World report on child injury prevention - Unicef
World report on child injury prevention - Unicef
World report on child injury prevention - Unicef
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
<str<strong>on</strong>g>World</str<strong>on</strong>g> <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong><strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>
<str<strong>on</strong>g>World</str<strong>on</strong>g> <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong><strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>Edited byMargie Peden, Kayode Oyegbite,Joan Ozanne-Smith, Adnan A Hyder,Christine Branche, AKM Fazlur Rahman,Frederick Rivara and Kidist Bartolomeos
WHO Library Cataloguing-in-Publicati<strong>on</strong> Data:<str<strong>on</strong>g>World</str<strong>on</strong>g> <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>/ edited by Margie Peden … [et al].1.Wounds and injures - preventi<strong>on</strong> and c<strong>on</strong>trol. 2.Accident preventi<strong>on</strong>.3.Child welfare. I.<str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>.ISBN 978 92 4 156357 4 (NLM classificati<strong>on</strong>: WA 250)© <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong> 2008All rights reserved. Publicati<strong>on</strong>s of the <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong> can be obtained from WHO Press, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 20 Avenue Appia,1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: bookorders@who.int). Requests for permissi<strong>on</strong> to reproduce ortranslate WHO publicati<strong>on</strong>s – whether for sale or for n<strong>on</strong>commercial distributi<strong>on</strong> – should be addressed to WHO Press, at the above address (fax:+41 22 791 4806; e-mail: permissi<strong>on</strong>s@who.int).The designati<strong>on</strong>s employed and the presentati<strong>on</strong> of the material in this publicati<strong>on</strong> do not imply the expressi<strong>on</strong> of any opini<strong>on</strong> whatsoever <strong>on</strong> the partof the <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong> or UNICEF c<strong>on</strong>cerning the legal status of any country, territory, city or area or of its authorities, or c<strong>on</strong>cerning thedelimitati<strong>on</strong> of its fr<strong>on</strong>tiers or boundaries. Dotted lines <strong>on</strong> maps represent approximate border lines for which there may not yet be full agreement.The menti<strong>on</strong> of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the <str<strong>on</strong>g>World</str<strong>on</strong>g> HealthOrganizati<strong>on</strong> or UNICEF in preference to others of a similar nature that are not menti<strong>on</strong>ed. Errors and omissi<strong>on</strong>s excepted, the names of proprietaryproducts are distinguished by initial capital letters.All reas<strong>on</strong>able precauti<strong>on</strong>s have been taken by the <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong> or UNICEF to verify the informati<strong>on</strong> c<strong>on</strong>tained in this publicati<strong>on</strong>.However, the published material is being distributed without warranty of any kind, either expressed or implied. The resp<strong>on</strong>sibility for the interpretati<strong>on</strong>and use of the material lies with the reader. In no event shall the <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong> or UNICEF be liable for damages arising from its use.Cover design by INIS.Graphics by minimum graphics and L’IV Com Sàrl.Printed in Switzerland.
CONTENTSC<strong>on</strong>tentsForewordC<strong>on</strong>tributorsAcknowledgementsIntroducti<strong>on</strong>viiixxiiixvChapter 1. Child injuries in c<strong>on</strong>text 1Background 1What is an <strong>injury</strong>? 1Who is a <strong>child</strong>? 1Why is <strong>child</strong> <strong>injury</strong> important? 1How does <strong>child</strong> <strong>injury</strong> relate to other <strong>child</strong> health c<strong>on</strong>cerns? 2Children’s injuries and the changing world 3The characteristics of <strong>child</strong> <strong>injury</strong> 5The <strong>child</strong>-<strong>injury</strong> pyramid 5Fatal <strong>child</strong> injuries 5N<strong>on</strong>-fatal <strong>child</strong> injuries 7Child <strong>injury</strong> and age 8Child <strong>injury</strong> and gender 9Child <strong>injury</strong> and socioec<strong>on</strong>omic factors 9The preventability of <strong>child</strong> <strong>injury</strong> 12The principles of <strong>injury</strong> preventi<strong>on</strong> 12Learning from places with good safety records 16Which approaches work? 16Universal and targeted interventi<strong>on</strong>s 18Cost and cost-effectiveness 20Overcoming the obstacles 20C<strong>on</strong>clusi<strong>on</strong> 22References 22Chapter 2. Road traffic injuries 31Introducti<strong>on</strong> 31Epidemiology of road traffic injuries 31Mortality 31Morbidity 33Types of road user 34Ec<strong>on</strong>omic impact of road traffic injuries 36Limitati<strong>on</strong>s of data 36Risk factors 36Child-related factors 36Vehicle-related factors 41Envir<strong>on</strong>mental factors 41Lack of prompt treatment 41Interventi<strong>on</strong>s 42Engineering measures 42Vehicle design 43Safety equipment 43WORLD REPORT ON CHILD INJURY PREVENTION III
Legislati<strong>on</strong> and standards 46Developing educati<strong>on</strong> and skills 47Emergency and trauma care 48Potentially harmful interventi<strong>on</strong>s 49Evaluating interventi<strong>on</strong>s 49C<strong>on</strong>clusi<strong>on</strong> and recommendati<strong>on</strong>s 49Recommendati<strong>on</strong>s 49References 51Chapter 3. Drowning 59Introducti<strong>on</strong> 59Epidemiology of drowning 59Mortality 59Morbidity 62Ec<strong>on</strong>omic impact of drowning 62Limitati<strong>on</strong>s of data 63Risk factors 63Child-related factors 63Agent factors 65Envir<strong>on</strong>mental factors 66Access to treatment and rehabilitati<strong>on</strong> 66Interventi<strong>on</strong>s 66Engineering measures 67Envir<strong>on</strong>mental measures 67Legislati<strong>on</strong> and standards 68Developing educati<strong>on</strong> and skills 69Managing drowning 71Adapting interventi<strong>on</strong>s 72Further research <strong>on</strong> interventi<strong>on</strong>s 72C<strong>on</strong>clusi<strong>on</strong>s and recommendati<strong>on</strong>s 72Recommendati<strong>on</strong>s 72References 73Chapter 4. Burns 79Introducti<strong>on</strong> 79Epidemiology of burns 80Mortality 80Morbidity 81Limitati<strong>on</strong>s of data 84Risk factors 84Child-related factors 85Agent factors 86Envir<strong>on</strong>mental factors 86Protective factors 86Interventi<strong>on</strong>s 87Engineering measures 87Envir<strong>on</strong>mental measures 88Laws and regulati<strong>on</strong>s 88Educati<strong>on</strong>al approaches 89Combined strategies 89Managing burns 90Adapting interventi<strong>on</strong>s 93Evaluating interventi<strong>on</strong>s 93IV WORLD REPORT ON CHILD INJURY PREVENTION
C<strong>on</strong>clusi<strong>on</strong>s and recommendati<strong>on</strong>s 93Recommendati<strong>on</strong>s 93References 94Chapter 5. Falls 101Introducti<strong>on</strong> 101Epidemiology of falls 101Mortality 102Morbidity 102Cost of fall-related <strong>injury</strong> 105Limitati<strong>on</strong>s of data 106Risk factors 106Child-related factors 106Agent factors 107Envir<strong>on</strong>mental factors 109Lack of treatment and rehabilitati<strong>on</strong> 110Interventi<strong>on</strong>s 110Engineering measures 110Envir<strong>on</strong>mental measures 110Laws and regulati<strong>on</strong>s 111Educati<strong>on</strong>al approaches 111Combining strategies 112Adapting interventi<strong>on</strong>s 113Involving a range of sectors 114C<strong>on</strong>clusi<strong>on</strong>s and recommendati<strong>on</strong>s 114Recommendati<strong>on</strong>s 114References 115Chapter 6. Pois<strong>on</strong>ings 123Introducti<strong>on</strong> 123Epidemiology of pois<strong>on</strong>ing 123Mortality 123Morbidity 125Types of pois<strong>on</strong> 125Cost of pois<strong>on</strong>ing-related <strong>injury</strong> 127Limitati<strong>on</strong>s of data 127Risk factors 129Child-related factors 129Agent factors 130Envir<strong>on</strong>mental factors 131Lack of prompt treatment 132Interventi<strong>on</strong>s 132Engineering measures 132Envir<strong>on</strong>mental measures 134Laws and regulati<strong>on</strong>s 134Educati<strong>on</strong>al approaches 135Managing pois<strong>on</strong>ing 135Involving a range of sectors 137Evaluating interventi<strong>on</strong>s 137C<strong>on</strong>clusi<strong>on</strong>s and recommendati<strong>on</strong>s 137Recommendati<strong>on</strong>s 138References 138WORLD REPORT ON CHILD INJURY PREVENTION V
Chapter 7. C<strong>on</strong>clusi<strong>on</strong>s and recommendati<strong>on</strong>s 145Introducti<strong>on</strong> 145Main messages from the <str<strong>on</strong>g>report</str<strong>on</strong>g> 145Child injuries are a major public health issue 145Injuries directly affect <strong>child</strong> survival 145Children are more susceptible to injuries 145Child injuries can be prevented 146The cost of doing nothing is unacceptable 147Few countries have good data <strong>on</strong> <strong>child</strong> injuries 148Research <strong>on</strong> <strong>child</strong> injuries is too limited 148There are too few practiti<strong>on</strong>ers in <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> 149Child injuries is the resp<strong>on</strong>sibility of many sectors 150Child <strong>injury</strong> preventi<strong>on</strong> is underfunded 150Awareness needs to be created and maintained 150Recommended acti<strong>on</strong>s 151Translating recommendati<strong>on</strong>s into reality 153C<strong>on</strong>clusi<strong>on</strong> 154References 155Statistical annex 157Index 203VI WORLD REPORT ON CHILD INJURY PREVENTION
FOREWORDForewordEvery day around the world the lives of more than 2000 families are torn apart by the loss of a <strong>child</strong> to an unintenti<strong>on</strong>al<strong>injury</strong> or so-called “accident” that could have been prevented. The grief that these families suffer – mothers, fathers,siblings, grandparents and friends – is immeasurable and often impacts entire communities. Such tragedy can changelives irrevocably.Once <strong>child</strong>ren reach the age of five years, unintenti<strong>on</strong>al injuries are the biggest threat to their survival. Unintenti<strong>on</strong>alinjuries are also a major cause of disabilities, which can have a l<strong>on</strong>g-lasting impact <strong>on</strong> all facets of <strong>child</strong>ren’s lives:relati<strong>on</strong>ships, learning and play. Am<strong>on</strong>g those <strong>child</strong>ren who live in poverty, the burden of <strong>injury</strong> is highest, as these<strong>child</strong>ren are less likely to benefit from the protective measures others may receive.Child injuries have been neglected for many years, and are largely absent from <strong>child</strong> survival initiatives presently <strong>on</strong>the global agenda. Through this <str<strong>on</strong>g>World</str<strong>on</strong>g> <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>, the <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, the UnitedNati<strong>on</strong>s Children’s Fund and many partners have set out to elevate <strong>child</strong> <strong>injury</strong> to a priority for the global public healthand development communities. The knowledge and experience of nearly two hundred experts from all c<strong>on</strong>tinents andvarious sectors were invaluable in grounding the <str<strong>on</strong>g>report</str<strong>on</strong>g> in the realities faced in many countries.Children’s maturity and their interests and needs differ from adults. Therefore, simply reproducing <strong>injury</strong> preventi<strong>on</strong>strategies that are relevant to adults does not adequately protect <strong>child</strong>ren. There are proven interventi<strong>on</strong>s such as <strong>child</strong>car seats, cycling helmets, <strong>child</strong>-resistant packaging for medicati<strong>on</strong>s, fencing around swimming pools, hot water taptemperature regulati<strong>on</strong> and window guards, to name a few.Ministries of Health can play a central role in preventi<strong>on</strong>, advocacy and research and in the care and rehabilitati<strong>on</strong> of<strong>child</strong>ren with disabilities. Other key sectors include educati<strong>on</strong>, transportati<strong>on</strong>, envir<strong>on</strong>ment and law enforcement.This <str<strong>on</strong>g>World</str<strong>on</strong>g> <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> should be seen as a complement to the UN Secretary-General’s study <strong>on</strong>violence against <strong>child</strong>ren released in late 2006. That <str<strong>on</strong>g>report</str<strong>on</strong>g> addressed violence-related or intenti<strong>on</strong>al injuries. Both <str<strong>on</strong>g>report</str<strong>on</strong>g>ssuggest that <strong>child</strong> <strong>injury</strong> and violence preventi<strong>on</strong> programmes need to be integrated into <strong>child</strong> survival and other broadstrategies focused <strong>on</strong> improving the lives of <strong>child</strong>ren.Evidence dem<strong>on</strong>strates the dramatic successes in <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> in countries which have made a c<strong>on</strong>certedeffort. These results make a case for increasing investments in human resources and instituti<strong>on</strong>al capacities. This wouldpermit the development, implementati<strong>on</strong> and evaluati<strong>on</strong> of programmes to stem the tide of <strong>child</strong> <strong>injury</strong> and enhance thehealth and well-being of <strong>child</strong>ren and their families the world over. Implementing proven interventi<strong>on</strong>s could save morethan a thousand <strong>child</strong>ren’s lives a day.Margaret ChanDirector-General<str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>Ann M VenemanExecutive DirectorUnited Nati<strong>on</strong>s Children’s FundWORLD REPORT ON CHILD INJURY PREVENTION VII
VIII WORLD REPORT ON CHILD INJURY PREVENTION
CONTRIBUTORSC<strong>on</strong>tributorsEditorial guidanceEditorial CommitteeMargie Peden, Kayode Oyegbite, Joan Ozanne-Smith, Adnan A Hyder, Christine Branche, AKM Fazlur Rahman,Frederick Rivara, Kidist Bartolomeos.Executive EditorMargie Peden.Advisory CommitteeChair of Advisory Committee: Ala Din Abdul Sahib Alwan.Advisory Committee: Ileana Arias, Sebastian van As, Martin Eichelberger, Mehmet Haberal, Saad Houry, Etienne Krug,Douglas “Pete” Peters<strong>on</strong>, Joy Phumaphi, Wim Rogmans, Fernando Stein, Alan Whelpt<strong>on</strong>, Fan Wu.C<strong>on</strong>tributors to individual chaptersIntroducti<strong>on</strong>Writer: Alis<strong>on</strong> Harvey.Box: Alis<strong>on</strong> Harvey, Amaya Gillespie.Chapter 1. Child injuries in c<strong>on</strong>textWriters: Elizabeth Towner, Ian Scott.Boxes: Margie Peden, T<strong>on</strong>y Kahane (Juan’s story), Margie Peden (1.1), Anuradha Bose (1.2), David Sleet, BarbaraMorr<strong>on</strong>giello (1.3), Charles Mock (1.4), Karen Ashby, Ken Winkel, Julie Gilchrist (1.5).Chapter 2. Road traffic injuriesWriters: Kate McMah<strong>on</strong>, Gururaj Gopalakrishna, Mark Stevens<strong>on</strong>.Working group members: Nicola Christie, Wils<strong>on</strong> Odero, Krishnan Rajam, Junaid Razzak, Eugênia Maria SilveiraRodrigues, Chamaiparn Santikarn, Isabelle Sévédé-Bardem, Jean van Wetter.Boxes: David Blanchard (Deana’s story), AKM Fazlur Rahman (2.1), Flaura Winst<strong>on</strong> (2.2), Mirjam Sidik (2.3).Chapter 3. DrowningWriters: Gitanjali Taneja, Ed van Beeck, Ruth Brenner.Working group members: Alfredo Celis, Steve Beerman, Julie Gilchrist, Olive Kobusingye, J<strong>on</strong>ath<strong>on</strong> Passmore, LindaQuan, Aminur Rahman, Carolyn Staines, Biruté Strukcinskiene, Li Yang.Boxes: Safekids New Zealand (Ruby’s story), Alfredo Celis, Frederick Rivara (3.1), Erin Cassell (3.2), Ruth Brenner,Gitanjali Taneja (3.3), Joan Ozanne-Smith (3.4), Frederick Rivara (3.5).Chapter 4. BurnsWriters: Samuel Forjuoh, Andrea Gielen.Working group members: Carlos Arreola-Rissa, Mohamoud El-Oteify, Alis<strong>on</strong> Macphers<strong>on</strong>, Ashley van Niekerk, MichaelPeck, Andrés Villaveces.Boxes: Children of Fire (Vusi’s story), Samuel Forjuoh (4.1), Reza Mohammadi, Homayoun Sadeghi-Bazargani, MohammadMehdi Gouya (4.2), Wijaya Godakumbura (4.3), Pam Albany (4.4), Junaid Razzak (4.5), Rene Albertyn, Sebastian vanAs, Heinz Rode (4.6).WORLD REPORT ON CHILD INJURY PREVENTION IX
Chapter 5. FallsWriters: Shanthi Ameratunga, Huan Linnan, Shaheen Sultana.Working group members: Francis Abantanga, Abdulbari Bener, Rieneke Dekker, Adisak Plitapolkarnpim, Shauna Sherker,Wendy Wats<strong>on</strong>.Boxes: Aminur Rahman (Sohel’s story), Kidist Bartolomeos, Baltazar Chilundo, Orvalho Joaquim (5.1), Caroline Finch(5.2), Joan Ozanne-Smith (5.3), Margie Peden (5.4).Chapter 6. Pois<strong>on</strong>sWriters: Yvette Holder, Richard Matzopoulos, Nerida Smith.Working group members: Mick Ballesteros, Anuradha Bose, Jenny Pr<strong>on</strong>czuk de Garbino, Marisa Ricardo, Dinesh Sethi,Nelmarie du Toit.Boxes: Debbie Scott (Harris<strong>on</strong>’s story), Ken Winkel, Karen Ashby, Julie Gilchrist (6.1), Richard Matzopoulos (6.2), YvetteHolder (6.3), Fernando Ravindra (6.4).Chapter 7. C<strong>on</strong>clusi<strong>on</strong>s and Recommendati<strong>on</strong>sWriters: Margie Peden, Adnan A Hyder.Boxes: Anupama Kumar (Anupama’s story), Lucie Laflamme (7.1), Adnan A Hyder, Nhan Tran, Abdulgafoor Bachani,David Bishai (7.2), Susan McKenzie (7.3), David Meddings (7.4), Ver<strong>on</strong>ika Benešová (7.5), Margie Peden (7.6).Statistical AnnexKidist Bartolomeos, Colin Douglas Mathers, Karen Oldenziel, Mike Linnan, Adnan A Hyder.Peer reviewersPam Albany, Rene Albertyn, Ruth Barker, Chris Brewster, Mariana Bruss<strong>on</strong>i, Marie Noël Brune, Erin Cassel, KerryChausmer, Chrissy Cianfl<strong>on</strong>e, Ann Dillenger, Moira D<strong>on</strong>ahue, Jacquie Dukehart, Martin Eichelberger, Robert Flanagan,Lucie Laflamme, Abdul Ghaffar, Rosa Gofin, Robin Ikeda, Denise Kendrick, Shyan Lall, Jacques Latarjet, EdilbertoLoaiza, Morag Mackay, Alis<strong>on</strong> Macphers<strong>on</strong>, Candida Moshiro, Milt<strong>on</strong> Mutto, Anth<strong>on</strong>y Oliver, Luciana O’Reilly, DavidParker, Eleni Petridou, Dragoslav Popovic, Aminur Rahman, Shum<strong>on</strong>a Shafinaz, David Silcock, David Sleet, HamidSoori, Joanna Tempowski, Maria Vegega, Andrés Villaveces, Joanne Vincenten, Diane Wigle.Additi<strong>on</strong>al c<strong>on</strong>tributorsRegi<strong>on</strong>al C<strong>on</strong>sultantsWHO African Regi<strong>on</strong> / Eastern Mediterranean Regi<strong>on</strong>Francis Abantanga, Hala Aboutaleb, Wahid Al-Kharusi, Jamela Al Raiby, Sebastian van As, Abdulbari Bener, HeshamEl-Sayed, Mahmoud El-Oteify, Mouloud Haddak, Lara Hussein, Syed Jaffar Hussain, Olive Kobusingye, RichardMatzopoulos, Candida Moshiro, Junaid Razzak, Jamil Salim, Babatunde Solagberu, Hamid Soori, Dehran Swart.WHO Regi<strong>on</strong> of the AmericasCarlos Arreola-Rissa, Sim<strong>on</strong>e G<strong>on</strong>çalves de Assis, Yadira Carrer, Alfredo Celis, Sara Diaz, Ann Dellinger, SamuelForjuoh, Andrea Gielen, Maria Isabel Gutierrez, Yvette Holder, Debra Houry, Sylvain Leduc, Luciana O’Reilly, MichaelPeck, Maria Fernanda Tourinho Peres, Eugênia Maria Silveira Rodrigues, Maria Ines Romero, Gitanjali Taneja, AndrésVillaveces, Billie Weiss, Elizabeth Ward.WHO South-East Asia Regi<strong>on</strong> / Western Pacific Regi<strong>on</strong>Pamela Albany, Shanthi Ameratunga, Nguyen Tr<strong>on</strong>g An, Anuradha Bose, Rafael C<strong>on</strong>sunji, Yoshikazu Fujisawa, WijayaGodakumbura, Gopalakrishna Gururaj, Huan Linnan, Michael Linnan, Hisashi Ogawa, Joan Ozanne-Smith, J<strong>on</strong>ath<strong>on</strong>Passmore, Adisak Plitp<strong>on</strong>karnpim, AKM Fazlur Rahman, Aminur Rahman, Krishnan Rajam, Marisa Ricardo, SiriwanSantijiarakul, Chamaiparn Santikarn, Ian Scott, Isabelle Sévédé-Bardem, Richard Tan, Tetsuro Tanaka.X WORLD REPORT ON CHILD INJURY PREVENTION
WHO European Regi<strong>on</strong>Ed van Beeck, Ver<strong>on</strong>ika Benešová, Christine Branche, Gudula Brandmayr, Murat Derbent, Olivier Duperrex, Rosa Gofin,Loek Hesemans, Rupert Kisser, Lucie Laflamme, Jacques Latarjet, Morag Mackay, Alis<strong>on</strong> Macphers<strong>on</strong>, Kate McMah<strong>on</strong>,Eleni Petridou, Dragoslav Popovic, Olga Poyiadji-Kalakouta, Francesca Racioppi, Ian Roberts, Wim Rogmans, Maria SeguiGomez, Dinesh Sethi, Biruté Strukcinskiene, Elizabeth Towner, Iva Truellova, Joanne Vincenten, Michael Wats<strong>on</strong>.N<strong>on</strong>e of the experts involved in the development of this <str<strong>on</strong>g>report</str<strong>on</strong>g> declared any c<strong>on</strong>flict of interest.WORLD REPORT ON CHILD INJURY PREVENTION XI
XII WORLD REPORT ON CHILD INJURY PREVENTION
ACKNOWLEDGEMENTSAcknowledgementsThe <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong> and UNICEF would like to thank the more than 180 c<strong>on</strong>tributors (editors, lead authors,working group members, regi<strong>on</strong>al c<strong>on</strong>sultati<strong>on</strong> participants and peer reviewers) to this <str<strong>on</strong>g>report</str<strong>on</strong>g> from 56 countries aroundthe world. In additi<strong>on</strong>, the support and guidance offered by the <str<strong>on</strong>g>report</str<strong>on</strong>g> advisors, WHO regi<strong>on</strong>al advisors and UNICEFstaff are acknowledged. Without their dedicati<strong>on</strong>, support and expertise this <str<strong>on</strong>g>report</str<strong>on</strong>g> would not have been possible.The <str<strong>on</strong>g>report</str<strong>on</strong>g> also benefited from the c<strong>on</strong>tributi<strong>on</strong> of a number of other people, in particular, T<strong>on</strong>y Kahane whoedited the final text of the main <str<strong>on</strong>g>report</str<strong>on</strong>g> and Angela Burt<strong>on</strong> who edited the summary versi<strong>on</strong>. Joanne Vincenten andMorag Mackay prepared the final text for the summary and fact sheets. Thanks are also due to the following: KidistBartolomeos and Ian Scott for the day-to-day coordinati<strong>on</strong> of the project; Mike Linnan for the UNICEF/TASC dataanalysis; Kidist Bartolomeos, Colin Mathers and Karen Oldenziel for analysis and interpretati<strong>on</strong> of WHO data; AdnanHyder and Prasanthi Puvanachandra for data analysis from the multicountry study; Laura Sminkey and Steven Lauwersfor communicati<strong>on</strong> and advocacy; Susan Kaplan for proofreading and Liza Furnival for indexing; Susan Hobbs, L’IVCom Sàrl and Aar<strong>on</strong> Andrade for graphic design; Pascale Broisin and Frederique Robin-Wahlin for coordinating theprinting; and finally, Pascale Lanvers-Casasola for her administrative support and for coordinating the translati<strong>on</strong> of thedifferent versi<strong>on</strong>s of this <str<strong>on</strong>g>report</str<strong>on</strong>g>.The <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong> and UNICEF also wish to thank the following for their generous financial support forthe development, translati<strong>on</strong> and publicati<strong>on</strong> of the <str<strong>on</strong>g>report</str<strong>on</strong>g>: the Arab Gulf Programme for United Nati<strong>on</strong>s DevelopmentOrganizati<strong>on</strong>s (AGFUND); the Public Health Agency of Canada, the Governments of Belgium, Mexico, the Netherlands,Norway, Sweden, and the United Kingdom; the Global Forum for Health Research; the United States Centers for DiseaseC<strong>on</strong>trol and Preventi<strong>on</strong>, Nati<strong>on</strong>al Center for Injury Preventi<strong>on</strong> and C<strong>on</strong>trol.WORLD REPORT ON CHILD INJURY PREVENTION XIII
XIV WORLD REPORT ON CHILD INJURY PREVENTION
INTRODUCTIONIntroducti<strong>on</strong>Child injuries are a growing global public health problem.They are a significant area of c<strong>on</strong>cern from the age of<strong>on</strong>e year, and progressively c<strong>on</strong>tribute more to overallrates of death until <strong>child</strong>ren reach adulthood. Hundredsof thousands of <strong>child</strong>ren die each year from injuries orviolence, and milli<strong>on</strong>s of others suffer the c<strong>on</strong>sequencesof n<strong>on</strong>-fatal injuries. For each area of <strong>child</strong> <strong>injury</strong> there areproven ways to reduce both the likelihood and severity of<strong>injury</strong> – yet awareness of the problem and its preventability,as well as political commitment to act to prevent <strong>child</strong><strong>injury</strong>, remain unacceptably low.Main causes of death am<strong>on</strong>g <strong>child</strong>ren, <str<strong>on</strong>g>World</str<strong>on</strong>g>, 2004Percentage of deathsa100806040200Under 1 1–4 5–9 10–14 15–19Age (years)Injuries N<strong>on</strong>communicable diseases Communicable diseases aIncludes communicable, maternal, perinatal and nutriti<strong>on</strong>al c<strong>on</strong>diti<strong>on</strong>s.Source: WHO (2008), Global Burden of Disease: 2004 update.In 2005, WHO and UNICEF issued a call for a greatlyexpanded global effort to prevent <strong>child</strong> <strong>injury</strong> (1). Thiswas followed in 2006 by WHO’s ten-year plan of acti<strong>on</strong> <strong>on</strong><strong>child</strong> <strong>injury</strong> (2). The plan listed objectives, activities andexpected outcomes <strong>on</strong> <strong>child</strong> <strong>injury</strong> and covered the fieldsof data, research, preventi<strong>on</strong>, services, capacity buildingand advocacy.This joint WHO/UNICEF <str<strong>on</strong>g>World</str<strong>on</strong>g> <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> <strong>child</strong> <strong>injury</strong>preventi<strong>on</strong> brings together all that is currently knownabout the various types of <strong>child</strong> injuries and how to preventthem. At the same time, it recognizes that there are majorgaps in knowledge. The <str<strong>on</strong>g>report</str<strong>on</strong>g> expands <strong>on</strong> and strengthensthe areas of acti<strong>on</strong> set out in the 2005 Global call to acti<strong>on</strong>and the WHO ten-year plan. It is intended, furthermore,to help transfer knowledge into practice, so that what hasproven effective in decreasing the burden of <strong>child</strong> injuriesin some countries can be adapted and implemented inothers, with similar results.The <str<strong>on</strong>g>World</str<strong>on</strong>g> <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> is directedat researchers, public health specialists, practiti<strong>on</strong>ers andacademics. A summary of the <str<strong>on</strong>g>report</str<strong>on</strong>g> c<strong>on</strong>taining the mainmessages and recommendati<strong>on</strong>s and a set of fact sheetsare available for policy-makers and development agencies.A versi<strong>on</strong> aimed at <strong>child</strong>ren – to create awareness andprovide <strong>child</strong>ren with a sense of ownership of the issues –and a set of posters have also been produced.AimsThe overall aims of the <str<strong>on</strong>g>report</str<strong>on</strong>g> are:– to raise awareness about the magnitude, risk factorsand impacts of <strong>child</strong> injuries globally;– to draw attenti<strong>on</strong> to the preventability of <strong>child</strong> injuriesand present what is known about the effectiveness ofinterventi<strong>on</strong> strategies;– to make recommendati<strong>on</strong>s that can be implemented byall countries to reduce <strong>child</strong> injuries effectively.Definiti<strong>on</strong> of <strong>child</strong>hoodThere is no universally agreed age range for what c<strong>on</strong>stitutes<strong>child</strong>hood – a c<strong>on</strong>cept that varies c<strong>on</strong>siderably acrosscultures. This <str<strong>on</strong>g>report</str<strong>on</strong>g> uses the definiti<strong>on</strong> of a <strong>child</strong> specifiedin the C<strong>on</strong>venti<strong>on</strong> <strong>on</strong> the Rights of the Child (3), and thusfocuses <strong>on</strong> injuries occurring in <strong>child</strong>ren “under the age of18 years”. However, it has not always been possible to reflectthis age cut-off in analysing data. The reader will notice,for instance, that in some cases WHO data could not bedisaggregated to
The UN Secretary-General’s Study <strong>on</strong> Violence against Children: a joint initiativeof UNICEF, WHO, OHCHR and ILOThis in-depth study was presented to the United Nati<strong>on</strong>s General Assembly in 2006 by an independent expert appointed by the Secretary-General tolead the effort. Supported by UNICEF, WHO, OHCHR, ILO and a wide network of n<strong>on</strong>governmental organizati<strong>on</strong>s, the study provided a global picture ofviolence against <strong>child</strong>ren, with recommendati<strong>on</strong>s to prevent and deal with such violence. The study examined violence against <strong>child</strong>ren in differentsettings: the family, school, community, alternative care instituti<strong>on</strong>s, detenti<strong>on</strong> facilities and places where <strong>child</strong>ren work. Experts from the fields ofhuman rights, public health and <strong>child</strong> protecti<strong>on</strong> all collaborated in this pi<strong>on</strong>eering <str<strong>on</strong>g>report</str<strong>on</strong>g>.Despite progress in preventing violence against <strong>child</strong>ren, much remains to be d<strong>on</strong>e, and several factors limit the impact of preventive measures.These include the lack of c<strong>on</strong>sistent data and incomplete knowledge of the root causes of violence against <strong>child</strong>ren. Furthermore, efforts to addressviolence against <strong>child</strong>ren are frequently reactive, focusing <strong>on</strong> symptoms and c<strong>on</strong>sequences rather than causes. Strategies tend to be fragmented, asopposed to integrated, and insufficient resources are allocated to address the problems. In additi<strong>on</strong>, internati<strong>on</strong>al commitments to protect <strong>child</strong>renfrom violence are often not translated into acti<strong>on</strong> at the nati<strong>on</strong>al level.The core message of the Secretary-General’s study is that no violence against <strong>child</strong>ren is justifiable; all violence against <strong>child</strong>ren is preventable. Whilegovernments have made commitments to protect <strong>child</strong>ren from all forms of violence, research and <strong>child</strong> testim<strong>on</strong>ies show that these commitmentsare far from being fulfilled. The legal obligati<strong>on</strong>s lie with governments. However, all sectors of society share the resp<strong>on</strong>sibility to c<strong>on</strong>demn andprevent violence against <strong>child</strong>ren and to deal with those <strong>child</strong>ren affected.The c<strong>on</strong>sequences of violence against <strong>child</strong>ren vary according to its nature and severity. Efforts to prevent and resp<strong>on</strong>d to such violence must thereforebe multifaceted. They must reflect the type of violence, the setting and the nature of the perpetrator or perpetrators, and they must always takeinto account the best interests of the <strong>child</strong>.The principal recommendati<strong>on</strong>s of the study were:1. to strengthen nati<strong>on</strong>al and local commitment and acti<strong>on</strong>;2. to prohibit all violence against <strong>child</strong>ren (including the death penalty, corporal punishment, harmful traditi<strong>on</strong>al practices, sexual violence,torture and other cruel, inhuman or degrading treatment or punishment);3. to make preventi<strong>on</strong> of violence against <strong>child</strong>ren a priority;4. to promote n<strong>on</strong>-violent values and raise awareness of violence;5. to enhance the capacity of all who work with and for <strong>child</strong>ren;6. to provide services for recovery and social reintegrati<strong>on</strong>;7. to ensure the participati<strong>on</strong> of <strong>child</strong>ren;8. to create accessible and <strong>child</strong>-friendly <str<strong>on</strong>g>report</str<strong>on</strong>g>ing systems and services;9. to ensure accountability and put an end to violence against <strong>child</strong>ren going unpunished;10. to address the gender dimensi<strong>on</strong> of violence against <strong>child</strong>ren;11. to develop and implement systematic nati<strong>on</strong>al data collecti<strong>on</strong> and research;12. to strengthen internati<strong>on</strong>al commitment <strong>on</strong> the issue of violence against <strong>child</strong>ren.Source: The United Nati<strong>on</strong>s Secretary General’s Study <strong>on</strong> Violence Against Children (http://www.violencestudy.org/r25, accessed 19 May 2008).This <str<strong>on</strong>g>World</str<strong>on</strong>g> <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> c<strong>on</strong>sists ofseven main chapters. Chapter 1 places <strong>child</strong> injuries in thec<strong>on</strong>text of other health c<strong>on</strong>cerns and related global issuesand discusses the fundamentals of <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>.Chapters 2 through 6 examine the five major mechanismsof <strong>child</strong> injuries: road traffic injuries, drowning, burns,falls and pois<strong>on</strong>ings. Each of these chapters reviews theepidemiology, the risk factors, the interventi<strong>on</strong>s and theeffectiveness of interventi<strong>on</strong>s, and c<strong>on</strong>cludes with someimportant strategies to prevent or manage the particulartype of <strong>injury</strong>. Chapter 7 draws together the comm<strong>on</strong>themes of earlier chapters. It also presents a set of broadrecommendati<strong>on</strong>s that governments and others c<strong>on</strong>cernedshould seriously c<strong>on</strong>sider implementing so as to beginreducing the burden of <strong>child</strong> injuries.In deciding which topics to include in this <str<strong>on</strong>g>report</str<strong>on</strong>g>, theeditors were guided by the overall magnitude of each typeof <strong>injury</strong> as presented in WHO’s Global Burden of DiseaseProject for 2004. C<strong>on</strong>sequently, smothering – although asignificant problem in infants – has not been included asa full chapter in the <str<strong>on</strong>g>report</str<strong>on</strong>g> because global data is scant.Similarly, bites and stings have been addressed throughboxes within other chapters as these injuries tend to behighly specific to certain regi<strong>on</strong>s and global data, again,are not readily available.This <str<strong>on</strong>g>report</str<strong>on</strong>g> relies heavily <strong>on</strong> the certain data sources,including: the WHO Global Burden of Disease project for2004, the Global School Health Survey, and the UNICEF/The Alliance for Safe Children community-based studiesc<strong>on</strong>ducted in Asia. No single database is perfect. However,optimal use is made of the available data, supplementedwith informati<strong>on</strong> from published literature. The limitati<strong>on</strong>sof the data are discussed briefly in each of the chapters. Amore detailed overview of the methodologies employed togather data for the various databases is presented in theStatistical Annex at the end of this <str<strong>on</strong>g>report</str<strong>on</strong>g>.ProcessThe development of this <str<strong>on</strong>g>report</str<strong>on</strong>g> was led by an AdvisoryCommittee and an Editorial Board and has taken placeXVI WORLD REPORT ON CHILD INJURY PREVENTION
over nearly three years. Based <strong>on</strong> outlines prepared by theEditorial Board, each chapter was written by two or threeauthors working with a small team of experts from aroundthe world. Nearly 200 professi<strong>on</strong>als from various sectorsand all the regi<strong>on</strong>s of world provided input to the <str<strong>on</strong>g>report</str<strong>on</strong>g>.The examples of good practice provided in each ofthe topic-specific chapters (Chapters 2 to 6) and thesubsequent recommendati<strong>on</strong>s made for each chapter werebased <strong>on</strong> rigorous scientific evidence supplemented, wherenecessary, with “grey literature”. Based <strong>on</strong> the literaturereviewed, evidence was graded as: effective, promising,insufficient evidence, ineffective or potentially harmful.Randomized c<strong>on</strong>trolled trials and case–c<strong>on</strong>trol studieswere used as the gold standard. Where study methodologieswere robust but they were limited to a few high-incomecountries they were classified as promising. Where therewas clear evidence that the interveni<strong>on</strong> did not work orwas harmful, these were classified as ineffective andpotentially harmfull, respectively. For many interventi<strong>on</strong>sin the area of <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> there is simplyinsufficient evidence.The drafts of specific chapters were reviewed andrevised following input from four regi<strong>on</strong>al c<strong>on</strong>sultati<strong>on</strong>sorganized by the WHO regi<strong>on</strong>al offices – involving localexperts, practiti<strong>on</strong>ers and government officials – as well asinput from a set of external peer reviewers.During the regi<strong>on</strong>al c<strong>on</strong>sultati<strong>on</strong>s, experts had theopportunity to propose overall recommendati<strong>on</strong>s <strong>on</strong><strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>, for inclusi<strong>on</strong> in Chapter 7. Theirproposals were then refined by the editors based <strong>on</strong>evidence of good practice, subjected to external peer reviewand finally approved by WHO and UNICEF, who advised<strong>on</strong> the <str<strong>on</strong>g>report</str<strong>on</strong>g>. It is anticipated that the recommendati<strong>on</strong>sin this <str<strong>on</strong>g>report</str<strong>on</strong>g> will remain valid until 2018. At that time,the Department of Violence and Injury Preventi<strong>on</strong> andDisability at WHO headquarters in Geneva will initiate areview of the document.Moving forwardThis comprehensive global <str<strong>on</strong>g>report</str<strong>on</strong>g> is an important stepin advancing the field of <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>, but itis <strong>on</strong>ly <strong>on</strong>e such step. It is the hope of WHO, UNICEFand all involved in the <str<strong>on</strong>g>report</str<strong>on</strong>g> that its launch will lead togreater awareness around the world and a much increasedpolitical will for acti<strong>on</strong> at all levels to combat the scourgeof <strong>child</strong> injuries.References1. Child and adolescent <strong>injury</strong> preventi<strong>on</strong>: a global call to acti<strong>on</strong>.Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong> and UNICEF, 2005(http://whqlibdoc.who.int/publicati<strong>on</strong>s/2005/9241593415_eng.pdf, accessed 21 January 2008).2. Child and adolescent <strong>injury</strong> preventi<strong>on</strong>: a WHO plan ofacti<strong>on</strong>. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2006 (http://whqlibdoc.who.int/publicati<strong>on</strong>s/2006/9241593385_eng.pdf,accessed 21 January 2008).3. C<strong>on</strong>venti<strong>on</strong> <strong>on</strong> the Rights of the Child, 1989. New York, NY,United Nati<strong>on</strong>s, 1989 (A/RES/44/25) (http://www.unhchr.ch/html/menu3/b/k2crc.htm, accessed 21 January 2008).4. Report of the independent expert for the United Nati<strong>on</strong>s study<strong>on</strong> violence against <strong>child</strong>ren. New York, NY, United Nati<strong>on</strong>s,29 August 2006 (A/61/299) (http://www.violencestudy.org/IMG/pdf/English-2-2.pdf, accessed 21 January 2008).5. Pinheiro PS. <str<strong>on</strong>g>World</str<strong>on</strong>g> <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> violence against <strong>child</strong>ren.Geneva, Switzerland, United Nati<strong>on</strong>s Secretary-General’sStudy <strong>on</strong> Violence against Children, 2006 (http://www.violencestudy.org/a553, accessed 21 January 2008).6. Krug EG et al., eds. <str<strong>on</strong>g>World</str<strong>on</strong>g> <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> violence and health.Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2002 (http://www.who.int/violence_<strong>injury</strong>_preventi<strong>on</strong>/violence/world_<str<strong>on</strong>g>report</str<strong>on</strong>g>/en/full_en.pdf, accessed 21 January 2008).WORLD REPORT ON CHILD INJURY PREVENTION XVII
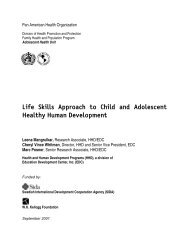
© WHOJuan lives with his mother,father, four youngerbrothers and two youngersisters in a small villageoutside Merida, in Mexico.Aged 14 years, Juan nol<strong>on</strong>ger goes to school,as he has to help hisfather selling fruit at theroadside.O VERVIEWJUAN’S STORYThe reas<strong>on</strong> that he left school is related to a terrible accident that the youngest inthe family, Martha, suffered 18 m<strong>on</strong>ths ago.Martha – six years old at the time – had fallen into the water well in the back yardof the family house, while trying to retrieve a toy that she had dropped into it. Juanwas the fi rst <strong>on</strong>to the scene of the incident and had called for his father who wasfurther up the road selling fruit. The two of them ran to the nearest clinic holdingMartha, who was limp and not crying. The doctors managed to resuscitate herbut she remained in a critical c<strong>on</strong>diti<strong>on</strong> and needed to be transferred to a largerhospital in Merida, where she stayed for many weeks.Juan went to visit his sister <strong>on</strong>ce in hospital, but did not like it there as he saidthat the hospital had a strange odour. He preferred to stay at home with hisgrandmother and help with the other <strong>child</strong>ren while his mother stayed at thehospital with Martha.Martha is a beautiful girl, who is now mentally disabled and needs assistance withall her daily needs.Juan is still very affected by this incident. He feels resp<strong>on</strong>sible for Martha’s fall intothe well, c<strong>on</strong>vinced that it would not have happened if he had been there. At thesame time, he is proud to show visitors the wooden c<strong>on</strong>structi<strong>on</strong> he and his fathermade to put over the well, to prevent a similar incident occurring.
