPORT - eRiding
ACCIDENT, INCIDENT & NEAR MISS REPORT - eRiding
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
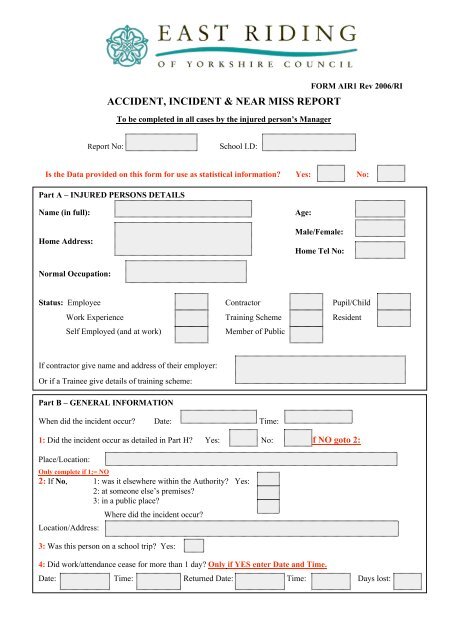
<strong>ACCIDENT</strong>, <strong>INCIDENT</strong> & <strong>NEAR</strong> <strong>MISS</strong> <strong>REPORT</strong>To be completed in all cases by the injured person’s ManagerFORM AIR1 Rev 2006/RIReport No: School I.D:Is the Data provided on this form for use as statistical information? Yes: No:Part A – INJURED PERSONS DETAILSName (in full): Age:Home Address:Male/Female:Home Tel No:Normal Occupation:Status: Employee Contractor Pupil/ChildWork Experience Training Scheme ResidentSelf Employed (and at work) Member of PublicIf contractor give name and address of their employer:Or if a Trainee give details of training scheme:Part B – GENERAL INFORMATIONWhen did the incident occur? Date: Time:1: Did the incident occur as detailed in Part H? Yes: No: if NO goto 2:Place/Location:Only complete if 1;= NO2: If No, 1: was it elsewhere within the Authority? Yes:2: at someone else’s premises?3: in a public place?Location/Address:Where did the incident occur?3: Was this person on a school trip? Yes:4: Did work/attendance cease for more than 1 day? Only if YES enter Date and Time.Date: Time: Returned Date: Time: Days lost:
Part C – MAJOR INJURY Tick either box 01/ or 02 then one box 03 – 15Fatality 01 Major injury/condition 02Death of a person or persons 03 Any other injury requiring resusc’n 10Any fracture (other than fingers, thumbs, toes) 04 Admitted/remained in hospital (ovr 24hrs) 11Any amputation (traumatic or surgical) 05 Loss of consciousness from:Dislocated shoulder, hip knee or spine 06 Asphyxiation/harmful substance/biological agent. 12Loss of sight (temporary or permanent) 07 by: inhaled/ingested/absorbed through skin 13Eye injury (chemical or permanent) 08 Acute illness-bio.agent/toxin/infected material 14Electric shock/burn leading to unconsciousness 09Any other injury leading to hypothermia, heatorrequiring resusc’n or hospital (over 24 hrs) induced illness or unconsciousness 15If Box 1 or 2 is Ticked (as a result of work etc) Tel. HSE within 24 hrs + Form F2508 to HSE within 10 Days)Part D - MINOR INJURIES Tick one box 16 – 21a then one box 22 – 31aMore than 3 days incapacity to work 16 3 days absence 182 days & under absence 19 No absence 20 Near Miss Incident 21Taken to hospital for treatment :-(member of public, child, resident, etc) Not Employees 17 Not Known 21a(None Employees only)Fracture (fingers, thumbs, toes only) 22 Dislocation (other than shoulder, hip, knee or spine) 27Cuts / abrasions 23 Foreign body in eye (grit etc) 28Bruising 24 Minor electric shock/burn 30Strains / sprains 25 Other (describe in details of accident box) 31Minor burns / scalds 26 No other Injury (describe in details of accident box 31aIf Box 01, 02, 16 or 21 is Ticked (as a result of work etc – Contact SSU ASAPIf Dangerous Occurrence: tick one of the above codes between 03 – 15 or 22 to 31a and 999 belowDangerous Occurrence (999) Reference Number TypePart E – AGENT OF INJURY (Please tick One Box 32 – 41a)Machinery 32 Hand Tool 33 Vehicle 34Ground or surface 35 Building 36 Physical Object 37Other 40 None 41a
Part F – PART OF BODY INJURED (Location of Injury)(Please tick ONE box 41 – 60a or 99 to indicate the most severely injured part of the body)Head 41 Finger/Thumb 46 Shoulder 51 Knee 56Face 42 Hand 47 Internal 52 Leg 57Neck 43 Wrist 48 Toe 53 Hip 58Chest 44 Elbow 49 Foot 54 Pelvis 59Back 45 Arm 50 Ankle 55 Multiple 60Other (Specify in ‘Details of Accident’ box below) 99 None 60aPart G – KIND OF <strong>ACCIDENT</strong> – (Please tick ONE box 61 – 76)Contact with machinery of material being machined 61 Struck by moving, falling or flying object 69Struck by moving vehicle 62 Struck against something fixed of stationary 70Injured while handling, lifting or carrying 63 Slip, trip or fall on same level 71Fall from a height metres 64 Trapped by something collapsing/overturning 72Drowned or asphyxiated 65 Exposed (contact with) harmful substance 73Exposed to fire 66Exposed to explosion 67Contact with electricity or electrical discharge 68 Other (Specify in ‘Details of Accident’ below)76Part H - ABOUT YOUName of person making report:Job Title:Directorate: Division:Section: Centre, Facility,Depot etc:Street: Town:Post Code:Tel No:
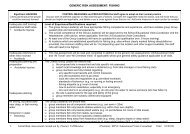
Part I – RECORDING PROCEDURESAccident recorded in Accident Book – Form BI.510 or equivalent Yes: No: Date:Has a Form F2508 (or F2508A) been sent to the H.S.E. Yes: No: Date:Has a Form AIR1 been sent to the relevant Trade Union Yes: No: Date:Part J – DETAILS OF <strong>ACCIDENT</strong> & OUTCOME OF INVESTIGATIONPart K – PREVENTATIVE ACTION (To be completed by [or on behalf of] Senior Management)What action has been, (or will be), taken to prevent recurrence?Please tick relevant box(es) and give brief explanation)Risk Assessment Review Discipline Protective clothing obtainedGuarding Prohibition Protective clothing enforcedTraining Procedures SupervisionOtherBrief Explanation:Signature: Date: Position:
<strong>ACCIDENT</strong> / <strong>INCIDENT</strong> PERSONAL STATEMENT Form AIR3Investigating Officer:Date:WITNESS DETAILSName (in full)Normal Occupation/Status:Home AddressEmployer/Directorate: Tel No:GENERAL INFORMATIONWhen did the accident occur? Date: Time: (24hr clock)Name of injured person:STATEMENTWhen taking this statement, consider the involvement of the witness. Ask them to sign and date the form at the end ofthe written statement
STATEMENT CONTINUEDPageofContinue Overleaf