part ii policies and procedures for rural health clinic services
part ii policies and procedures for rural health clinic services
part ii policies and procedures for rural health clinic services

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
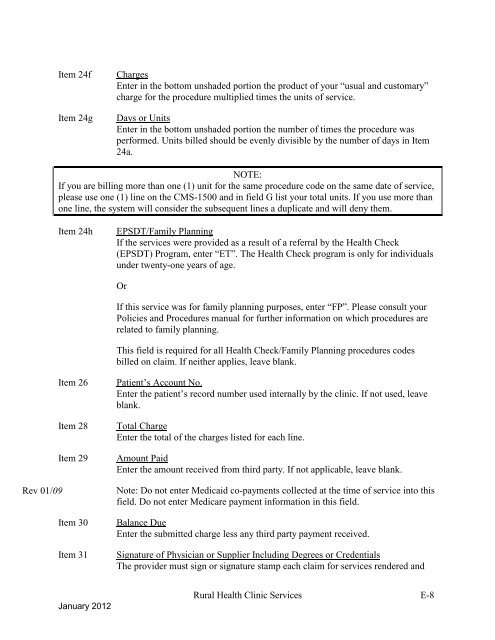
Item 24fItem 24gChargesEnter in the bottom unshaded portion the product of your “usual <strong>and</strong> customary”charge <strong>for</strong> the procedure multiplied times the units of service.Days or UnitsEnter in the bottom unshaded portion the number of times the procedure wasper<strong>for</strong>med. Units billed should be evenly divisible by the number of days in Item24a.NOTE:If you are billing more than one (1) unit <strong>for</strong> the same procedure code on the same date of service,please use one (1) line on the CMS-1500 <strong>and</strong> in field G list your total units. If you use more thanone line, the system will consider the subsequent lines a duplicate <strong>and</strong> will deny them.Item 24hEPSDT/Family PlanningIf the <strong>services</strong> were provided as a result of a referral by the Health Check(EPSDT) Program, enter “ET”. The Health Check program is only <strong>for</strong> individualsunder twenty-one years of age.OrIf this service was <strong>for</strong> family planning purposes, enter “FP”. Please consult yourPolicies <strong>and</strong> Procedures manual <strong>for</strong> further in<strong>for</strong>mation on which <strong>procedures</strong> arerelated to family planning.This field is required <strong>for</strong> all Health Check/Family Planning <strong>procedures</strong> codesbilled on claim. If neither applies, leave blank.Item 26Item 28Item 29Rev 01/09Item 30Item 31Patient‟s Account No.Enter the patient‟s record number used internally by the <strong>clinic</strong>. If not used, leaveblank.Total ChargeEnter the total of the charges listed <strong>for</strong> each line.Amount PaidEnter the amount received from third <strong>part</strong>y. If not applicable, leave blank.Note: Do not enter Medicaid co-payments collected at the time of service into thisfield. Do not enter Medicare payment in<strong>for</strong>mation in this field.Balance DueEnter the submitted charge less any third <strong>part</strong>y payment received.Signature of Physician or Supplier Including Degrees or CredentialsThe provider must sign or signature stamp each claim <strong>for</strong> <strong>services</strong> rendered <strong>and</strong>January 2012Rural Health Clinic Services E-8