CHAPTER 1 – CHILD INJURIES IN CONTEXTChapter 1Child injuries in c<strong>on</strong>textBackgroundEvery <strong>child</strong> in the world matters. The landmarkC<strong>on</strong>venti<strong>on</strong> <strong>on</strong> the Rights of the Child, ratified by almostall governments, states that <strong>child</strong>ren around the worldhave a right to a safe envir<strong>on</strong>ment and to protecti<strong>on</strong>from <strong>injury</strong> and violence. It further states that theinstituti<strong>on</strong>s, services and facilities resp<strong>on</strong>sible for thecare or protecti<strong>on</strong> of <strong>child</strong>ren should c<strong>on</strong>form withestablished standards, particularly in the areas of safetyand health. Safeguarding these rights everywhere is noteasy, but it can be achieved by c<strong>on</strong>certed acti<strong>on</strong>. Childrenare exposed to hazards and risks as they go about theirdaily lives and are vulnerable everywhere to the sametypes of <strong>injury</strong>. However, the physical, social, cultural,political and ec<strong>on</strong>omic envir<strong>on</strong>ments in which they livediffer greatly. Their particular envir<strong>on</strong>ments are thusvery important.This chapter provides an overview for the <str<strong>on</strong>g>report</str<strong>on</strong>g>. Thefirst secti<strong>on</strong> sets the scene, examining why <strong>child</strong> <strong>injury</strong> isimportant, how the issue relates to other c<strong>on</strong>cerns about<strong>child</strong>ren, and why there is an urgency to tackle it. Thesec<strong>on</strong>d secti<strong>on</strong> examines major features of the problem:the multiple types and causes of <strong>injury</strong> to <strong>child</strong>ren, andthe associati<strong>on</strong>s between <strong>injury</strong> and age, gender and arange of socioec<strong>on</strong>omic factors. The third secti<strong>on</strong> seeksto show that <strong>child</strong> <strong>injury</strong> is preventable. It describes theprinciples of <strong>injury</strong> preventi<strong>on</strong>, the types of approachesthat are successful and the problem of adapting proveninterventi<strong>on</strong>s to different settings. It also discusses thecost and cost-effectiveness of interventi<strong>on</strong>s to prevent<strong>child</strong> <strong>injury</strong>. The final secti<strong>on</strong> summarizes some of theobstacles in this field and the approaches to overcomingthem.What is an <strong>injury</strong>?Throughout the <str<strong>on</strong>g>report</str<strong>on</strong>g>, an <strong>injury</strong> is defined as “thephysical damage that results when a human body issuddenly subjected to energy in amounts that exceed thethreshold of physiological tolerance – or else the result of alack of <strong>on</strong>e or more vital elements, such as oxygen” (1). Theenergy in questi<strong>on</strong> can be mechanical, thermal, chemicalor radiated.As discussed in the introductory secti<strong>on</strong>, the focus ofthis <str<strong>on</strong>g>report</str<strong>on</strong>g> is <strong>on</strong> unintenti<strong>on</strong>al injuries: traffic injuries,drowning, pois<strong>on</strong>ings, burns and falls. For moreinformati<strong>on</strong> <strong>on</strong> intenti<strong>on</strong>al <strong>injury</strong>, see the <str<strong>on</strong>g>World</str<strong>on</strong>g> <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong>violence against <strong>child</strong>ren (2).Who is a <strong>child</strong>?This <str<strong>on</strong>g>report</str<strong>on</strong>g> uses the definiti<strong>on</strong> of the United Nati<strong>on</strong>sC<strong>on</strong>venti<strong>on</strong> <strong>on</strong> the Rights of the Child, Article 1: “a <strong>child</strong>means every human being below the age of 18 years” (3).Other c<strong>on</strong>cepts related to <strong>child</strong>ren, though, are more fluid.“Childhood” is a social c<strong>on</strong>structi<strong>on</strong>, whose boundariesshift with time and place (4, 5) and this has implicati<strong>on</strong>s forvulnerability to <strong>injury</strong>. A 10-year-old in <strong>on</strong>e country maybe protected from ec<strong>on</strong>omic and domestic resp<strong>on</strong>sibilities,but in another country these tasks may be the norm andc<strong>on</strong>sidered beneficial for both the <strong>child</strong> and the family (6).Thus, <strong>child</strong>hood and developmental stages are intertwinedwith age, sex, family and social background, school, workand culture (6, 7). Rather than being rigidly measured,they should be viewed through “c<strong>on</strong>text, culture andcompetences” (8).Why is <strong>child</strong> <strong>injury</strong> important?Childhood <strong>injury</strong> is a major public health problem thatrequires urgent attenti<strong>on</strong>. Injury and violence is a majorkiller of <strong>child</strong>ren throughout the world, resp<strong>on</strong>sible forabout 950 000 deaths in <strong>child</strong>ren and young people under theage of 18 years each year (WHO Global Burden of Disease:2004 update). Unintenti<strong>on</strong>al injuries account for almost90% of these cases. They are the leading cause of death for<strong>child</strong>ren aged 10–19 years. Table 1.1 shows the c<strong>on</strong>tributi<strong>on</strong>sthat the various types of unintenti<strong>on</strong>al injuries make to theleading causes of death am<strong>on</strong>g <strong>child</strong>ren. Road traffic injuriesal<strong>on</strong>e are the leading cause of death am<strong>on</strong>g 15–19-yearoldsand the sec<strong>on</strong>d leading cause am<strong>on</strong>g 10–14-year-olds.In additi<strong>on</strong> to the deaths, tens of milli<strong>on</strong>s of <strong>child</strong>renrequire hospital care for n<strong>on</strong>-fatal injuries. Many areleft with some form of disability, often with lifel<strong>on</strong>gc<strong>on</strong>sequences. Table A.2 in the Statistical Annex showsthe leading causes of disability-adjusted life years (DALYs)lost for <strong>child</strong>ren aged 0–14 years, with road traffic crashesand falls ranking in the top 15 causes.The burden of <strong>injury</strong> <strong>on</strong> <strong>child</strong>ren falls unequally. Itis heaviest am<strong>on</strong>g the poor with the burden greatest <strong>on</strong><strong>child</strong>ren in the poorer countries with lower incomes (seeTable A.1 and A.2 in the Statistical Annex). Within allcountries, the burden is greatest <strong>on</strong> those from low-incomefamilies. Overall, more than 95% of all <strong>injury</strong> deathsin <strong>child</strong>ren occur in low-income and middle-incomecountries. Although the <strong>child</strong> <strong>injury</strong> death rate is muchlower am<strong>on</strong>g <strong>child</strong>ren from developed countries, injuriesare still a major cause of death, accounting for about 40%of all <strong>child</strong> deaths (WHO Global Burden of Disease: 2004update).WORLD REPORT ON CHILD INJURY PREVENTION 1
TABLE 1.1Leading causes of death in <strong>child</strong>ren, both sexes, <str<strong>on</strong>g>World</str<strong>on</strong>g>, 2004Rank Under 1 year 1–4 years 5–9 years 10–14 years 15–19 years Under 201 Perinatal Lower respiratory Lower respiratory Lower respiratory Road traffi c Perinatalcauses infecti<strong>on</strong>s infecti<strong>on</strong>s infecti<strong>on</strong>s injuries causes2 Diarrhoeal Diarrhoeal Road traffic Road traffic Self-inflicted Lower respiratorydiseases diseases injuries injuries injuries infecti<strong>on</strong>s3 Lower respiratory Measles Malaria Drowning Violence Diarrhoealinfecti<strong>on</strong>sdiseases4 Malaria Malaria Diarrhoeal Malaria Lower respiratory Malariadiseasesinfecti<strong>on</strong>s5 C<strong>on</strong>genital HIV/AIDS Meningitis Meningitis Drowning Measlesanomalies6 Pertussis C<strong>on</strong>genital Drowning HIV/AIDS Tuberculosis C<strong>on</strong>genitalanomaliesanomalies7 HIV/AIDS Protein–energy Protein–energy Tuberculosis Fire-related HIV/AIDSmalnutriti<strong>on</strong> malnutriti<strong>on</strong> burns8 Tetanus Drowning Measles Diarrhoeal HIV/AIDS Road trafficdiseasesinjuries9 Meningitis Road traffic Tuberculosis Protein–energy Leukaemia Pertussisinjuriesmalnutriti<strong>on</strong>10 Measles Meningitis HIV/AIDS Self-inflicted Meningitis Meningitisinjuries11 Protein–energy Fire-related Fire-related Leukaemia Maternal Drowningmalnutriti<strong>on</strong> burns burns haemorrhage12 Syphilis Pertussis Falls Fire-related Falls Protein–energyburnsmalnutriti<strong>on</strong>13 Endocrine Tuberculosis C<strong>on</strong>genital War Pois<strong>on</strong>ings Tetanusdisordersanomalies14 Tuberculosis Upper respiratory Epilepsy Violence Aborti<strong>on</strong> Tuberculosisinfecti<strong>on</strong>s15 Upper respiratory Syphilis Leukaemia Trypanosomiasis Epilepsy Fire-relatedinfecti<strong>on</strong>sburnsSource: WHO (2008), Global Burden of Disease: 2004 update.Injuries are not inevitable; they can be preventedor c<strong>on</strong>trolled. In the Organisati<strong>on</strong> for Ec<strong>on</strong>omic Cooperati<strong>on</strong>and Development (OECD) countries, forexample, the number of <strong>injury</strong> deaths am<strong>on</strong>g <strong>child</strong>renunder the age of 15 years fell by half between 1970 and1995 (9). Until recently, little attenti<strong>on</strong> had been paidto the issue of injuries in low-income and middleincomecountries. The lack of awareness of the problem,compounded by the particular circumstances that thesecountries face, has meant that proven measures have notbeen implemented to the same extent as they have inhigh-income countries.Countries face many competing priorities and <strong>injury</strong>interventi<strong>on</strong>s need to be properly assessed for theireffectiveness. However, a great deal more is known aboutpreventing <strong>child</strong> <strong>injury</strong> and death than has been actedup<strong>on</strong>. Research c<strong>on</strong>tinues to shed new light <strong>on</strong> the scale ofthe problem as well as <strong>on</strong> the potential that exists for savinglives and preventing injuries. For example, the analyses ofthe South and East Asian community surveys of <strong>injury</strong>(see Statistical Annex, Table B.1) show just how significant<strong>child</strong> <strong>injury</strong> is. Injury is resp<strong>on</strong>sible for 30% of deaths in1–3-year-olds, with the figure approaching 40% in 4-yearoldsand 50% to 60% am<strong>on</strong>g those aged 5 to 17 years (10).How does <strong>child</strong> <strong>injury</strong> relate to other <strong>child</strong> healthc<strong>on</strong>cerns?As <strong>injury</strong> is a leading cause of death and disability am<strong>on</strong>g<strong>child</strong>ren worldwide, preventing <strong>child</strong> <strong>injury</strong> is closelyc<strong>on</strong>nected to other issues related to <strong>child</strong>ren’s health.Tackling <strong>child</strong> <strong>injury</strong> must be a central part of all initiativesto improve the situati<strong>on</strong> of <strong>child</strong> mortality and morbidityand the general well-being of <strong>child</strong>ren (see Box 1.1).In recent decades, programmes related to <strong>child</strong> survivaltargeted infectious diseases and nutriti<strong>on</strong>al deficienciesin infants and <strong>child</strong>ren. Campaigns were c<strong>on</strong>ducted for2 WORLD REPORT ON CHILD INJURY PREVENTION
BOX 1.1Internati<strong>on</strong>al c<strong>on</strong>tributi<strong>on</strong>s towards improving <strong>child</strong> healthC<strong>on</strong>venti<strong>on</strong> <strong>on</strong> the Rights of the ChildIn November 1989, the United Nati<strong>on</strong>s C<strong>on</strong>venti<strong>on</strong> <strong>on</strong> the Rights of the Child set a new internati<strong>on</strong>al standard for respecting <strong>child</strong>ren and theirrights (3). The C<strong>on</strong>venti<strong>on</strong> stresses the resp<strong>on</strong>sibilities of society to protect <strong>child</strong>ren (from birth up to the age of 18 years) and provide them withappropriate support and services. It further states that <strong>child</strong>ren have the right to the highest attainable level of health and the right to a safe envir<strong>on</strong>ment,free from <strong>injury</strong> and violence.<str<strong>on</strong>g>World</str<strong>on</strong>g> Health Assembly resoluti<strong>on</strong>sThe <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Assembly, the annual meeting of the world’s health ministers, has str<strong>on</strong>gly promoted, through its resoluti<strong>on</strong>s, the recommendati<strong>on</strong>sc<strong>on</strong>tained in WHO’s <str<strong>on</strong>g>World</str<strong>on</strong>g> <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> violence and health (11) and <str<strong>on</strong>g>World</str<strong>on</strong>g> <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> road traffic <strong>injury</strong> preventi<strong>on</strong> (12). These include Resoluti<strong>on</strong>WHA 56.24 <strong>on</strong> violence and health (13) and Resoluti<strong>on</strong> WHA 57.10 <strong>on</strong> road safety and health (14). Children are frequently menti<strong>on</strong>ed in these andother resoluti<strong>on</strong>s as a special target group for interventi<strong>on</strong>s.Millennium Development GoalsIn September 2000, the General Assembly of the United Nati<strong>on</strong>s adopted a series of Millennium Development Goals. The fourth goal is to reduce, bytwo thirds, the mortality rate of <strong>child</strong>ren under the age of 5 years, between 1990 and 2015 (15). Because of the large number of deaths of <strong>child</strong>renunder the age of 1 year from infectious diseases and ne<strong>on</strong>atal causes, <strong>injury</strong> is resp<strong>on</strong>sible for <strong>on</strong>ly around 1.5%–2.0% of deaths in this age group.However, for <strong>child</strong>ren aged between 1 and 4 years, injuries are a more significant cause of death, accounting for just over 6% of all deaths. UnitedNati<strong>on</strong>s Member States are committed to meeting all eight Millennium Development Goals by 2015. Not all countries will meet the fourth goal if theydo not include <strong>injury</strong> preventi<strong>on</strong> in their programmes.A <str<strong>on</strong>g>World</str<strong>on</strong>g> Fit for ChildrenIn May 2002, the United Nati<strong>on</strong>s General Assembly held a Special Sessi<strong>on</strong> <strong>on</strong> <strong>child</strong>ren, from which a document, A world fit for <strong>child</strong>ren, was produced.This sets out a number of health goals for <strong>child</strong>ren. One of these, specific to injuries, calls <strong>on</strong> all Member States to “reduce <strong>child</strong> injuries due to accidentsor other causes through the development and implementati<strong>on</strong> of appropriate preventive measures” (16).Child survivalChild survival has become an important issue globally, as part of a broader and growing c<strong>on</strong>cern for the health and well-being of <strong>child</strong>ren and youngpeople. Indeed, <strong>child</strong> survival has been described as “the most pressing moral dilemma of the new millennium” (17). The Bellagio papers provide newestimates of the numbers and causes of <strong>child</strong> deaths, including injuries, and suggest that two thirds of the nearly 11 milli<strong>on</strong> annual deaths am<strong>on</strong>g<strong>child</strong>ren under the age of 5 years can be prevented by implementing a set of 23 proven and cost-effective interventi<strong>on</strong>s (18). To be most effective,<strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> efforts should be integrated into broader <strong>child</strong> health initiatives.breastfeeding, growth m<strong>on</strong>itoring, immunizati<strong>on</strong> andoral rehydrati<strong>on</strong> therapy. Milli<strong>on</strong>s of lives were saved, andthe lives of many more <strong>child</strong>ren were improved. However,unless <strong>injury</strong> preventi<strong>on</strong> is included in such programmes,as these <strong>child</strong>ren grow up and are subjected to injuries,the impact of the large investments in immunizati<strong>on</strong>,nutriti<strong>on</strong> and maternal and <strong>child</strong> health care may be lost(19).“If we are ultimately going to meet the Millennium Development Goalto reduce <strong>child</strong> mortality, it is imperative that we take acti<strong>on</strong> to addressthe causes of <strong>child</strong>hood <strong>injury</strong> ” Anupama Rao Singh, Regi<strong>on</strong>alDirector of UNICEF East Asia and Pacific.Child injuries and the changing worldOver fifty years ago, <strong>on</strong>e <strong>child</strong> <strong>injury</strong> expert declared that:“it is now generally recognized that accidents c<strong>on</strong>stitutea major problem in public health” (20). A <str<strong>on</strong>g>report</str<strong>on</strong>g> of 1960from the <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong> Regi<strong>on</strong>al Officefor Europe shared this view: in high-income countries,it announced, <strong>injury</strong> had become the leading cause ofdeath in <strong>child</strong>ren older than <strong>on</strong>e year (21). However, theacknowledgement that <strong>child</strong>hood injuries are a significantproblem in developing countries has been more recent.With improvements in other areas of <strong>child</strong> health andbetter methods of collecting data, it is now clear that<strong>injury</strong> is a leading cause of <strong>child</strong> death and ill-health inlow-income and middle-income countries (22, 23). Thefull extent of the problem of injuries in many countries,though, is still not fully understood. Recent large-scalecommunity-based surveys in five countries in South andEast Asia (Bangladesh, China, the Philippines, Thailandand Viet Nam) of overall <strong>child</strong> mortality, have foundmuch higher levels of death from <strong>injury</strong> – both beforeand after the age of five years – than had been previouslythought (19). This approach has complemented hospitalbasedand clinic-based health informati<strong>on</strong> systems,which often miss many <strong>injury</strong> deaths since, for example,a drowned <strong>child</strong> is almost never taken to a hospital orlocal clinic. Drowning, although unrecognized as amajor cause of <strong>child</strong> death in earlier estimates, accountedfor around half of all <strong>child</strong> <strong>injury</strong> deaths in each of thecountries surveyed (19).WORLD REPORT ON CHILD INJURY PREVENTION 3
Tackling the <strong>injury</strong> problem is possible. Experience andresearch have both shown that most <strong>child</strong> injuries, anddeaths from injuries, are preventable in all countries (9,24, 25).Globalizati<strong>on</strong>Globalizati<strong>on</strong> involves a set of socioec<strong>on</strong>omic, cultural,political and envir<strong>on</strong>mental processes that intensify thec<strong>on</strong>necti<strong>on</strong>s between nati<strong>on</strong>s, businesses and people (26–28). The more rapid disseminati<strong>on</strong> of ideas and knowledgeof <strong>injury</strong> preventi<strong>on</strong> (29), and the growth of a global civilsociety (26) involving networks of formal and informalgroups, can have a positive influence <strong>on</strong> <strong>injury</strong> issues.However, there are also negative effects (see Box 1.2). Withgreater freedom of movement of capital across nati<strong>on</strong>alboundaries, the producti<strong>on</strong> of goods – often a hazardousprocess – can more easily shift to regi<strong>on</strong>s of cheaper labour(28). This, in turn, can lead to increased transport in placeswhere road safety is poorly developed (30). Centres of cheapproducti<strong>on</strong> often have weaker c<strong>on</strong>trols <strong>on</strong> occupati<strong>on</strong>alhealth and <strong>child</strong> labour.Whether globalizati<strong>on</strong> will increase or decrease theamount of <strong>child</strong> labour has been the subject of debate (31).According to the Internati<strong>on</strong>al Labour Organizati<strong>on</strong>, in2004 there were still 218 milli<strong>on</strong> <strong>child</strong> labourers under theage of 15 years. However, over the past four years, there hasbeen a global fall in the number of <strong>child</strong>ren working, particularlyof those working in hazardous occupati<strong>on</strong>s (32).In some places, though – such as Gujarat state in India –ec<strong>on</strong>omic growth has led to more <strong>child</strong>ren working, whichis likely to lead to a greater number of injuries (33, 34).BOX 1.2The effects of globalizati<strong>on</strong> <strong>on</strong> <strong>child</strong>injuriesValli was devastated. She had left her small daughter al<strong>on</strong>e for a fewminutes, to go out to fetch water from the communal tap. On herreturn, she found the <strong>child</strong> had drowned in just 10 cm of water. Valliusually carried water from the tap in the traditi<strong>on</strong>al kodam, but storedit in the new plastic buckets that are now cheaply available in India.With increasing globalizati<strong>on</strong> and a fast-expanding Indian middleclass, the country’s use of plastic has soared. Plastic is everywhere– in products, packaging and bags for carrying home goods. Unlikemany other countries, though, India recycles almost half of all plasticgoods, c<strong>on</strong>verting them into other cheap plastic products such aswater buckets, that are often sold without lids. Local bucket-makingfactories buy plastic from recycling shops for about 35 rupees (lessthan <strong>on</strong>e US dollar) a kilogram and make cheap c<strong>on</strong>tainers of variousshapes and sizes from the processed plastic.Drowning can occur in even just a shallow amount of liquid at thebottom of a bucket. Given the shape, size and stability of these buckets,they may not tip over when a <strong>child</strong> leans into <strong>on</strong>e and falls inside. Theolder and safer practice of storing water in a kodam – with its narrowopening that kept water cool and dirt-free and prevented drowning –has been discarded in favour of a cheaper plastic soluti<strong>on</strong>.A similar problem of drowning in buckets was observed by theC<strong>on</strong>sumer Product Safety Commissi<strong>on</strong> in the United States some15 years ago. The Commissi<strong>on</strong> subsequently recommended a performancestandard, a ban <strong>on</strong> this type of bucket and an informati<strong>on</strong> andeducati<strong>on</strong> campaign.Urbanizati<strong>on</strong>Urbanizati<strong>on</strong>, much of it unplanned and ill-resourced,is accelerating <strong>child</strong>ren’s exposure to risk (35). Over thenext two decades, a large part of the world’s populati<strong>on</strong>growth will be in urban areas. The proporti<strong>on</strong> of the globalpopulati<strong>on</strong> in urban areas is predicted to rise from around50% today to over 60% by 2030 (36). Most of this growthwill be in Asia and Africa (37).Urbanizati<strong>on</strong> can promote positive attributes forhealth (38, 39). Medical care for injuries may be easierto provide in urban than in scattered rural areas andthere are ec<strong>on</strong>omies of scale in providing better housingand services. However, as a result of natural growth andmigrati<strong>on</strong>, cities may expand bey<strong>on</strong>d the capacity ofresources to cope adequately (40, 41). Urban slums andsquatter camps pose high risks of <strong>injury</strong> for <strong>child</strong>renacross the world (42, 43).Motorizati<strong>on</strong>The increase in motorizati<strong>on</strong> is related to trends inglobalizati<strong>on</strong> and urbanizati<strong>on</strong>, yet it is worth examiningseparately because of its significant impact <strong>on</strong> <strong>child</strong> <strong>injury</strong>.© P. Virot/WHORoads have always been dangerous places for <strong>child</strong>ren.However, the rapid increase of traffic and the shift oftransport systems around the world to roads make theissue especially pressing. Deaths and injuries from roadtraffic crashes are forecast to rise across the world by 67%between 1990 and 2020 (12).Improved transport and a good road infrastructure areusually c<strong>on</strong>sidered crucial for overall development (44,45). The OECD Development Co-operati<strong>on</strong> Directorate’sTask Team <strong>on</strong> Infrastructure for Poverty Reducti<strong>on</strong> (46)has pointed to benefits for the poor who need better4 WORLD REPORT ON CHILD INJURY PREVENTION
transport to access markets, job opportunities, educati<strong>on</strong>and health facilities. In Morocco, for instance, paved roadshave helped increase school attendance substantially (44).A major increase in road infrastructure has been proposedfor Africa by the Commissi<strong>on</strong> for Africa (47) as part ofthe efforts to achieve the Millennium Development Goals.It would be ir<strong>on</strong>ic, though, if pursuing the MillenniumDevelopment Goals – without strictly c<strong>on</strong>sidering healthand safety issues – led to an increase in death and <strong>injury</strong>am<strong>on</strong>g <strong>child</strong>ren from road traffic crashes or as a result ofincreased polluti<strong>on</strong>.Envir<strong>on</strong>mental changeThe scale and impact of envir<strong>on</strong>mental risks may wellbe accelerating, induced by the global effects of climatechange. The Intergovernmental Panel <strong>on</strong> Climate Changehas predicted an increase of between 1.5 °C and 6 °C by2100, depending <strong>on</strong> future carb<strong>on</strong> emissi<strong>on</strong>s (48). Thecausal pathways by which climate change could affect<strong>child</strong>ren’s health are not clear; they are often indirect andtheir c<strong>on</strong>sequences may be felt at different times (49–53).Children may be exposed to risk of <strong>injury</strong> through anincrease in extreme weather c<strong>on</strong>diti<strong>on</strong>s that pose directhazards – such as flooding, cycl<strong>on</strong>es or mud flows fromheavy rains. They may also be exposed through l<strong>on</strong>gertermdegradati<strong>on</strong> of envir<strong>on</strong>ments – such as droughts,desertificati<strong>on</strong> or rises in sea level (54, 55). Childrenin low-income countries face the greatest problems.Squatter and other makeshift urban settlements areoften highly vulnerable to flooding, and health systemsin these places are generally less able to cope (56). Bothextreme and l<strong>on</strong>g-term envir<strong>on</strong>mental change can leadto migrati<strong>on</strong>, with people ending up living in marginal,unsafe c<strong>on</strong>diti<strong>on</strong>s.The characteristics of <strong>child</strong> <strong>injury</strong>Unintenti<strong>on</strong>al injuries are <strong>on</strong>e of the leading causes ofdeath, hospitalizati<strong>on</strong> and disability across the world.However, the pattern and aetiology of injuries and theiroutcome vary substantially within populati<strong>on</strong>s and acrosscountries. Epidemiologic analysis has l<strong>on</strong>g identifiedbroad factors that, within specific envir<strong>on</strong>ments, pinpointthe types of <strong>injury</strong> and the groups of <strong>child</strong>ren most at risk(21, 57).In high-income countries, research has identified riskfactors and protective factors for individual types of <strong>child</strong><strong>injury</strong> (58, 59). Detailed work <strong>on</strong> <strong>child</strong> <strong>injury</strong> in low-incomeand middle-income countries began more recently and isnow indicating priorities for preventi<strong>on</strong>.The characteristics of <strong>child</strong>ren susceptible to <strong>injury</strong>vary greatly by age, gender, race and socioec<strong>on</strong>omic status.These factors are dealt with in the following secti<strong>on</strong> and ingreater detail in the individual chapters in this <str<strong>on</strong>g>report</str<strong>on</strong>g>.The <strong>child</strong>-<strong>injury</strong> pyramidDeath is the most notable measure of <strong>injury</strong> but it is neitherthe <strong>on</strong>ly outcome nor the most comm<strong>on</strong>. Injury is oftengraphically represented as a pyramid, with the smallestgroup, that of death, at the top, hospitalized <strong>injury</strong> in themiddle and the largest group, n<strong>on</strong>-hospitalized <strong>injury</strong>,at the base. The first study of the sizes of these groupswas carried out by the Child Safety Network in theUnited States in the early 1980s. Their analysis showedthat for every <strong>on</strong>e <strong>child</strong> under 19 years of age who wasfatally injured, 45 <strong>child</strong>ren required hospitalizati<strong>on</strong> anda further 1300 were seen in an emergency departmentand discharged (60).This pattern has been c<strong>on</strong>firmed by detailed work inother regi<strong>on</strong>s and countries, although the exact ratios areaffected by the local provisi<strong>on</strong> of services and the degreeof access to hospital care. UNICEF and the Alliance forSafe Children have examined health histories for twoand a quarter milli<strong>on</strong> people in five countries of Southand East Asia (10). The combined data show that, for<strong>child</strong>ren under 18 years of age, for each death there are 12<strong>child</strong>ren admitted to hospital or permanently disabled and34 <strong>child</strong>ren who needed medical care or missed school orwork because of an <strong>injury</strong>.Children are not <strong>on</strong>ly affected by injuries to themselves,but also by <strong>injury</strong> to others. This applies particularly tothe loss or disability of parents or caregivers through<strong>injury</strong>, and indeed of other members of the family, andthey are affected by expenses and loss of income withinthe family as a result of <strong>injury</strong> (61, 62). In Jiangxi Provincein China, for instance, for <strong>child</strong>ren of primary school ageor younger, about half of parental deaths are associatedwith <strong>injury</strong> (63).Fatal <strong>child</strong> injuriesIn 2004, approximately 950 000 <strong>child</strong>ren under the ageof 18 years died of an <strong>injury</strong>. The majority of these <strong>child</strong>injuries were the result of road traffic collisi<strong>on</strong>s, drowning,burns (fire or scalds), falls or pois<strong>on</strong>ing (see Figure 1.1).These five categories, classified as unintenti<strong>on</strong>al injuries,make up 60% of all <strong>child</strong> <strong>injury</strong> deaths. A furthercategory, labelled “other unintenti<strong>on</strong>al injuries”, includessmothering, asphyxiati<strong>on</strong>, choking, animal or snakebites,hypothermia and hyperthermia. This group accounts for23% of <strong>child</strong>hood deaths, a significant proporti<strong>on</strong>.The rate of <strong>child</strong> <strong>injury</strong> death is 3.4 times higher in lowincomeand middle-income countries than in high-incomecountries, but there are large variati<strong>on</strong>s according to thecategory of <strong>injury</strong> death. For fire and flame deaths, the ratein low-income countries is close to 11 times higher than inhigh-income countries, for drowning it is six times higher,for pois<strong>on</strong>s four times and for falls around six times higher(see Table 1.2).WORLD REPORT ON CHILD INJURY PREVENTION 5
FIGURE 1.1Distributi<strong>on</strong> of global <strong>child</strong> <strong>injury</strong> deaths by cause, 0–17 years,<str<strong>on</strong>g>World</str<strong>on</strong>g>, 2004aOther unintenti<strong>on</strong>al a31.1%War2.3%Self-inflicted injuries4.4%Homicide5.8%Pois<strong>on</strong>ing3.9%Falls4.2%“Other unintenti<strong>on</strong>al” includes categories such as smothering, asphyxiati<strong>on</strong>, choking,animal and venomous bites, hypothermia and hyperthermia as well as natural disasters.Source: WHO (2008), Global Burden of Disease: 2004 update.Road traffic injuries22.3%Drowning16.8%Fire-related burns9.1%TABLE 1.2Unintenti<strong>on</strong>al <strong>injury</strong> death rates per 100 000 <strong>child</strong>ren a by causeand country income level, <str<strong>on</strong>g>World</str<strong>on</strong>g>, 2004RoadtrafficDrowningUNINTENTIONAL INJURIESFireburnsFalls Pois<strong>on</strong>s Other bTOTALHIC 7.0 1.2 0.4 0.4 0.5 2.6 12.2LMIC 11.1 7.8 4.3 2.1 2.0 14.4 41.7<str<strong>on</strong>g>World</str<strong>on</strong>g> 10.7 7.2 3.9 1.9 1.8 13.3 38.8These data refer to those under 20 years of age.“Other” includes categories such as smothering, asphyxiati<strong>on</strong>, choking, animal orsnakebites, hypothermia and hyperthermia as well as natural disasters.HIC = High-income countries; LMIC = low-income and middle-income countries.abTABLE 1.3Unintenti<strong>on</strong>al <strong>injury</strong> death rates per 100 000 <strong>child</strong>ren by age andcountry income level, <str<strong>on</strong>g>World</str<strong>on</strong>g>, 2004AGE (in years)Under 1 1–4 5–9 10–14 15–19 Under 20HIC 28.0 8.5 5.6 6.1 23.9 12.2LMIC 102.9 49.6 37.6 25.8 42.6 41.7<str<strong>on</strong>g>World</str<strong>on</strong>g> 96.1 45.8 34.4 23.8 40.6 38.8Source: WHO (2008), Global Burden of Disease: 2004 update.In an analysis of <strong>child</strong> death rates by sex, the rate ofmale deaths exceeds that of female deaths in nearly allcategories of <strong>injury</strong>, with the excepti<strong>on</strong> of fire-relatedburns (see Figure 1.2). The female excess in fire-relatedburns is particularly noticeable in certain parts of theworld, such as the WHO South-East Asia Regi<strong>on</strong> and thelow-income and middle-income countries of the EasternMediterranean Regi<strong>on</strong>, where deaths of female adolescentscan exceed those of males by up to 50% (see StatisticalAnnex, Table A.1).In most regi<strong>on</strong>s and countries, the gender gap forfatal injuries increases with age. At the global level,<strong>injury</strong> death rates am<strong>on</strong>g <strong>child</strong>ren under the age of1 year, as well as those aged 1–4 years, are about thesame for males and females. However, in <strong>child</strong>ren aged5–9 years, male death rates are a third higher than femalerates, a discrepancy that increases to 60% am<strong>on</strong>g thoseaged 10–14 years. Adolescents aged 15–17 years show anadult profile, with males in that age group accountingfor more than 86% of all <strong>injury</strong> deaths, particularly inhigh-income countries.Source: WHO (2008), Global Burden of Disease: 2004 update.The associati<strong>on</strong> of age with <strong>injury</strong> type is found in bothrich and poor countries. As can be seen in Table B.1 in theStatistical Annex, the combined results of the South andEast Asian community surveys show that, in that part ofthe world, the main cause of <strong>injury</strong> death in <strong>child</strong>ren under1 year of age is suffocati<strong>on</strong>. In <strong>child</strong>ren under 5 years it isdrowning, for those aged between 5 and 9 years drowningis joined by road traffic injuries and animal bites, whileam<strong>on</strong>g <strong>child</strong>ren aged 10–17 years, road traffic deaths arethe most significant unintenti<strong>on</strong>al <strong>injury</strong>. However, thereare great differences between rich and poor countries.While drowning is the leading cause of <strong>injury</strong> deatham<strong>on</strong>g <strong>child</strong>ren under 5 years in both the United Statesand Asia, the rate of death per 100 000 <strong>child</strong>ren is 30 timeshigher in Asia (19, 62).Table 1.3 shows that rates of <strong>injury</strong> death varysubstantially by age in high-income countries with thehighest rate, that for 15–19-year-olds, being four times thelowest rate, that for 5–9-year-olds.FIGURE 1.2Unintenti<strong>on</strong>al <strong>injury</strong> death rates per 100 000 <strong>child</strong>ren a by causeand sex, <str<strong>on</strong>g>World</str<strong>on</strong>g>, 2004Rate per 100 000 populati<strong>on</strong>ab151050RoadtrafficinjuriesBoysGirlsDrowning Falls FirerelatedburnsThese data refer to those under 20 years of age.“Other unintenti<strong>on</strong>al” includes categories such as smothering, asphyxiati<strong>on</strong>, choking,animal and venomous bites as well as natural disasters.Source: WHO (2008), Global Burden of Disease: 2004 update.Pois<strong>on</strong>ingOtherunintenti<strong>on</strong>alb6 WORLD REPORT ON CHILD INJURY PREVENTION
N<strong>on</strong>-fatal <strong>child</strong> injuriesThe types of <strong>injury</strong> associated with <strong>child</strong> death aredifferent from those that cause n<strong>on</strong>-fatal <strong>injury</strong> andcan again be different from those that cause l<strong>on</strong>g-termeffects. The community surveys c<strong>on</strong>ducted in South andEast Asia have shown up the relative significance of n<strong>on</strong>fatal<strong>injury</strong> and how it differs from fatal <strong>injury</strong>. Similarly,in Brazil, for <strong>child</strong>ren under 15 years of age, the leadingcauses of unintenti<strong>on</strong>al <strong>injury</strong> death are associated withtraffic-related injuries and drowning, while more thanhalf of all n<strong>on</strong>-fatal injuries are the result of a fall (64).These findings also come out in the 28-country GlobalSchool Health Survey, where in all countries, except<strong>on</strong>e, falls are the leading causes of n<strong>on</strong>-fatal <strong>injury</strong> butaccount for <strong>on</strong>ly a small proporti<strong>on</strong> of fatal <strong>child</strong> injuries(see Statistical Annex, Table A.3). Focusing <strong>on</strong> deathdata al<strong>on</strong>e, therefore, may result in <strong>injury</strong> preventi<strong>on</strong>strategies ignoring frequent injuries that are also costlyto the health care system.Injuries and subsequent disabilityHead injuries are the single most comm<strong>on</strong> – and potentiallymost severe – type of <strong>injury</strong> sustained by <strong>child</strong>ren. Am<strong>on</strong>gminor injuries incurred by <strong>child</strong>ren, cuts and bruises arethose seen most frequently. However, the most comm<strong>on</strong>category of unintenti<strong>on</strong>al injuries suffered by <strong>child</strong>renunder 15 years and requiring hospital admissi<strong>on</strong> are varioustypes of fractures to the arms and legs (see Table 1.4).In additi<strong>on</strong> to mortality, hospital admissi<strong>on</strong>s, emergencydepartment attendances and days lost from school can allbe used as markers of <strong>injury</strong> severity. There are also morespecific scoring methods, including notably, the InjurySeverity Score, the Revised Trauma Score and the PaediatricTrauma Score. A review of the different types of measurescurrently used indicates that there is no standard methodto determine the severity of an <strong>injury</strong> in a particular <strong>child</strong>(65). Each type of measure has its drawbacks and may varyaccording to the cause of <strong>injury</strong> or access to care. Measuresof disability also tend to be n<strong>on</strong>-standard.TABLE 1.4Nature of unintenti<strong>on</strong>al injuries sustained a by <strong>child</strong>ren under 15 years, <str<strong>on</strong>g>World</str<strong>on</strong>g>, 2004Type of <strong>injury</strong> sustained Rate per 100 000 populati<strong>on</strong> Proporti<strong>on</strong> of all unintenti<strong>on</strong>al injuries (%)Intracranial <strong>injury</strong> b – short-term c 419.4 16.3Open wound 316.9 12.3Pois<strong>on</strong>ing 282.4 10.9Fractured ulna or radius 209.3 8.1Burns
