C.M. Bono and R.F. Heary / The Spine Journal 4 (2004) 230–240 235characterized. If, after appropriate measures, cervical stabilityremains in question, surgical stabilization may be considered<strong>to</strong> prevent un<strong>to</strong>ward neurologic injury, particularlyif an intracanal bullet or bone fragment is in close proximity <strong>to</strong><strong>the</strong> spinal cord or nerve roots.In contrast <strong>to</strong> blunt traumatic injuries, which have moredefined radiographic criteria for instability, any degree <strong>of</strong>abnormal angulation or translation may represent instabilityafter gunshot <strong>wounds</strong> <strong>to</strong> <strong>the</strong> cervical <strong>spine</strong>. In cases <strong>of</strong> instability,<strong>the</strong> affected segments can be stabilized with a variety<strong>of</strong> instrumentation and fusion constructs. In <strong>the</strong> patient withneurologic deficit, spinal stability is deduced from imagingfindings. Severe comminution <strong>of</strong> both anterior and posteriorelements with evidence <strong>of</strong> segmental deformity is indicative<strong>of</strong> instability.The majority <strong>of</strong> cases <strong>of</strong> instability after gunshot <strong>wounds</strong>have been associated with overly aggressive decompression[34]. Fortunately, <strong>the</strong>re are few indications for decompressionin a neurologically intact patient. New onset orprogressive neurological deficit associated with an intramedullarybullet, bone fragment or expanding epidural hema<strong>to</strong>mais an indication for urgent decompression. Importantly,neurologic progression is most accurately detected by means<strong>of</strong> serial examinations performed by a single experiencedobserver and documented in <strong>the</strong> chart so that follow-upexaminations can be compared with baseline. Less frequentlycited indications are for <strong>the</strong> treatment <strong>of</strong> lead in<strong>to</strong>xicationfrom <strong>the</strong> bullet or contact <strong>of</strong> a copper jacketed missilewith <strong>the</strong> neural elements [11,31,35]. Routine removal <strong>of</strong><strong>the</strong> bullet is not warranted for transcolonic injury and isassociated with a high rate <strong>of</strong> complications.<strong>Gunshot</strong> injury: neurologic deficitSpinal cord injuries are devastating <strong>to</strong> <strong>the</strong> patient, familyand society. In a study by Roye et al. [2] in 1988, <strong>the</strong> averageinitial admission hospital costs for survivors <strong>of</strong> cervicallevel injury can be greater than $50,000. High-level completeinjuries frequently leave patients ventila<strong>to</strong>r dependent,requiring highly specialized units for prolonged care. <strong>Gunshot</strong><strong>wounds</strong> more frequently result in complete injuriescompared with blunt trauma, which may be paraplegic orquadriplegic depending on <strong>the</strong> level. Approximately 59%<strong>of</strong> penetrating cervical <strong>spine</strong> injuries result in completespinal cord injury, compared with 49% for blunt trauma [36].In contrast <strong>to</strong> <strong>the</strong> predominance <strong>of</strong> cervical level injuriesafter blunt trauma, <strong>the</strong> majority <strong>of</strong> spinal cord injuries aftergunshot <strong>wounds</strong> occur at <strong>the</strong> thoracic level [36]. Incompleteinjuries can present in a variety <strong>of</strong> manners, includingBrown-Sequard, central cord, anterior cord or in rare casescruciate hemiplegic syndromes [37].Decompression/bullet removalThe first rule <strong>of</strong> medicine is primum non nocere, or “donor harm.” This must be kept in mind in managemen<strong>to</strong>f neurologic deficit after gunshot <strong>wounds</strong> <strong>to</strong> <strong>the</strong> <strong>spine</strong> (Fig.3). It is our tendency as surgeons <strong>to</strong> be compelled <strong>to</strong> removebullets and decompress <strong>the</strong> spinal