part ii policies and procedures for rural health clinic services
part ii policies and procedures for rural health clinic services
part ii policies and procedures for rural health clinic services

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
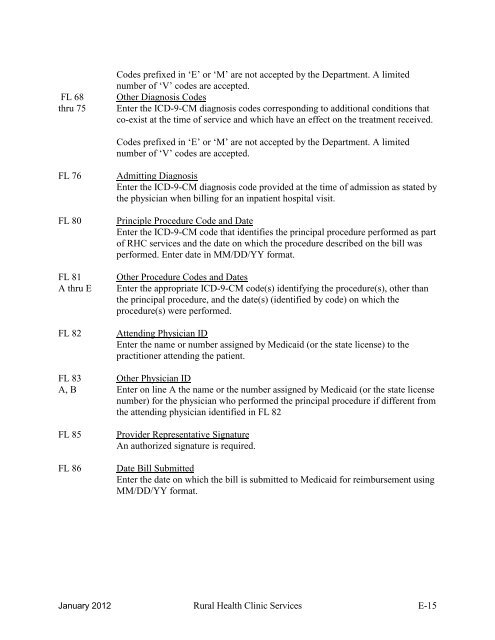
FL 68thru 75Codes prefixed in „E‟ or „M‟ are not accepted by the De<strong>part</strong>ment. A limitednumber of „V‟ codes are accepted.Other Diagnosis CodesEnter the ICD-9-CM diagnosis codes corresponding to additional conditions thatco-exist at the time of service <strong>and</strong> which have an effect on the treatment received.Codes prefixed in „E‟ or „M‟ are not accepted by the De<strong>part</strong>ment. A limitednumber of „V‟ codes are accepted.FL 76FL 80FL 81A thru EFL 82Admitting DiagnosisEnter the ICD-9-CM diagnosis code provided at the time of admission as stated bythe physician when billing <strong>for</strong> an inpatient hospital visit.Principle Procedure Code <strong>and</strong> DateEnter the ICD-9-CM code that identifies the principal procedure per<strong>for</strong>med as <strong>part</strong>of RHC <strong>services</strong> <strong>and</strong> the date on which the procedure described on the bill wasper<strong>for</strong>med. Enter date in MM/DD/YY <strong>for</strong>mat.Other Procedure Codes <strong>and</strong> DatesEnter the appropriate ICD-9-CM code(s) identifying the procedure(s), other thanthe principal procedure, <strong>and</strong> the date(s) (identified by code) on which theprocedure(s) were per<strong>for</strong>med.Attending Physician IDEnter the name or number assigned by Medicaid (or the state license) to thepractitioner attending the patient.FL 83 Other Physician IDA, B Enter on line A the name or the number assigned by Medicaid (or the state licensenumber) <strong>for</strong> the physician who per<strong>for</strong>med the principal procedure if different fromthe attending physician identified in FL 82FL 85FL 86Provider Representative SignatureAn authorized signature is required.Date Bill SubmittedEnter the date on which the bill is submitted to Medicaid <strong>for</strong> reimbursement usingMM/DD/YY <strong>for</strong>mat.January 2012 Rural Health Clinic Services E-15