Data from the Global Childhood Unintenti<strong>on</strong>alInjury Surveillance c<strong>on</strong>ducted in four cities showed thatnearly 50% of <strong>child</strong>ren under the age of 12 years who hadsuffered an unintenti<strong>on</strong>al <strong>injury</strong> severe enough to warrantpresentati<strong>on</strong> to an emergency deparment were left withsome form of disability (Statistical Annex, Table C.1).Am<strong>on</strong>g <strong>child</strong>ren who had suffered a burn, 8% were leftwith permanent disabilities, while <strong>child</strong>ren injured intraffic crashes were significantly more likely to be left withsome form of disability (Table 1.5).Many young people who survive major trauma are leftwith <strong>on</strong>going disabilities, with a major impact <strong>on</strong> theirown lives as well as <strong>on</strong> the lives of their families. Thesedisabilities may be physical, mental or psychological. Someof the problems encountered in the years following <strong>injury</strong>include an inability to attend school, find suitable work orengage in an active social life. There are also other morebasic problems such as having to cope with c<strong>on</strong>tinuedpain. Support for these young people most often falls <strong>on</strong>their close family and friends (66).Child <strong>injury</strong> and ageInjury preventi<strong>on</strong> strategies need to take into account<strong>child</strong> development in different and sometimes changingc<strong>on</strong>texts. Adolescence, for example, has become a moresignificant developmental stage in many low-incomecountries, whereas before there had been a more directtransiti<strong>on</strong> from <strong>child</strong>hood to adulthood (67). Childhoodis also changing at earlier stages in some places. In partsof sub-Saharan Africa, HIV/AIDS is creating parentlesshouseholds. With young <strong>child</strong>ren forced to take <strong>on</strong> adultresp<strong>on</strong>sibilities (68) the nature of <strong>child</strong>hood in these areashas changed radically (69).Exposure to <strong>injury</strong> risk for <strong>child</strong>ren also depends <strong>on</strong>the particular set of laws that are in place and the degreeto which these are enforced. These laws include the legalages for entering the formal workforce, for driving, and fordrinking alcohol. There are often c<strong>on</strong>siderable differencesbetween countries. Alcohol can be legally c<strong>on</strong>sumed at 15 years in Belgium,but not until the age of 20 years in New Zealand. A car can be legally driven in New Zealand at the age of15 years. In Sweden the legal driving age is 18 years (70).What makes <strong>child</strong>ren particularly susceptible to <strong>injury</strong>?Children are not just small adults. Their physical andcognitive abilities, degrees of dependence, activities andrisk behaviours all change substantially as they grow older(50, 71–75). As <strong>child</strong>ren develop, their curiosity and wishto experiment are not always matched by their capacity tounderstand or to resp<strong>on</strong>d to danger (76).At about 3 m<strong>on</strong>ths of age <strong>child</strong>ren will start to wriggleand roll, at about 6 m<strong>on</strong>ths they will sit up, and they willstart crawling at around 9 m<strong>on</strong>ths. Objects are reachedfor, grasped and put in their mouth. At 18 m<strong>on</strong>ths they aremobile and exploring the world. Child development andbehaviour is therefore highly associated with particularinjuries. Pois<strong>on</strong>ing, for example, is linked to the graspingand drinking behaviour of <strong>child</strong>ren aged 1–3 years, whilefalls are related to the stage of learning to walk.Analysis of <strong>injury</strong> using age ranges in years can betoo broad to detect the rapid change in development and<strong>injury</strong> risk am<strong>on</strong>g very young <strong>child</strong>ren. By using 3-m<strong>on</strong>thage brackets, <strong>on</strong>e study showed that falls were the leadingcause of <strong>injury</strong> in <strong>child</strong>ren aged under 3 years, but that theparticular items that caused their falls – such as furniture,TABLE 1.5Injury severity and estimated l<strong>on</strong>g-term effects of unintenti<strong>on</strong>al injuries am<strong>on</strong>g <strong>child</strong>ren a presenting to emergency departments infour countries bRoad traffic injuries(n = 350)TYPE OF UNINTENTIONAL INJURYFalls(n = 913)Burns(n = 210)Pois<strong>on</strong>ing(n = 66)Drowning(n = 20)Injury Severity Score (ISS)Lowest score 0 0 0 0 0 0Highest score 75 75 75 16 75 75Median ISS 4 4 3 1 4 4Mean ISS c 10 5 5 3 11 7DisabilityNo significant disability 38% 53% 51% 80% 65% 56%Short term temporary disability (< 6 weeks) 43% 39% 24% 12% 20% 40%L<strong>on</strong>g term temporary disability (> 6 weeks) 17% 8% 17% 8% 5% 12%Permanent disability 3% 1% 8% 0% 10% 2%Totalabcaged under 12 years.Bangladesh, Colombia, Egypt, Pakistan.to nearest whole number.Source: see Statistical Annex, Table C1.8 WORLD REPORT ON CHILD INJURY PREVENTION
stairs and playground equipment – were important atdifferent ages. The study also showed that pois<strong>on</strong>ing<strong>injury</strong> started to rise at the age of 9 m<strong>on</strong>ths, c<strong>on</strong>tinuingup to 21 to 23 m<strong>on</strong>ths, and then declined. Burns from hotliquids were substantially higher am<strong>on</strong>g those aged 12 to18 m<strong>on</strong>ths (73).The small stature of <strong>child</strong>ren increases their risk in aroad envir<strong>on</strong>ment. They are less visible than adults andif hit by a vehicle, they are more likely than an adult tosustain a head or neck <strong>injury</strong> (77). At the same time, small<strong>child</strong>ren have difficulty seeing over vehicles, judging thespeed of <strong>on</strong>coming vehicles and discerning the distanceof a vehicle from the sound of its engine (78).Other physical characteristics make <strong>child</strong>ren vulnerableto injuries. The skin of infants burns more deeply andquickly and at lower temperatures than the thicker skinof adults (77). Smaller airway size increases the danger ofaspirati<strong>on</strong> (24). In additi<strong>on</strong>, certain physical characteristicsof young <strong>child</strong>ren may affect <strong>injury</strong> outcomes. For example,<strong>child</strong>ren’s larger ratio of body surface area to volume meansthat not <strong>on</strong>ly will the size of a burn – for a given volume of hotliquid – be greater than for an adult, but also that there willbe more fluid lost from the burnt area, thus complicating themanagement of the <strong>injury</strong> (79). Similarly, a given amount ofa pois<strong>on</strong>ous substance will more likely be toxic for a <strong>child</strong>than an adult because of the <strong>child</strong>’s smaller mass. Children’ssmaller size also creates a risk of entrapment of body parts,most dangerously for the head. Many products and settingsdo not properly take these risks into account.Studies of <strong>child</strong>ren in road traffic have shown thatyoung <strong>child</strong>ren may lack the knowledge, skills and levels ofc<strong>on</strong>centrati<strong>on</strong> needed to manage the road envir<strong>on</strong>ment, nomatter how benign the road c<strong>on</strong>diti<strong>on</strong>s (80). Their physicalabilities may not be matched by cognitive abilities. Forinstance young <strong>child</strong>ren, in the process of exploring theirworld, may fall from heights because their climbing abilityis not matched by their ability to balance or reas<strong>on</strong> (77).Children’s worldsYoung <strong>child</strong>ren’s behaviour differs from that of adults.A vivid illustrati<strong>on</strong> of this is in the home envir<strong>on</strong>ment.“[They] crawl about the floor, climb <strong>on</strong>to the windowledge, squeeze through stair balustrades, slide down thestair handrail, swing <strong>on</strong> the gate, run from room to roomand ride bikes inside as well as out, making use of theirhouses in ways that seem to them reas<strong>on</strong>able, but have notapparently been foreseen by the designer” (81).Physical and mental stages are important, but <strong>child</strong>renare especially vulnerable to <strong>injury</strong> because they live ina world in which they have little power or c<strong>on</strong>trol. Thevulnerability of <strong>child</strong>ren is exacerbated by their lack ofpower and status (6). They find themselves in urban andrural envir<strong>on</strong>ments c<strong>on</strong>structed by and for adults (82).Their voices are seldom heard and <strong>on</strong>ly rarely are placesdesigned in c<strong>on</strong>sultati<strong>on</strong> with <strong>child</strong>ren (83).Urban planners and policy-makers know little of<strong>child</strong>ren’s c<strong>on</strong>cerns and often assume change will benefitall (84). For example, improving water supplies to aneighbourhood may result in young <strong>child</strong>ren – oftenthe family water carriers – having to travel an increaseddistance to a standpipe to fetch water, with possible damageto their head, neck and spine (85). New products are oftendesigned without taking into c<strong>on</strong>siderati<strong>on</strong> their possibleuse by <strong>child</strong>ren and the c<strong>on</strong>sequent harm.Child <strong>injury</strong> and genderBoys tend to have both more frequent and more severeinjuries than girls (1, 76). Sex differences in <strong>injury</strong> ratesappear within the first year of life for most types of <strong>injury</strong>(86). According to WHO data, in <strong>child</strong>ren under 15 years,there are, <strong>on</strong> average, 24% more <strong>injury</strong> deaths am<strong>on</strong>g boysthan there are am<strong>on</strong>g girls.Data from developed countries indicate that, from birth<strong>on</strong>wards, males have higher rates of <strong>injury</strong> than females,for all types of <strong>injury</strong> (87). The pattern is less uniform inlow-income and middle-income countries, but the overallgender differential is clear, with <strong>injury</strong> death rates around<strong>on</strong>e third higher for males under 20 years of age than forfemales.A number of reas<strong>on</strong>s for these differences in <strong>injury</strong> havebeen put forward and investigated. One study found thatsex differences were not completely explained by differencesin exposure to risk and that differences in <strong>injury</strong> rates beginto appear at the same age as differences in behaviour (86).Various theories have been proposed for the differencein <strong>injury</strong> rates between boys and girls (88). These includethe idea that boys engage in more risk taking thangirls (89), that they have higher activity levels (90), thatthey behave more impulsively. Also included are thesuggesti<strong>on</strong>s that boys are socialized in a different wayfrom girls and are less likely to have their explorati<strong>on</strong>restrained by parents (91), that they are more likely tobe allowed to roam further (92), and that they are morelikely to be allowed to play al<strong>on</strong>e (93).Child <strong>injury</strong> and socioec<strong>on</strong>omic factorsAs can be seen in Figure 1.3, most of the <strong>child</strong>hood<strong>injury</strong> burden rests in low-income and middle-incomecountries, and within these countries, poor <strong>child</strong>renare disproporti<strong>on</strong>ately affected (94). Some of the mostvulnerable groups are those who live in chr<strong>on</strong>ic poverty(95). They are a heterogeneous group, often living inremote rural areas or c<strong>on</strong>flict z<strong>on</strong>es or else displaced. Inthe Islamic Republic of Iran, for example, a communitybasedsurvey has shown that the majority of fatalunintenti<strong>on</strong>al injuries to <strong>child</strong>ren under the age of 15years occur in remote or rural areas (96). The chr<strong>on</strong>icpoor have few buffers against shocks – such as income andsocial networks (97). The first target of the MillenniumDevelopment Goals is to halve, between 1990 and 2015,WORLD REPORT ON CHILD INJURY PREVENTION 9
FIGURE 1.3Rate of unintenti<strong>on</strong>al injuries per 100 000 <strong>child</strong>ren a , by WHO regi<strong>on</strong> and country income level, <str<strong>on</strong>g>World</str<strong>on</strong>g>, 200445+30–44.9915–29.99
BOX 1.3Child supervisi<strong>on</strong>Supervisi<strong>on</strong> is widely recognized as vital to protecting <strong>child</strong>ren from harm. Some estimates suggest that 90% of injuries to young <strong>child</strong>ren occur inor around their home when they are supposedly being supervised by a caregiver. Despite the beliefs that <strong>child</strong>hood <strong>injury</strong> is often related to a lack ofsupervisi<strong>on</strong>, evidence to support this premise is limited.There have been few attempts formally to define the term “supervisi<strong>on</strong>” in the c<strong>on</strong>text of <strong>injury</strong> preventi<strong>on</strong>. A reas<strong>on</strong>able definiti<strong>on</strong>, c<strong>on</strong>sistentwith existing evidence, is that supervisi<strong>on</strong> refers to behaviours that are related to attenti<strong>on</strong> (watching and listening) and to proximity (touching, orbeing within reach). Furthermore, these behaviours are judged by how c<strong>on</strong>tinuous they are (whether c<strong>on</strong>stant, intermittent or not at all).What some researchers are finding, though, is that caregivers exhibit a spectrum of patterns of supervisi<strong>on</strong> – ranging from almost total neglectto extreme vigilance. While there are many parallels between good parenting skills and good supervisi<strong>on</strong> practices, there does not seem to be anyagreed-up<strong>on</strong> supervisory style that is uniformly protective. In additi<strong>on</strong>, the effectiveness of supervisi<strong>on</strong> will be affected by whether the caregiverbecomes distracted, and by the caregiver’s mental health status, use of alcohol or drugs, complacency or overc<strong>on</strong>fidence.Models of supervisi<strong>on</strong> have focused <strong>on</strong>:– the need for supervisi<strong>on</strong> based <strong>on</strong> a <strong>child</strong>’s age, developmental status and exposure to possible hazards;– the supervisor’s judgement, skills and ability to influence the <strong>child</strong>;– the physical proximity of the supervisor to the <strong>child</strong>, taking into account the setting and the characteristics of the <strong>child</strong>;– the degree of verbal and physical interventi<strong>on</strong>s with the <strong>child</strong>;– how much of the time the supervisor is actively supervising.Tools are needed to measure these various c<strong>on</strong>structs more accurately.There is c<strong>on</strong>siderable indirect evidence that associates supervisi<strong>on</strong> with a <strong>child</strong>’s risk of <strong>injury</strong>. This risk increases substantially when the <strong>child</strong> liveswith a single caregiver, in a home with multiple siblings, or with a substance-abusing caregiver – all of which can compromise the ability of a caregiverto attend closely to the <strong>child</strong>. In large families, supervisi<strong>on</strong> of younger <strong>child</strong>ren by older <strong>child</strong>ren may be comm<strong>on</strong>, but is usually inadequate.Good <strong>child</strong> supervisi<strong>on</strong> is likely to be an important interventi<strong>on</strong> to protect <strong>child</strong>ren from <strong>injury</strong>. However, the role of supervisi<strong>on</strong> and guidelinesfor its age-appropriate applicati<strong>on</strong> in various settings of <strong>injury</strong> risk need further investigati<strong>on</strong>. Research to improve the effectiveness of supervisi<strong>on</strong>as an <strong>injury</strong> preventi<strong>on</strong> strategy should include efforts to define and measure different types of supervisi<strong>on</strong>. Models of good supervisi<strong>on</strong> should bedeveloped, and cultural influences <strong>on</strong> the ways supervisi<strong>on</strong> is c<strong>on</strong>ducted should be examined. Interventi<strong>on</strong>s to influence the behaviour of caregiversalso need to be c<strong>on</strong>sidered. A final critical step is to evaluate different supervisi<strong>on</strong> strategies and measure their impact <strong>on</strong> reducing injuries.A few studies in developed countries have attemptedto look at the associati<strong>on</strong> between <strong>child</strong>hood injuries andsocioec<strong>on</strong>omic status. In England and Wales, a study examined <strong>injury</strong>mortality data by occupati<strong>on</strong>al group of the parentsfor <strong>child</strong>ren aged 1–15 years over two time periods– 1979–1983 and 1989–1992 (100). All <strong>child</strong>hood<strong>injury</strong> deaths had declined between the two periodsof study, but the associati<strong>on</strong>s of <strong>injury</strong> deaths withsocioec<strong>on</strong>omic factors had become str<strong>on</strong>ger. Socialgradients were particularly steep for certain types of<strong>injury</strong> such as homicide, fire burns and pedestrianinjuries. A recent study in New South Wales c<strong>on</strong>firmed thatthe associati<strong>on</strong> between relative socioec<strong>on</strong>omicdisadvantage and n<strong>on</strong>-fatal <strong>injury</strong> risk am<strong>on</strong>g <strong>child</strong>renin this Australian state was str<strong>on</strong>gest for transportrelatedinjuries, burns and pois<strong>on</strong>ing (101).There are even fewer studies from developing countriesthat have examined <strong>child</strong>hood injuries according tosocioec<strong>on</strong>omic group. A study in South Africa explored the incidenceand causes of <strong>injury</strong> across socioec<strong>on</strong>omic andenvir<strong>on</strong>mental settings in six neighbourhoods in apoor area of Johannesburg – two informal settlements,two neighbourhoods of council houses and two ofcouncil-built apartment buildings (102). The informalsettlements <str<strong>on</strong>g>report</str<strong>on</strong>g>ed higher rates of <strong>injury</strong> than theother types of neighbourhood. A survey <strong>on</strong> the ec<strong>on</strong>omic impacts of <strong>injury</strong> in rural VietNam showed that poverty was a significant risk factorfor <strong>injury</strong>, and also that <strong>child</strong>ren in poor householdshad higher rates of <strong>injury</strong> sustained in the home thanbetter-off <strong>child</strong>ren (103).Injuries as a cause of povertyPoor populati<strong>on</strong>s are particularly vulnerable to a range ofcalamities, which can trigger a further decline in familyresources. Crises brought about by ill-health, a road trafficcrash or an episode of flooding may push people intopoverty (104). A study in Bangalore, India and in Bangladesh found thatthe burden from road crashes had pushed many householdsinto poverty. In Bangalore, 71% of households inurban areas and 53% in rural areas were not poor beforethe crash; in Bangladesh the comparable figures were33% in urban areas and 49% in rural areas (105). In Viet Nam, the cost of <strong>injury</strong> to poor householdswas estimated as equivalent <strong>on</strong> average to 11 m<strong>on</strong>ths’income. The risk of a poor household falling below thepoverty line was 21% higher am<strong>on</strong>g those that had hadan <strong>injury</strong> than am<strong>on</strong>g those that had not (106). Health-WORLD REPORT ON CHILD INJURY PREVENTION 11
care costs and the loss of income were the main factorsc<strong>on</strong>tributing to this effect.Children are a particularly vulnerable group, eitherdirectly through being injured themselves or indirectlythrough the loss of their parents. In a Bangladesh slum, 40% of malnourished <strong>child</strong>rencame from households where the breadwinner hadbeen incapacitated by illness or <strong>injury</strong> (107). In Ghana, a study of the ec<strong>on</strong>omic c<strong>on</strong>sequences of<strong>injury</strong> within the family found that in rural households,28% of families <str<strong>on</strong>g>report</str<strong>on</strong>g>ed a decline in food c<strong>on</strong>sumpti<strong>on</strong>following an <strong>injury</strong> (108). A study in Bangladesh found that <strong>injury</strong> was theleading cause of <strong>child</strong>ren losing a parent, with about7900 fathers and 4300 mothers dying each year (61).Certain groups of <strong>child</strong>ren have higher than averagerates of <strong>injury</strong>. These rates may be associated with thespecific circumstances and envir<strong>on</strong>ment of the <strong>child</strong>ren –for instance, being refugees or being homeless. The groupsthat stand out most clearly with respect to their higher <strong>injury</strong>rates are indigenous populati<strong>on</strong>s, who also tend to experiencegreater relative poverty than their compatriots (109). Injury is a major cause of death and morbidity am<strong>on</strong>gthe Maori populati<strong>on</strong> in New Zealand (110). In the United States and Australia, <strong>injury</strong> death rates inindigenous people are two to three times the rates forn<strong>on</strong>-indigenous people (111). The death rate from road traffic injuries am<strong>on</strong>gindigenous Australians under 15 years of age, is two anda half times that for n<strong>on</strong>-indigenous young Australians(16.7 per 100 000, compared to 6.6 per 100 000) (112).The preventability of <strong>child</strong> <strong>injury</strong>The principles of <strong>injury</strong> preventi<strong>on</strong>Injuries can be prevented or c<strong>on</strong>trolled. Because of theirmany causes and the close interrelati<strong>on</strong>ship between them,a wide range of preventi<strong>on</strong> approaches is called for. Variouspreventi<strong>on</strong> models have been proposed, but for the purposeof this <str<strong>on</strong>g>report</str<strong>on</strong>g> the classic model is used, including:– primary preventi<strong>on</strong>: preventing new injuries;– sec<strong>on</strong>dary preventi<strong>on</strong>: reducing the severity of injuries;– tertiary preventi<strong>on</strong>: decreasing the frequency andseverity of disability after an <strong>injury</strong> (see Box 1.4).The c<strong>on</strong>tributi<strong>on</strong> of Hadd<strong>on</strong>William Hadd<strong>on</strong> Jr developed a scheme (known as the“Hadd<strong>on</strong> Matrix”) in the 1960s to apply the principles ofpublic health to the problem of road traffic safety (117, 118).It has since been used as a means of developing ideas toprevent <strong>injury</strong> of all types. The matrix c<strong>on</strong>sists of 12 cells.These are arranged in a table of four columns relating tothe host, agent/vehicle, physical envir<strong>on</strong>ment and socialenvir<strong>on</strong>ment, and of three rows relating to the periodsbefore, during and after the <strong>injury</strong> (corresp<strong>on</strong>ding toprimary, sec<strong>on</strong>dary and tertiary preventi<strong>on</strong>).The resulting matrix provides a means to identify, cellby cell:– strategies and priorities for <strong>injury</strong> preventi<strong>on</strong>, in termsof their costs and effects;– existing research and research that needs to beundertaken;– the allocati<strong>on</strong> of resources in the past and the future,and the effectiveness of such allocati<strong>on</strong>.Hadd<strong>on</strong> went <strong>on</strong> to describe 10 strategies to accompanythe matrix, which describe the ways in which the harmfultransfer of energy can be prevented or c<strong>on</strong>trolled in someway (119) (see Table 1.6, where Hadd<strong>on</strong>’s 10 strategies havebeen applied to <strong>child</strong> injuries).The significance of the Hadd<strong>on</strong> Matrix and Hadd<strong>on</strong>’s 10<strong>injury</strong> preventi<strong>on</strong> countermeasures is that they highlightthe fact that not <strong>on</strong>ly can society intervene to reduce<strong>injury</strong>, but that such interventi<strong>on</strong>s can occur at differentstages (120).Public health approachesAs has occurred with several other health issues, theemphasis has shifted over recent years from the individualto the envir<strong>on</strong>mental c<strong>on</strong>text in which an <strong>injury</strong> occurs.Al<strong>on</strong>g with this shift of emphasis, there has also been arealizati<strong>on</strong> that single-cause explanati<strong>on</strong>s of <strong>injury</strong> areincomplete and that models using a range of causes areneeded instead. The public health model is therefore usefulas it approaches the issue in a systematic and coordinatedway, following four logical steps (Figure 1.4) – all of whichcall for good evidence <strong>on</strong> which to base activities. It is amodel that can reveal important emerging issues in <strong>child</strong><strong>injury</strong> preventi<strong>on</strong> (see Box 1.5).FIGURE 1.4The public health approach to <strong>injury</strong> preventi<strong>on</strong>1. SurveillanceWhat is theproblem?4. Implementati<strong>on</strong>How is it d<strong>on</strong>e?2. Risk factoridentificati<strong>on</strong>What are thecauses?3. Developmentand evaluati<strong>on</strong> ofinterventi<strong>on</strong>sWhat works?A public health perspective also allows for a holisticapproach to the issue of <strong>child</strong> <strong>injury</strong>. Such an approachcan bring together, as partners, the diverse range ofnati<strong>on</strong>al and local agencies and organizati<strong>on</strong>s involved in<strong>injury</strong> preventi<strong>on</strong>, and coordinate acti<strong>on</strong>s under a singleumbrella (120).12 WORLD REPORT ON CHILD INJURY PREVENTION
© P. Virot/WHOBOX 1.4Access to careMuch can be d<strong>on</strong>e to lower the burden of death and disability from <strong>injury</strong> by strengthening trauma care services across the spectrum from prehospitalcare through hospital care to rehabilitati<strong>on</strong>. The chain of survival starts at the scene of the incident. Prompt, quality pre-hospital care cansave many lives after an <strong>injury</strong>. Where formal emergency medical services (usually with ambulances) exist, their performance can be improvedby standardizing equipment, training, infrastructure and operati<strong>on</strong>s. Where they do not exist, starting new formal emergency medical servicescan be a reas<strong>on</strong>able opti<strong>on</strong>, especially al<strong>on</strong>g busy roads with high rates of crashes. However, these services can be costly. In any circumstance, andespecially where there are no formal emergency medical services, pre-hospital care can be improved by building up<strong>on</strong> existing, informal systems ofpre-hospital care and transport. In many cases this involves drawing up<strong>on</strong> resources in the community to train and possibly equip those whose jobit is to be the first <strong>on</strong> the scene of an emergency. These may be members of the lay public, members of organizati<strong>on</strong>s such as the Red Cross and RedCrescent societies, or members of nati<strong>on</strong>al emergency services, such as the police and fire services.A good example of the effectiveness of such an approach is a project, creating a two-tier system, that operated in northern Iraq and Cambodia. Severalthousand villagers, forming the first tier, were trained in basic first aid. When needed, a sec<strong>on</strong>d tier of more highly trained paramedics was called up<strong>on</strong>.This system sharply decreased mortality rates am<strong>on</strong>g victims of mine explosi<strong>on</strong> and of other trauma, and is a good example of how pre-hospital care canbe improved at low cost without developing ambulance systems (113). Similar examples can be found in WHO’s Prehospital trauma care systems (114).The treatment that an injured <strong>child</strong> receives <strong>on</strong> reaching the hospital is another point in the chain of survival where lives can be saved. Improvingthe organizati<strong>on</strong> and planning of trauma care services is an affordable and sustainable way to raise the quality and outcome of care. This includesdefining a set of essential trauma care services, which every injured <strong>child</strong> should receive, as well as the required resources, both human and physical,to assure such services. C<strong>on</strong>tinuing educati<strong>on</strong> courses <strong>on</strong> trauma care should be introduced, al<strong>on</strong>g with quality improvement programmes, and thesystem for referrals between different parts of the health care system should be strengthened through inter-hospital transfer agreements.The essential elements of trauma care need not be expensive. However, the cost of care can be a barrier to access, especially where users are askedto pay in advance of receiving emergency services. It is therefore essential to ensure that the essential trauma care services can be delivered to allwho need them irrespective of the ability to pay, with cost recovery coming <strong>on</strong>ly after the treatment is given. More detailed recommendati<strong>on</strong>s <strong>on</strong>strengthening trauma care at hospitals and clinics can be found in WHO’s Guidelines for essential trauma care (115).A visit to the emergency department after an <strong>injury</strong> is often the first encounterthat <strong>child</strong>ren have with a hospital. The experience can add to theirphysical distress if there is a lack of understanding or informati<strong>on</strong> or if theyfeel l<strong>on</strong>ely or frightened. When treating <strong>child</strong>ren who have been injured,health-care pers<strong>on</strong>nel should provide informati<strong>on</strong>, communicated in amanner appropriate to the <strong>child</strong>’s age, and seek to make the hospital envir<strong>on</strong>mentless intimidating and inhospitable (116). In short, both hospitalsand their health-care staff should do their utmost to be <strong>child</strong>-friendly.Finally, many injured survivors lead lives of disability. Much of this disabilitycould be avoided with improved rehabilitati<strong>on</strong> services. This would involveimproving ser vices in health care facilities and as well as access to communit y-based rehabilitati<strong>on</strong>. Assessments have shown that such rehabilitati<strong>on</strong>services are poorly developed globally and are in fact am<strong>on</strong>g the least developedwithin the spectrum of trauma care services. Strengthening suchrehabilitati<strong>on</strong> services will reduce the extent of disability following an <strong>injury</strong>and help those with persistent disabilities to achieve their maximumpotential and lead meaningful lives.TABLE 1.6Ten countermeasures and examples of <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>StrategyExample related to <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>1 Prevent the creati<strong>on</strong> of the hazard in the first place Banning the manufacture and sale of inherently unsafe products2 Reduce the amount of energy c<strong>on</strong>tained in the hazard Speed reducti<strong>on</strong>3 Prevent the release of the hazard Child-resistant medicine c<strong>on</strong>tainers4 Modify the rate or spatial distributi<strong>on</strong> of the hazard from its source Use of seat-belts and <strong>child</strong> restraints5 Separate people in time or space from the hazard and its release Bicycle and pedestrian pathways6 Separate people from the hazard by interposing a material barrier Window bars, pools fencing, covering wells7 Modify the relevant basic qualities of the hazard Softer playground surfaces8 Make the pers<strong>on</strong> more resistant to damage Good nutriti<strong>on</strong> for <strong>child</strong>ren9 Counter the damage already d<strong>on</strong>e by the hazard First aid treatment for scalds – “cool the burn”10 Stabilize, repair and rehabilitate the injured pers<strong>on</strong> Burn grafting, rec<strong>on</strong>structive surgery and physical therapyWORLD REPORT ON CHILD INJURY PREVENTION 13
BOX 1.5Dog bites: <strong>injury</strong> data reveal significant public health problemDog-bite <strong>injury</strong> has been the subject of very few scientific publicati<strong>on</strong>s. It was <strong>on</strong>ly after the introducti<strong>on</strong> of external cause coding of hospitalized<strong>injury</strong> cases and the setting up of emergency department <strong>injury</strong> surveillance systems that populati<strong>on</strong>-based rates of dog bites could be estimated.With greater <strong>injury</strong> surveillance and more country-wide or province-wide household surveys of injuries, the real burden of dog-bite <strong>injury</strong> is nowbecoming apparent. Death registrati<strong>on</strong> and <strong>injury</strong> surveillance data in high-income countries show that dog bites are a potentially serious <strong>injury</strong> anda frequent cause of hospitalizati<strong>on</strong>, but that they are <strong>on</strong>ly rarely fatal.Children are particularly vulnerable to dog attacks as a result of their size and the fact that their face is usually close to that of the dog. Bites to thehead and neck are comm<strong>on</strong> in small <strong>child</strong>ren and decrease with age (121).The table below summarizes the most comm<strong>on</strong> circumstances resulting in a dog bite.Source: reference 122In high-income countries, examples of <str<strong>on</strong>g>report</str<strong>on</strong>g>ed fatality rates from dog bites include:– Australia: 0.04 per 100 000 populati<strong>on</strong>;– Canada and the United States: 0.07 per 100 000 populati<strong>on</strong>.In these countries, <strong>child</strong>ren are over-represented. They account for 36% of dog-bite fatalities in Australia and between 70% and 80% in the UnitedStates (123). Similarly, published rates for hospitalizati<strong>on</strong> or emergency department visits in these high-income countries, as well as in some other places,highlight the over-representati<strong>on</strong> of <strong>child</strong>ren, with those aged 0–4 years, followed by those aged 5–9 years, the most vulnerable (121, 124).There are fewer <str<strong>on</strong>g>report</str<strong>on</strong>g>s specifically <strong>on</strong> dog-bite <strong>injury</strong> from low-income and middle-income countries. Recently, UNICEF and The Alliancefor Safe Children (TASC) collaborated with partner instituti<strong>on</strong>s in five Asian countries <strong>on</strong> community <strong>injury</strong> surveys. Such surveys supplement<strong>injury</strong> surveillance, and record more minor cases of bites and as well as those that are treated outside the hospital system by local practiti<strong>on</strong>ers,traditi<strong>on</strong>al healers orfamily members. Thesecommunity surveys haverevealed the previouslyunrecognized burden ofanimal-related <strong>injury</strong>, especiallyof dog bites,am<strong>on</strong>g <strong>child</strong>ren in low-incomeand middle-incomecountries. From these surveys,TASC has also estimatedthe number of dayslost from school or work,following an <strong>injury</strong>, for<strong>child</strong>ren aged between 0and 17 years. Data for thisage group from surveys infive countries estimate theanimal-related <strong>injury</strong> rateat 380 per 100 000 populati<strong>on</strong>,sec<strong>on</strong>d <strong>on</strong>ly to falls asa leading cause of time lostfrom school or work (19).© Gaggero/PAHOExternal circumstances of dog bitesCircumstance %Playing with or near the dog 28Passing the dog (walking) 14Cuddling the dog 10Feeding the dog 8Passing the dog (cycling) 4Disturbing the dog while eating 4Surprising the dog 2Pulling the dog’s tail 2Interfering during a dog fight 2Unknown 2614 WORLD REPORT ON CHILD INJURY PREVENTION
The 2001 community survey in Viet Nam showed that around 360 000 Vietnamese <strong>child</strong>ren suffer animal bites each year, with dog bites accounting foralmost 80% of these. Every day, some 30 <strong>child</strong>ren in Beijing suffer animal bites, 81% of them caused by pet dogs. While two decades ago dog ownershipwas not allowed in China, it is now comm<strong>on</strong>. The cost of treatment of such bites in Beijing has been estimated at US$ 4.2 milli<strong>on</strong> annually (19).Dog bites in poor countries come with the added risk of rabies. In countries where rabies is endemic – including India, China and many parts ofAfrica – a dog bite that may not otherwise be serious can lead to death. Rabies is the tenth most comm<strong>on</strong> cause of death from infecti<strong>on</strong> worldwide.More than 99% of the 55 000 annual worldwide deaths from rabies occur in Asia and Africa (125). There is evidence that between 30% and 60% ofthe victims of dog bites in endemic areas of canine rabies are <strong>child</strong>ren under 15 years of age (126).A study in New Delhi estimatedthe rate of rabies from animalbites at 80 per 100 000 populati<strong>on</strong>,and significantly higher for5–14-years-olds, with bites fromstray dogs accounting for 90% ofcases (127).A study of 2622 Thai <strong>child</strong>renwith rabies exposure found that86.3% of the cases were relatedto dog bites (128).A Ugandan study found that themajority of dog bites were to<strong>child</strong>ren under the age of 15 yearsand that these <strong>child</strong>ren were atgreater risk of developing rabies,in the absence of treatment, dueto the locati<strong>on</strong> of the bites theyhad suffered (129).A study from the United Republicof Tanzania showed that significantlymore <strong>child</strong>ren aged 5–15years are bitten by a suspectedrabid dog than are adults (130).Most <strong>child</strong>ren who die from rabies were either not treated or else received inadequate post-exposure treatment. Many bite victims do not receiverabies immunoglobulin because of a perennial global shortage. Its high price makes it frequently unaffordable in countries where canine rabies is endemic(126). In additi<strong>on</strong> to human vaccinati<strong>on</strong>, an estimated 50 milli<strong>on</strong> dogs are vaccinated against rabies worldwide, either privately or through governmentorganizedcampaigns (125). In some countries – including China, the Islamic Republic of Iran, Thailand, South Africa and much of Latin America – asustainable reducti<strong>on</strong> in dog rabies has been achieved by programmes of improved post-exposure treatment of humans and of c<strong>on</strong>trol measures againstdog rabies. In others, including Morocco, Sri Lanka and Tunisia, such activities have at least led to rabies being c<strong>on</strong>tained. However, in some African andAsian countries, vaccinati<strong>on</strong> coverage has reached <strong>on</strong>ly 30%–50% of the dog populati<strong>on</strong>, a level insufficient to break the disease transmissi<strong>on</strong> cycle.In additi<strong>on</strong> to training school-aged <strong>child</strong>ren, it is advisable to teach dog owners and parents to be alert when <strong>child</strong>ren are close to dogs. The blamefor a dog attack should not be placed <strong>on</strong> the <strong>child</strong>ren. The table below summarizes some of the behaviours older <strong>child</strong>ren can be taught in order tominimize attacks by dogs.Code of behaviour to prevent dog bitesCharacteristics of dogsInstructi<strong>on</strong>s to <strong>child</strong>renDogs sniff as a means of communicati<strong>on</strong>.Before petting a dog, let it sniff you.Dogs like to chase moving objects.Do not run past dogs.Dogs run faster than humans.Do not try to outrun a dog.Screaming may incite predatory behaviour.Remain calm if a dog approaches.Dogs may regard infants, especially new members of the family intoFor infants and small <strong>child</strong>ren, do not hug or kiss a dog.which the dog already feels integrated, as intruders or as subordinate.Direct eye c<strong>on</strong>tact may be interpreted as aggressi<strong>on</strong>.Avoid direct eye c<strong>on</strong>tact.Dogs tend to attack extremities, face and neck.If attacked, stand still (with feet together) and protect neck andface with arms and hands.Lying <strong>on</strong> the ground provokes attacks.Stand up. If attacked while lying, keep face down and cover the earswith the hands. Do not move.Fighting dogs bite at anything that is near.Do not try to stop two fighting dogs.Source: reference 122© WHOIn c<strong>on</strong>clusi<strong>on</strong>, dog-bite <strong>injury</strong> is a widespread and hitherto poorly-documented global problem, disproporti<strong>on</strong>ately affecting <strong>child</strong>ren and adolescents.Good data collecti<strong>on</strong> systems are vital for identifying the characteristics of injuries such as dog bites. Only when good data become availablecan the extent and nature of such injuries be appreciated and proper preventi<strong>on</strong> measures set up.WORLD REPORT ON CHILD INJURY PREVENTION 15