canal. However, <strong>the</strong> clinicalbenefit <strong>of</strong> <strong>the</strong>se actions is inconsistent and is not withoutcomplications.In both complete and incomplete spinal cord injuries, <strong>the</strong>role <strong>of</strong> decompression has been studied. Stauffer et al. [34]reviewed 185 cases <strong>of</strong> gunshot paralysis, half <strong>of</strong> which weretreated with laminec<strong>to</strong>my and half with observation only.The authors documented no appreciable return <strong>of</strong> neurologicalfunction after both surgery and nonoperative managementfor complete lesions. With incomplete injuries, 71%<strong>of</strong> decompressed <strong>spine</strong>s and 77% <strong>of</strong> nonsurgically treated<strong>spine</strong>s demonstrated neural improvement. Incomplete lesions<strong>to</strong> <strong>the</strong> lumbar <strong>spine</strong> and thoracolumbar junction hadbetter neurologic recovery than more cranial levels regardlessif surgery was performed. Although antibiotic regimenwas not documented, four wound infections and sixspinal fistulae were reported in <strong>the</strong> operative group as wellas six cases <strong>of</strong> late spinal instability. There were no cases<strong>of</strong> infection, cerebrospinal fluid fistula or spinal instabilityin <strong>the</strong> nonsurgically treated patients. Both groups had ahigh incidence <strong>of</strong> causalgia (19% and 15% for operative andnonoperative groups, respectively). In support <strong>of</strong> a nonoperativeapproach, Robertson and Simpson [38] reported no neurologicimprovements with lumbar laminec<strong>to</strong>my versusnonsurgical treatment in 30 patients with gunshot <strong>wounds</strong> <strong>to</strong><strong>the</strong> cauda equina region. A high rate <strong>of</strong> pos<strong>to</strong>perative complicationswas reported. In no case did <strong>the</strong> authors report anintracanal bullet.In a more recent prospective study <strong>of</strong> lesions associatedwith intracanal bullets, Waters and Adkins [39] demonstratedstatistically significant mo<strong>to</strong>r improvement after surgicaldecompression from <strong>the</strong> T12 <strong>to</strong> L4 levels comparedwith nonoperatively treated <strong>spine</strong>s (Fig. 4). At more cranialsites in <strong>the</strong> thoracic and cervical regions, surgical removal anddecompression had no significant effect on neurologic outcome.No case <strong>of</strong> infection was reported in ei<strong>the</strong>r group.Surgical decompression is indicated for progressive neurologicdeficits associated with compressive intracanalblood, bullet or bone fragments. In <strong>the</strong>se situations, <strong>the</strong>surgeon is lead <strong>to</strong> conclude that neural damage is activelyadvancing secondary <strong>to</strong> spinal cord compression and immediateoperation is indicated. Intracanal bullets in <strong>the</strong> lumbar<strong>spine</strong> should also be removed <strong>to</strong> improve <strong>the</strong> rate <strong>of</strong> mo<strong>to</strong>r recoveryin cauda equina level injuries. The role <strong>of</strong> decompressionand bullet removal in <strong>the</strong> cervical and thoracic levelsremains unclear, with <strong>the</strong> complications <strong>of</strong> surgery a forebodingdetrac<strong>to</strong>r. Because <strong>of</strong> <strong>the</strong> possible potential benefits <strong>of</strong>decompression, <strong>the</strong> authors sometimes elect <strong>to</strong> removecervical-level intracanal fragments, especially in incompletespinal cord injuries. In <strong>the</strong> current authors’ opinion,<strong>the</strong> possibility <strong>of</strong> even one or two levels <strong>of</strong> recovery justifies<strong>the</strong> risk <strong>of</strong> cerebrospinal leak, fistula or infection in <strong>the</strong>cervical region. This, however, would be difficult <strong>to</strong> justify in<strong>the</strong> thoracic <strong>spine</strong>, where little functional return is sacrificed.