Learning from places with good safety recordsExperience from countries with the best safety recordsshows that positive leadership, together with widespread,multisectoral efforts to provide safer physical and socialenvir<strong>on</strong>ments can produce sustained reducti<strong>on</strong>s in <strong>injury</strong>mortality and morbidity (131). In additi<strong>on</strong>, those countrieswhich have a designated government focal point withoverall resp<strong>on</strong>sibility for addressing <strong>injury</strong> have madesignificant advances (132).Sweden was the first country to recognize theimportance of injuries as a threat to <strong>child</strong> health and totackle the problem in a coordinated manner (133). In the1950s, Sweden had death rates from <strong>child</strong> <strong>injury</strong> higherthan those in the United States. Since the late 1980s, it hashad the lowest <strong>child</strong> <strong>injury</strong> death rates of any country inthe world. Factors c<strong>on</strong>tributing to its success have included(134):– good surveillance data;– a commitment to research;– regulati<strong>on</strong>s and legislati<strong>on</strong> for safer envir<strong>on</strong>ments;– broad-based safety educati<strong>on</strong> campaigns involvingpartnerships of different agencies;– committed leadership <strong>on</strong> safety issues.In additi<strong>on</strong>, Sweden was <strong>on</strong>e of the few countries thatfollowed WHO’s recommendati<strong>on</strong>s to set up policiesfor safety, to organize a nati<strong>on</strong>al multisectoral safetypromoti<strong>on</strong> programme and to allow academic institutes toparticipate in public health policy-making (135). A senseof corporate resp<strong>on</strong>sibility in Sweden has greatly helpedin allowing the protecti<strong>on</strong> of <strong>child</strong>ren to become a majorgoal of society.There have been relatively few systematic attempts toexamine factors that might explain differences betweencountries in <strong>child</strong> <strong>injury</strong> rates. One example is theOECD study of road safety policy and practice. Thisused mortality data, demographic and socioec<strong>on</strong>omicindicators, exposure surveys and surveys based <strong>on</strong>questi<strong>on</strong>naires addressed to the leading informantsin transportati<strong>on</strong> departments in OECD countries.The study identified the pivotal role of good data. Thebest-performing countries in the study – those with thelowest <strong>injury</strong> rates – had a comprehensive, coordinatedpolicy <strong>on</strong> road traffic injuries and had adopted a holisticapproach (136). The importance of internati<strong>on</strong>alnetworks of researchers has also been identified toencourage the rapid disseminati<strong>on</strong> of ideas betweencountries (137).Which approaches work?Interventi<strong>on</strong>s to prevent unintenti<strong>on</strong>al injuries havetraditi<strong>on</strong>ally been c<strong>on</strong>sidered in terms of the “three E’s”:educati<strong>on</strong>, enforcement and engineering – and withinthe framework of the Hadd<strong>on</strong> matrix discussed before.While randomized c<strong>on</strong>trolled trials are c<strong>on</strong>sidered thegold standard for assessing the effectiveness of <strong>injury</strong>interventi<strong>on</strong>s, such trials are still relatively rare in relati<strong>on</strong>to <strong>child</strong> injuries. Many trials would be impractical orunethical to implement because their benefits are obvious.A recent publicati<strong>on</strong> <strong>on</strong> disease c<strong>on</strong>trol priorities indeveloping countries included a chapter <strong>on</strong> the preventi<strong>on</strong>of unintenti<strong>on</strong>al injuries in low-income and middle-incomecountries (138). Although the interventi<strong>on</strong>s suggested aspromising or proven are for all ages, many are applicableto the preventi<strong>on</strong> of <strong>child</strong> injuries.“Evidence is the foundati<strong>on</strong> for setting priorities, crafting policies, andmeasuring results. Evidence can have great persuasive power at thepolicy level” Dr Margaret Chan, WHO Director-General.The secti<strong>on</strong>s below summarize the approaches thathave been adopted in a number of countries. Examplesare given for each approach, al<strong>on</strong>g with evidence, whereavailable, from systematic reviews, using the Cochranedatabase of systematic reviews and other reviews.Legislati<strong>on</strong> and enforcementLegislati<strong>on</strong> is a powerful tool in the preventi<strong>on</strong> of <strong>injury</strong>.It can be regarded as a “test of commitment to the causeof <strong>child</strong> safety” (9). There is evidence that legislati<strong>on</strong> hasincreased the uptake of preventive measures and reduced<strong>child</strong>hood injuries in a number of areas. These areasinclude:In the road envir<strong>on</strong>ment:– <strong>child</strong> passenger restraints (139);– seat-belts (140);– bicycle helmets (141);– motorcycle helmets.In the home envir<strong>on</strong>ment:– smoke alarms (142);– hot water temperature legislati<strong>on</strong> (143);– <strong>child</strong>-resistant c<strong>on</strong>tainers (144). In the leisure envir<strong>on</strong>ment:– isolati<strong>on</strong> fencing of swimming pools (145).There is some evidence of the beneficial effect oflegislati<strong>on</strong> <strong>on</strong> the use of booster seats (restraints in carsfor <strong>child</strong>ren who have outgrown <strong>child</strong> seats), though thiswas mainly from unc<strong>on</strong>trolled before-and-after studies(146). A systematic review (147) found legislati<strong>on</strong> <strong>on</strong>bicycle helmets to be effective in increasing helmet use,particularly in the younger age group and in areas withprevious low rates of use (148), and in reducing headinjuries (141).As well as the introducti<strong>on</strong> of new laws, howc<strong>on</strong>sistently they are applied and how rigorouslyenforced are important. The UNICEF league table <str<strong>on</strong>g>report</str<strong>on</strong>g>compared the legislative record for seven areas of <strong>injury</strong>legislati<strong>on</strong> in 26 OECD countries. Only three countries16 WORLD REPORT ON CHILD INJURY PREVENTION
had legislated in at least six of the seven areas assessed:Australia, Canada and the United States (9).Many countries have specific standards or regulati<strong>on</strong>s– some mandatory – for a wide range of goods andservices, including:– toys and nursery furniture;– playground equipment;– items designed for <strong>child</strong>care – such as nail clippers andhair brushes;– safety equipment such as helmets;– furniture and furnishings – such as the provisi<strong>on</strong> ofbaby gates at the top of stairs.There are also usually regulati<strong>on</strong>s and standards relatedto c<strong>on</strong>structi<strong>on</strong> work <strong>on</strong> buildings, as well as to health andsafety generally in the workplace. All these standards andregulati<strong>on</strong>s have an important bearing <strong>on</strong> the extent towhich <strong>child</strong> <strong>injury</strong> can be prevented.Since, for many products, standards often do not exist,and the introducti<strong>on</strong> of standards for individual productscan be a slow process, a useful approach is to identifythe particular hazards for a product and the measuresand mechanisms that reduce risk. So-called “verticalstandards” based <strong>on</strong> hazards compile this informati<strong>on</strong>so that manufacturers and regulators can identify knownhazards in products and reduce them to acceptable levels.This approach is the <strong>on</strong>e adopted, for instance, in ISO/IECGuide 50: Safety aspects: guidelines for <strong>child</strong> safety (149).Risk reducti<strong>on</strong> here is meant to cover the way peopleactually use the products and it should be for the life ofthe product. In 2007, for example, there was a worldwiderecall of toys that had been found to c<strong>on</strong>tain hazardouslevels of lead paint.In developed countries, the way in which legislati<strong>on</strong> isenforced varies c<strong>on</strong>siderably. Because of a frequent lackof structures and resources, enforcement in developingcountries is even more difficult. In Karachi, a study of bussafety showed that legislati<strong>on</strong> was not likely to producemuch effect, but that instead increases in bus drivers’wages and small changes to the vehicles were potentiallymore effective (150).Product modificati<strong>on</strong>Changing the design and manufacture of products can:– reduce the risk of an <strong>injury</strong> – for instance, bymanufacturing staircase railings with the gap betweenthe upright banisters sufficiently narrow to preventsmall <strong>child</strong>ren putting their heads through;– reduce access to a hazard – an example being the use of<strong>child</strong>-resistant closures for medicines;– reduce the severity of an <strong>injury</strong> – for instance, bymodifying the design of the caps <strong>on</strong> pens to reduce therisk of fatal choking in the case of a cap being inhaled.Product modificati<strong>on</strong> has c<strong>on</strong>tributed to preventing<strong>child</strong>hood injuries. However, often a series of smallchanges is made in products and it is difficult to attributea reducti<strong>on</strong> in injuries to any <strong>on</strong>e specific change. Thereis c<strong>on</strong>siderable evidence that the introducti<strong>on</strong> of <strong>child</strong>resistantclosures has been effective in reducing thenumber of <strong>child</strong>hood deaths from pois<strong>on</strong>ing (151). Anevaluati<strong>on</strong> of an interventi<strong>on</strong> in South Africa involved thedistributi<strong>on</strong> of <strong>child</strong>-resistant c<strong>on</strong>tainers for the storageof paraffin. This strategy proved an effective means ofreducing paraffin ingesti<strong>on</strong> and provided evidence thatfamilies will use such free devices when they are provided(152).Modificati<strong>on</strong> of basic cooking and heating productsmay also offer c<strong>on</strong>siderable possibilities. About half theworld’s populati<strong>on</strong> still relies <strong>on</strong> solid fuels – includingwood, animal dung, crop residues and coal for every dayenergy needs – and a high proporti<strong>on</strong> of households burnthe fuel in open fires (153). In rural Guatemala, an improvedwood-burning stove, the plancha (an enclosed combusti<strong>on</strong>chamber and cooking surface out of reach of young<strong>child</strong>ren), has been introduced. The stove has the potentialto reduce not <strong>on</strong>ly acute lower respiratory tract infecti<strong>on</strong>sin <strong>child</strong>ren, but also burns and scalds. Preliminary resultshave been promising for young <strong>child</strong>ren (153). Reducingthe number of open fires would have a beneficial impactin places such as sub-Saharan Africa, where 80% to 90%of rural homes use open fires.“Adapting the envir<strong>on</strong>ment to the characteristics of <strong>child</strong>ren andintegrating safety into the design of products are am<strong>on</strong>g the mostsuccessful <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> strategies” Wim Rogmans, Director,C<strong>on</strong>sumer Safety Institute.Envir<strong>on</strong>mental modificati<strong>on</strong>Modifying the envir<strong>on</strong>ment to make it more user-friendlyhas become an important approach in <strong>injury</strong> preventi<strong>on</strong>,benefiting people of all ages, not just <strong>child</strong>ren, in thepassive protecti<strong>on</strong> that it affords. Area-wide engineeringsoluti<strong>on</strong>s can lower the rate of injuries in pedestrians,cyclists and car occupants. One review examined whethertraffic-calming schemes reduced rates of crash-relateddeaths and injuries, for all age groups (154). It c<strong>on</strong>cludedthat traffic calming in towns did indeed have the potentialto reduce the rate of injuries. As regards modificati<strong>on</strong> ofthe home envir<strong>on</strong>ment, there is at present insufficientevidence from trials to show that such changes reduce thenumber of injuries (155).In high-income countries, there has been c<strong>on</strong>siderableprogress in making the transport infrastructure safer,including around schools and kindergartens. But inlow-income countries, such expensive opti<strong>on</strong>s may notbe possible. In most low-income countries, pedestrians,cyclists, cars, animals and buses share the same roadspace. The c<strong>on</strong>flicting requirements of n<strong>on</strong>-motorizedvehicles need to be addressed using various models ofWORLD REPORT ON CHILD INJURY PREVENTION 17
traffic safety, including the separati<strong>on</strong> of different typesof road user (156).Supportive home visitsHome visiting by paediatric nurses to families at highrisk of <strong>injury</strong> has been used for a wide range of purposes.These include: to improve the home envir<strong>on</strong>ment, toprevent problems of <strong>child</strong> behaviour or supply and explainsafety equipment. A review of the effects of home visits inearly <strong>child</strong>hood has shown substantial positive effects forthe preventi<strong>on</strong> of <strong>child</strong> maltreatment (157). The greatestimpacts were for programmes using professi<strong>on</strong>al visitorsand for programmes of a l<strong>on</strong>ger durati<strong>on</strong>. Home-visitingprogrammes have been shown to be associated with animprovement in the quality of the home envir<strong>on</strong>ment as ameans to reduce unintenti<strong>on</strong>al injuries (158).Safety devicesThe promoti<strong>on</strong> of safety devices can lead to a fall in injuriesand increased compliance in using the device. A varietyof approaches has been used, including professi<strong>on</strong>alcounselling, to encourage the use of safety devices,supported by a range of media. Some programmes haveincluded rewards or coerci<strong>on</strong>, such as fines, to encouragecompliance. The positive effects from such programmesdiminish <strong>on</strong>e or two m<strong>on</strong>ths after the interventi<strong>on</strong> andmore intensive programmes produce more positiveresults (159).Wearing a bicycle helmet dramatically reduces the riskof severe and fatal head injuries and facial injuries forbicyclists involved in a crash involving a motor vehicle(148). Community-based projects that provided freehelmets al<strong>on</strong>g with an educati<strong>on</strong>al comp<strong>on</strong>ent led toan increase in the observed wearing of helmets (160). Astudy in Canada has shown that, despite less wearing ofhelmets in low-income areas, populati<strong>on</strong>-based bicyclehelmet campaigns can still have an impact in these areasin cutting the risk of <strong>injury</strong> (161). The WHO helmetmanual (162) provides a number of examples of goodpractice, such as the Helmets for Kids safety campaignin Viet Nam.Motorcyclists are also at high risk in traffic crashes,particularly for head <strong>injury</strong>. A review of studiesc<strong>on</strong>cluded that helmets reduce the risk of head <strong>injury</strong>by around 69% and death by around 42% (163).Fires detected with smoke alarms are associated withlower death rates. However, <strong>on</strong>e review found thatprogrammes to promote smoke alarms <strong>on</strong>ly, withoutlegislati<strong>on</strong>, functi<strong>on</strong> modestly, if at all, and have not yetdem<strong>on</strong>strated a reducti<strong>on</strong> in fires or fire-related injuries(142).Educati<strong>on</strong>, skills and behaviour changeThe value of educati<strong>on</strong>al programmes as a form of <strong>injury</strong>preventi<strong>on</strong> has been subject to debate in the field of <strong>child</strong><strong>injury</strong>. Clearly, educati<strong>on</strong> underpins many other strategies– such as legislati<strong>on</strong>, the promoti<strong>on</strong> of safety devices andhome visiting. Educati<strong>on</strong> <strong>on</strong> pedestrian safety can result inan improvement in <strong>child</strong>ren’s knowledge and can changeobserved behaviour of crossing roads. Whether, though,this reduces the risk of <strong>injury</strong> or of a pedestrian sufferinga collisi<strong>on</strong> with a motor vehicle is unknown (164). Thefocus of educati<strong>on</strong> should extend bey<strong>on</strong>d the immediatecaregivers of <strong>child</strong>ren, to include health professi<strong>on</strong>als,policy-makers, the media and the business community(120, 165). Novel ways of introducing safety messages intotelevisi<strong>on</strong> programmes should be explored. These mightinclude a pers<strong>on</strong> testing the water temperature beforebathing a <strong>child</strong>, portrayals of swimming pools surroundedby fencing, and characters in dramas putting <strong>on</strong> their seatbeltsin a car (166).The PRECEDE-PROCEED model (a planning modelfor health educati<strong>on</strong> and health promoti<strong>on</strong> programmes)provides a comprehensive structure to assess people’shealth and quality-of-life needs. It also helps in the design,implementati<strong>on</strong> and evaluati<strong>on</strong> of health promoti<strong>on</strong>programmes and other public health programmes tomeet those needs (167). These principles have been furtherelaborated in a guideline <strong>on</strong> generic behaviour change. Thisguideline recommends collaborati<strong>on</strong> between individuals,communities and organizati<strong>on</strong>s to plan interventi<strong>on</strong>s andprogrammes (168).Community-based studiesInjury preventi<strong>on</strong>, with its broad range of <strong>injury</strong>types and possible countermeasures, lends itself tocommunity-based approaches. It is important to havel<strong>on</strong>g-term strategies, effective and focused leadership,collaborati<strong>on</strong> between a range of agencies, appropriatetargeting and sufficient time to develop local networksand programmes (169). The use of multiple interventi<strong>on</strong>s,repeated in different forms and c<strong>on</strong>texts, can lead to aculture of safety being developed within a community.There is some evidence that the WHO SafeCommunities model is effective in reducing injuries inwhole populati<strong>on</strong>s (170). However, the countries that haveevaluated their Safe Communities with a sufficiently rigorousstudy design are am<strong>on</strong>g the wealthier countries andhave lower <strong>injury</strong> rates than most other countries. No evaluati<strong>on</strong>sare available yet from other parts of the world.Universal and targeted interventi<strong>on</strong>sThere have been a c<strong>on</strong>siderable number of systematicreviews of <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>. However, “theevidence <strong>on</strong> its own does not provide a complete recipe forsuccess, or an imperative for acti<strong>on</strong>” (171). The findings ofresearch need to be translated into practice, so that theyare tailored to local c<strong>on</strong>texts and circumstances (172).Proven interventi<strong>on</strong>s in developed countries may not bereadily transferable across all social groups or to other18 WORLD REPORT ON CHILD INJURY PREVENTION
c<strong>on</strong>texts within developed countries. They may also notbe transferable to developing countries. Cauti<strong>on</strong> is neededhere, because of the very different envir<strong>on</strong>ments in somelow-income countries (173). In these places, <strong>child</strong>hooddrowning, for instance, does not generally take place inswimming pools and bathtubs as in developed countries,but in natural bodies of water such as p<strong>on</strong>ds, lakes andrivers, as well as cisterns, wells, irrigati<strong>on</strong> ditches andpaddy fields.Closing the <strong>child</strong>hood <strong>injury</strong> gapAs stated previously, within all countries, the burden of <strong>child</strong><strong>injury</strong> falls most heavily <strong>on</strong> those from the most disadvantagedgroups. The gap in <strong>injury</strong> rates between the most affluentand the most disadvantaged provides “some measure ofpreventability and shows that there is c<strong>on</strong>siderable scope forimprovement and interventi<strong>on</strong> and a yardstick of what isachievable” (74).There is a range of interventi<strong>on</strong>s known to be effectivein preventing and reducing injuries (see Chapter 7). Whatis less well known, though, is how such approaches canbe applied to close the socioec<strong>on</strong>omic gap with regard to<strong>child</strong>hood injuries. It is partly in resp<strong>on</strong>se to this problem,where active strategies have not yet been successful, thatpassive soluti<strong>on</strong>s – that is, design soluti<strong>on</strong>s – may be mostsuccessful. In the broader field of health promoti<strong>on</strong>, fourbroad approaches to tackling socioec<strong>on</strong>omic inequalitiesin health have been suggested (174):– strengthening individuals;– strengthening communities;– improving access to services;– encouraging macroec<strong>on</strong>omic and cultural change.Approaches for strengthening individuals can includetargeting <strong>child</strong>ren and their carers.Preventi<strong>on</strong> initiatives for parents <strong>on</strong> drowning can beintegrated into existing <strong>child</strong> survival and developmentprogrammes – particularly for the period, from ninem<strong>on</strong>ths of age <strong>on</strong>wards, when <strong>child</strong>ren are entering intothe ‘window’ of drowning risk (61).A study c<strong>on</strong>ducted in a deprived community ofScotland, a high-income country, that reviewed atraining programme in practical road-safety skills,found improved skills in 5–7-year-old <strong>child</strong>ren incrossing the road (175).Strengthening communities is an approach adoptedby many organizati<strong>on</strong>s working <strong>on</strong> safety issues, and isthe leading strategy employed in the Safe Communitiesnetwork.The Waitakere Community Injury Preventi<strong>on</strong> Projectin New Zealand included a range of programmestargeting different indigenous and ethnic groups (176).For <strong>on</strong>e of these programmes, the coordinator employedwas a Maori, with experience of the culture andperspectives of the target group, and <strong>injury</strong> preventi<strong>on</strong>was incorporated into a holistic view of health.The Safe Block project, based in a poor African-American inner-city community in Philadelphia, PA,USA, used a network of community volunteers. Theproject involved making simple modificati<strong>on</strong>s to homesto prevent injuries, inspecting homes and providinginformati<strong>on</strong> <strong>on</strong> home hazards, and educating people– with the use of cascade training – <strong>on</strong> specific <strong>injury</strong>preventi<strong>on</strong> practices (177).A partnership with residents from townships in SouthAfrica worked effectively to lobby the local governmentto provide a pedestrian bridge over a highway (102).There are various ways in which improving access toservices can help prevent <strong>child</strong> injuries.New roads can c<strong>on</strong>tribute to improving access to arange of community services, including to health care,educati<strong>on</strong> and leisure facilities.Electrificati<strong>on</strong> can reduce exposure to more hazardousfuels such as kerosene.Removing dangerous debris and improving wastecollecti<strong>on</strong> can directly reduce injuries to <strong>child</strong>ren.Providing sanitati<strong>on</strong> can help <strong>child</strong>ren avoid having towalk in darkness to toilet facilities.Encouraging macroec<strong>on</strong>omic and cultural changeincludes:– broad land-use policies, such as locating schools awayfrom busy roads;– transport policies that take into full account the needsof pedestrians;– the promoti<strong>on</strong> of walking as a healthy activity;– the design of communities, to include safe outdoor playfacilities.Financial problems and poor living c<strong>on</strong>diti<strong>on</strong>s havebeen found to preoccupy adults, with the result that theyspend less time supervising <strong>child</strong>ren (24, 76). Policiestargeting poverty reducti<strong>on</strong> could reduce <strong>child</strong>hoodinjuries in the l<strong>on</strong>g term, but need to be accompanied bymore short-term and medium-term measures.Most researchers believe that packages of policies andinterventi<strong>on</strong>, rather than single policies and interventi<strong>on</strong>s,are needed to substantially reduce socioec<strong>on</strong>omicinequalities in health.Transfer of knowledgeOne study in low-income countries looked at successfulinterventi<strong>on</strong>s to prevent transport and home injuries(25). It also evaluated <strong>injury</strong> interventi<strong>on</strong>s developedin industrialized countries that might be usable inlow-income countries. The c<strong>on</strong>clusi<strong>on</strong> was that severalinterventi<strong>on</strong>s could be imported by low-income countriesand should be c<strong>on</strong>sidered, including:– vehicle seat-belts, bicycle helmets and motorcyclehelmets;WORLD REPORT ON CHILD INJURY PREVENTION 19
– speed limits;– pedestrian crossing signs;– adequate road lighting;– the separati<strong>on</strong> of pedestrians from vehicles;– measures to enhance c<strong>on</strong>spicuity, such as the use ofreflective products;– simple safety equipment;– packaging of items to prevent pois<strong>on</strong>ing.The importance of transferring knowledge in a sensitiveand c<strong>on</strong>text-specific manner has been repeatedly stressed.The Commissi<strong>on</strong> for Global Road Safety (44), for instance,has stated: “Public acceptance and support, based <strong>on</strong>informati<strong>on</strong> and knowledge and evidence of effectiveness,will be achieved <strong>on</strong>ly if road safety messages are seen to beappropriate and targeted at local needs”.Interventi<strong>on</strong>s that appear most effective are thoseencompassing a variety of strategies, including legislati<strong>on</strong>,envir<strong>on</strong>mental modificati<strong>on</strong> and educati<strong>on</strong> (178, 179).There is a general need for more interventi<strong>on</strong>s to beevaluated and for research experiences to be sharedworldwide. Many of the principles of <strong>injury</strong> preventi<strong>on</strong>can be transferred, but interventi<strong>on</strong>s need to be tailoredto the social and physical envir<strong>on</strong>ments of those localities.Interventi<strong>on</strong>s should reach across different sectors, build<strong>on</strong> existing networks and involve communities.Cost and cost-effectivenessThe costs of injuries are enormous. In developingcountries, road traffic injuries al<strong>on</strong>e account for 1%–2% ofgross domestic product (about US$ 100 billi<strong>on</strong>) each year,or twice the total development aid received worldwide bydeveloping countries (180). There are no global data <strong>on</strong> thecost of unintenti<strong>on</strong>al <strong>child</strong> injuries, but a recent evaluati<strong>on</strong>in the United States has shown that the medical costs andlosses in productivity as a result of all injuries to 0–14-yearoldsare in the range of US$ 50 billi<strong>on</strong> (181). There is thus agreat need for cost-effective and well-targeted resp<strong>on</strong>ses.Costs of safetyNot much research has been carried out <strong>on</strong> the availability,price and affordability of <strong>child</strong>-safety or family-safetydevices, and this is especially the case in low-income andmiddle-income countries. Data from 18 ec<strong>on</strong>omicallydiverse countries have been compared for four effectivedevices: <strong>child</strong> safety seats, booster seats, <strong>child</strong> bicyclehelmets and smoke alarms (182). The prices of thesedevices varied widely and in many countries they werevery expensive. A factory worker in a low-income countryhad to work 11 times as l<strong>on</strong>g as a counterpart in a highincomecountry to buy a bicycle helmet, while for a <strong>child</strong>safety seat 16 times as many hours’ work were required.Low-income countries manufacturing devices for exportdid not generally use spare plant capacity to producedevices for local c<strong>on</strong>sumpti<strong>on</strong>.Cost-effectiveness of interventi<strong>on</strong>sThere are very few analyses in low-income and middleincomecountries of the cost-effectiveness of <strong>injury</strong>preventi<strong>on</strong> measures (183). There is also scarce data <strong>on</strong><strong>injury</strong> epidemiology and the efficacy of interventi<strong>on</strong>s inthese countries. One study attempted to model the costsand effectiveness of five interventi<strong>on</strong>s for which therewere data <strong>on</strong> effectiveness in a low-income or middleincomecountry (184). Four out of the five interventi<strong>on</strong>srelated to the road envir<strong>on</strong>ment: vehicle speed c<strong>on</strong>trol,treatment of dangerous juncti<strong>on</strong>s, bicycle helmetlegislati<strong>on</strong> and motorcycle helmet legislati<strong>on</strong>. The fifthwas <strong>on</strong> the home envir<strong>on</strong>ment, and involved <strong>child</strong>resistantc<strong>on</strong>tainers to reduce pois<strong>on</strong>ing from paraffin.In the United States, a survey c<strong>on</strong>ducted in the late1990s <strong>on</strong> the costs of <strong>child</strong>hood unintenti<strong>on</strong>al injuriesand the cost-effectiveness of interventi<strong>on</strong>s to preventthem showed that approximately 15% of medicalspending resulted from an <strong>injury</strong> (185). The same studyfound that seven <strong>child</strong> <strong>injury</strong> safety measures – <strong>child</strong>safety seats, bicycle helmets, zero tolerance of alcohol foryoung drivers, provisi<strong>on</strong>al licensing, smoke detectors,<strong>child</strong>proof cigarette lighters and pois<strong>on</strong> c<strong>on</strong>trol centres– had similar cost-effectiveness ratios to other wellacceptedstrategies to prevent <strong>child</strong>hood illness. Theimplementati<strong>on</strong> of these strategies, though, is not yetwidespread (185). As can be seen from Table 1.7, manycost-effective strategies for unintenti<strong>on</strong>al <strong>injury</strong> can savenot <strong>on</strong>ly lives but costs to society as well.TABLE 1.7Financial savings from selected <strong>injury</strong> preventi<strong>on</strong> interventi<strong>on</strong>sExpenditure of US$ 1 each <strong>on</strong>:Savings (US$)Smoke alarms 65Child restraints 29Bicycle helmets 29Preventi<strong>on</strong> counselling by paediatricians 10Pois<strong>on</strong> c<strong>on</strong>trol services 7Road safety improvements 3Source: reference 186.Cost and cost-effectiveness analysis of interventi<strong>on</strong>sto reduce or mitigate <strong>child</strong> injuries is urgently called for.Such evidence can have a str<strong>on</strong>g impact <strong>on</strong> policy-makersand persuade them to invest in the appropriate primarypreventi<strong>on</strong> interventi<strong>on</strong>s.Overcoming the obstaclesAlthough c<strong>on</strong>siderable progress has been made duringrecent decades to reduce the rates of <strong>child</strong> death and<strong>injury</strong> in developed countries, more needs to be d<strong>on</strong>e. In20 WORLD REPORT ON CHILD INJURY PREVENTION
developing countries such efforts are just beginning. Thissecti<strong>on</strong> examines some of the fallacies, limitati<strong>on</strong>s andother obstacles that efforts to prevent <strong>child</strong> <strong>injury</strong> face.“Injuries are due to fate”If <strong>injury</strong> is c<strong>on</strong>sidered to be the result of random,unc<strong>on</strong>trolled factors and that chance and bad luck or fateare the main factors, then there is little that can be d<strong>on</strong>eto prevent <strong>injury</strong>.However, injuries are preventable. The public healthapproach to <strong>injury</strong> preventi<strong>on</strong> involves data collecti<strong>on</strong>,risk factor analysis, interventi<strong>on</strong>, evaluati<strong>on</strong> and thewidespread implementati<strong>on</strong> of proven preventi<strong>on</strong>methods. Scientific research and evidence underpin thisapproach.The wide range of <strong>injury</strong> typesThe nature of <strong>injury</strong> presents problems. Injuries fall intoa wide range of categories that occur in many differentenvir<strong>on</strong>ments. They can therefore be the resp<strong>on</strong>sibility of anumber of separate agencies or government departments,each of which may favour a different approach.Injuries need to be viewed collectively as a single“disease”, with broadly similar approaches being used toprevent them. Collaborati<strong>on</strong> between a range of agenciesis necessary, with some form of principal agency tocoordinate activities.Limitati<strong>on</strong>s of dataData <strong>on</strong> the scope and patterns of <strong>injury</strong> are essentialfor identifying priority issues, understanding the causesof <strong>injury</strong> and identifying groups at high risk of <strong>injury</strong>.With limited data it is difficult to c<strong>on</strong>vince policymakersand others that there is an <strong>injury</strong> problem. It isalso impossible to decide how to prioritize and developeffective programmes.It is estimated that, of the 193 WHO Member States,<strong>on</strong>ly 109 currently provide usable vital registrati<strong>on</strong> data toWHO in coded form, using the Internati<strong>on</strong>al Classificati<strong>on</strong>of Disease tax<strong>on</strong>omy. Unfortunately, the quality of thedata tends to be weakest where the problems are greatest.In developing countries, data coverage is particularly poorin relati<strong>on</strong> to <strong>child</strong> drowning, burns, pois<strong>on</strong>ing, roadtraffic injuries and bites and stings. Data <strong>on</strong> the evaluati<strong>on</strong>of interventi<strong>on</strong>s and the cost of injuries are also largelyabsent or – at best – are weak in these places. High-qualitydata relating to hospital usage are similarly skewed. Theyare available in some high-income countries, but rare incountries with the highest <strong>injury</strong> rates.The general lack of data <strong>on</strong> health care, in particular<strong>on</strong> high-cost hospital admissi<strong>on</strong>s and trauma care, resultsin the burden of <strong>injury</strong> being underestimated in manycountries. It also prevents a proper analysis being madeof the groups receiving such expensive and scarce healthcare and of the nature of their injuries. A high proporti<strong>on</strong>of trauma deaths occur outside hospital in developingcountries, so that many deaths – and other injuries – arenot counted in data collecti<strong>on</strong> systems in these countries.An important goal in <strong>injury</strong> preventi<strong>on</strong> is thus toestablish reliable estimates of the level and pattern of <strong>child</strong><strong>injury</strong> and death, especially in low-income and middleincomecountries. To this end, the volume, quality andavailability of nati<strong>on</strong>al and regi<strong>on</strong>al data needs to beincreased. This should be d<strong>on</strong>e through a combinati<strong>on</strong>of better data collecti<strong>on</strong> systems, improved hospitalsurveillance, more community-based surveys and otherappropriate research.Lack of political commitment and understandingThe significance of <strong>child</strong> <strong>injury</strong> in absolute and relativeterms is not always widely appreciated and the possibilitiesof preventi<strong>on</strong> are often underestimated. This lack ofunderstanding inhibits the allocati<strong>on</strong> of resources topreventi<strong>on</strong> efforts and also the political and organizati<strong>on</strong>alwill that are necessary for change.Injury must become an issue for c<strong>on</strong>cern and debateat all levels, not just at the global level, but at nati<strong>on</strong>al andlocal levels as well. One example of high-level politicalcommitment that led to immediate and observablereducti<strong>on</strong>s in <strong>injury</strong> was in France, where in 2002 thepresident declared road safety a nati<strong>on</strong>al priority. This ledto the formati<strong>on</strong> of an interministerial committee and anati<strong>on</strong>al acti<strong>on</strong> plan (131). Between 2002 and 2004, a 34%reducti<strong>on</strong> in road traffic deaths was <str<strong>on</strong>g>report</str<strong>on</strong>g>ed, as a result ofthe coordinated implementati<strong>on</strong> of a range of preventivemeasures, including: speed reducti<strong>on</strong>, traffic calming,c<strong>on</strong>trol of drinking and driving, and increased seat-belt use(187).Effective and inexpensive interventi<strong>on</strong>s must bedeveloped (188). The aim should be to develop measuresthat give as much return <strong>on</strong> m<strong>on</strong>ey invested as immunizing<strong>child</strong>ren against measles, polio or tetanus.Limited capacityAll countries face limitati<strong>on</strong>s in their capacity to prevent<strong>injury</strong>, to provide emergency and c<strong>on</strong>tinuing care followingan <strong>injury</strong>, and to provide appropriate rehabilitati<strong>on</strong>services. This is particularly the case in countrieswhere the burden of <strong>child</strong> <strong>injury</strong> is greatest. The trainingof more <strong>injury</strong> preventi<strong>on</strong> practiti<strong>on</strong>ers and researchersacross the world is urgently needed, and particularly inlow-income and middle-income countries. For low-incomecountries, incentives may be necessary to encourageprofessi<strong>on</strong>als to remain in their country of origin and notemigrate to high-income countries.The c<strong>on</strong>tent of training courses also needs to be carefullyplanned. Such syllabuses generally include principles andc<strong>on</strong>cepts that further knowledge and understanding.Competencies, though, also need to be taught, includingskills in group work, community development, collaborati<strong>on</strong>across sectors and lobbying.WORLD REPORT ON CHILD INJURY PREVENTION 21
Difficulties of implementati<strong>on</strong>As already stated, the main aim in <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>is the adaptati<strong>on</strong> of proven preventi<strong>on</strong> measures to localcircumstances. In areas of the world where substantialprogress has already been made, efforts are requiredto apply effective interventi<strong>on</strong>s more widely. A recentanalysis c<strong>on</strong>ducted in the United States showed that <strong>child</strong><strong>injury</strong> deaths could be reduced by <strong>on</strong>e third if practicesthat had proved effective in certain states were adopted inother similar states (189).Lack of fundingFunding levels need to reflect the importance of <strong>injury</strong> asa major cause of death and ill-health in <strong>child</strong>ren. “Thosewho c<strong>on</strong>trol the purse strings must be persuaded that mostinjuries are truly preventable and that the cost of failingto do so greatly outweighs the relatively small costs ofpreventi<strong>on</strong>” (190).C<strong>on</strong>clusi<strong>on</strong>Despite the many and complex obstacles, <strong>injury</strong>preventi<strong>on</strong> nevertheless offers opportunities. The publichealth significance of road traffic <strong>injury</strong> and of violencehas increasingly been recognized in recent years. Therehas been much experience and understanding developed<strong>on</strong> all aspects of <strong>injury</strong> preventi<strong>on</strong>. These developmentscan create a str<strong>on</strong>g basis to bring about significant andsustainable reducti<strong>on</strong>s in <strong>child</strong> mortality and ill-healththroughout the world.All countries need to urgently investigate the full extentof the problem of <strong>child</strong> injuries. Their results should beused in developing an acti<strong>on</strong> plan, coordinating theactivities of different sectors – including n<strong>on</strong>governmentalorganizati<strong>on</strong>s, academic instituti<strong>on</strong>s and industry.Measures that are known to work should be implementedeverywhere, with adaptati<strong>on</strong>s where necessary to suit localcircumstances.Resources devoted to <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> must beappropriate for the size of the problem. More investmentis needed for such activities as data collecti<strong>on</strong>, communitybased<strong>injury</strong> surveys, capacity building, programmes aimedat local communities, and evaluati<strong>on</strong>s of the costs of injuriesand of the cost-effectiveness of preventi<strong>on</strong> measures.Child survival initiatives have been highly successful.At the beginning of the “<strong>child</strong> survival revoluti<strong>on</strong>”, morethan 75% of the world’s <strong>child</strong>ren lived in countries where<strong>child</strong> mortality was high – while now, <strong>on</strong>ly 30 years later,less than 20% of <strong>child</strong>ren do so. Further improvements in<strong>child</strong> health, though, will require broad programmes for<strong>injury</strong> reducti<strong>on</strong> and c<strong>on</strong>trol for <strong>child</strong>ren up to the age of18 years.Now is the right time to address this avoidable harm to<strong>child</strong>ren and to society. While there is much research thatstill needs to be carried out, there is already c<strong>on</strong>siderableinformati<strong>on</strong> available. This informati<strong>on</strong> is quite sufficientto make a substantial impact in bringing down theincidence of <strong>child</strong> <strong>injury</strong> death and morbidity.Every <strong>child</strong> lost to <strong>injury</strong> or severely disabled will costthe future ec<strong>on</strong>omy of that country. Putting into practicewhat is known about reducing <strong>child</strong> <strong>injury</strong> will helpmeet the Millennium Development Goals. It will reducecosts in the health care system, improve the capacity tomake further reducti<strong>on</strong>s in <strong>injury</strong> rates, and will mostimportantly protect <strong>child</strong>ren.Chapters 2 to 6 of this <str<strong>on</strong>g>report</str<strong>on</strong>g> will discuss the fiveleading causes of unintenti<strong>on</strong>al <strong>injury</strong>. These will focus<strong>on</strong> the magnitude of the problem, the risk and protectivefactors for each type of <strong>injury</strong>, as well as interventi<strong>on</strong>s andrecommendati<strong>on</strong>s for primary, sec<strong>on</strong>dary and tertiarypreventi<strong>on</strong>.References1. Baker SP et al., eds. The <strong>injury</strong> fact book, 2nd ed. Lexingt<strong>on</strong>,MA, Lexingt<strong>on</strong> Books, 1992.2. Pinheiro PS. <str<strong>on</strong>g>World</str<strong>on</strong>g> <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> violence against <strong>child</strong>ren.Geneva, Switzerland, Secretary-General’s Study<strong>on</strong> Violence against Children, 2006 (http://www.violencestudy.org/a553, accessed 21 January 2008).3. C<strong>on</strong>venti<strong>on</strong> <strong>on</strong> the Rights of the Child. New York, NY,United Nati<strong>on</strong>s, 1989 (A/RES/44/25) (http://www.unhchr.ch/html/menu3/b/k2crc.htm, accessed 21 January 2008).4. James A, Prout A. C<strong>on</strong>structing and rec<strong>on</strong>structing<strong>child</strong>hood: c<strong>on</strong>temporary issues in the sociological study of<strong>child</strong>hood. L<strong>on</strong>d<strong>on</strong>, Falmer, 1990.5. Kabeer N, Nambissan GB, Subrahmanian R. Child labourand the right to educati<strong>on</strong> in South Asia. New Delhi, Sage,2003.6. Lansdown G. The evolving capacities of the <strong>child</strong>. Florence,UNICEF Innocenti Research Centre, 2005 (http://www.unicef-irc.org/publicati<strong>on</strong>s/pdf/evolving-eng. pdf, accessed21 January 2008).7. Tamburlini G. Children’s special vulnerability toenvir<strong>on</strong>mental health hazards: an overview. In: TamburliniG, v<strong>on</strong> Ehrenstein O, Bertollini R, eds. Children’s healthand envir<strong>on</strong>ment: a review of evidence. Rome, EuropeanEnvir<strong>on</strong>ment Agency, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>Regi<strong>on</strong>al Office for Europe, 2002 [Envir<strong>on</strong>mental IssueReport 29].8. Alders<strong>on</strong> P. Young <strong>child</strong>ren’s rights: exploring beliefs,principles and practice. L<strong>on</strong>d<strong>on</strong>, Kingsley, 2000.9. A league table of <strong>child</strong> deaths by <strong>injury</strong> in rich countries.Innocenti <str<strong>on</strong>g>report</str<strong>on</strong>g> card No. 2. Florence, UNICEF InnocentiResearch Centre, 2001 (http://www.unicef-icdc.org/publicati<strong>on</strong>s/pdf/repcard2e.pdf, accessed 22 January2008).10. Linnan M et al. Child mortality and <strong>injury</strong> in Asia:survey results and evidence. Florence, UNICEF InnocentiResearch Centre, 2007 (http://www.unicef-irc.org/publicati<strong>on</strong>s/pdf/iwp_2007_06.pdf, accessed 21 January22 WORLD REPORT ON CHILD INJURY PREVENTION
2008). (Innocenti Working Paper 2007-06, Special series<strong>on</strong> <strong>child</strong> <strong>injury</strong> No. 3).11. Krug EG et al., eds. <str<strong>on</strong>g>World</str<strong>on</strong>g> <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> violence and health.Geneva, Switzerland, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2002(http://www.who.int/entity/violence_<strong>injury</strong>_preventi<strong>on</strong>/violence/world_<str<strong>on</strong>g>report</str<strong>on</strong>g>/en/full_en.pdf, accessed 18 December2007).12. Peden M et al., eds. <str<strong>on</strong>g>World</str<strong>on</strong>g> <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> road traffic <strong>injury</strong>preventi<strong>on</strong>. <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, Geneva, 2004(http://www.who.int/violence_<strong>injury</strong>_preventi<strong>on</strong>/publicati<strong>on</strong>s/road_traffic/world_<str<strong>on</strong>g>report</str<strong>on</strong>g>/en/index.html,accessed 18 December 2007).13. Resoluti<strong>on</strong> WHA56.24. Implementing the recommendati<strong>on</strong>sof the <str<strong>on</strong>g>World</str<strong>on</strong>g> <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> violence and health. In:Fifty-sixth <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Assembly resoluti<strong>on</strong>, Geneva,19–28 May 2003. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>,2003 (http://www.who.int/gb/ebwha/pdf_files/WHA56/ea56r24.pdf, accessed 22 January 2008).14. Resoluti<strong>on</strong> WHA 57.10. Road safety and health. In: Fiftyseventh<str<strong>on</strong>g>World</str<strong>on</strong>g> Health Assembly, Geneva, 17–22 May 2004.Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2004 (http://www.who.int/gb/ebwha/pdf_files/WHA57/A57_R10-en. pdf,accessed 22 January 2008).15. United Nati<strong>on</strong>s Millennium Declarati<strong>on</strong>. New York, NY,United Nati<strong>on</strong>s, 2000 (A/RES/55/2) (http://www.un.org/millennium/declarati<strong>on</strong>/ares552e.htm, accessed 22 January2008).16. A world fit for <strong>child</strong>ren. New York, NY, United Nati<strong>on</strong>sGeneral Assembly, 2002 (A/RES/S-27/2) (http://www.unicef.org/specialsessi<strong>on</strong>/docs_new/documents/A-RES-S27-2E. pdf, accessed 18 February 2008).17. The Bellagio Group <strong>on</strong> Child Survival. The Lancet series.Child survival [WHO press release]. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> HealthOrganizati<strong>on</strong> (http://www.who.int/<strong>child</strong>-adolescent-health/NEWS/news_27. htm, accessed 22 January 2008).18. J<strong>on</strong>es G et al. How many <strong>child</strong> deaths can we prevent thisyear? The Lancet, 2003, 362:65–71.19. Linnan M et al. Child mortality and <strong>injury</strong> in Asia: policyand programme implicati<strong>on</strong>s. Florence, UNICEF InnocentiResearch Centre, 2007 (http://www.unicef-irc.org/publicati<strong>on</strong>s/pdf/iwp_2007_07.pdf, accessed 21 January2008). (Innocenti Working Paper 2007-07, Special series<strong>on</strong> <strong>child</strong> <strong>injury</strong> No. 4).20. McFarland RA. Epidemiologic principles applicable tothe study and preventi<strong>on</strong> of <strong>child</strong> accidents. AmericanJournal of Public Health, 1955, 45:1302–1308.21. The preventi<strong>on</strong> of accidents in <strong>child</strong>hood. Report of aseminar, Spa, Belgium 16–25 July 1958. Copenhagen,<str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong> Regi<strong>on</strong>al Office for Europe,1960.22. Peden MM, Scott I, Krug E, eds. Injury: a leading causeof the global burden of disease, 2002. <str<strong>on</strong>g>World</str<strong>on</strong>g> HealthOrganizati<strong>on</strong>, Geneva, 2006 (http://whqlibdoc.who.int/publicati<strong>on</strong>s/2002/9241562323.pdf, accessed 21 January2008).23. Child and adolescent <strong>injury</strong> preventi<strong>on</strong>: a global call toacti<strong>on</strong>. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2005 (http://whq.libdoc.who.int/publicati<strong>on</strong>s/2005/9241593415_eng.pdf, accessed 22 January 2008).24. Berger LR, Mohan D, eds. Injury c<strong>on</strong>trol: a global view.Delhi, Oxford University Press, 1996.25. Forjuoh S, Guohua L. A review of successful transport andhome <strong>injury</strong> interventi<strong>on</strong>s to guide developing countries.Social Science and Medicine, 1996, 43:1551–1560.26. Bettcher D, Lee K. Globalisati<strong>on</strong> and public health. Journalof Epidemiology and Community Health, 2002, 56:8–17.27. Scholte JA. Globalizati<strong>on</strong>: a critical introducti<strong>on</strong>. L<strong>on</strong>d<strong>on</strong>,Macmillan, 2000.28. Lab<strong>on</strong>te R, Schrecker T. Globalizati<strong>on</strong> and socialdeterminants of health: analytic and strategic review paper.Ottawa, Institute of Populati<strong>on</strong> Health, 2006 (http://www.who.int/social_determinants/resources/globalizati<strong>on</strong>.pdf, accessed 21 January 2008).29. Bettcher D, Wipfli H. Towards a more sustainableglobalisati<strong>on</strong>: the role of the public health community.Journal of Epidemiology and Community Health, 2001,55:617–618.30. Roberts I. Injury and globalisati<strong>on</strong>. Injury Preventi<strong>on</strong>,2004, 10:65–66.31. Neumayer E, de Soysa I. Trade openness, foreign directinvestment and <strong>child</strong> labor. <str<strong>on</strong>g>World</str<strong>on</strong>g> Development, 2005,33:43–63.32. The end of <strong>child</strong> labour: within our reach. Report of theDirector-General, Internati<strong>on</strong>al Labour C<strong>on</strong>ference, 95thSessi<strong>on</strong>. Geneva, Internati<strong>on</strong>al Labour Organizati<strong>on</strong>,2006 (http://www.ilo.org/public/english/standards/relm/ilc/ilc95/pdf/rep-i-b.pdf, accessed 5 May 2008).33. Kambhampati US, Rajan R. Ec<strong>on</strong>omic growth: a panaceafor <strong>child</strong> labor? <str<strong>on</strong>g>World</str<strong>on</strong>g> Development, 2006, 34:426–445.34. Swaminathan M. Ec<strong>on</strong>omic growth and the persistenceof <strong>child</strong> labour: evidence from an Indian city. <str<strong>on</strong>g>World</str<strong>on</strong>g>Development, 1998, 26:1513–1528.35. Gracey M. Child health in an urbanizing world. ActaPaediatrica, 2002, 91:1–8.36. <str<strong>on</strong>g>World</str<strong>on</strong>g> urbanizati<strong>on</strong> prospects: the 1999 revisi<strong>on</strong>. New York,NY, United Nati<strong>on</strong>s Populati<strong>on</strong> Divisi<strong>on</strong>, 2000 (http://www.un.org/esa/populati<strong>on</strong>/publicati<strong>on</strong>s/wup1999/urbanizati<strong>on</strong>.pdf, accessed 22 January 2008).37. <str<strong>on</strong>g>World</str<strong>on</strong>g> populati<strong>on</strong> policies 2003. New York, NY, UnitedNati<strong>on</strong>s Department of Ec<strong>on</strong>omic and Social Affairs,Populati<strong>on</strong> Divisi<strong>on</strong>, 2004 (http://www.un.org/esa/populati<strong>on</strong>/publicati<strong>on</strong>s/wpp2003/Publicati<strong>on</strong>_index.htm, accessed 22 January 2008).38. Chowla L. Growing up in an urbanising world. L<strong>on</strong>d<strong>on</strong>,Earthscan Publicati<strong>on</strong>s, UNESCO, 2002.39. Stark O. The migrati<strong>on</strong> of labour. Oxford, Blackwell, 1991.40. Chaplin SE. Cities, sewers and poverty: India’s politics ofsanitati<strong>on</strong>. Envir<strong>on</strong>ment and Urbanizati<strong>on</strong>, 1999, 11:145–158.WORLD REPORT ON CHILD INJURY PREVENTION 23
41. McMichael AJ. The urban envir<strong>on</strong>ment and health in aworld of increasing globalizati<strong>on</strong>: issues for developingcountries. Bulletin of the <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>,2000, 78:1117–1126.42. Reichanheim ME, Harpham T. Child accidents andassociated risk factors in a Brazilian squatter settlement.Health Policy and Planning, 1989, 4:162–167.43. Rizvi N et al. Distributi<strong>on</strong> and circumstances of injuriesin squatter settlements of Karachi, Pakistan. AccidentAnalysis and Preventi<strong>on</strong>, 2006, 38:526–531.44. Make roads safe: a new priority for sustainable development.L<strong>on</strong>d<strong>on</strong>, Commissi<strong>on</strong> for Global Road Safety, 2006 (http://www.makeroadssafe.org/documents/make_roads_safe_low_res.pdf, accessed <strong>on</strong> 21 January 2008).45. van de Walle D. Choosing rural road investments to helpreduce poverty. <str<strong>on</strong>g>World</str<strong>on</strong>g> Development, 2002, 30:575–589.46. Task Team <strong>on</strong> Infrastructure for Poverty Reducti<strong>on</strong>.Guiding principles <strong>on</strong> using infrastructure to reduce poverty.Paris, OECD, Development Co-operati<strong>on</strong> Directorate,2006 (http://www.oecd.org/dataoecd/43/45/36427725.pdf,accessed 22 January 2008).47. Our comm<strong>on</strong> interest. Report of the Commissi<strong>on</strong> forAfrica. L<strong>on</strong>d<strong>on</strong>, Commissi<strong>on</strong> for Africa, 2005 (http://www.commissi<strong>on</strong>forafrica.org/english/<str<strong>on</strong>g>report</str<strong>on</strong>g>/the<str<strong>on</strong>g>report</str<strong>on</strong>g>/english/11-03-05_cr_<str<strong>on</strong>g>report</str<strong>on</strong>g>. pdf, accessed 21 January2008).48. Hought<strong>on</strong> J. Global warming: the complete briefing, 3rd ed.Cambridge, Cambridge University Press, 2004.49. Bunyavanich S, Landrigan C, McMichael A. The impactof climate change <strong>on</strong> <strong>child</strong> health. Ambulatory Pediatrics,2003, 3:44–52.50. Prüss-Ürsün A, Corvalán C. Preventing disease throughhealthy envir<strong>on</strong>ments. Towards an estimate of theenvir<strong>on</strong>mental burden of disease. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> HealthOrganizati<strong>on</strong>, 2006.51. Corvalan C, Hales S, McMichael A. Ecosystems andhuman well-being: health synthesis. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> HealthOrganizati<strong>on</strong>, 2005 (http://www.who.int/globalchange/ecosystems/ecosystems05/en/index.html, accessed 21January 2008).52. McMichael AJ, Haines A. Global climate change: thepotential effects <strong>on</strong> health. British Medical Journal, 1997,315:805–809.53. Patz JA et al. The potential health impacts of climatevariability and change for the United States: executivesummary of the <str<strong>on</strong>g>report</str<strong>on</strong>g> of the health sector of the USNati<strong>on</strong>al Assessment. Envir<strong>on</strong>mental Health Perspectives,2000, 108:367–376.54. Haines A et al. Climate change and human health:impacts, vulnerability and public health. Public Health,2006, 120:585–596.55. Roberts I, Hillman M. Climate change: the implicati<strong>on</strong>s for<strong>injury</strong> c<strong>on</strong>trol and health promoti<strong>on</strong>. Injury Preventi<strong>on</strong>,2005, 11:326–329.56. McCarthy J et al., eds. Climate change 2001: impacts,adaptati<strong>on</strong> and vulnerability. Cambridge, CambridgeUniversity Press, 2001 (http://www.grida.no/climate/ipcc_tar/wg2/index.htm, accessed 21 January 2008).57. Gord<strong>on</strong> JE. The epidemiology of accidents. AmericanJournal of Public Health, 1949, 39:504–515.58. Nati<strong>on</strong>al Committee for Injury Preventi<strong>on</strong> and C<strong>on</strong>trol.Injury preventi<strong>on</strong>: meeting the challenge. New York,Oxford University Press, 1989.59. Pless B, Towner E, eds. Acti<strong>on</strong> <strong>on</strong> <strong>injury</strong>. Setting theagenda for <strong>child</strong>ren and young people in the UK. InjuryPreventi<strong>on</strong>, 1998, 4:S1–S46.60. Gallagher SS et al. The incidence of injuries in 87,000Massachusetts <strong>child</strong>ren and adolescents. AmericanJournal of Public Health, 1984, 74:1340–1347.61. Rahman A et al. Bangladesh health and <strong>injury</strong> survey:<str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> <strong>child</strong>ren. Dhaka, Ministry of Health and FamilyWelfare, 2005.62. Grossman DC. The history of <strong>injury</strong> c<strong>on</strong>trol and theepidemiology of <strong>child</strong> and adolescent injuries. The Futureof Children, 2000, 10:23–52.63. Linnan M et al. Child mortality and <strong>injury</strong> in Asia: an overview.Florence, UNICEF Innocenti Research Centre, 2007 (http://www.unicef-irc.org/publicati<strong>on</strong>s/pdf/iwp_2007_04.pdf,accessed 21 January 2008). (Innocenti Working Paper 2007-04, Special series <strong>on</strong> <strong>child</strong> <strong>injury</strong> No. 1).64. Banco de dados do Sistema Único de Saúde (DATASUS) [inPortuguese]. Brazilia, Ministério da Saúde, Departamentode Informática do SUS (http://w3.datasus.gov.br/datasus/datasus.php, accessed 7 March 2008).65. Beattie RF et al. Measures of <strong>injury</strong> severity in <strong>child</strong>hood:a critical overview. Injury Preventi<strong>on</strong>, 1998, 4:228–231.66. Evans SA et al. Disability in young adults following majortrauma: 5 year follow up of survivors. BMC Public Health,2003, 3(8) (http://www.biomedcentral.com/1471-2458/3/8,accessed 14 February 2008).67. Lloyd CB. Growing up global: the changing transiti<strong>on</strong>sto adulthood in developing countries. Washingt<strong>on</strong>, DC,Nati<strong>on</strong>al Academies Press, 2005.68. Bourdill<strong>on</strong> M. Children in development. Progress inDevelopment Studies, 2004, 4:99–113.69. Hope K. Child survival, poverty and labor in Africa.Journal of Children and Poverty, 2005, 11:19–42.70. On DWI laws in other countries. Washingt<strong>on</strong>, DC,Nati<strong>on</strong>al Highway Traffic Safety Administrati<strong>on</strong>, 2000(http://www.nhtsa.dot.gov/people/<strong>injury</strong>/research/pub/DWIothercountries/dwiothercountries.html, accessed 21January 2008) (DOT HS 809 037).71. Rivara FP. Developmental and behavioural issues in<strong>child</strong>hood <strong>injury</strong> preventi<strong>on</strong>. Journal of DevelopmentalBehaviour Pediatrics, 1995, 16:362–370.72. Agran PF et al. Rates of pediatric and adolescent injuriesby year of age. Pediatrics, 2001, 108:45–56.24 WORLD REPORT ON CHILD INJURY PREVENTION
73. Agran PF et al. Rates of pediatric injuries by 3-m<strong>on</strong>thintervals for <strong>child</strong>ren 0 to 3 years of age. Pediatrics, 2003,111:683–692.74. Towner E et al. Injuries in <strong>child</strong>ren aged 0–14 years andinequalities. L<strong>on</strong>d<strong>on</strong>, Health Development Agency, 2005(http://www.nice.org.uk/niceMedia/pdf/injuries_in_<strong>child</strong>ren_inequalities.pdf, accessed 22 January 2008).75. Flavin MP et al. Stages of development and <strong>injury</strong> patternsin the early years: a populati<strong>on</strong>-based analysis. BMCPublic Health, 2006, 6(187) (http://www.biomedcentral.com/1471-2458/6/187, accessed 21 January 2008).76. Bartlett S. The problem of <strong>child</strong>ren’s injuries in lowincomecountries: a review. Health Policy and Planning,2002, 17:1–13.77. Wils<strong>on</strong> M et al. Saving <strong>child</strong>ren: a guide to <strong>injury</strong> preventi<strong>on</strong>.New York, NY, Oxford University Press, 1991.78. Toroyan T, Peden M, eds. Youth and road safety. Geneva,Switzerland, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2007 (http://whqlibdoc.who.int/publicati<strong>on</strong>s/2007/9241595116_eng.pdf, accessed 18 February 2008).79. Kalayi G, Muhammed I. Burns in <strong>child</strong>ren under 3 years ofage: the Zaria experience. Annals of Tropical Paediatrics,1996, 16:243–248.80. Thoms<strong>on</strong> J et al. Child development and the aims of roadsafety educati<strong>on</strong>: a review and analysis. Norwich, TheStati<strong>on</strong>ery Office, 1996 (Department of Transport RoadSafety Research No. 1).81. Sinnott W. Safety aspects of domestic architecture. In:Jacks<strong>on</strong> RH, ed. Children, the envir<strong>on</strong>ment and accidents.L<strong>on</strong>d<strong>on</strong>, Pittman Medical, 1977:76–90.82. Ward C. The <strong>child</strong> in the city. L<strong>on</strong>d<strong>on</strong>, Bedford SquarePress, 1990.83. Towner E, Towner J. The preventi<strong>on</strong> of <strong>child</strong>hoodunintenti<strong>on</strong>al <strong>injury</strong>. Current Paediatrics, 2001, 11:403–408.84. Bartlett S. Children’s experience of the physicalenvir<strong>on</strong>ment in poor urban settlements and the implicati<strong>on</strong>sfor policy, planning and practice. Envir<strong>on</strong>mentand Urbanizati<strong>on</strong>, 1999, 11:63–73.85. Nicol A. Carrying the can: <strong>child</strong>ren and their waterenvir<strong>on</strong>ments. L<strong>on</strong>d<strong>on</strong>, Save the Children, 1998.86. Rivara FP et al. Epidemiology of <strong>child</strong>hood injuries. II. Sexdifferences in <strong>injury</strong> rates. American Journal of Diseasesof Children, 1982, 13:502–506.87. Spady DW et al. Patterns of <strong>injury</strong> in <strong>child</strong>ren: a populati<strong>on</strong>-basedapproach. Pediatrics, 2004, 113:522–529.88. Morr<strong>on</strong>giello BA, Rennie H. Why do boys engage in morerisk taking than girls? Journal of Pediatric Psychology,1998, 23:33–43.89. Rosen BN, Peters<strong>on</strong> L. Gender differences in <strong>child</strong>ren’soutdoor play injuries: a review and integrati<strong>on</strong>. ClinicalPsychology Review, 1990, 10:187–205.90. Eat<strong>on</strong> W. Are sex differences in <strong>child</strong> motor activity levela functi<strong>on</strong> of sex differences in maturati<strong>on</strong>al status? ChildDevelopment, 1989, 60:1005–1011.91. Block J. Differential premises arising from differentialsocializati<strong>on</strong> of the sexes: some c<strong>on</strong>jectures. ChildDevelopment, 1983, 54:1335–1354.92. Saegert S, Hart R. The development of sex differences inthe envir<strong>on</strong>mental c<strong>on</strong>fidence of <strong>child</strong>ren. In: Burnett P,ed. Women in society. Chicago, Maaroufa Press, 1990:157–175.93. Fagot B. The influence of sex of <strong>child</strong> <strong>on</strong> parental reacti<strong>on</strong>sto toddler <strong>child</strong>ren. Child Development, 1978, 49:459–465.94. Hyder A, Peden M. Inequality and road traffic injuries:call for acti<strong>on</strong>. The Lancet, 2002, 362:2034–2035.95. Hulme D. Chr<strong>on</strong>ic poverty and development policy: anintroducti<strong>on</strong>. <str<strong>on</strong>g>World</str<strong>on</strong>g> Development, 2003, 31:399–402.96. Soori H, Naghavi M. Childhood deaths from unintenti<strong>on</strong>alinjuries in rural areas of Iran. Injury Preventi<strong>on</strong>, 1998,4:222–224.97. Hulme D, Shepherd A. C<strong>on</strong>ceptualizing chr<strong>on</strong>ic poverty.<str<strong>on</strong>g>World</str<strong>on</strong>g> Development, 2003, 31:403–423.98. Sen AK. Poor, relatively speaking. Oxford Ec<strong>on</strong>omicPapers, 1983, 35:153–169.99. Bang RL et al. Scalds am<strong>on</strong>g <strong>child</strong>ren in Kuwait. EuropeanJournal of Epidemiology, 1997, 13:33–39.100. Roberts I, Power C. Does the decline in <strong>child</strong> <strong>injury</strong>mortality vary by social class? A comparis<strong>on</strong> of classspecific mortality in 1981 and 1991. British MedicalJournal, 1996, 313:784–786.101. Reading R. Area socioec<strong>on</strong>omic status and <strong>child</strong>hood<strong>injury</strong> morbidity in New South Wales, Australia. Child CareHealth and Development, 2008, 34:136–137.102. Butchart A et al. Percepti<strong>on</strong>s of <strong>injury</strong> causes and soluti<strong>on</strong>sin a Johannesburg township: implicati<strong>on</strong>s for preventi<strong>on</strong>.Social Science and Medicine, 2000, 50:331–344.103. Thanh NX. The <strong>injury</strong> poverty trap in rural Vietnam:causes, c<strong>on</strong>sequences and possible soluti<strong>on</strong>s [unpublisheddoctoral thesis]. Sweden, Umeå University, 2005 (http://www.diva-portal.org/diva/getDocument? urn_nbn_se_umu_diva-627-2__fulltext. pdf, accessed 22 January2008).104. Sen B. Drivers of escape and descent: changing householdfortunes in rural Bangladesh. <str<strong>on</strong>g>World</str<strong>on</strong>g> Development, 2003,31:513–534.105. Aer<strong>on</strong>-Thomas A et al. The involvement and impact of roadcrashes <strong>on</strong> the poor: Bangladesh and Indian case studies.Crowthorne, Transport Research Laboratory, 2004 (TRLProject Report 010).106. Thanh NX et al. Does the <strong>injury</strong> poverty trap exist? Al<strong>on</strong>gitudinal study in Bavi, Vietnam. Health Policy, 2006,78:249–257.WORLD REPORT ON CHILD INJURY PREVENTION 25
107. Pryer J. When breadwinners fall ill: preliminary findingsfrom a case study in Bangladesh. Institute of DevelopmentStudies Bulletin, 1989, 20:49–57.108. Mock C et al. Ec<strong>on</strong>omic c<strong>on</strong>sequences of injuries andresulting family coping strategies in Ghana. AccidentAnalysis and Preventi<strong>on</strong>, 2003, 35:81–90.109. Pressley JC et al. Twenty-year trends in fatal injuries tovery young <strong>child</strong>ren: the persistence of racial disparities.Pediatrics, 2007, 119:e875–e884 (http://pediatrics.aappublicati<strong>on</strong>s.org/cgi/reprint/119/4/e875, accessed 21January 2008).110. Langley J, Brought<strong>on</strong> J. Injury to Maori I: fatalities. NewZealand Medical Journal, 2000, 113:508–510.111. Stevens<strong>on</strong> M et al. At risk in two worlds: <strong>injury</strong> mortalityam<strong>on</strong>g indigenous people in the US and Australia, 1990–92. Australian and New Zealand Journal of Public Health,1998, 22:641–644.112. Clapham KF, Stevens<strong>on</strong> MR, Lo SK. Injury profiles ofindigenous and n<strong>on</strong>-indigenous people in New SouthWales. Medical Journal of Australia, 2006, 184:212–220.113. Husum H et al. Rural prehospital trauma systems improvetrauma outcome in low-income countries: a prospectivestudy from North Iraq and Cambodia. Journal of Trauma,2003, 54:1188–1196.114. Sasser S et al. Prehospital trauma care systems. Geneva,<str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2005 (http://www.who.int/entity/violence_<strong>injury</strong>_preventi<strong>on</strong>/publicati<strong>on</strong>s/services/39162_oms_new.pdf, accessed 16 May 2008).115. Mock C et al. Guidelines for essential trauma care. Geneva,<str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2004 (http://whqlibdoc.who.int/publicati<strong>on</strong>s/2004/9241546409.pdf, accessed 16 May2008).116. Salter E, Stallard P. Young people’s experience of emergencymedical services as road traffic accident victims: apilot qualitative study. Journal of Child Health Care, 2004,8:301–311.117. Hadd<strong>on</strong> W. On the escape of tigers: an ecologic note.American Journal of Public Health, 1970, 60:2229–2234.118. Runyan CW. Using the Hadd<strong>on</strong> matrix: introducing thethird dimensi<strong>on</strong>. Injury Preventi<strong>on</strong>, 1998, 4:302–307.119. Hadd<strong>on</strong> W. Energy damage and the ten countermeasurestrategies. Journal of Trauma, 1973, 13:321–331.120. Christoffel T, Gallagher SS. Injury preventi<strong>on</strong> andpublic health: practical knowledge, skills, and strategies.Gaithersburg, MD, Aspen Publishers, 1999.121. Gilchrist J, Gotsch K, Ryan G. N<strong>on</strong>-fatal dog bite-relatedinjuries treated in hospital emergency departments –United States, 2001. Morbidity and Mortality WeeklyReport, 4 July 2003, 52:605–610.122. Schalam<strong>on</strong> J et al. Analysis of dog bites in <strong>child</strong>ren whoare younger than 17 years. Pediatrics, 2006, 117:e374–e379(http://pediatrics.aappublicati<strong>on</strong>s.org/cgi/c<strong>on</strong>tent/full/117/3/e374, accessed 9 April 2008).123. Ozanne-Smith J, Ashby K, Stathakis V. Dog bite and <strong>injury</strong>preventi<strong>on</strong>: analysis, critical review and research agenda.Injury Preventi<strong>on</strong>, 2001, 7:321–326.124. Kreisfeld R, Harris<strong>on</strong> J. Dog related injuries. Adelaide,Research Centre for Injury Studies, Flinders University,2005 (NISU Briefing).125. Human and animal rabies. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> HealthOrganizati<strong>on</strong> (http://www.who.int/rabies/, accessed 9April 2008).126. Rabies. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2006(Fact sheet No. 99) (http://www.who.int/mediacentre/factsheets/fs099/en/index.html, accessed 9 April 2008).127. Singh J et al. Epidemiological characteristics of rabies inDelhi and surrounding areas, 1998. Indian Pediatrics,2001, 38:1354–1360.128. Pancharoen C et al. Rabies exposure in Thai <strong>child</strong>ren.Wilderness and Envir<strong>on</strong>mental Medicine, 2001, 12:239–243.129. Fèvre EM et al. The epidemiology of animal bite injuries inUganda and projecti<strong>on</strong>s of the burden of rabies. TropicalMedicine and Internati<strong>on</strong>al Health, 2005, 10:790–798.130. Cleaveland S et al. Estimating human rabies mortality inthe United Republic of Tanzania from dog bite injuries.Bulletin of the <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2002, 80:304–310.131. Sethi D et al. Injuries and violence in Europe: why theymatter and what can be d<strong>on</strong>e. Copenhagen, WHORegi<strong>on</strong>al Office for Europe, 2006 (http://www.euro.who.int/document/E88037.pdf, accessed 22 January 2008).132. MacKay M, Vincenten J. Acti<strong>on</strong> planning for <strong>child</strong> safety: astrategic and coordinated approach to reducing the number<strong>on</strong>e cause of death for <strong>child</strong>ren in Europe. Amsterdam,European Child Safety Alliance, Eurosafe, 2007.133. Pless I, Towner E. Practiti<strong>on</strong>ers and policy makers.In: Aynsley-Green A et al., eds. Unintenti<strong>on</strong>al <strong>injury</strong> in<strong>child</strong>hood and adolescence. L<strong>on</strong>d<strong>on</strong>, Bailliere Tindall,1997:393–409.134. Bergman AB, Rivara FP. Sweden’s experience in reducing<strong>child</strong>hood injuries. Pediatrics, 1991, 88:69–74.135. Ramsay S. Child-<strong>injury</strong> death rates: do internati<strong>on</strong>alcomparis<strong>on</strong>s help? The Lancet, 2001, 357:454.136. Christie N et al. Children’s road traffic safety: aninternati<strong>on</strong>al survey of policy and practice. L<strong>on</strong>d<strong>on</strong>,Department for Transport, 2004.137. Whitehead M. Diffusi<strong>on</strong> of ideas <strong>on</strong> social inequalities inhealth: a European perspective. The Millbank Quarterly,1998, 76:469–492.138. Nort<strong>on</strong> R et al. Unintenti<strong>on</strong>al injuries. In: Jamis<strong>on</strong> DT etal., eds. Disease c<strong>on</strong>trol priorities in developing countries,2nd ed. New York, Oxford University Press and the <str<strong>on</strong>g>World</str<strong>on</strong>g>Bank, 2006:737–753 (http://www.dcp2.org/pubs/DCP/39/,accessed 14 February 2008).26 WORLD REPORT ON CHILD INJURY PREVENTION
139. Zaza S et al. Reviews of evidence regarding interventi<strong>on</strong>sto increase use of <strong>child</strong> safety seats. American Journal ofPreventive Medicine, 2001, 21(4S):31–34.140. Dinh-Zarr T et al. Reviews of evidence regardinginterventi<strong>on</strong>s to increase the use of safety belts. AmericanJournal of Preventive Medicine, 2001, 21(4S):48–65.141. Macphers<strong>on</strong> A, Spinks A. Bicycle helmet legislati<strong>on</strong>for the uptake of helmet use and preventi<strong>on</strong> of headinjuries. Cochrane Database of Systematic Reviews. 2007,(2):CD005401.142. DiGuiseppi C, Goss C, Higgins JPT. Interventi<strong>on</strong>s forpromoting smoke alarm ownership and functi<strong>on</strong>. CochraneDatabase of Systematic Reviews, 2001, (2):CD002246.143. MacArthur C. Evaluati<strong>on</strong> of Safe Kids Week 2001:Preventi<strong>on</strong> of Scald and Burn Injuries in Young Children.Injury Preventi<strong>on</strong>, 2003, 9:112–116.144. Best practices: Pois<strong>on</strong>ing interventi<strong>on</strong>s. Harborview InjuryPreventi<strong>on</strong> Research Centre (http://depts.washingt<strong>on</strong>.edu/hiprc/practices/topic/pois<strong>on</strong>ing/packaging.html,accessed 6 April 2008).145. Thomps<strong>on</strong> DC, Rivara FP. Pool fencing for preventingdrowning in <strong>child</strong>ren. Cochrane Database of SystematicReviews, 2000, (2):CD001047.146. Ehiri JE et al. Interventi<strong>on</strong>s for promoting boosterseat use in four to eight year olds traveling in motorvehicles. Cochrane Database of Systematic Reviews, 2006,(1):CD004334.147. Karkhaneh M et al. Effectiveness of bicycle helmetlegislati<strong>on</strong> to increase helmet use: a systematic review.Injury Preventi<strong>on</strong>, 2006, 12:76–82.148. Thomps<strong>on</strong> DC, Rivara FP, Thomps<strong>on</strong> R. Helmets forpreventing head and facial injuries in bicyclists. CochraneDatabase of Systematic Reviews. 1999, (4):CD001855.149. ISO/IEC Guide 50:2002. Safety aspects: guidelines for <strong>child</strong>safety, 2nd ed. Geneva, Internati<strong>on</strong>al Organizati<strong>on</strong> forStandardizati<strong>on</strong>, 2002.150. Razzak J et al. Injuries am<strong>on</strong>g <strong>child</strong>ren in Karachi,Pakistan: what, where and how. Public Health, 2004,118:114–120.151. Child <strong>injury</strong> preventi<strong>on</strong> [Evidence-Based HealthPromoti<strong>on</strong> No. 4]. Melbourne, Victorian GovernmentDepartment of Human Services, 2001 (http://health.vic.gov.au/healthpromoti<strong>on</strong>/quality/<strong>child</strong>_<strong>injury</strong>.htm,accessed 22 January 2008).152. Krug A et al. The impact of <strong>child</strong> resistant c<strong>on</strong>tainers inthe incidence of paraffin (kerosene) ingesti<strong>on</strong> in <strong>child</strong>ren.South African Medical Journal, 1994, 84:730–734.153. Bruce N et al. Preventi<strong>on</strong> of burns am<strong>on</strong>g <strong>child</strong>ren in woodfuel using homes in rural Guatemala. Poster presentati<strong>on</strong>at the 16th Annual C<strong>on</strong>ference of the Internati<strong>on</strong>alSociety for Envir<strong>on</strong>mental Epidemiology, New York, NY,1–4 August 2004.154. Bunn F et al. Traffic calming for the preventi<strong>on</strong> of roadtraffic injuries: systematic review and meta-analysis.Injury Preventi<strong>on</strong>, 2003, 9:200–204.155. Ly<strong>on</strong>s RA et al. Modificati<strong>on</strong> of the home envir<strong>on</strong>ment forthe reducti<strong>on</strong> of injuries. Cochrane Database of SystematicReviews, 2003, (4):CD003600.156. Tiwari G. Traffic flow and safety: need for new models forheterogeneous traffic. In: Mohan D, Tiwari G, eds. InjuryPreventi<strong>on</strong> and C<strong>on</strong>trol. L<strong>on</strong>d<strong>on</strong>, Taylor and Francis,2000:71–78.157. Bilukha O, et al. The effectiveness of early <strong>child</strong>hood homevisitati<strong>on</strong> in preventing violence: a systematic review.American Journal of Preventive Medicine, 2005, 28(Suppl.2)1:11–39.158. Kendrick D et al. Does home visiting improve parentingand the quality of the home envir<strong>on</strong>ment? A systematicreview and meta analysis. Archives of Diseases in Children,2000, 82:443–451.159. Grossman D, Garcia C. Effectiveness of health promoti<strong>on</strong>programs to increase motor vehicle occupant restraint useam<strong>on</strong>g young <strong>child</strong>ren. American Journal of PreventiveMedicine, 1999, 16:12–22.160. Royal ST, Kendrick D, Coleman T. N<strong>on</strong>-legislativeinterventi<strong>on</strong>s for the promoti<strong>on</strong> of cycle helmet wearingby <strong>child</strong>ren. Cochrane Database of Systematic Reviews,2005, (2):CD003985.161. Farley C, Laflamme L, Vaez M. Bicycle helmet campaignsand head injuries am<strong>on</strong>g <strong>child</strong>ren. Does poverty matter?Journal of Epidemiology and Community Health, 2003,57:668–672.162. Helmets: a road safety manual for decisi<strong>on</strong>-makers andpractiti<strong>on</strong>ers. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>,2006 (http://www.who.int/violence_<strong>injury</strong>_preventi<strong>on</strong>/publicati<strong>on</strong>s/road_traffic/helmet_manual.pdf, accessed22 January 2008).163. Liu BC et al. Helmets for preventing <strong>injury</strong> in motorcycleriders. Cochrane Database of Systematic Reviews, 2004,(2):CD004333.164. Duperrex O, Roberts I, Bunn F. Safety educati<strong>on</strong> ofpedestrians for <strong>injury</strong> preventi<strong>on</strong>. Cochrane Database ofSystematic Reviews, 2002, (2):CD001531.165. Towner EML. The role of health educati<strong>on</strong> in <strong>child</strong>hood<strong>injury</strong> preventi<strong>on</strong>. Injury Preventi<strong>on</strong>, 1995, 1:53–58.166. Manganello JA, McKenzie LB. Home and <strong>child</strong> safety <strong>on</strong>reality televisi<strong>on</strong>. Health Educati<strong>on</strong> Research, 2008 [Epubahead of print] (http://her.oxfordjournals.org/cgi/reprint/cym088v1, accessed 18 July 2008).167. Green LW, Kreuter M. Health promoti<strong>on</strong> planning:an educati<strong>on</strong>al and envir<strong>on</strong>mental approach, 2nd ed.Mountain View, CA, Mayfield Publishing Co., 1991.168. Behaviour change at populati<strong>on</strong>, community and individuallevels. L<strong>on</strong>d<strong>on</strong>, Nati<strong>on</strong>al Institute for Health and ClinicalExcellence (NICE), 2007 (NICE public health guidance 6).WORLD REPORT ON CHILD INJURY PREVENTION 27
169. Towner E, Dowswell T. Community-based <strong>child</strong>hood<strong>injury</strong> preventi<strong>on</strong>: what works? Health Promoti<strong>on</strong>Internati<strong>on</strong>al, 2002, 17:273–284.170. Spinks A et al. The ‘WHO Safe Communities’ model forthe preventi<strong>on</strong> of <strong>injury</strong> in whole populati<strong>on</strong>s. CochraneDatabase of Systematic Reviews, 2005, (2):CD004445.171. Kelly M, Speller V, Meyrick J. Getting evidence into practicein public health. L<strong>on</strong>d<strong>on</strong>, Health Educati<strong>on</strong> Authority,2004.172. Bruss<strong>on</strong>i M, Towner E, Hayes M. Evidence into practice:combining the art and science of <strong>injury</strong> preventi<strong>on</strong>. InjuryPreventi<strong>on</strong>, 2006, 12:373–377.173. Mock C et al. Strengthening the preventi<strong>on</strong> and care ofinjuries worldwide. The Lancet, 2004, 363:2172–2179.174. Whitehead M. Tackling inequalities: a review of policyinitiatives. In: Benzeval M, Judge K, Whitehead M, eds.Tackling inequalities in health: an agenda for acti<strong>on</strong>.L<strong>on</strong>d<strong>on</strong>, King’s Fund, 1995.175. Thoms<strong>on</strong> J, Whelan K. Community approach to roadsafety educati<strong>on</strong>. L<strong>on</strong>d<strong>on</strong>, Department of Transport, 1997(http://www.dft.gov.uk/pdf/pgr/roadsafety/research/rsrr/theme1/communityapproachtoroadsafet4735, accessed22 January 2008). (Road Safety Research Report No. 3).176. Coggan C et al. Evaluati<strong>on</strong> of the Waitakere community<strong>injury</strong> preventi<strong>on</strong> project. Injury Preventi<strong>on</strong>, 2000, 6:130–134.177. Schwartz D et al. An <strong>injury</strong> preventi<strong>on</strong> program in anurban African-American community. American Journalof Public Health, 1993, 83:675–680.178. MacKay M et al. Child safety good practice guide: goodinvestments in unintenti<strong>on</strong>al <strong>injury</strong> preventi<strong>on</strong> and safetypromoti<strong>on</strong>. Amsterdam, European Child Safety Alliance,2006.179. Schopper D, Lormand JD, Waxweiler R, eds. Developingnati<strong>on</strong>al policies to prevent violence and injuries: a guidelinefor policy-makers and planners. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> HealthOrganizati<strong>on</strong>, 2006 (http://www.who.int/violence_<strong>injury</strong>_preventi<strong>on</strong>/publicati<strong>on</strong>s/39919_oms_br_2.pdf, accessed22 January 2008).180. Peden M, Hyder AA. Road traffic injuries are a globalpublic health problem. British Medical Journal, 2002,324:1153.181. Doll LS et al., eds. Handbook of <strong>injury</strong> and violencepreventi<strong>on</strong>. Atlanta, GA, Springer, 2007.182. Hendrie D et al. Child and family device availability bycountry income level: an 18 country comparis<strong>on</strong>. InjuryPreventi<strong>on</strong>, 2004, 10:338–343.183. Waters H, Hyder AA, Phillips TL. Ec<strong>on</strong>omic evaluati<strong>on</strong>of interventi<strong>on</strong>s to reduce road traffic injuries: a reviewof literature with applicati<strong>on</strong>s to low and middle incomecountries. Asia Pacific Journal of Public Health, 2004,16:23–31.184. Bishai DM, Hyder AA. Modeling the cost effectivenessof <strong>injury</strong> interventi<strong>on</strong>s in lower and middle incomecountries: opportunities and challenges. Cost Effectivenessand Resource Allocati<strong>on</strong>, 2006, 4:2.185. Miller TR, Romano EO, Spicer RS. The cost of <strong>child</strong>hoodunintenti<strong>on</strong>al injuries and the value of preventi<strong>on</strong>.The Future of Children [issue <strong>on</strong> “Unintenti<strong>on</strong>alinjuries in <strong>child</strong>hood”], 2000, 10:137–163 (http://www.futureof<strong>child</strong>ren.org/usr_doc/vol10no1Art6.pdf, accessed7 March 2008).186. Miller TR, Levy DT. Cost outcome analysis in <strong>injury</strong>preventi<strong>on</strong> and c<strong>on</strong>trol: eighty-four recent estimates forthe United States. Medical Care. 2000, 38:570–573.187. France: recent developments in road safety. Paris, FrenchNati<strong>on</strong>al Observatory for Road Safety, 2005 (http://securiteroutiere.gouv.fr/IMG/pdf/FRDI.pdf, accessed 22January 2008).188. Rivara FP. Preventi<strong>on</strong> of injuries to <strong>child</strong>ren andadolescents. Injury Preventi<strong>on</strong>, 2002, 8(Suppl. 4):iv5–iv8.189. Philippakis A et al. A quantificati<strong>on</strong> of preventableunintenti<strong>on</strong>al <strong>child</strong>hood <strong>injury</strong> mortality in the UnitedStates. Injury Preventi<strong>on</strong>, 2004, 10:79–82.190. Pless B. Acti<strong>on</strong> <strong>on</strong> <strong>injury</strong>: setting the agenda for <strong>child</strong>renand young people in the UK [Preface]. Injury Preventi<strong>on</strong>,1998, 4:S1–S3.28 WORLD REPORT ON CHILD INJURY PREVENTION
WORLD REPORT ON CHILD INJURY PREVENTION 29
TRAFFIC INJURIESDEANA’S STORY© D. BlanchardDeana is my daughter. She was 17 years old when her life wascut short. Deana was with four friends going to a birthday party.They had just got out of a taxi and were trying to cross the NileCorniche in Maadi. The traffic is heavy, chaotic. There are notraffic lights, no crosswalks, just a c<strong>on</strong>stant stream of speeding,weaving cars, trucks and buses. You have to dart across severallanes of traffic to get to the other side. Deana was hit and killedby a speeding bus as she tried to cross the road. The bus driverdidn’t even slow down.I was in Damascus at the time, travelling for my work. My brother-in-law called meto tell me the terrible news that my baby girl had been hit. You can imagine myguilt. I should have been in Cairo. I could have driven her to the party.Deana loved so many things, she loved life. She had an infectious smile. Shealways had time for other people more than for herself. She wanted to be apaediatric dentist – she loved kids. She had a special love of angels. She alwayshad pictures or figurines of angels in her room. For us, she has become the “Angelof the Nile”.Every<strong>on</strong>e was deeply affected by Deana’s death, her family her friends, the entirecommunity. I think of ripples of pain, an ever-widening circle of those who wereaffected. My wife, s<strong>on</strong> and I had to leave Cairo after Deana’s death. It was toopainful, too many memories. We came back to Cairo just a few m<strong>on</strong>ths ago.I guess that early <strong>on</strong> I made a decisi<strong>on</strong>. I could roll up into a ball in a foetalpositi<strong>on</strong> and never wake up. It would be very easy to do this and give up. But I feltthat I had tried to make sense out of the senseless, the unbelievable. I decided todo something tangible, something that would save other people’s lives.An NGO, the Safe Road Society, started because our daughter lost her life. It isdedicated to making the roads in Egypt safer for its citizens. Our first project is thebuilding of a pedestrian tunnel under the Maadi Corniche El Nile. Governmentalpermits have been obtained and request for c<strong>on</strong>structi<strong>on</strong> bids sent. Our next stepis to ensure sufficient funds are raisedthrough voluntary d<strong>on</strong>ati<strong>on</strong>s to completethis life saving project. This busy roadof death runs al<strong>on</strong>gside the serenity ofthe Nile River. Many c<strong>on</strong>cerned anddedicated Egyptians and foreignershave joined together with the goalto make the tunnel a reality. Also, ascholarship was started in Deana’sname at her school and every yeara graduating senior who smiles andbrings light to another student’s dayis awarded a helping hand.By building a pedestrian tunnelwe hope to save lives and, in mydreams, to see my Deana, myAngel of the Nile, looking downup<strong>on</strong> us and smiling in approval.