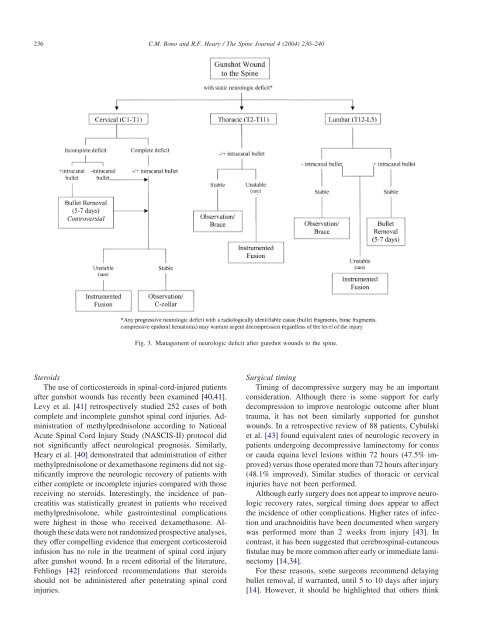
236C.M. Bono and R.F. Heary / The Spine Journal 4 (2004) 230–240Fig. 3. Management <strong>of</strong> neurologic deficit after gunshot <strong>wounds</strong> <strong>to</strong> <strong>the</strong> <strong>spine</strong>.SteroidsThe use <strong>of</strong> corticosteroids in spinal-cord-injured patientsafter gunshot <strong>wounds</strong> has recently been examined [40,41].Levy et al. [41] retrospectively studied 252 cases <strong>of</strong> bothcomplete and incomplete gunshot spinal cord injuries. Administration<strong>of</strong> methylprednisolone according <strong>to</strong> NationalAcute Spinal Cord Injury Study (NASCIS-II) pro<strong>to</strong>col didnot significantly affect neurological prognosis. Similarly,Heary et al. [40] demonstrated that administration <strong>of</strong> ei<strong>the</strong>rmethylprednisolone or dexamethasone regimens did not significantlyimprove <strong>the</strong> neurologic recovery <strong>of</strong> patients wi<strong>the</strong>i<strong>the</strong>r complete or incomplete injuries compared with thosereceiving no steroids. Interestingly, <strong>the</strong> incidence <strong>of</strong> pancreatitiswas statistically greatest in patients who receivedmethylprednisolone, while gastrointestinal complicationswere highest in those who received dexamethasone. Although<strong>the</strong>se data were not randomized prospective analyses,<strong>the</strong>y <strong>of</strong>fer compelling evidence that emergent corticosteroidinfusion has no role in <strong>the</strong> treatment <strong>of</strong> spinal cord injuryafter gunshot wound. In a recent edi<strong>to</strong>rial <strong>of</strong> <strong>the</strong> literature,Fehlings [42] reinforced recommendations that steroidsshould not be administered after penetrating spinal cordinjuries.Surgical timingTiming <strong>of</strong> decompressive surgery may be an importantconsideration. Although <strong>the</strong>re is some support for earlydecompression <strong>to</strong> improve neurologic outcome after blunttrauma, it has not been similarly supported for gunshot<strong>wounds</strong>. In a retrospective review <strong>of</strong> 88 patients, Cybulskiet al. [43] found equivalent rates <strong>of</strong> neurologic recovery inpatients undergoing decompressive laminec<strong>to</strong>my for conusor cauda equina level lesions within 72 hours (47.5% improved)versus those operated more than 72 hours after injury(48.1% improved). Similar studies <strong>of</strong> thoracic or cervicalinjuries have not been performed.Although early surgery does not appear <strong>to</strong> improve neurologicrecovery rates, surgical timing does appear <strong>to</strong> affect<strong>the</strong> incidence <strong>of</strong> o<strong>the</strong>r complications. Higher rates <strong>of</strong> infectionand arachnoiditis have been documented when surgerywas performed more than 2 weeks from injury [43]. Incontrast, it has been suggested that cerebrospinal-cutaneousfistulae may be more common after early or immediate laminec<strong>to</strong>my[14,34].For <strong>the</strong>se reasons, some surgeons recommend delayingbullet removal, if warranted, until 5 <strong>to</strong> 10 days after injury[14]. However, it should be highlighted that o<strong>the</strong>rs think