CHAPTER 2 – ROAD TRAFFIC INJURIESChapter 2Road traffic injuriesIntroducti<strong>on</strong>In many places the road network is c<strong>on</strong>structed withoutc<strong>on</strong>sidering <strong>child</strong>ren. Children, though, use the roads aspedestrians, bicyclists, motorcyclists and occupants ofvehicles. They may live close to a road, play <strong>on</strong> a road, oreven work <strong>on</strong> the roads. All these interacti<strong>on</strong>s with roads,together with a range of other risk factors associated with<strong>child</strong>hood, increase the susceptibility of <strong>child</strong>ren to roadtraffic <strong>injury</strong>.This chapter examines the extent and characteristics ofroad traffic injuries for different types of road users am<strong>on</strong>g<strong>child</strong>ren aged 0–17 years, as well as their risk factors.Proven and promising interventi<strong>on</strong>s, for the different typesof road user, are discussed, al<strong>on</strong>g with their effectivenessand cost-effectiveness. The chapter c<strong>on</strong>cludes with somerecommendati<strong>on</strong>s for preventing the growing toll of roadtraffic <strong>injury</strong>.For the purpose of this <str<strong>on</strong>g>report</str<strong>on</strong>g>, a road traffic crash isdefined as “a collisi<strong>on</strong> or incident that may or may not leadto <strong>injury</strong>, occurring <strong>on</strong> a public road and involving at least<strong>on</strong>e moving vehicle”. Road traffic injuries are defined as“fatal or n<strong>on</strong>-fatal injuries incurred as a result of a roadtraffic crash” (1). Although other definiti<strong>on</strong>s exist, a roadtraffic fatality is c<strong>on</strong>sidered to be a death occurring within30 days of a road traffic crash (2).This chapter focuses <strong>on</strong> <strong>child</strong>ren aged 0–17 years.Comprehensive data, however, are not always availableacross the whole age range. In particular, informati<strong>on</strong> isoften limited for <strong>child</strong>ren aged between 15 and 17 years.There are also problems of under-<str<strong>on</strong>g>report</str<strong>on</strong>g>ing of road trafficdeaths and injuries, particularly in low-income andmiddle-income countries, limitati<strong>on</strong>s that need to betaken into account when interpreting the data.The road is a dangerous place for <strong>child</strong>ren and youngpeople. However, road traffic injuries do not have to bethe price <strong>child</strong>ren and their families pay for the increasingmobility and independence of <strong>child</strong>ren as they grow up.There are proven and effective measures that can be putinto place to reduce their risks to a minimum.Epidemiology of road traffic injuriesAccording to the WHO Global Burden of Disease project,in 2004 nearly 1.3 milli<strong>on</strong> people of all ages were killed inroad traffic crashes around the world and up to 50 milli<strong>on</strong>more were injured or disabled. The South-East Asia andthe Western Pacific Regi<strong>on</strong>s of WHO together accountedfor two thirds of all road traffic deaths. However, thehighest rates of road traffic death were in the African andEastern Mediterranean Regi<strong>on</strong>s. Globally, 21% of roadtraffic deaths were am<strong>on</strong>g <strong>child</strong>ren.There have been downward trends in the numbers ofroad traffic deaths and injuries over the last couple ofdecades in several developed countries. Globally, though,the outlook is disturbing. By the year 2030, road trafficinjuries are predicted to be the fifth leading cause of deathworldwide (3) and the seventh leading cause of disabilityadjustedlife years lost (4). The South-East Asia, Africanand Western Pacific regi<strong>on</strong>s are expected to see the mostsignificant increases in road traffic injuries. Of particularc<strong>on</strong>cern is the fact that in India and China – each withmore than a sixth of the world’s populati<strong>on</strong> – the numberof road traffic deaths is predicted to increase, by 2020, byapproximately 147% and 97%, respectively (5).MortalityIn 2004, road traffic injuries accounted for approximately262 000 <strong>child</strong> deaths am<strong>on</strong>g <strong>child</strong>ren and youth aged0–19 years – almost 30% of all <strong>injury</strong> deaths am<strong>on</strong>g<strong>child</strong>ren (see Statistical Annex, Table A.1). Road trafficinjuries are the leading cause of death am<strong>on</strong>g young peopleaged 15 to 19 years (see Table 1.1). Globally, these deaths<strong>on</strong> the roads account for nearly 2% of all deaths am<strong>on</strong>g<strong>child</strong>ren. There are significant geographic variati<strong>on</strong>s,however. In the South-East Asia Regi<strong>on</strong>, the proporti<strong>on</strong>of <strong>child</strong>hood deaths due to road traffic injuries is 1.3%,while in the Americas it is as high as 4.7%. Some 93%of <strong>child</strong> road deaths occur in low-income and middleincomecountries (see Statistical Annex, Table A.1). In2004, the South-East Asia and African Regi<strong>on</strong>s and thelow-income and middle-income countries of the WesternPacific Regi<strong>on</strong> accounted for two thirds of all road trafficdeaths am<strong>on</strong>g <strong>child</strong>ren.Data shows that globally, the road traffic death rateam<strong>on</strong>g <strong>child</strong>ren is 10.7 per 100 000 populati<strong>on</strong> (seeFigure 2.1). In South-East Asia, however, the rate is 7.4per 100 000 populati<strong>on</strong>, while in the African Regi<strong>on</strong> it is19.9 per 100 000 populati<strong>on</strong>. Although the mortality rateis not as high in Europe, road traffic injuries still accountfor around a fifth of all <strong>child</strong>hood <strong>injury</strong> deaths across theEuropean Uni<strong>on</strong> (6).In additi<strong>on</strong> to regi<strong>on</strong>al differences, there are alsovariati<strong>on</strong>s according to the type of road user. In 70countries – mainly middle-income and high-incomecountries – that provide sufficiently detailed mortalitydata to WHO, about 33% of all <strong>child</strong> deaths around theworld are pedestrians, while 65% are car occupants orbicycle or motorcycle riders (7).WORLD REPORT ON CHILD INJURY PREVENTION 31
FIGURE 2.1Road-traffic <strong>injury</strong> mortality rates per 100 000 <strong>child</strong>ren a by WHO regi<strong>on</strong> and country income level, 200415+8.0–14.9
is similar to that seen in adulthood (see Table 2.1). Overall,the death rate for boys is 13.8 per 100 000 populati<strong>on</strong>,compared to a rate for girls of 7.5 per 100 000 populati<strong>on</strong>. Inthe high-income countries of the Eastern MediterraneanRegi<strong>on</strong> the gender gap is greatest am<strong>on</strong>g young <strong>child</strong>renwhile in the regi<strong>on</strong>s of Europe, the Western Pacific andthe Americas the gap is more pr<strong>on</strong>ounced am<strong>on</strong>g older<strong>child</strong>ren (see Statistical Annex, Table A.1).TABLE 2.1Fatal road-traffic <strong>injury</strong> rates per 100 000 <strong>child</strong>ren by age andsex, <str<strong>on</strong>g>World</str<strong>on</strong>g>, 2004Age ranges (in years)Under 1 1–4 5–9 10–14 15–19 Under 20These survey results are supported by a hospitalbasedstudy of injured <strong>child</strong>ren under the age of 12 years,c<strong>on</strong>ducted in four low-income countries. The study foundthat, am<strong>on</strong>g those suffering road traffic injuries, morethan a quarter had incurred a c<strong>on</strong>cussi<strong>on</strong> or other head<strong>injury</strong>, followed by various cuts, bruises, open wounds,fractures and sprains (see Statistical Annex, Table C.1 andFigure 2.3).FIGURE 2.3Injuries sustained by <strong>child</strong>ren a presenting to an emergencydepartment as a result of a road traffic crash in four countries bin 2007Other3.2%Fracture21.1%Boys 11.5 9.7 13.3 8.7 23.4 13.8Girls 7.4 8.3 9.3 4.5 7.9 7.5Source: WHO (2008), Global Burden of Disease: 2004 update.C<strong>on</strong>cussi<strong>on</strong>26.0%Sprain10.7%MorbidityThe number of <strong>child</strong>ren injured or disabled each year asa result of road traffic crashes is not precisely known, buthas been estimated at around 10 milli<strong>on</strong>. This figure isbased <strong>on</strong> data from health-care instituti<strong>on</strong>s that suggestthat <strong>child</strong>ren make up between a fifth and a quarter ofthose involved in a road traffic crash and admitted to ahospital (10–12). However, community-based surveysfrom Asia suggest that the figure could be much higher.The surveys found that, for every <strong>child</strong> who died as aresult of a traffic <strong>injury</strong>, 254 presented to a hospital facilitywith injuries, four of whom where left with permanentdisabilities (13).In <strong>child</strong>ren under the age of 15 years, road traffic injuresrank as the eleventh cause of death and the tenth cause ofburden of disease am<strong>on</strong>g <strong>child</strong>ren (see Statistical Annex,Table A.2). Globally, road traffic injuries am<strong>on</strong>g this agegroup account for 9482 disability-adjusted life years lost –1.7% of the total disability-adjusted life years lost.In general, there is a lack of data <strong>on</strong> morbidity,particularly from low-income and middle-incomecountries. This is partly because not all <strong>child</strong>ren injuredin road traffic incidents are taken to hospital and partly asa result of poor data collecti<strong>on</strong> systems.Nature and severity of road traffic injuriesThe head and limbs are the most comm<strong>on</strong> parts of the bodyinjured in <strong>child</strong>ren involved in road traffic crashes. Theseverity of injuries will vary, depending <strong>on</strong> the age of the<strong>child</strong>, the type of road user and whether protective deviceswere used. A recent school-based survey c<strong>on</strong>ducted byWHO looked at 13–15-year-olds in 26 countries. Of those<strong>child</strong>ren <str<strong>on</strong>g>report</str<strong>on</strong>g>ing an <strong>injury</strong> involving a motor vehicle inthe previous 12 m<strong>on</strong>ths, 10% had sustained a minor head<strong>injury</strong> and 37% had fractured a limb.abBruise13.6%Children were under 12 years.The four countries were Bangladesh, Colombia, Egypt and Pakistan.Source: Statistical Annex, Table C.1.Cut/open wound25.3%Chest and abdominal injuries, although not as comm<strong>on</strong>as head and limb injuries, can be very serious becauseof the organs involved and the difficulties in managingsuch injuries. Multiple trauma has also been <str<strong>on</strong>g>report</str<strong>on</strong>g>ed inapproximately 10% to 20% of <strong>child</strong>ren involved in roadtraffic crashes (14).C<strong>on</strong>sequences of road traffic injuriesRoad traffic injuries are a leading cause of disability for<strong>child</strong>ren. Recent surveys in Asia show that road trafficinjuries are <strong>on</strong>e of the five leading causes of disability for<strong>child</strong>ren. The exact proporti<strong>on</strong> of <strong>child</strong>ren disabled by roadtraffic injuries varies by age group and across countries(15). According to these surveys, the rate of permanentdisability am<strong>on</strong>g <strong>child</strong>ren aged 1 to 17 years injured as aresult of a road traffic crash was 20 per 100 000 <strong>child</strong>ren.In additi<strong>on</strong>, significant numbers of <strong>child</strong>ren requiredhospitalizati<strong>on</strong> or missed school as a result of their injuries(see Figure 2.4).Studies c<strong>on</strong>ducted am<strong>on</strong>g both adults and <strong>child</strong>renhighlight the fact that many individuals still retain somefuncti<strong>on</strong>al disability 6 to 12 m<strong>on</strong>ths following a roadtraffic crash. Clearly, the type of <strong>injury</strong> sustained affectsthe period needed for complete recovery. Research inBangalore, India, for instance, found that 14% of <strong>child</strong>renwho sustained a traumatic brain <strong>injury</strong> from a road trafficWORLD REPORT ON CHILD INJURY PREVENTION 33
FIGURE 2.4Severity of road traffic injuries per 100 000 populati<strong>on</strong> am<strong>on</strong>g<strong>child</strong>ren aged 0–17 years, in five Asian countries aRate per 100 000 <strong>child</strong>rena300250200150100500Bangladesh, China (Beijing, Jiangxi province), Philippines, Thailand, Viet Nam.Source: Reference 15.MissedschoolHospital1–9 daysHospital10+ daysPermanentdisabilityDeathcrash still required assistance with day-to-day activitiessix m<strong>on</strong>ths after the crash (16).The outcome of a road traffic <strong>injury</strong> is also related toroad user type. One study found that 72% of pedestrians,64% of bicyclists struck by a car, and 59% of <strong>child</strong> vehicleoccupants required assistance six m<strong>on</strong>ths after a crash(17). In Canada, 22% of bicyclists injured without a motorvehicle being involved in the incident required subsequentassistance (18).Disabilities and impairments impede the progress of<strong>child</strong>ren in their early years depriving them of educati<strong>on</strong>and social development. Children who sustain disabilitiesfollowing a road traffic crash frequently require l<strong>on</strong>g-termcare and their quality of life is often poor. The excessivestrain placed <strong>on</strong> families who have to care for their injured<strong>child</strong>ren may result in adults having to leave their jobs,leading to c<strong>on</strong>diti<strong>on</strong>s of poverty.Psychosocial impactA number of mental health c<strong>on</strong>diti<strong>on</strong>s have been observedin <strong>child</strong>ren following a road traffic crash. These includephobias, post-traumatic stress disorder and anxiety, as wellas behavioural problems. These psychosocial disturbancesmay be exacerbated by family impoverishment followinga road traffic crash, particularly if a parent or caregiverwas also involved in the collisi<strong>on</strong> and was severely injuredor died. Injured <strong>child</strong>ren can thus experience high levelsof psychosocial distress (19) and feel isolated in theirsuffering (20).Several studies have <str<strong>on</strong>g>report</str<strong>on</strong>g>ed high levels of distress in<strong>child</strong>ren during and immediately after a road traffic <strong>injury</strong>(17, 21, 22). One study <str<strong>on</strong>g>report</str<strong>on</strong>g>ed that that within five days ofa traumatic event, such as a road traffic crash, 98% of the<strong>child</strong>ren involved suffered post-traumatic stress disorder,depressi<strong>on</strong> or anxiety. One m<strong>on</strong>th after <strong>injury</strong>, 82% stillhad symptoms. Twelve m<strong>on</strong>ths after <strong>injury</strong>, 44% were stillhaving flashbacks, feared being injured again, or sufferedmood disorders, body-image changes, sleep disturbancesor anxiety (23). Another study found that a quarter of<strong>child</strong>ren were exhibiting post-traumatic stress disorderthree m<strong>on</strong>ths after the crash (22).Road traffic crashes can also have a profoundpsychological effort <strong>on</strong> <strong>child</strong>ren not directly involved inthe incident themselves but who lose a parent or caregiver(see Box 2.1). Results from Asia show that am<strong>on</strong>g orphans,20% to 66% have lost a father, mother or both in roadtraffic crashes (15). The loss of a parent or parents can leavea <strong>child</strong> with l<strong>on</strong>g-term psychosocial problems as well asec<strong>on</strong>omic impoverishment.Types of road userChildren suffer injuries while in a variety of roles relatedto different types of transport. They may be pedestrians,bicyclists, car occupants, motorcycle riders or motorcyclepassengers, or passengers <strong>on</strong> public transport. In somecountries, <strong>child</strong>ren work <strong>on</strong> the streets, usually sellingmerchandise, where they weave in and out of movingtraffic.BOX 2.1Children orphaned through roadtraffic deathsThe Bangladesh Health and Injury Survey, a populati<strong>on</strong>-based surveyof 171 366 households, was c<strong>on</strong>ducted in 2003. A verbal autopsy modulewas used, adapted from the WHO standards for verbal autopsy(24), with specific questi<strong>on</strong>s <strong>on</strong> each type of <strong>injury</strong>. Data were analysedfor the causes of death of parents of <strong>child</strong>ren aged 0 to 17 years.Injury was a leading cause of death of parents of <strong>child</strong>ren underthe age of 18 years. Some 4 300 mothers die from injuries in Bangladesheach year, leaving about 17 700 <strong>child</strong>ren without their primarycaregiver. As shown in the table below, the leading cause of <strong>injury</strong>death for mothers is suicide (41%), followed by road traffic crashes(29%), burns (12%) and violence (10%).CAUSES OF INJURY-RELATED DEATHS AMONG PARENTS OF CHILDRENAGED 0–17 YEARSCauses of all <strong>injury</strong> deaths (%)Suicide Road traffic Burns Violence Falls OtherinjuriesMothers 41 29 12 10 3 5Fathers 12 36 0 27 5 13Source: Reference 8.Around 7 900 fathers die from <strong>injury</strong> annually, leaving nearly22 100 <strong>child</strong>ren in households that have lost their primary wageearner. The most comm<strong>on</strong> causes of <strong>injury</strong> death in fathers are roadtraffic crashes (36%), followed by violence (27%) and suicide (12%).Children deprived of <strong>on</strong>e or both parents are vulnerable to malnutriti<strong>on</strong>,illness, impaired development, psychosocial trauma, exploitati<strong>on</strong>and abuse. In Bangladesh, as in many countries, fatal injuries ofparents are a significant cause of orphaning. This damages the <strong>child</strong>renleft behind and is a huge burden <strong>on</strong> society. As well as preventing injuriesam<strong>on</strong>g <strong>child</strong>ren, societies need to take greater steps to reducethe incidence of injuries, both unintenti<strong>on</strong>al and intenti<strong>on</strong>al, am<strong>on</strong>gadults.34 WORLD REPORT ON CHILD INJURY PREVENTION
The patterns of road use am<strong>on</strong>g <strong>child</strong>ren vary bycountry, affecting the type of injuries they sustain (seeFigure 2.5).FIGURE 2.5Proporti<strong>on</strong> of fatal road traffic deaths am<strong>on</strong>g <strong>child</strong>ren a by typeof road user in selected OECD countriesAustraliaCanadaCzech RepublicDenmarkFinlandFranceGermanyIcelandNetherlandsNew ZealandNorwayPolandRepublic of KoreaSpainSwedenSwitzerlandTurkeyUnited KingdomUnited States0 20 40 60 80 100Proporti<strong>on</strong> of all road traffic injuries (%)aThese data refer to <strong>child</strong>ren under the age of 15 years.OECD = Organisati<strong>on</strong> for Ec<strong>on</strong>omic Co-operati<strong>on</strong> and Development.Source: Reference 25, reproduced with permissi<strong>on</strong>.Bicyclists Car passengers PedestriansPedestriansGlobally, pedestrians form the single largest category of<strong>child</strong>ren involved in road traffic crashes. In high-incomecountries between 5% and 10% of <strong>child</strong>ren suffering roadtraffic injuries are pedestrians, while in low-income andmiddle-income countries the proporti<strong>on</strong> ranges from 30%to 40% (26). Child pedestrian <strong>injury</strong> is highest in Africaand Asia where it is usual for people to walk al<strong>on</strong>g roads(12, 15). Despite significant reducti<strong>on</strong>s in <strong>child</strong> pedestrian<strong>injury</strong> in many high-income countries, the preventi<strong>on</strong>of such <strong>injury</strong> remains a problem, particularly am<strong>on</strong>g5–14-year-olds.OccupantsChildren injured or killed while travelling in cars asoccupants are a serious c<strong>on</strong>cern in high-income countries,where such cases can account for up to 50% of <strong>child</strong>hoodtraffic deaths (27). As motorizati<strong>on</strong> increases, <strong>child</strong>occupant deaths are also an emerging problem in manymiddle-income countries.BicyclistsIn many countries, <strong>child</strong>ren are taught to ride bicycles asa form of recreati<strong>on</strong>. In many parts of Asia, bicycles arealso a comm<strong>on</strong> means of transport. This is reflected in thestatistics. Bicyclists c<strong>on</strong>stitute 3%–15% of <strong>child</strong>ren injuredin traffic collisi<strong>on</strong>s and 2%–8% of <strong>child</strong> traffic-relatedfatalities around the world (26). In some Asian countries,though, the latter figure can be as high as 33% (28). Whilethere has been a decline in bicyclist deaths am<strong>on</strong>g <strong>child</strong>renin high-income countries (27), bicycle-related injuriesare increasing in many low-income and middle-incomecountries, particularly in South-East Asia and the WesternPacific (28).MotorcyclistsWhere motorcycles are comm<strong>on</strong>ly family vehicles,<strong>child</strong>ren may begin to travel <strong>on</strong> motorcycles at an earlyage, either sitting <strong>on</strong> the petrol tank or behind thedriver. In some Asian countries, where motorized twowheelersare the most comm<strong>on</strong> form of transportati<strong>on</strong>and <strong>child</strong>ren are legally allowed to drive small-enginemotorcycles from their 15th year, motorcycle crashesare the leading cause of mortality and morbidity am<strong>on</strong>gteenagers (15).Young driversInjuries and fatalities am<strong>on</strong>g young drivers are a majorproblem in high-income countries, where a large studyshowed that crashes involving young drivers accountedfor between 20% and 30% of all road traffic fatalities (29).In particular, young drivers are at high risk of a crash intheir first year of driving by themselves. Research fromSweden shows that novice drivers are 33 times more likelyto have a crash than other drivers (30), while in WesternAustralia, drivers <strong>on</strong> a provisi<strong>on</strong>al licence are 15 timesmore likely than older drivers to be involved in a crash(31). In the United States, the risk of a crash for a driveraged 16 years is five times the average risk for all ages (32)(see Figure 2.6). Although mortality rates am<strong>on</strong>g youngdrivers have decreased in most high-income countries inrecent decades, the relative proporti<strong>on</strong> of young driversam<strong>on</strong>g all drivers killed remains high, c<strong>on</strong>firmingthat greater preventi<strong>on</strong> efforts are required am<strong>on</strong>g thiscategory of road user.Heavy vehiclesOnly a few studies have specifically examined the risk to<strong>child</strong>ren involved in heavy vehicle crashes (33). Publictransport vehicles for <strong>child</strong>ren are primarily buses, heavyvehicles and school transport vehicles. Unsafe buses inlow-income and middle-income countries are frequentlyinvolved in major crashes involving <strong>child</strong>ren. In highincomecountries, the greatest risk to school <strong>child</strong>ren iswhile alighting from a bus – rather than from a crashinvolving a school bus (34, 35).WORLD REPORT ON CHILD INJURY PREVENTION 35
FIGURE 2.6Driver crash involvement per milli<strong>on</strong> miles a travelled by driverage, United States, 2001–2002Crash involvement permili<strong>on</strong> miles travelleda30252015105016 17 18 19 20– 25– 30– 35– 40– 45– 50– 55– 60– 65– 70– 75– 80– 85+1 mile is approximately 1.60934 kilometres.Source: Reference 32, reproduced with permissi<strong>on</strong>.Ec<strong>on</strong>omic impact of road traffic injuriesThe global losses due to road traffic injuries are estimatedto be US$518 billi<strong>on</strong> per annum (36), with the annualcost of road crashes in low-income and middle-incomecountries estimated at between US$65 billi<strong>on</strong> and US$100billi<strong>on</strong>. This means that road traffic collisi<strong>on</strong>s and theirc<strong>on</strong>sequences cost governments up to 3% of their grossnati<strong>on</strong>al product (1). Informati<strong>on</strong> <strong>on</strong> the global cost ofroad traffic injuries exclusively am<strong>on</strong>g <strong>child</strong>ren is notavailable.The direct and indirect costs of road traffic injuries, bothfor those directly involved and for nati<strong>on</strong>al ec<strong>on</strong>omies, arenumerous. The direct and indirect costs include:– permanent disabilities;– loss of schooling;– medical care;– legal costs;– vehicle repair costs;– loss of income to parents, resulting from absence fromwork to care for the <strong>child</strong>.In additi<strong>on</strong>, there are l<strong>on</strong>g-term ec<strong>on</strong>omic costs arisingfrom: premature death; rehabilitati<strong>on</strong>; the loss of healthyyears in <strong>child</strong>ren; and the inability of those with seriousdisabilities to work to the full extent.The poor, who are over-represented in road traffic crashstatistics, are hardest hit by these costs. Findings fromresearch in Bangladesh and India suggest that there is afurther decline into poverty when the poor are injured.This is because additi<strong>on</strong>al resources are needed to carefor the injured pers<strong>on</strong>, achieved by taking <strong>on</strong> extra work,selling assets or taking out further loans (37).Limitati<strong>on</strong>s of dataAge (years)Many countries do not have <strong>injury</strong> surveillance systemsthat provide reliable data <strong>on</strong> road traffic crashes andinjuries. Indicators, particularly <strong>on</strong> n<strong>on</strong>-fatal outcomes,are scarce and those that are used suffer from a lack ofstandard definiti<strong>on</strong> – particularly as regards what is meantby minor, moderate or severe injuries. There are frequentdisparities between data – for example, between police andhealth-related sources – making comparis<strong>on</strong>s difficult (1).These difficulties are made worse by the fact that there iswidespread under-<str<strong>on</strong>g>report</str<strong>on</strong>g>ing of road traffic fatalities andinjuries – both in health-related and police data.In additi<strong>on</strong> to these limitati<strong>on</strong>s, there is an additi<strong>on</strong>alproblem of different age cut-off points when dealing with<strong>child</strong>-related road traffic injuries and deaths. This makescomparis<strong>on</strong>s particularly difficult.Solid data are needed to provide a basis for decisi<strong>on</strong>making.Establishing a simple, cost-effective system orimproving systems currently in use should be prioritiesin improving road safety. All the same, a current lack ofreliable data should not prevent other necessary measuresfrom being undertaken.Risk factorsMost of the factors that increase the risk of road trafficinjuries for the general populati<strong>on</strong> do so similarly for<strong>child</strong>ren. Thus <strong>child</strong>ren are affected by speeding anddrink-driving, by not using safety equipment and byfactors related to vehicle safety and the road envir<strong>on</strong>ment.However, there are also risk factors that are specific to<strong>child</strong>ren. The road envir<strong>on</strong>ment is c<strong>on</strong>structed withc<strong>on</strong>siderati<strong>on</strong> for adults. It is not built for use by <strong>child</strong>ren,and when <strong>child</strong>ren come into c<strong>on</strong>tact with it they areplaced at greater risk than need have been the case. The setof risk factors that increase a <strong>child</strong>’s susceptibility in roadtraffic can be c<strong>on</strong>sidered within the c<strong>on</strong>ceptual frameworkof the Hadd<strong>on</strong> Matrix (see Table 2.2).Child-related factorsPhysical developmentA <strong>child</strong>’s head, chest, abdomen and limbs are all in a stateof growth. Their relative softness make a <strong>child</strong> physicallymore vulnerable to the impact of <strong>injury</strong> than an adult.Furthermore, the smaller physical stature of <strong>child</strong>ren cancreate problems, as it limits their ability to see or be seenover certain heights such as parked cars or large trucks – aknown risk factor in <strong>child</strong> pedestrian injuries. Children’ssensory facilities are also less fully developed. Their abilityto synthesize informati<strong>on</strong>, from their peripheral fields ofvisi<strong>on</strong> and their auditory sense, is limited, which can leadto their missing critical cues of danger, thus increasingtheir risk of road traffic <strong>injury</strong> (38).Cognitive developmentThe developmental processes taking place in <strong>child</strong>ren havean effect <strong>on</strong> their ability to make safe decisi<strong>on</strong>s in the roadenvir<strong>on</strong>ment, and these processes are closely related to age(39).36 WORLD REPORT ON CHILD INJURY PREVENTION
TABLE 2.2Hadd<strong>on</strong> Matrix applied to the risk factors for road traffic crash injuries am<strong>on</strong>g <strong>child</strong>renChild factors Vehicle and safety equipment Physical envir<strong>on</strong>ment Socioec<strong>on</strong>omic envir<strong>on</strong>mentPre-eventEventPost-eventAge; gender; lack of supervisi<strong>on</strong>;risk-taking; impulsivebehaviour; disobedience; lackof police enforcement.Size and physical developmentof <strong>child</strong>; lack of equipmentto protect occupants, orequipment improperly used;underlying c<strong>on</strong>diti<strong>on</strong>s in <strong>child</strong>.Child’s lack of resilience;<strong>child</strong>’s general c<strong>on</strong>diti<strong>on</strong>; lackof access to appropriate healthcare; post-<strong>injury</strong> complicati<strong>on</strong>s.Lack of roadworthiness of vehicle;poor lighting; poor state ofbrakes; speeding; overloading.Child restraints and seat-beltsnot fitted or incorrectly used;bicycle and motorcycle helmetsnot used; poor design of vehiclefor protecti<strong>on</strong> in crashes; norollover protecti<strong>on</strong>.Difficult access to victim; lack oftrained health-care and rescueworkers.Poor road design; lack of publictransport; no enforcement ofspeed limits; no safety barriers;lack of alcohol laws; poor infrastructurefor pedestrian safety.Roadside objects such as treesand poles.Lack of availability of adequatepre-hospital care, acute care andrehabilitati<strong>on</strong>.Poverty; single-parent family;large family size; poor maternaleducati<strong>on</strong>; lack of awareness ofrisks am<strong>on</strong>g caregivers, <strong>child</strong>careproviders and educators.Lack of safety culture in the carand <strong>on</strong> the road.Lack of culture of supportinginjured people; no first aid givenat scene.Young <strong>child</strong>ren aged between five and seven years havemastered the c<strong>on</strong>cepts of speed and distance (40). However,they exhibit poor skills in recognizing dangerous places tocross the road, relying exclusively <strong>on</strong> the visible presenceof cars in the vicinity. They are also unlikely to assessthe presence of <strong>on</strong>coming traffic with accuracy. “Blind”secti<strong>on</strong>s of the road, obstacles by the road that couldobscure a <strong>child</strong> from a driver’s field of visi<strong>on</strong> and complexroad juncti<strong>on</strong>s are not perceived by young <strong>child</strong>renas threatening situati<strong>on</strong>s (39, 41). Road traffic crashesinvolving young <strong>child</strong>ren include a large proporti<strong>on</strong> of“dart and dash” cases. In such cases, a <strong>child</strong> pedestrian isinjured through a “critical behavioural error”, where it hasfailed to stop or slow down before attempting to cross theroad. This type of behaviour is due to a <strong>child</strong>’s “centrati<strong>on</strong>”– the inability of the <strong>child</strong> to switch attenti<strong>on</strong> from <strong>on</strong>etask to another (42).These cognitive processes are more developed in<strong>child</strong>ren aged 11 years and older who appear to be ableto recognize a given road locati<strong>on</strong> as dangerous andshow judgement that allows them to be safe <strong>on</strong> the roads(43). Children over the age of 12 years have the capacityto modify their behaviour when faced with a situati<strong>on</strong>involving two tasks.This is an area of <strong>on</strong>going research and new evidencerelating to <strong>child</strong>ren’s abilities <strong>on</strong> the road is regularlypublished. Two issues have recently arisen in thisc<strong>on</strong>necti<strong>on</strong>, both related to cognitive development.There is growing evidence that, although the visualprocesses needed for a <strong>child</strong> to cross a road are fullydeveloped as infants, the full integrati<strong>on</strong> of visualsignals into a meaningful c<strong>on</strong>text is not fully developeduntil <strong>child</strong>ren are around 10–12 years old (44, 45).Cognitive processes taking place in an adolescent’sbrain could affect their risk of road traffic crash asyoung drivers. Through the use of brain-imagingtechniques, neurobiological research c<strong>on</strong>ducted overthe past decade has found that parts of the fr<strong>on</strong>tal lobe– in particular the prefr<strong>on</strong>tal cortex which governsjudgement, decisi<strong>on</strong>-making, reas<strong>on</strong>ing and impulsec<strong>on</strong>trol – appears not to fully mature until the age of20 or 25 years (46). While research linking this newevidence <strong>on</strong> brain development directly to drivinghas yet to be undertaken, these findings provide someinsight into the biological mechanisms that may putmany young drivers at risk.Risk-taking behaviourWhile young <strong>child</strong>ren may inadvertently take risksbecause they lack appropriate skills to do otherwise,older <strong>child</strong>ren and adolescents may actively seek outrisk. Risk-taking behaviour may allow adolescents tofeel a sense of c<strong>on</strong>trol over their lives or else to opposeauthority. Research shows that there are high levels ofsensati<strong>on</strong>-seeking behaviour am<strong>on</strong>g young adults andthat there exists a need to maintain a heightened levelof physiological arousal. Young people c<strong>on</strong>sequentlyseek new situati<strong>on</strong>s and experiences to maintain thislevel, irrespective of the risks inherent in the experience.Such sensati<strong>on</strong>-seeking frequently focuses <strong>on</strong> riskybehaviours, including while driving a vehicle or crossinga road. Sensati<strong>on</strong>-seeking has been shown to rise betweenthe ages 9 and 14 years, peaking in late adolescence or inearly adulthood, and declining steadily with age (47).Risk-seeking behaviour is a significant predictor ofinvolvement in road traffic <strong>injury</strong> am<strong>on</strong>g <strong>child</strong> pedestriansas it is for young adolescent drivers aged 16–17 years (48–50). Across all ages and particularly am<strong>on</strong>g the young,sensati<strong>on</strong>-seeking is more comm<strong>on</strong> am<strong>on</strong>g boys thanam<strong>on</strong>g girls. Boys as young as 11 years have a greaterWORLD REPORT ON CHILD INJURY PREVENTION 37
affinity for speed, risk-taking and competitive behaviour,all of which place them at an increased risk of road traffic<strong>injury</strong> (51).A certain amount of risk-taking is a normalphysiological attribute and is necessary for a <strong>child</strong>’sgrowth and development. Children, though, often do notrealize that they need to make a complex set of decisi<strong>on</strong>s toavoid harm. It is the resp<strong>on</strong>sibility of adults to understandthe vulnerability of <strong>child</strong>ren in the road envir<strong>on</strong>ment andtheir developmental limitati<strong>on</strong>s, and to ensure their safetyby providing developmentally appropriate behaviouralinterventi<strong>on</strong>s.Peer influenceAs young <strong>child</strong>ren become adolescents, they enter a phasewhere the influence of their parents is reduced, and theybegin to discover and assert their independence. Thistransiti<strong>on</strong> can be expressed in their lifestyle, and in anincreasing c<strong>on</strong>formity with certain social norms, that inturn influence their behaviour and decisi<strong>on</strong>-making. Formany young people, peers are of significant importanceand can be the primary source of the social norms withwhich they strive to c<strong>on</strong>form (29).Social norms, including peer pressure and the emphasisplaced <strong>on</strong> rebelli<strong>on</strong> in the culture of young people, can affectthe manner in which young people drive a vehicle. Directpeer pressure may be exerted <strong>on</strong> the driver’s behaviourthrough the influence of a passenger. Research has shownthat young drivers experience higher peer pressure thanolder drivers to commit traffic violati<strong>on</strong>s such as speeding,driving under the influence of alcohol and dangerousovertaking (52). There is a close link between the presenceof similarly aged passengers in the car and increasing risklevels. A number of studies have shown that young drivers,both male and female, drive faster and with a shorterfollowing distance at road juncti<strong>on</strong>s if they have youngpassengers in the car (51, 53).GenderThere is evidence of a str<strong>on</strong>g relati<strong>on</strong>ship between gender,road safety behaviour and road traffic <strong>injury</strong>. Most studiesc<strong>on</strong>ducted show a str<strong>on</strong>g male bias, with the male-tofemaleratio ranging between 3:1 and 5:1. This relati<strong>on</strong>shipholds true across different regi<strong>on</strong>s of the world and appliesto fatal and n<strong>on</strong>-fatal injuries.A part of the predominance of boys in road traffic <strong>injury</strong>statistics can be accounted for by differences in exposure.Research <strong>on</strong> 10–12-year-old boy pedestrians has foundthat the amount of exposure, together with nature of theroad envir<strong>on</strong>ment, influences <strong>injury</strong> rates am<strong>on</strong>g thisgroup, particularly those from poorer areas (54). However,exposure does not account for the entire difference.Am<strong>on</strong>g young drivers, men have more fatal crashes perkilometre driven than do young women, even taking intoc<strong>on</strong>siderati<strong>on</strong> their increased exposure levels. Factorsthought to c<strong>on</strong>tribute towards this difference includeincreased risk-taking and sensati<strong>on</strong>-seeking.Type of road userThere is no specific age at which <strong>child</strong>ren can be saidto be safe road users. Children understand and react tocomplex traffic situati<strong>on</strong>s in different ways from adults.Younger <strong>child</strong>ren have different informati<strong>on</strong>-processingand psychomotor abilities compared to older <strong>child</strong>ren.Adolescents are characterized by impulsiveness, curiosityand experimentati<strong>on</strong>. Developmentally, <strong>child</strong>ren developat different rates and the differences between individualscan be large.PedestriansIn many parts of the world the majority of <strong>child</strong>ren injuredor killed <strong>on</strong> the roads are pedestrians, particularly inlow-income and middle income countries. The physicaland cognitive developmental factors already discussedincrease the risk of a road traffic crash am<strong>on</strong>g <strong>child</strong>pedestrians, especially am<strong>on</strong>g younger <strong>child</strong>ren, wherephysical stature and cognitive limitati<strong>on</strong>s restrict theirability to make safe decisi<strong>on</strong>s. In many low-income andmiddle-income countries <strong>child</strong>ren use roads for playingand for c<strong>on</strong>ducting small roadside businesses, both ofwhich increase their exposure significantly. Risk-takingbehaviour and peer pressure may increase risk am<strong>on</strong>gadolescents who are pedestrians.OccupantsFor young <strong>child</strong>ren who are occupants of vehicles themain risk factor is the lack or improper use of a restraint.Children should be strapped in appropriate restraintsbased <strong>on</strong> their age, weight or height (Box 2.2). The rateof use of appropriate <strong>child</strong> restraints in motor vehiclesvaries c<strong>on</strong>siderably across countries – from nearly 90%in the United States (55) to almost zero in Oman (56).While many parents use car seats for infants, the use ofappropriate seat restraints decreases markedly after a <strong>child</strong>has outgrown the infant device.Adolescents and young adults have the lowest wearingrates for seat-belts around the world. In a survey of youthrisk behaviour, <strong>on</strong>ly a third of 14–17-year-olds <str<strong>on</strong>g>report</str<strong>on</strong>g>edthat they always wore a seat-belt as a passenger in a vehicle.More than a third noted that they had been a passenger witha driver who had been drinking alcohol (60). In additi<strong>on</strong>,having passengers of around the same age increases thelikelihood of a novice driver, aged 16–18 years, incurringa crash (61).BicyclistsThe major risk to bicyclists relates to exposure (62). Inmost high-income countries, <strong>child</strong>ren ride bicycles forpleasure and so make up a small proporti<strong>on</strong> of roadtraffic deaths, though many minor bicycle collisi<strong>on</strong>s38 WORLD REPORT ON CHILD INJURY PREVENTION
BOX 2.2How <strong>child</strong> restraints prevent injuries to <strong>child</strong> passengersIn the first half of the 20th century, traffic safety efforts c<strong>on</strong>centrated <strong>on</strong> preventing crashes by changing the behaviour of drivers. In the 1950s,c<strong>on</strong>cepts already prevalent in aviati<strong>on</strong> safety, including safety-belts, started to be applied to motor vehicles. Properly fitted seat-belts were foundto absorb the energy caused by a rapid decelerati<strong>on</strong> in a crash. In additi<strong>on</strong>, a safety-belt reduced the risk of ejecti<strong>on</strong> from the vehicle and – if it fittedproperly – spread the forces from a crash over hard b<strong>on</strong>es rather than softer internal organs. The first laws came in 1966, when the United Statesfederal government introduced regulati<strong>on</strong>s requiring new vehicles to be equipped with seat-belts.European engineers recognized that biological differences between adults and <strong>child</strong>ren would limit the effectiveness of seat-belts for <strong>child</strong>ren.In the 1960s, they came up, for the first time, with a design specifically for <strong>child</strong>ren. This was a seat with <strong>child</strong>-sized internal harnesses attached tothe vehicle frame by the vehicle’s safety-belt. Various designs to accommodate growing <strong>child</strong>ren followed quickly. In 1963, the first rear-facing infantseat was developed.Despite the commercial availability by the late 1960s of both seat-belts and <strong>child</strong> restraint systems, their safety benefits were not widely publicizedand their use remained low. As countries became increasingly motorized, the numbers of deaths from crashes c<strong>on</strong>tinued to rise. In 1970,the Australian state of Victoria introduced a safety-belt law and by 1977, rates of seat-belt use in the state had increased to 90%. Other countriesgradually followed with their own seat-belt laws.In the United States, in the late 1970s, studies found that infant deaths were over-represented am<strong>on</strong>g <strong>child</strong> passenger fatalities (57). The stateof Tennessee, in 1978, was the first to adopt a <strong>child</strong> restraint law for all <strong>child</strong>ren under the age of four years. As a result, <strong>child</strong> restraint use increasedfrom 8% to 30% and the incidence of deaths am<strong>on</strong>g <strong>child</strong> passengers was halved. By 1985, all of the United States and many other countries hadintroduced similar <strong>child</strong> restraint laws. Today, most of these laws havebeen amended to include requirements for the use of belt-positi<strong>on</strong>ingbooster seats, that are effective in preventing injuries to <strong>child</strong>ren whohave outgrown their <strong>child</strong> safety seats (58).Ideas about how best to protect <strong>child</strong> passengers c<strong>on</strong>tinue to evolvewith new scientific findings and new technology. It is important,however, always to follow the current guidelines for the safety of <strong>child</strong>passengers (59). These guidelines urge that <strong>child</strong> restraint systemsthat have been certified as passing nati<strong>on</strong>al standards should be usedand that <strong>child</strong>ren should be placed in the rear seat. In rapidly motorizingcountries, <strong>child</strong> deaths and injuries can be avoided through programmesand laws to promote <strong>child</strong> restraint use, through nati<strong>on</strong>alstandards to deliver the full benefits of the <strong>child</strong> restraint systems,and through a surveillance system to identify emerging hazards to<strong>child</strong>ren.© NCIPCare never <str<strong>on</strong>g>report</str<strong>on</strong>g>ed to the police (63). However, in manylow-income and middle-income countries where cyclingprincipally exists as a mode of transport, the proporti<strong>on</strong>of road traffic deaths is c<strong>on</strong>siderably higher. In Beijing,for example, about a third of all traffic deaths are thoseof cyclists (28).Other risks associated with bicycling include:– the lack of correctly worn helmets (64);– riding in mixed patterns of traffic (33);– cycling <strong>on</strong> pavements (65);– the visibility of cyclists (66).The rate of helmet wearing am<strong>on</strong>g <strong>child</strong> cyclists islow in many countries, even in developed countries. Astudy c<strong>on</strong>ducted in South Africa in the late 1990s showedthat <strong>on</strong>ly 1.4% of <strong>child</strong>ren presenting to an emergencydepartment following a bicycle-related <strong>injury</strong> had worn ahelmet at the time of the collisi<strong>on</strong> (67), although in thoseprovinces where there were laws <strong>on</strong> helmet wearing, therates were higher (68).MotorcyclistsAs with other types of road users, the greatest risk for<strong>child</strong>ren <strong>on</strong> motorcycles relates to exposure. In manycountries <strong>child</strong>ren travel as passengers <strong>on</strong> a motorcyclefrom a very young age. The rates of helmet wearing am<strong>on</strong>gthese small <strong>child</strong>ren is very low – partly as a result of thelack of appropriately sized helmets, or of their cost.In many countries adolescents are legally entitled todrive a motorcycle with a restricted engine size from theage of 15 years. This age, though, coincides with a periodin the <strong>child</strong>’s development in which risk-taking behaviouris known to occur. Unsurprisingly, in some countries upto a third of all motorcycle deaths are young riders or theirpassengers (69). The use of helmets am<strong>on</strong>g motorcyclistsand their passengers is low in many countries and is asignificant risk factor for head injuries (70). In Viet Nam,for instance, helmet wearing rates am<strong>on</strong>g adolescent andyoung adult riders are generally lower than those am<strong>on</strong>golder adults (71).WORLD REPORT ON CHILD INJURY PREVENTION 39
Studies have shown that helmet wearing is highlydependent <strong>on</strong> the presence of a law mandating helmet use(60). The absence of universal helmet laws that cover allages, together with poor enforcement and high prices forstandard helmets, may c<strong>on</strong>tribute to the low prevalence ofmotorcycle helmet use in many places.Young driversAdolescent and young drivers are a special risk group. Anumber of countries have <str<strong>on</strong>g>report</str<strong>on</strong>g>ed increased collisi<strong>on</strong>sand deaths am<strong>on</strong>g novice drivers, particularly during theirfirst year of driving (72–75). For a given distance driven,16-year-old drivers are more than twice as likely as driversaged 20–24 years, and four times as likely as drivers aged25–29 years, to be involved in a fatal passenger vehiclecrash (76). A number of interrelated factors appear to placeyoung drivers at an elevated risk for road traffic <strong>injury</strong>.Age appears to be independent of the level of drivingexperience (29, 75, 77). Novice drivers aged 16–19 yearshave more crashes than novice drivers aged 20 yearsand over with the same amount of driving experience(77). However, there is a sharp decrease in crash riskduring the first few years of driving, mainly associatedwith experience rather than age.Risky behaviours am<strong>on</strong>g young drivers include thefollowing.– Drinking and driving. Alcohol significantly impairsdriving ability am<strong>on</strong>g adolescents – typicallyat lower blood c<strong>on</strong>centrati<strong>on</strong> levels than is thecase for adults. New evidence suggests that thephysiological resp<strong>on</strong>se of adolescents to alcoholmight be different to that of adults (78), makingadolescents less sensitive to signals that their abilityis impaired. Research in New Zealand found thatdrivers aged under 20 years were five times morelikely to have elevated blood alcohol c<strong>on</strong>centrati<strong>on</strong>levels compared with drivers aged 30 years and above(79, 80). In the United States, 30% of adolescents<str<strong>on</strong>g>report</str<strong>on</strong>g>ed driving with an intoxicated driver in theprevious m<strong>on</strong>th. One in 10 admitted to drinkingand driving themselves (81).– Speeding. Adolescents are more likely to drive atexcessive speed than are older adults (82). In a surveyof 20 000 drivers aged 16 to 24 years, researchersfound that the younger drivers were significantlymore likely than the older <strong>on</strong>es to drive at more than20 km/h above the speed limit (83).– N<strong>on</strong>-use of seat-belts. Compared with other agegroups, adolescents have the lowest rate of seat-beltuse. In 2005, 10% of high school students in theUnited States <str<strong>on</strong>g>report</str<strong>on</strong>g>ed they rarely or never wore seatbeltswhen in a vehicle with some<strong>on</strong>e else (81).– Distracti<strong>on</strong>. Using a mobile ph<strong>on</strong>e, iPod or otherelectr<strong>on</strong>ic device, even if it is operated using handsfreedevices, leads to slower informati<strong>on</strong> processingand c<strong>on</strong>sequently an increased risk of a crash (84).The risk is even greater than that caused by thedistracti<strong>on</strong> of two or more passengers in the car(85).– Fatigue. Adolescent drivers who lack adequate sleepare at greater risk of crashing. Fatigue can alsoexacerbate the effects of other risk factors such asalcohol, speed and inexperience (86–88).Young drivers of both sexes have a higher proporti<strong>on</strong> ofroad traffic crashes in the evenings and early mornings.Many of these crashes involve <strong>on</strong>ly a single vehicle.The presence of other adolescents in the vehicle with anadolescent driver is <strong>on</strong>e of the str<strong>on</strong>gest predictors of acrash (73, 82, 89–91).There is a tendency am<strong>on</strong>g young drivers to violatetraffic rules (92). A study in India found that 20% to30% of traffic violati<strong>on</strong>s occurred am<strong>on</strong>g drivers lessthan 20 years of age, with more than a third of thesedrivers either unlicenced or having obtained a licencewithout taking a mandatory test (93).Lack of supervisi<strong>on</strong>Differences in parents’ understanding of what activitiesare safe, given the particular age of the <strong>child</strong>, may partlyexplain the variati<strong>on</strong>s by age, gender and socioec<strong>on</strong>omicstatus in the patterns of road traffic <strong>injury</strong> am<strong>on</strong>g <strong>child</strong>renacross the world. The exact role, though, that a parent’spercepti<strong>on</strong> of risk plays in determining the risk of a <strong>child</strong>incurring a road traffic <strong>injury</strong> is not clear. Attitudes todriving and road use appear to be formed at an age asearly as 11 years, suggesting that a parent’s percepti<strong>on</strong>of risk has the potential to influence a <strong>child</strong>’s behaviour<strong>on</strong> the roads (51). However, there has been little researchto date attempting to quantify the role that parentalpercepti<strong>on</strong> plays in a <strong>child</strong>’s risk for road traffic <strong>injury</strong>.Lack of adult supervisi<strong>on</strong> has often been cited as a riskfactor am<strong>on</strong>g <strong>child</strong>ren for road traffic <strong>injury</strong>. However, itis just <strong>on</strong>e of several interrelated risk factors. There area number of characteristics associated with parents orcaregivers with a limited ability to supervise <strong>child</strong>ren.These include being a single parent, being a workingparent, and being a parent affected by illness or depressi<strong>on</strong>(94). Such characteristics are found in families across theworld, and are fairly independent of the ec<strong>on</strong>omic statusof a country.N<strong>on</strong>etheless, if there is adult supervisi<strong>on</strong>, the probabilityof a <strong>child</strong> incurring road traffic <strong>injury</strong> is significantlyreduced. A Malaysian study found that the risk of <strong>injury</strong>was reduced by 57% am<strong>on</strong>g <strong>child</strong>ren supervised by theirparents (95). Another study, in Canada, found that lack ofparental supervisi<strong>on</strong> increased the risk of <strong>injury</strong> to <strong>child</strong>pedestrians and cyclists by a factor of 2.6 (96). Researchthat examined the risk of <strong>child</strong> pedestrian <strong>injury</strong> inc<strong>on</strong>necti<strong>on</strong> with specific supervisi<strong>on</strong> practices showed astr<strong>on</strong>g positive associati<strong>on</strong> between pedestrian <strong>injury</strong> anda lack of supervisi<strong>on</strong> both after school and <strong>on</strong> the journeyto school (97).40 WORLD REPORT ON CHILD INJURY PREVENTION
PovertyThe socioec<strong>on</strong>omic status of a family affects the likelihoodof a <strong>child</strong> or young adult being killed or injured in a roadtraffic crash, with those <strong>child</strong>ren from poorer backgroundsat greater risk. This relati<strong>on</strong>ship is true not just betweenricher and poorer countries, but within countries as well.Data from both Sweden and the United Kingdom, forinstance, show that the risks of <strong>child</strong>ren and young adultsfor road traffic injuries are higher if they are from poorerfamilies (98–100). In Kenya, the choice of transport usedis often related to a family’s income – with those fromlow-income families more likely to be vulnerable roadusers (101). A study in Mexico found that family size wasstr<strong>on</strong>gly associated with the risk of pedestrian <strong>injury</strong>am<strong>on</strong>g <strong>child</strong>ren (102).Vehicle-related factorsGiven the small stature of <strong>child</strong>ren, poor vehicle designis an important risk factor for <strong>child</strong> road traffic <strong>injury</strong>.The standard design of a vehicle can have a major effect<strong>on</strong> the risk and severity of injuries sustained by a <strong>child</strong>pedestrian, particularly if the <strong>child</strong>’s head makes c<strong>on</strong>tactwith the rigid windshield (103). Vehicle designers arenow examining ways to reduce the severity of pedestrianinjuries. In particular, bumpers are being redesigned soas to prevent a pedestrian’s head making c<strong>on</strong>tact with thefr<strong>on</strong>t window, by allowing the impact to be absorbed bya softer b<strong>on</strong>net (104). The adaptati<strong>on</strong>s of vehicle designthat have successfully reduced the incidence and severityof injuries in collisi<strong>on</strong>s between adult pedestrians andvehicles are now being modified to benefit <strong>child</strong>ren.“Back-over” injuries – usually in a driveway or parkinglot – result when a car is reversed over a small <strong>child</strong>.Children aged between 1 and 3 years are at particularrisk because of their small size and their inability to alertthe driver. Unfortunately, with the increased demand forsports utility vehicles, such injuries are becoming morecomm<strong>on</strong> (105, 106). Many vehicles are now being fittedwith reverse backup sensors that could help reduce theincidence of such injuries (107).As regards bicycle-related factors, about three quartersof the crashes in the Netherlands involving passengers –often <strong>child</strong>ren – carried <strong>on</strong> bicycles are associated with feetbeing trapped in the wheel spokes, and 60% of bicycleshave no protective features to prevent this from occurring(108). Erg<strong>on</strong>omic changes in the design of bicycles canthus lead to an improvement in bicycle safety (108, 109).Envir<strong>on</strong>mental factorsIt is normal for <strong>child</strong>ren to carry out activities in the roadenvir<strong>on</strong>ment – such as cycling, walking, running, playingand other comm<strong>on</strong> group activities. It is also important fortheir healthy development that <strong>child</strong>ren, from an early age,undertake such activities. For this reas<strong>on</strong>, it is importantfor the road envir<strong>on</strong>ment to be safe so that these activitiescan be undertaken without the <strong>child</strong>’s safety being put atrisk.Motorizati<strong>on</strong> and urbanizati<strong>on</strong> are proceeding rapidlyin much of the world today. Increased and more rapidmobility tend to be the goals, while safe mobility – andparticularly the safety of <strong>child</strong>ren – are rarely taken intoaccount. A number of specific envir<strong>on</strong>mental factorsincrease the risk for <strong>child</strong>ren using the road system. Thesefactors include the following:– sites with a volume of traffic exceeding 15 000 motorvehicles per day;– poor planning of land use and road networks,including:l<strong>on</strong>g, straight through-roads that encourage highvehicle speeds, together with mixed land use madeup of residential housing, schools and commercialoutlets (110, 111);a lack of playgrounds, resulting in <strong>child</strong>ren playingin the road;a lack of facilities to separate road users – such as lanesfor bicyclists and pavements for <strong>child</strong> pedestrians(112, 113);the existence of street vendor businesses, in which<strong>child</strong>ren may work;– a lack of safe, efficient public transportati<strong>on</strong> systems;– inappropriate speed, particularly in residential areaswhere <strong>child</strong>ren play or walk to and from school (97,113–115);Lack of prompt treatmentGood recovery from road traffic injuries depends up<strong>on</strong>the availability, accessibility and quality of trauma careservices. Such services are either not available or else arelimited in scope and capacity in many low-income andmiddle-income countries. The surveys c<strong>on</strong>ducted in Asiabrought out the fact that numerous <strong>child</strong>ren are injuredwho do not receive medical care. In Beijing, this ratio ofthose receiving care to those injured was 1:254, while inThailand it was 1:170 (15).The most critical problems in relati<strong>on</strong> to pre-hospitaland emergency care in many low-income and middleincomecountries are (116, 117):– a lack of first-aid services and trained pers<strong>on</strong>nel;– unsafe modes of transportati<strong>on</strong> to reach emergency care;– the l<strong>on</strong>g delay between the time of <strong>injury</strong> and reachinga hospital;– inappropriate referral services;– the absence of a triage system.The availability of good rehabilitati<strong>on</strong> services isalso an important requirement for the proper recoveryof <strong>child</strong>ren following a road traffic <strong>injury</strong>. Again, suchservices may be limited in many countries due to the lackof rehabilitati<strong>on</strong> pers<strong>on</strong>nel, the necessary infrastructureand the availability of guidelines and protocols forrehabilitati<strong>on</strong>.WORLD REPORT ON CHILD INJURY PREVENTION 41
Interventi<strong>on</strong>sMuch has been written over the past decade about howbest to reduce the incidence of road traffic injuries. The<str<strong>on</strong>g>World</str<strong>on</strong>g> <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> road traffic <strong>injury</strong> preventi<strong>on</strong> describesproven interventi<strong>on</strong>s and makes six recommendati<strong>on</strong>s toprevent road traffic injuries at country level (1). Promotingthe systems approach, the <str<strong>on</strong>g>report</str<strong>on</strong>g>’s recommendati<strong>on</strong>s areequally applicable to the preventi<strong>on</strong> of road traffic crashesinvolving <strong>child</strong>ren. There are a number of interventi<strong>on</strong>s,though, that focus specifically <strong>on</strong> <strong>child</strong>ren.The systems approach is of particular value in <strong>child</strong>road safety since it moves away from the idea that <strong>child</strong>renshould adapt their behaviour to cope with traffic, in favourof an approach that recognizes that <strong>child</strong>ren’s needs shouldbe addressed in the design and management of the wholeroad system.Success in improving safety for <strong>child</strong>ren is most likely to be achievedthrough a holistic approach combining measures to address thebehaviour of all road users, to improve the road envir<strong>on</strong>ment and todesign vehicles that better protect both their occupants and those atrisk outside the vehicle (27).The following secti<strong>on</strong>s discuss interventi<strong>on</strong>s that targetyounger road users.Engineering measuresCreating a safe envir<strong>on</strong>ment for <strong>child</strong>ren requires that spacefor walking and cycling is given priority and not treatedas an afterthought, after space for motorized traffic hasbeen designed. The routes that <strong>child</strong>ren are likely to taketo reach schools, playgrounds and shops, and how theseroutes can be integrated into a logical, coherent and safenetwork for walking and cycling, need to be c<strong>on</strong>sidered(118). Greater attenti<strong>on</strong> should be given to how the builtenvir<strong>on</strong>ment can safely cater for the healthy pursuits ofwalking and bicycle riding, while at the same time focusing<strong>on</strong> sustainable public transport systems.Reducing speedThe policies of both Visi<strong>on</strong> Zero in Sweden and sustainablesafety in the Netherlands promote the design of roads andthe setting of speed limits that are appropriate for thefuncti<strong>on</strong> of the road (119, 120). Survival rates for pedestriansand cyclists are much higher at collisi<strong>on</strong> speeds of below30 km/h (1). This speed should be the norm in residentialareas and around schools. Various measures to achieveappropriate speeds should be c<strong>on</strong>sidered (26), including:– traffic-calming measures that reduce the speed of trafficthrough infrastructural engineering measures, suchas:speed humps;mini-roundabouts;designated pedestrian crossings;pedestrian islands;– visual changes – such as treating the road surface, andimproving the road lighting;– the redistributi<strong>on</strong> of traffic – by blocking roads, andcreating <strong>on</strong>e-way streets near schools.Where a higher speed limit is allowed there shouldbe provisi<strong>on</strong> to keep pedestrians and cyclists separatefrom traffic by using single-lane roundabouts, footways,pedestrian signal phasing and pedestrian refuge islands,and to improve safety with better street lighting (121).Managing speed is problematic in many low-incomeand middle-income countries, where the effectivenessof many infrastructural measures proposed for highincomecountries has yet to be tested (122, 123). Somespeed reducti<strong>on</strong> measures have indeed been shown tobe affordable and sustainable in urban areas, such assuccessful introducti<strong>on</strong> of speed humps in Ghana (124).The problem is how to protect vulnerable road users,particularly <strong>child</strong>ren, <strong>on</strong> rural roads, many of which lackessential infrastructural requirements.Safe play areasChildren need access to safe spaces for play and physicalexercise. If such spaces are not available, <strong>child</strong>ren willbe tempted to play <strong>on</strong> the streets. Play spaces should besecure and well maintained, with features that <strong>child</strong>renfind interesting. Designing safe play areas should beincorporated into urban planning and the developmentof school facilities and residential complexes. In theDominican Republic, UNICEF is working with localgovernment authorities to develop safe play areas, underthe “Child Friendly Cities” programme. Working inc<strong>on</strong>sultati<strong>on</strong> with <strong>child</strong>ren and adolescents, a team ofarchitects have planned parks where <strong>child</strong>ren can playsafely (125).Safe routes to schoolMuch effort has been spent <strong>on</strong> designing ways of gettingto school, particularly for <strong>child</strong>ren of primary-school age.The measures include the provisi<strong>on</strong> of buses to transport<strong>child</strong>ren to school and encouraging <strong>child</strong>ren to walk toschool, using the c<strong>on</strong>cept of “walking buses”. In the latter,adult volunteers accompany groups of <strong>child</strong>ren, whowalk al<strong>on</strong>g safe routes wearing c<strong>on</strong>spicuous, possiblyfluorescent, vests. Walking buses teach <strong>child</strong>ren howto walk safely, as well as teaching the health benefits ofwalking. They also reduce traffic c<strong>on</strong>gesti<strong>on</strong> and polluti<strong>on</strong>,particularly near schools (126). Although this measurehas been implemented in a number of developed anddeveloping countries, with clear health and social benefits(127), its effectiveness in reducing the incidence of <strong>child</strong>traffic injuries has yet to be calculated.Some schools in high-income countries have engageda “school travel coordinator”, who advises teachersand parents <strong>on</strong> the safest routes to school. However,42 WORLD REPORT ON CHILD INJURY PREVENTION
a randomized c<strong>on</strong>trol trial c<strong>on</strong>ducted in the UnitedKingdom failed to show that the preparati<strong>on</strong> of schooltravel plans had an effect <strong>on</strong> how <strong>child</strong>ren travelled toschool (128).Many countries have introduced school safety z<strong>on</strong>es,that include car-free areas, speed reducti<strong>on</strong> measures andadult supervisi<strong>on</strong> to cross the road safely. In Thailand,for example, the areas around schools have beencomprehensively improved and educati<strong>on</strong>al programmesintroduced <strong>on</strong> safe routes to school. In Bangalore, India,the focus has been <strong>on</strong> better public transport, makingvehicles park or stop at a given distance from the school,dedicated school buses and pedestrian crossings nearselected schools, sometimes overseen by traffic wardens(129).Separati<strong>on</strong> of two-wheelersChild cyclists need to be separated physically, by barriersor kerbs, or else by the demarcati<strong>on</strong> of white lines, fromother road users (130). In Denmark and the Netherlands,where there are large numbers of cyclists, bicycles are afeasible means of <strong>child</strong> transport if safety c<strong>on</strong>cerns areproperly addressed. A meta-analysis of the effects of cyclelanes found an estimated 4% reducti<strong>on</strong> in the incidence ofinjuries (122).Exclusive motorcycle lanes, separated from the maincarriageway by a raised central reservati<strong>on</strong>, have beenshown to reduce the likelihood of crashes. In Malaysia,where there are large numbers of young motorcyclists,reducti<strong>on</strong>s in crash rates of 27% have been recorded sincemotorcycles were separated from the rest of the traffic(131).Vehicle designVehicle design and standards c<strong>on</strong>tribute to the safety of<strong>child</strong>ren both inside and outside the vehicle. Primary safetymeasures for vehicles – to prevent a crash – such as brakingand lighting systems, improve road safety in general butare not specifically designed for <strong>child</strong>ren. Some sec<strong>on</strong>darysafety measures, though, are <strong>child</strong>-specific. They may beeither active or passive.Modern vehicles are designed with energy-absorbingcrumple z<strong>on</strong>es and side impact bars to limit the extentto which the vehicle will intrude into the passengercompartment in the event of a collisi<strong>on</strong>, thus reducingpotential injuries to <strong>child</strong>ren (1).Redesigning car fr<strong>on</strong>ts has the potential to reduce injuriesto pedestrians, and to <strong>child</strong>ren in particular, as they arevulnerable to head injuries <strong>on</strong> impact (1). The New CarAssessment Programmes in Europe, the United Statesand Australia include ratings for pedestrian protecti<strong>on</strong>,but most vehicles still obtain low scores. A new EuropeanDirective will, by 2010, require new car models to passa crash test incorporating protecti<strong>on</strong> requirements forpedestrians.Motor manufacturers should help protect <strong>child</strong>renin vehicles by providing suitable facilities to fit <strong>child</strong>restraints. Vehicles with these improved designs willresult in <strong>child</strong>ren being less likely to strike the car’sinterior in case of an impact (132).Children are at risk when vehicles are reversing. Thedevelopment of better visibility aids, such as cameras,and use of audible alarms and reversing lights can allhelp prevent injuries caused in this way (107).Alcohol interlock systems are beginning to be usedin some countries. They require a driver to blow intoa device before starting the car. The igniti<strong>on</strong> will notfuncti<strong>on</strong> if alcohol is present. Such devices have led toreducti<strong>on</strong>s of between 40% and 95% in the rate of repeatoffending under drink-driving laws (1). The devicesare therefore valuable for adolescents who drink anddrive.Safety equipmentChild restraint systemsAppropriate <strong>child</strong> restraint systems are designed to takeaccount of the <strong>child</strong>’s developmental stage. Like seat-belts,they work to secure the <strong>child</strong> to the vehicle in a way that,in the event of a crash, distributes forces over a broad bodyarea, thus reducing the chance of a severe <strong>injury</strong> occurring.Three types of restraint systems for <strong>child</strong> passengers areused:– rear-facing restraints for infants;– forward-facing <strong>child</strong> restraints;– booster cushi<strong>on</strong>s or booster seats, for older <strong>child</strong>ren.These systems take into account a <strong>child</strong>’s physicaldimensi<strong>on</strong>s and proporti<strong>on</strong>s.Child restraint systems are very effective at preventingfatalities, and are the most important “in-vehicle” safetymeasure for <strong>child</strong>ren. In the event of a crash, if restraintsystems are properly installed and used, they can:– reduce deaths am<strong>on</strong>g infants by around 70% (133);– reduce deaths am<strong>on</strong>g small <strong>child</strong>ren, aged 1–4 years, by54% (133);– reduce the chances of sustaining clinically significantinjuries by 59% am<strong>on</strong>g <strong>child</strong>ren aged 4–7 years whoare strapped in booster seats, as compared to the rateof injuries sustained using ordinary vehicle seat-belts(134).Despite the overwhelming evidence of theireffectiveness, though, many <strong>child</strong>ren are not restrained inage-appropriate <strong>child</strong> or booster seats.In many high-income countries the use of <strong>child</strong>restraints is comm<strong>on</strong>, with usage rates as high as 90%.Elsewhere, though, <strong>child</strong> restraints are still rarely used.Choosing and installing the appropriate <strong>child</strong> restraintsystem is important. Even in countries where the useof <strong>child</strong> restraints is comm<strong>on</strong> – such as in Sweden, theWORLD REPORT ON CHILD INJURY PREVENTION 43
United Kingdom and the United States – restraints arefrequently used inappropriately. A <strong>child</strong> may, for instance,be restrained in a device that is wr<strong>on</strong>g for its age or weight,or the straps or harnesses may be inadequately secured ormay be left entirely und<strong>on</strong>e. In all these situati<strong>on</strong>s, the<strong>child</strong> is placed at increased risk of both fatal and n<strong>on</strong>-fatalinjuries (133, 134).In many places, the use of <strong>child</strong> restraints may be limitedby access or cost, or else may not be practical because ofthe many <strong>child</strong>ren in the family. In additi<strong>on</strong>, parents needto be aware of what type of seat to choose, where to place itand how to install it. Research in Greece found that 88.4%of parents placed their <strong>child</strong>ren unrestrained <strong>on</strong> the backseat, while 76.1% of those who used a restraint did not doso c<strong>on</strong>sistently (135).A number of measures have been shown to increase theuse of <strong>child</strong> restraints.Mandatory laws <strong>on</strong> <strong>child</strong> restraint use and theirenforcement can lead to reducti<strong>on</strong>s in the rate of severeor fatal crash injuries.Public awareness can be raised through publicitycampaigns emphasizing the need for appropriaterestraints for <strong>child</strong>ren of different ages (136). Suchcampaigns are most effective when backed up byenforcement.Appropriate restraints can be subsidized or distributedfree to families. Loan schemes have been used in somecountries, thus increasing both the accessibility andaffordability of appropriate restraint systems (137,138).A rear-facing <strong>child</strong> safety seat should never be placedin fr<strong>on</strong>t of an airbag (139). Recent research suggests that<strong>child</strong>ren whose restraints are placed in the centre rearseating positi<strong>on</strong> incur less injuries than those placed <strong>on</strong>the outer seats, though this c<strong>on</strong>tradicts earlier studies thatfound that the centre seat was a less safe positi<strong>on</strong> (140, 141).Although <strong>child</strong>ren are best protected when secured in ageappropriate<strong>child</strong> restraints, where such restraints are notavailable it is still better to use an adult seat-belt <strong>on</strong> the<strong>child</strong> than to leave the <strong>child</strong> wholly unrestrained <strong>on</strong> theback seat (142, 143).Seat-beltsFor <strong>child</strong>ren over the age of 10 years, or above 150 cmin height, normal seat-belts should be used. Like <strong>child</strong>restraints, they serve to keep the <strong>child</strong> away from thevehicle structure in the event of a crash, prevent ejecti<strong>on</strong>from the vehicle, and distribute the forces of the crash overthe str<strong>on</strong>gest parts of the body.Wearing a seat-belt reduces the risk of being ejectedfrom a vehicle and suffering serious or fatal <strong>injury</strong> bybetween 40% and 65% (144). However, rates of seat-belt usevary widely between countries, in large part as a result ofthe differing enforcement of seat-belt laws (1). In general,though, seat-belt use am<strong>on</strong>g adolescent passengers anddrivers is noticeably less than am<strong>on</strong>g older occupants(29).As with <strong>child</strong> restraints, seat-belt use can be improvedthrough:– introducing and enforcing a law mandating seat-beltuse;– requiring all vehicles to be fitted with appropriate seatbelts;– c<strong>on</strong>ducting public awareness campaigns <strong>on</strong> seat-belts,targeted at young people.Such measures can increase awareness about the benefitsof wearing seat-belts and help make seat-belt use a socialnorm am<strong>on</strong>g young people.Bicycle helmetsA <strong>child</strong>’s brain is particularly vulnerable to <strong>injury</strong>.Approximately two thirds of hospital admissi<strong>on</strong>s am<strong>on</strong>gcyclists are for head injuries, and three quarters of deathsam<strong>on</strong>g injured cyclists are from head injuries (64).Helmets for cyclists afford protecti<strong>on</strong> from head <strong>injury</strong>in both traffic crashes and falls. The str<strong>on</strong>gest evidencefor the effectiveness of helmets comes from case-c<strong>on</strong>trolstudies. A systematic review of five such studies foundthat helmets reduced the risk of head and severe brain<strong>injury</strong> by between 63% and 88%, am<strong>on</strong>g cyclists of all ages(64). The use of cycle helmets is particularly importantfor older <strong>child</strong>ren because of their increased exposure totraffic. Helmets should be designed to match the age ofthe <strong>child</strong>, and when purchasing helmets parents shouldensure that they are the appropriate size and fit the <strong>child</strong>’shead.A number of measures have been shown to increase theuse of cycle helmets am<strong>on</strong>g <strong>child</strong>ren, including:– laws <strong>on</strong> bicycle helmet use and their enforcement;– the promoti<strong>on</strong> of bicycle helmets am<strong>on</strong>g <strong>child</strong>ren;– public awareness campaigns.Although the questi<strong>on</strong> of bicycle helmet use as itrelates to adult use has been c<strong>on</strong>troversial (26), promotinghelmet use am<strong>on</strong>g <strong>child</strong>ren, whose basic motor skillsare still developing, is more generally accepted. In theNetherlands, for instance, the road envir<strong>on</strong>ment has beenmodified to make it very safe for cycling. Although thereis no law <strong>on</strong> bicycle helmet use, Dutch crash data showthat <strong>child</strong>ren in the 4–8-year age group are particularlylikely to be involved in bicycle crashes and suffer headinjuries, and thus helmet use am<strong>on</strong>g <strong>child</strong>ren is str<strong>on</strong>glypromoted (145). While some countries, such as Australiaand the United States, have introduced and enforcemandatory bicycle helmet laws for all cyclists, others havelaws stipulating an age below which <strong>child</strong>ren must wearhelmets (27). Data from before and after such laws werepassed show an increase in helmet use – suggesting thatreducti<strong>on</strong>s in head <strong>injury</strong> rates can be achieved throughthis strategy (27).44 WORLD REPORT ON CHILD INJURY PREVENTION
Motorcycle helmetsIn most high-income countries young <strong>child</strong>ren are rarelyseen <strong>on</strong> the backs of motorcycles. However, in many places,especially in parts of South-East Asia, <strong>child</strong>ren are routinelytransported as passengers <strong>on</strong> motorized two-wheelers. It istherefore important to protect these <strong>child</strong>ren by ensuringthat they wear appropriate helmets (Box 2.3).Helmets, as already stated, reduce the risk of serioushead and brain injuries by lessening the impact of a forceto the head. Wearing a helmet is the single most effectiveway of preventing head injuries and fatalities resultingfrom motorcycle crashes (26).Wearing a helmet <strong>on</strong> a motorcycle (70):– decreases the risk and severity of injuries by about72%;– decreases the likelihood of death by up to 39%, with theprobability depending <strong>on</strong> the speed of the motorcycleinvolved;– decreases the health-care costs associated with crashes.A number of factors work against the wearing ofhelmets am<strong>on</strong>g <strong>child</strong> motorcycle passengers, includingthe following.Passengers <strong>on</strong> motorcycles may be exempt frommandatory helmet wearing laws or exempt from fines.Standard <strong>child</strong> helmets may not be available.The cost of purchasing <strong>child</strong> helmets may be prohibitive.Studies have shown that in some low-income countries,to afford a motorcycle helmet, factory workers have towork 11 times l<strong>on</strong>ger than their counterparts in highincomecountries (146).Risk-taking behaviours am<strong>on</strong>g adolescent motorcycleriders may result in their not wearing helmets. In a studyin Brazil, those under 18 years were significantly lesslikely than older people to wear a helmet, particularlyif they had been c<strong>on</strong>suming alcohol (147).C<strong>on</strong>spicuityC<strong>on</strong>spicuity is the ability of a road user to be seen byother road users. Vulnerable road users are at increasedrisk for road traffic injuries if they are not seen in timefor the other road users to take evasive acti<strong>on</strong> and avoid acollisi<strong>on</strong>. Children, whose small stature means that theyare less likely to be seen by motorists, are at even greaterrisk of not being seen.Improving the visibility of n<strong>on</strong>-motorized road users is<strong>on</strong>e way to reduce the risk of a road traffic crash, as it givesdrivers more time to notice and avoid a collisi<strong>on</strong>. Interventi<strong>on</strong>sto increase c<strong>on</strong>spicuity include the following.Retro-reflective clothing or strips <strong>on</strong> backpackscan increase the visibility of both pedestrians andBOX 2.3Getting helmets <strong>on</strong> <strong>child</strong>ren’s heads: the experience of Viet NamSince 1999, the Asia Injury Preventi<strong>on</strong> Foundati<strong>on</strong> in Hanoi has worked hard to get more people <strong>on</strong> motorcycles in Viet Nam to wear helmets and bydoing so cut the rate of road traffic injuries am<strong>on</strong>g <strong>child</strong>ren. It has staged public awareness campaigns, lobbied the government, helped develophelmet standards for both adults and <strong>child</strong>ren, distributed <strong>child</strong> helmets al<strong>on</strong>g with informati<strong>on</strong> <strong>on</strong> their use, and pushed to increase the producti<strong>on</strong>of helmets.At the end of 2007, the Vietnamese government passed a law making helmet wearing compulsory for drivers and passengers <strong>on</strong> motorcycles.Following its introducti<strong>on</strong>, rates of helmet use soared to over 90%. At the same time, hospitals began <str<strong>on</strong>g>report</str<strong>on</strong>g>ing reducti<strong>on</strong>s in the number of deathsand brain injuries resulting from motorcycle crashes.So<strong>on</strong>, however, certain problems arose. It was pointed out that although helmets for <strong>child</strong>ren under 14 years were required by the new law, therewas no provisi<strong>on</strong> to fine motorcycle drivers carrying <strong>child</strong>ren who were not wearing helmets. Furthermore, some doctors publicly questi<strong>on</strong>ed whetherhelmets might have an adverse effect <strong>on</strong> the development of a <strong>child</strong>’s skull, suggesting that the weight of a helmet could lead to serious neck injuriesam<strong>on</strong>g <strong>child</strong>ren involved in collisi<strong>on</strong>s. As a result, parents wereless enthusiastic about putting helmets <strong>on</strong> their <strong>child</strong>ren’s heads.While the proporti<strong>on</strong> of adult motorcyclists using helmets remainedat over 90%, helmet use am<strong>on</strong>g <strong>child</strong>ren under the age of 7 yearsfell to between 10% and 25% in the large cities. Most parents quotedthe risk of serious neck <strong>injury</strong> when asked why they avoided helmetsfor their <strong>child</strong>ren.An effort is currently being made to tackle this problem, with measuresincluding:– public educati<strong>on</strong> <strong>on</strong> the facts regarding <strong>child</strong>ren and helmet use,including publishing in newspapers assurances signed by internati<strong>on</strong>alexperts;– collaborati<strong>on</strong> with the government to remove the loophole in thelaw, whereby drivers were not penalized if their <strong>child</strong> passengerswere without a helmet;– further research <strong>on</strong> standards for <strong>child</strong> helmets.© AIPFWORLD REPORT ON CHILD INJURY PREVENTION 45
cyclists. Although this interventi<strong>on</strong> aids visibility, itsactual effectiveness in reducing injuries still needsto be evaluated (148). Some programmes using thistechnique, though, are beginning to show promise(149–151).Daytime running lights for motorcyclists have beenshown to be effective in reducing fatalities in countries,including Malaysia and Singapore, that have largenumbers of motorcycles (152, 153).The colour of the helmet seems to have an effect <strong>on</strong> thec<strong>on</strong>spicuity of motorcyclists. A case–c<strong>on</strong>trol study inNew Zealand found that retro-reflective or fluorescentclothing, white helmets and daytime running lightswere all effective in reducing crashes (154).Legislati<strong>on</strong> and standardsSetting and rigorously enforcing road safety regulati<strong>on</strong>smay prevent up to half of all deaths and serious injuries(155). As with all other road safety interventi<strong>on</strong>s, mostlaws which are designed to prevent crash injuries in thegeneral populati<strong>on</strong> will also help reduce the incidence of<strong>child</strong> road traffic injuries. Some laws, though, are specificto <strong>child</strong>ren and young people.Motor vehicle licensingIn most countries the minimum age for obtaining a licenceallowing unaccompanied driving is 18 years, though insome places the minimum age is as low as 16 years (1).Driver licensing systems exist to regulate the entry of newdrivers and to c<strong>on</strong>trol the c<strong>on</strong>diti<strong>on</strong>s under which theylearn to drive. These systems involve both a test <strong>on</strong> theoryand a practical driving test, usually c<strong>on</strong>ducted in normaltraffic during the day. The driving test is intended to ensurethat new drivers fulfil certain minimum performancestandards and to identify drivers who are unfit to drive(122).Novice drivers are over-represented in crash statistics.As a result, many countries have introduced graduateddriver licensing systems that place restricti<strong>on</strong>s <strong>on</strong> newdrivers, typically for the first two years of their driving(see Box 2.4). As well as restricting young drivers, thegraduated driver licensing system serves to increase theamount of accompanied driving time an adolescent has –something that has been shown to produce positive resultsin preventing crashes (53).Motorized two-wheeler licensingIn many countries <strong>child</strong>ren over 14 years of age areallowed to drive light mopeds with a maximum speedof 25 km/h, while more powerful mopeds, with amaximum speed of 45 km/h, and motorcycles are<strong>on</strong>ly permitted at 16 years. Raising the age limit forall powered two-wheelers from 16 to 18 years has beenfound to be effective in reducing the number of roadtraffic casualties (156, 157).Drink-driving lawsVarious methods have been adopted to restrict drinkingand driving am<strong>on</strong>g younger drivers, including thefollowing.Setting lower blood alcohol c<strong>on</strong>centrati<strong>on</strong> limits foryounger drivers. The risk of a crash for inexperiencedyoung adult drivers starts to rise at significantly lowerblood alcohol c<strong>on</strong>centrati<strong>on</strong> levels than is the case forolder drivers. For this reas<strong>on</strong>, many countries have seta lower blood alcohol c<strong>on</strong>centrati<strong>on</strong> limit – usuallybetween zero and 0.02 g/dl – for drivers under the ageof 21 years. These lower limits may cut the incidence ofcrashes am<strong>on</strong>g young or novice drivers by between 4%and 24% (158).Enforcing blood alcohol limits. C<strong>on</strong>sistent enforcementof blood alcohol c<strong>on</strong>centrati<strong>on</strong> limits is essential for thelaw to be effective. There are two basic ways in whichthis can be d<strong>on</strong>e.– Sobriety checks, or selective breath-testing. Inthese checks, drivers are stopped at checkpointsor roadblocks and <strong>on</strong>ly those suspected of beingover the alcohol limit are tested. This approach hasbeen shown to be effective in cutting the number ofalcohol-related crashes by about 20% (159).– Random breath-testing. This involves stoppingdrivers at random and breath-testing them.Australia, New Zealand and some Europeancountries use this strategy with excellent results(160). An Australian study has found randombreath-testing to be twice as effective as c<strong>on</strong>ductingsobriety checks at selective checkpoints (161).Raising the legal drinking age. Minimum drinkingagelaws specify an age below which the purchase orpublic c<strong>on</strong>sumpti<strong>on</strong> of alcoholic beverages is illegal.The laws may also include penalties for the possessi<strong>on</strong>or c<strong>on</strong>sumpti<strong>on</strong> of alcohol by those under that age.Evidence from the United States, where over the lastfew years every state has raised the legal drinking ageto 21 years, suggests that laws <strong>on</strong> the minimum legaldrinking age have reduced drinking, driving afterdrinking, and alcohol-related crashes and injuriesam<strong>on</strong>g young people (158, 162). However, in manyplaces, the enforcement of the law is very lax.Child restraintsMandatory <strong>child</strong> restraint laws and their enforcementlead to an increase in the use of <strong>child</strong> restraints, and somestudies show a corresp<strong>on</strong>ding reducti<strong>on</strong> in traffic-relateddeaths and injuries am<strong>on</strong>g <strong>child</strong>ren. In some countriesa penalty-point system is used to encourage people tocomply with the legislati<strong>on</strong>. In Latvia, the law <strong>on</strong> the useof <strong>child</strong> seats was revised in 2006 so that the penalty pointscould be incurred for failing to use a restraint.The effectiveness of such laws, though, will depend <strong>on</strong>how correctly <strong>child</strong> restraints are used. A study in Japan46 WORLD REPORT ON CHILD INJURY PREVENTION
BOX 2.4Graduated driver licensing programmesBeginner drivers of all ages lack skills in driving and in recognizing possible dangers, and are therefore at increased risk of a crash. In the case ofnewly-licensed adolescent drivers, their immaturity combined with limited driving experience can result in a disproporti<strong>on</strong>ately higher rate ofcrashes. Graduated licensing systems are schemes that allow for a c<strong>on</strong>trolled and supervised phasing-in of full driving licences for young novice drivers.The schemes protect beginners while they are learning, allowing them to obtain experience <strong>on</strong> the road under c<strong>on</strong>diti<strong>on</strong>s of low risk. Graduateddriver licensing is widely used in many high-income countries. Although the schemes vary between countries, most of them c<strong>on</strong>sist of a three-stagemodel.Stage 1: an extended period as a learner driver. The purpose of this stage is to increase the amount of supervised driving experience before receivinga full licence.Stage 2: a provisi<strong>on</strong>al or intermediate licence. Such a licence will c<strong>on</strong>tain temporary provisi<strong>on</strong>s, such as restricti<strong>on</strong>s <strong>on</strong> unsupervised driving, latenightdriving and driving with young passengers.Stage 3: a full licence.In many countries, progressing from <strong>on</strong>e stage to another requires a certain number of supervised driving hours. There may also be stipulati<strong>on</strong>sthat a proporti<strong>on</strong> of these hours should be c<strong>on</strong>ducted at night-time.The areas that graduated driver licensing schemes typically address include the following.Alcohol restricti<strong>on</strong>s. Permitted blood alcohol c<strong>on</strong>centrati<strong>on</strong>s limits range from zero in some countries to levels somewhat below the levels forexperienced drivers – for instance, 0.02 g/dl, against 0.05 g/dl for drivers with full licences.Passenger restricti<strong>on</strong>s. In the first phase, most graduated driver licensing systems do not allow passengers in the same vehicle. In the sec<strong>on</strong>d stage,passengers are usually allowed, but <strong>on</strong>ly if a parent or supervisor is present during the first three m<strong>on</strong>ths, after which <strong>on</strong>ly immediate family arepermitted as passengers.Seat-belt use. Almost all graduated driver licensing systems require that drivers and other occupants wear seat-belts.Speed. In some countries, drivers at the learning stage are prohibited from driving <strong>on</strong> any highway with a speed limit of over 80 km/h.Restricti<strong>on</strong>s <strong>on</strong> driving at night. Drivers in the first stage are prohibitedin some places from driving between midnight and 05:00.Mobile ph<strong>on</strong>e use. A number of countries have recently introduced restricti<strong>on</strong>s<strong>on</strong> mobile ph<strong>on</strong>e use, even with hands-free devices.Evaluati<strong>on</strong>s of graduated driver licensing systems have <str<strong>on</strong>g>report</str<strong>on</strong>g>edsignificant reducti<strong>on</strong>s in crashes and fatalities. Estimates of their effectivenesshave ranged from 4% to 60%, reflecting differences in thesystems, in the drivers’ ages and in the methodologies used in the evaluati<strong>on</strong>s(163, 164). Recent data from the United States have shown a23% reducti<strong>on</strong> over a decade in crashes am<strong>on</strong>g 16-year-olds, with greaterreducti<strong>on</strong>s for night-time driving and driving with occupants. Thesingle most effective provisi<strong>on</strong> within graduated driver licensing schemesappears to be the extensi<strong>on</strong> of Stage 1, the learner period, whichdelays unsupervised driving (165).© Utah Safety Counciltried to assess the impact <strong>on</strong> <strong>child</strong> injuries of laws mandatingthe use of <strong>child</strong> restraints. Despite overall increases inthe use of <strong>child</strong> restraints, overall rates of fatalities andserious injuries am<strong>on</strong>g <strong>child</strong>ren aged 1–5 years did notchange after the law was introduced, possibly because therestraints were not being used properly (166).HelmetsLegislati<strong>on</strong> and the enforcement of mandatory helmetuse for moped and motorcycle users is an effectiveinterventi<strong>on</strong> measure, particularly where accompaniedby public awareness campaigns. In countries where theselaws are enforced, helmet-wearing rates have been foundto increase to 90% or higher. In places where existinglaws have been repealed, wearing rates have fallen back togenerally under 60% (26). Standards for helmets shouldalso be enforced, including provisi<strong>on</strong>s for helmets for<strong>child</strong>ren. Some countries, such as Malaysia, have alreadyextended their standards to include helmets designedspecially for <strong>child</strong>ren (26, 152).Developing educati<strong>on</strong> and skillsEducati<strong>on</strong> can improve skills, behaviour and attitudes.A systematic review of safety educati<strong>on</strong> for pedestriansfound an improvement in behaviours and attitudes thatpredispose people to risk-taking, but n<strong>on</strong>e of the studiesreviewed actually recorded a reducti<strong>on</strong> in injuries(167). Follow-up l<strong>on</strong>gitudinal studies would be neededam<strong>on</strong>g those <strong>child</strong>ren whose attitudes were changed byeducati<strong>on</strong>al approaches to see if their risk of <strong>injury</strong> wasdiminished (168), though such a study would be l<strong>on</strong>g andexpensive.Traditi<strong>on</strong>ally, road safety educati<strong>on</strong> has been c<strong>on</strong>ductedin the classroom and has often involved an approachbased <strong>on</strong> teaching <strong>child</strong>ren the rules of the road. Whathas usually been absent in educati<strong>on</strong>al programmes is theWORLD REPORT ON CHILD INJURY PREVENTION 47
applicati<strong>on</strong> of modern ideas <strong>on</strong> educati<strong>on</strong>al and behaviourchange. Social scientists working in <strong>injury</strong> preventi<strong>on</strong> havein recent times taken an increasingly ecological approach,<strong>on</strong>e that involves the interacti<strong>on</strong> between the fields of <strong>child</strong>development, educati<strong>on</strong>al theory and behavioural theory(169).Younger <strong>child</strong>renCurrent research <strong>on</strong> road safety educati<strong>on</strong> suggeststhat an approach that stresses behaviour, focusing <strong>on</strong>the development of practical skills, is more likely tobe effective for younger <strong>child</strong>ren. Children learn bestthrough methods that develop problem-solving anddecisi<strong>on</strong>-making skills. Young <strong>child</strong>ren also learn byexample.In any case, educati<strong>on</strong> is an important ingredient of anycomprehensive effort to prevent <strong>injury</strong>. Some examples ofeffective educati<strong>on</strong>al approaches include the following.Roadside skills development for 6–8-year-olds. Suchprogrammes include the Kerbcraft pilot programmein the United Kingdom that teaches a number of basicskills, such as finding a safe place to cross, crossing safelynear parked vehicles, and crossing safely at juncti<strong>on</strong>s(170).Simulated envir<strong>on</strong>ments that teach pedestrian and cycleskills in a safe setting off the road. Examples include the“Safety City” programmes in New York City and PuertoRico, and traffic gardens in the Netherlands. Suchprogrammes need to be used as part of a progressiveprogramme, as they cannot address real interacti<strong>on</strong>swith traffic.Basic cycle skills can be taught both <strong>on</strong> and off theroad. The Oreg<strong>on</strong> bicycle educati<strong>on</strong> curriculum has tenmodules, half of them c<strong>on</strong>ducted <strong>on</strong> the road. Whileskills are developed, evidence as regards the extent of<strong>injury</strong> preventi<strong>on</strong> is lacking (171).C<strong>on</strong>spicuity is covered in many pedestrian educati<strong>on</strong>alprogrammes. In Norway, <strong>child</strong>ren receive caps, vestsor bags in bright colours with retro-reflective materialsto make them more visible, especially <strong>on</strong> dark winterevenings. In South Africa, the Drive Alive PedestrianVisibility Campaign that does public educati<strong>on</strong> workhas campaigned for laws to make it compulsory for allschool uniforms to c<strong>on</strong>tain retro-reflective material, soas to increase the visibility of <strong>child</strong> pedestrians (149).AdolescentsBy the time <strong>child</strong>ren reach adolescence they should havemastered the skills needed to act safely as pedestriansand cyclists, though some choose to engage in risk-takingbehaviour. This is a difficult age group to reach througheducati<strong>on</strong>al approaches and some methods may even becounterproductive. Greater involvement of adolescentsin designing programme may be helpful (172), as maythe use of televisi<strong>on</strong> programmes, such as “Soul City”(173, 174), theatrical presentati<strong>on</strong>s, games and peereducati<strong>on</strong>.Young driversThe c<strong>on</strong>troversy over the effectiveness of school-baseddriver educati<strong>on</strong> has a l<strong>on</strong>g history (139). Both therandomized c<strong>on</strong>trolled trials c<strong>on</strong>ducted in 1999 (175)and those d<strong>on</strong>e by the Cochrane Injuries Group in2001 (176) found that driver educati<strong>on</strong> did not reducethe number of traffic crashes or violati<strong>on</strong>s am<strong>on</strong>gstudents. On the c<strong>on</strong>trary, driver educati<strong>on</strong> programmescan lead to earlier driving by novices, resulting inmore crashes (139) offsetting any benefits from drivereducati<strong>on</strong> programmes. A more recent randomized trialof the effectiveness of post-licence driver educati<strong>on</strong> inpreventing road traffic crashes has also found no evidenceof effectiveness (177).Emergency and trauma careMost initiatives for cutting the incidence of road trafficinjuries focus <strong>on</strong> preventing crashes and <strong>on</strong> restricting theextent of their c<strong>on</strong>sequences. Much, though, can be d<strong>on</strong>eto reduce the number of deaths and injuries from roadtraffic crashes by strengthening the emergency medicalservices – including pre-hospital care, hospital care andrehabilitati<strong>on</strong>.Pre-hospital careAt the scene of the crash, prompt, efficient and effectivepre-hospital care can save many lives. In places whereformal emergency medical services exist, usually withambulances, they are most effective if their equipment,training, infrastructure and operati<strong>on</strong>s are standardized.These emergency vehicles need to be equipped withsupplies and medical devices for <strong>child</strong>ren as well as foradults – such as airway tubes, cervical collars and bloodpressure cuffs. Staff need to be trained <strong>on</strong> how to evaluateand manage injured <strong>child</strong>ren, and to recognize that what isnormal in an adult may not necessarily be normal in a <strong>child</strong>.Where no pre-hospital trauma care system exists, the firstand fundamental tier of the system should be establishedby teaching interested volunteers the basic techniques offirst aid (178). In many countries, organizati<strong>on</strong>s such as theInternati<strong>on</strong>al Federati<strong>on</strong> of Red Cross and Red CrescentSocieties, and the St John’s Ambulance teach young peoplehow to recognize an emergency, call for help and providebasic first aid until formally-trained health-care pers<strong>on</strong>nelarrive.Setting up a new emergency medical service may be avaluable step, especially al<strong>on</strong>g busy roads with high crashrates. These services, though, can be costly. In all cases, andespecially where there are no formal emergency medicalservices, pre-hospital care can be improved by buildingup<strong>on</strong> existing – even if informal – systems of pre-hospitalcare and transport (178).48 WORLD REPORT ON CHILD INJURY PREVENTION
Trauma careEntry into the hospital is the sec<strong>on</strong>d stage at which thelife of an injured <strong>child</strong> can be saved (179). Improving theorganizati<strong>on</strong> of trauma care services is an affordable andsustainable way of raising the quality and outcome of care.This involves improving the human resources that arerequired to provide care – including skills, training andstaffing – and the physical resources, including equipmentand supplies. The essential elements of trauma care neednot be expensive, though the cost of care is often a barrierto access, especially where user fees are required in advanceof services in emergency situati<strong>on</strong>s.Rehabilitati<strong>on</strong>Many injured survivors of traffic crashes lead livesof disability. Much of this disability, particularlyam<strong>on</strong>g young people, could be avoided with improvedrehabilitati<strong>on</strong> services. This includes improved services inhealth-care facilities and improved access to communitybasedrehabilitati<strong>on</strong>. Such rehabilitati<strong>on</strong> services need tobe strengthened everywhere, so as to reduce the prevalenceof disability after <strong>injury</strong> and to help those with persistentdisabilities to lead full and meaningful lives.Potentially harmful interventi<strong>on</strong>sAirbags deployed in the event of a sudden decelerati<strong>on</strong> aredesigned to supplement, and not to replace, the protecti<strong>on</strong>provided by a seat-belt. Although they have provenbenefits for adults, airbags pose serious risks for <strong>child</strong>ren.Available data indicate that, <strong>on</strong> average, <strong>child</strong>ren underthe age of 13 years are more likely to be harmed by anairbag than to be helped by it. Children should not sit inthe fr<strong>on</strong>t passenger seat of cars with airbags unless thereis absolutely no alternative or unless the airbag has beendeactivated (180). In most high-income countries, parentsare warned about the danger of airbags to <strong>child</strong>ren andadvised <strong>on</strong> the correct seating positi<strong>on</strong>s to be used invehicles where airbags have been fitted. A rear-facing <strong>child</strong>safety seat should never be placed in fr<strong>on</strong>t of an airbag(139). Current research is focusing <strong>on</strong> new technologicalsoluti<strong>on</strong>s that will detect the presence of a <strong>child</strong> and adjustthe deployment of the airbag or deactivate it. Newer airbagdesigns have cut the number of injuries to <strong>child</strong>ren, withoutwholly eliminating such injuries, but have provided noadditi<strong>on</strong>al benefit to adults (181).Evaluating interventi<strong>on</strong>sThere is no single blueprint for road safety. Many of theinterventi<strong>on</strong>s discussed in this chapter have been evaluated<strong>on</strong>ly in high-income countries. It is quite possible that theywill also work in low-income or middle-income countries,but their feasibility, acceptability and effectiveness in thesecountries have yet to be tested. While some countries havebegun to implement and evaluate road safety interventi<strong>on</strong>sin general, few countries have evaluated <strong>child</strong>-specific roadsafety interventi<strong>on</strong>s and fewer still have looked at theircost-effectiveness. More evaluati<strong>on</strong> studies are needed,so as to obtain compelling evidence that will persuadepolicy-makers to prioritize road traffic <strong>injury</strong> preventi<strong>on</strong>,particularly as it affects <strong>child</strong>ren.C<strong>on</strong>clusi<strong>on</strong>s and recommendati<strong>on</strong>sAround 10 milli<strong>on</strong> <strong>child</strong>ren annually are estimated tobe injured or disabled as a result of road traffic injuries.Road traffic injuries are the leading cause of death in<strong>child</strong>ren aged 10–19 years, and are also the leading causeof disability am<strong>on</strong>g <strong>child</strong>ren generally. Over the next 15years, significant increases in road traffic casualties arepredicted, particularly in low-income and middle-incomecountries. In India and China in particular, in that period,the annual incidence of road traffic fatalities is expected toat least double.The road envir<strong>on</strong>ment is c<strong>on</strong>structed in most caseswithout c<strong>on</strong>siderati<strong>on</strong> for <strong>child</strong>ren. Children <strong>on</strong> the roadare therefore at greater risk than they need have been.Rises in motorizati<strong>on</strong> and urbanizati<strong>on</strong> are both fuellingroad traffic tolls in many countries.A <strong>child</strong> is more susceptible to road traffic injuriesbecause of a smaller height and other less developedphysical characteristics, including sensory facilities.Young <strong>child</strong>ren may unknowingly take risks <strong>on</strong> the roadbecause they lack appropriate skills to act safely. Older<strong>child</strong>ren and adolescents may actively indulge in risktakingbehaviours, that are exacerbated by peer pressure.Children from poorer backgrounds are generally at greaterrisk of road traffic <strong>injury</strong>.Recommendati<strong>on</strong>sTraditi<strong>on</strong>ally, road safety measures for <strong>child</strong>ren havefocused largely <strong>on</strong> road safety educati<strong>on</strong> – with theassumpti<strong>on</strong> that <strong>child</strong>ren must be taught how to adapttheir behaviour to the demands of a motorized society.However, when used in isolati<strong>on</strong>, without c<strong>on</strong>sideringthe safety of vehicles and road envir<strong>on</strong>ments, educati<strong>on</strong>almeasures do not deliver tangible and sustained reducti<strong>on</strong>sin deaths and serious injuries.The systems approach has proved valuable in deliveringgreater road safety for <strong>child</strong>ren. It moves away from theidea that <strong>child</strong>ren should adapt their behaviour to copewith traffic, in favour of an approach in which <strong>child</strong>ren’sneeds are addressed in the design and management of thewhole road system.Large gains can be made in terms of injuries avoided andlives saved if proven and effective strategies – increasinglyused in high-income countries – are adapted to the c<strong>on</strong>textof low-income and middle-income countries where<strong>child</strong>ren are at c<strong>on</strong>siderably higher risk (see Table 2.3). Inline with the systems approach, the following acti<strong>on</strong>s arerecommended to reduce the toll of <strong>child</strong> road traffic <strong>injury</strong>,death and disability.WORLD REPORT ON CHILD INJURY PREVENTION 49
TABLE 2.3Key strategies to prevent road traffic injuries am<strong>on</strong>g <strong>child</strong>renStrategyEffectivePromisingInsufficientevidenceIneffectiveHarmfulIntroducing (and enforcing) minimum drinking-age lawsSetting (and enforcing) lower blood alcohol c<strong>on</strong>centrati<strong>on</strong> limits for novice driversand zero tolerance for offendersUtilizing appropriate <strong>child</strong> restraints and seat-beltsWearing motorcycle and bicycle helmetsForcing a reducti<strong>on</strong> of speed around schools, residential areas, play areasSeparating different types of road userIntroducing (and enforcing) daytime running lights for motorcyclesIntroducing graduated driver licensing systemsImplementing designated driver programmesIncreasing the visibility of pedestriansIntroducing instructi<strong>on</strong> in schools <strong>on</strong> the dangers of drink-drivingC<strong>on</strong>ducting school-based driver educati<strong>on</strong>Putting babies or <strong>child</strong>ren <strong>on</strong> a seat with an air bagLicensing novice teenage driversSource: references 1 and 139.Reducing speed. Survival rates for pedestrians andcyclists are much higher at collisi<strong>on</strong> speeds of below30 km/h. This speed should be the norm in residentialareas, around schools and other play areas.Separati<strong>on</strong> of two-wheelers. Child cyclists shouldbe separated physically from other road users – forinstance, by using dedicated cycle lanes. Exclusivemotorcycle lanes, separated from the main stream ofroad traffic by a raised central reservati<strong>on</strong>, have beenshown to reduce motorcycle casualties and should bec<strong>on</strong>sidered.Vehicle modificati<strong>on</strong>s. Several modificati<strong>on</strong>s are alreadybeing introduced in many high-income countries.This process needs to be accelerated in high-incomecountries, and c<strong>on</strong>sidered, where resources allow, inmiddle-income and low-income countries.Child restraint systems should always be used incars. These include: rear-facing restraints for infants;forward-facing <strong>child</strong> restraints; and booster cushi<strong>on</strong>sor booster seats, for older <strong>child</strong>ren.Seat-belts. For <strong>child</strong>ren over the age of 10 years, or above150 cm in height, normal seat-belts should be used.Bicycle helmets. Appropriate helmets always shouldalways be worn by <strong>child</strong>ren cycling <strong>on</strong> the roads astheir heads are even more susceptible to <strong>injury</strong> thanadults.Motorcycle helmets. Wearing a helmet is the single mosteffective way of preventing head injuries and fatalitiesresulting from motorcycle crashes. All drivers andpassengers <strong>on</strong> motorcycles, irrespective of their ages,should wear approved helmets, appropriate for theirhead size and in a c<strong>on</strong>spicuous colour.Drink-driving laws. Strict laws <strong>on</strong> drink-driving shouldbe introduced and enforced. Methods include:– setting lower blood alcohol c<strong>on</strong>centrati<strong>on</strong> limits foryoung drivers;– undertaking sobriety checks, or selective breathtesting;– undertaking random breath-testing;– raising the legal drinking age.Daytime running lights for motorcyclists have been shownto be effective in reducing fatalities in several countries,and should be c<strong>on</strong>sidered as a preventive measure.Novice drivers. Countries should c<strong>on</strong>sider introducinggraduated driver licensing systems that place restricti<strong>on</strong>s<strong>on</strong> new drivers, for the initial period (possiblytwo years) of their driving.Teaching knowledge and skills. For younger <strong>child</strong>renin particular, educati<strong>on</strong> is an important ingredient ofany comprehensive effort to prevent <strong>injury</strong>. Measuresinclude:– roadside skills development for 6–8-year-olds;50 WORLD REPORT ON CHILD INJURY PREVENTION
– simulated envir<strong>on</strong>ments that teach pedestrian andcycle skills in a safe setting off the road;– basic cycle skills, taught both <strong>on</strong> and off the road.In additi<strong>on</strong> to the various primary preventi<strong>on</strong> measuresrecommended above, emergency medical care – both prehospitaland hospital care – as well as rehabilitati<strong>on</strong> servicesshould be improved and equipped with the <strong>child</strong> in mind.Furthermore, emergency health-care staff should be trained<strong>on</strong> how to evaluate and manage injured <strong>child</strong>ren.References1. Peden M et al., eds. <str<strong>on</strong>g>World</str<strong>on</strong>g> <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> road traffic <strong>injury</strong>preventi<strong>on</strong>. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2004(http://www.who.int/violence_<strong>injury</strong>_preven-ti<strong>on</strong>/publicati<strong>on</strong>s/road_traffic/world_<str<strong>on</strong>g>report</str<strong>on</strong>g>/en/index.html,accessed 22 January 2008).2. Ec<strong>on</strong>omic Commissi<strong>on</strong> for Europe. Glossary of transportstatistics, 3rd ed. New York, NY, United Nati<strong>on</strong>s Ec<strong>on</strong>omicand Social Council, 2003 (TRANS/WP.6/2003/6) (http://www.unece.org/trans/main/wp6/pdfdocs/glossen3.pdf,accessed 23 February 2008).3. <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Statistics 2008. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> HealthOrganizati<strong>on</strong>, 2008 (http://www.who.int/whosis/whostat/2008/en/index.htm, accessed 20 June 2008).4. Mathers C, L<strong>on</strong>car D. Updated projecti<strong>on</strong>s of global mortalityand burden of disease, 2002–2030: data sources, methodsand results. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2005.5. Kopits E, Cropper M. Traffic fatalities and income growth.Accident Analysis and Preventi<strong>on</strong>, 2005, 37:169–178.6. Vincenten J, Michalsen A. Priorities for <strong>child</strong> safety in theEuropean Uni<strong>on</strong>: agenda for acti<strong>on</strong>. Injury C<strong>on</strong>trol andSafety Promoti<strong>on</strong>, 2003, 9:1–8.7. WHO mortality database: tables. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g>Health Organizati<strong>on</strong> (http://www.who.int/healthinfo/morttables/en/index.html, accessed 21 April 2008).8. Rahman A et al. Bangladesh health and <strong>injury</strong> survey:<str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> <strong>child</strong>ren. Dhaka, Ministry of Health and FamilyWelfare, 2005.9. Sitthi-amorn C et al. Child <strong>injury</strong> in Thailand: a <str<strong>on</strong>g>report</str<strong>on</strong>g><strong>on</strong> the nati<strong>on</strong>al <strong>injury</strong> survey. Bangkok, Institute ofHealth Research, TASC and UNICEF, 2006 (http://www.tasc-gcipf.org/downloads/Thai%20<strong>child</strong>%20<str<strong>on</strong>g>report</str<strong>on</strong>g>.pdf,accessed 22 January 2008).10. Bener A. The neglected epidemic: road traffic accidents ina developing country. State of Qatar. Internati<strong>on</strong>al Journalof Injury C<strong>on</strong>trol and Safety Promoti<strong>on</strong>, 2005, 12:45–47.11. Nizamo H et al. Mortality due to injuries in Maputo city,Mozambique. Internati<strong>on</strong>al Journal of Injury C<strong>on</strong>trol andSafety Promoti<strong>on</strong>, 2006, 13:1–6.12. Hyder AA, Labinjo M, Muzaffar SSF. A new challengeto <strong>child</strong> and adolescent survival in urban Africa: anincreasing burden of road traffic injuries. Traffic InjuryPreventi<strong>on</strong>, 2006, 7:381–388.13. Linnan M et al. Child mortality and <strong>injury</strong> in Asia: policyand programme implicati<strong>on</strong>s. Florence, UNICEF InnocentiResearch Centre, 2007 (http://www.unicef-irc.org/publicati<strong>on</strong>s/pdf/iwp_2007_07.pdf, accessed 21 January2008). (Innocenti Working Paper 2007-07, Special Series<strong>on</strong> Child Injury No. 4).14. Brown JK et al. Patterns of severe <strong>injury</strong> in pediatriccar crash victims: Crash Injury Research EngineeringNetwork database. Journal of Pediatric Surgery, 2006,41:362–367.15. Linnan M et al. Child mortality and <strong>injury</strong> in Asia:survey results and evidence. Florence, UNICEF InnocentiResearch Centre, 2007 (http://www.unicef-irc.org/publicati<strong>on</strong>s/pdf/iwp_2007_06.pdf, accessed 21 January2008). (Innocenti Working Paper 2007-06, Special Series<strong>on</strong> Child Injury No. 3).16. Gururaj G et al. Traumatic brain <strong>injury</strong>. Bangalore,Nati<strong>on</strong>al Institute of Mental Health and Neurosciences,2005 (Publicati<strong>on</strong> no. 61).17. Bryant B et al. Psychological c<strong>on</strong>sequences of road trafficaccidents for <strong>child</strong>ren and their mothers. PsychologicalMedicine, 2004, 4:335–346.18. Macphers<strong>on</strong> AK et al. Mechanism of <strong>injury</strong> affects 6-m<strong>on</strong>thfuncti<strong>on</strong>al outcome in <strong>child</strong>ren hospitalized because ofsevere injuries. Journal of Trauma: Injury, Infecti<strong>on</strong>, andCritical Care, 2003, 55:454–458.19. Blanchard E, Hickling EJ. After the crash: psychologicalassessment and treatment of survivors of motor vehicleaccidents, 2nd ed. Washingt<strong>on</strong>, DC, AmericanPsychological Associati<strong>on</strong>, 2004.20. Sleet DA et al. Injury and violence preventi<strong>on</strong> in thecommunity. In: Rozensky RH et al., eds. Psychology’s rolein public health. Washingt<strong>on</strong>, DC, American PsychologicalAssociati<strong>on</strong>, 2004:185–216.21. Di Gallo A. Verletzung v<strong>on</strong> Körper und Seele:psychiatrische Folgen v<strong>on</strong> Verkehrsunfällen bei Kindernund Jugendlichen [Injury to body and soul: psychiatricc<strong>on</strong>sequences of road traffic accidents in <strong>child</strong>ren andadolescents]. Schweizerische Rundschau für MedizinPraxis, 2005, 94:467−470.22. Schafer I et al. Posttraumatic syndromes in <strong>child</strong>ren andadolescents after road traffic accidents: a prospectivecohort study. Psychopathology, 2006, 39:159−164.23. Rusch MD et al. Psychological adjustment in <strong>child</strong>renafter traumatic disfiguring injuries: a 12-m<strong>on</strong>th followup.Journal of American Society of Plastic Surge<strong>on</strong>s, 2000,106:1451−1458.24. Verbal autopsy standards: ascertaining andattributing causes of death. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> HealthOrganizati<strong>on</strong>, 2007 (http://www.who.int/whosis/mort/verbalautopsystandards/en/index.html, accessed 23January 2008).25. Christie N et al. Children’s road traffic safety: an internati<strong>on</strong>alsurvey of policy and practice. L<strong>on</strong>d<strong>on</strong>, Department forTransport, 2004 (http://eprints.ucl.ac.uk/1211/1/2004_4.WORLD REPORT ON CHILD INJURY PREVENTION 51
pdf, accessed 22 January 2008) (Road Safety ResearchReport No. 47).26. Toroyan T, Peden M, eds. Youth and road safety. Geneva,<str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2007 (http://whqlibdoc.who.int/publicati<strong>on</strong>s/2007/9241595116_eng.pdf, accessed 22January 2008).27. Keeping <strong>child</strong>ren safe in traffic. Paris, Organisati<strong>on</strong> forEc<strong>on</strong>omic Co-operati<strong>on</strong> and Development, 2004.28. Li G, Baker SP. Injuries to bicyclists in Wuhan, People’sRepublic of China. American Journal of Public Health,1997, 87:1049–1052.29. Young Drivers: the road to safety. Paris, Organisati<strong>on</strong> forEc<strong>on</strong>omic Co-operati<strong>on</strong> and Development, 2006.30. Gregersen N, Nyberg A, Berg H. Accident involvementam<strong>on</strong>g learner drivers: an analysis of the c<strong>on</strong>sequencesof supervised practice. Accident Analysis and Preventi<strong>on</strong>,2003, 35:725–730.31. Palamara P, Legge M, Stevens<strong>on</strong> M. The relati<strong>on</strong>shipbetween years of licensing, traffic offences and crashinvolvement: implicati<strong>on</strong>s for driver licensing in WesternAustralia. In: Proceedings of the Developing Safer Driversand Riders C<strong>on</strong>ference, 21–23 July 2002, Brisbane. Brisbane,2002.32. Oesch SL. Statement before the Maryland House Committee<strong>on</strong> Envir<strong>on</strong>mental Matters. Passenger restricti<strong>on</strong>s for youngdrivers. Arlingt<strong>on</strong>, VA, Insurance Institute for HighwaySafety, 2005.33. Mohan D. Road safety in less-motorized envir<strong>on</strong>ments:future c<strong>on</strong>cerns. Internati<strong>on</strong>al Journal of Epidemiology,2002, 31:527–532.34. Cass DT, Ross F, Lam L. School bus-related deaths andinjuries in New South Wales. Medical Journal of Australia,1996, 165:134–137.35. Miller T, Spicer RS. How safe are our schools? AmericanJournal of Public Health, 1998, 88:413–418.36. Jacobs G, Thomas AA, Astrop A. Estimating global roadfatalities. Crowthorne, Transport Research Laboratory,2000 (TRL Report 445) (http://www.transport-links.org/transport_links/filearea/publicati<strong>on</strong>s/1_329_TRL445.pdf,accessed 22 January 2008).37. Aer<strong>on</strong>-Thomas AA et al. The involvement and impactof road crashes <strong>on</strong> the poor: Bangladesh and India casestudies. Crowthorne, Transport Research LaboratoryLimited, 2004 (http://www.grsproadsafety.org/themes/default/pdfs/The%20Poor_final%20final%20<str<strong>on</strong>g>report</str<strong>on</strong>g>.pdf,accessed 22 January 2008).38. Whitebread D, Neils<strong>on</strong> K. The c<strong>on</strong>tributi<strong>on</strong> of visualsearch strategies to the development of pedestrian skillsby 4–11 year-old <strong>child</strong>ren. British Journal of Educati<strong>on</strong>alPsychology, 2000, 70:539–557.39. Dunbar G, Hill R, Lewis V. Children’s attenti<strong>on</strong>al skillsand road behaviour. Journal of Experimental Psychology:Applied, 2001, 7:227–234.40. Siegler RS, Richards DD. The development of speed, time,and distance c<strong>on</strong>cepts. Developmental Psychology, 1979,15:288–298.41. Zeedyk MS, Wallace L, Spry L. Stop, look, listen, andthink? What young <strong>child</strong>ren really do when crossing theroad. Accident Analysis and Preventi<strong>on</strong>, 2002, 34:43–50.42. Pitcairn TK, Edlemann T. Individual differences in roadcrossing ability in young <strong>child</strong>ren and adults. BritishJournal of Psychology, 2000, 91:391–410.43. Ampofo-Boateng K, Thoms<strong>on</strong> JA. Children’s percepti<strong>on</strong>of safety and danger <strong>on</strong> the road. British Journal ofPsychology, 1991, 82:487–505.44. Kovács I et al. Late maturati<strong>on</strong> of visual spatial integrati<strong>on</strong>in humans. Proceedings of the Nati<strong>on</strong>al Academy of Sciencesof the United States of America, 1999, 96:12204–12209.45. Káldy Z, Kovács I. Visual c<strong>on</strong>text integrati<strong>on</strong> is not fullydeveloped in 4-year-old <strong>child</strong>ren. Percepti<strong>on</strong>, 2003, 2:657–666.46. Giedd J. Structural magnetic res<strong>on</strong>ance imaging of theadolescent brain. Annals of the New York Academy ofSciences, 2004, 1021:77–85.47. Arnett J. Developmental sources of crash risk in youngdrivers. Injury Preventi<strong>on</strong>, 2002, 8(Suppl II):ii17–ii23.48. Cross D, Hall M. Child pedestrian safety: the role ofbehavioural science [editorial]. The Medical Journal ofAustralia, 2005, 182:318–319.49. Bina M, Graziano F, B<strong>on</strong>ino S. Risky driving and lifestylesin adolescence. Accident Analysis and Preventi<strong>on</strong>, 2006,38:472–481.50. Stevens<strong>on</strong> M et al. Behavioural factors as predictors ofmotor vehicle crashes in young drivers. Journal of CrashPreventi<strong>on</strong> and Injury C<strong>on</strong>trol, 2001, 2:247–254.51. Waylen A, McKenna F. Cradle attitudes: grave c<strong>on</strong>sequences.The development of gender differences in risky attitudesand behaviour in road use. Basingstoke, AA Foundati<strong>on</strong>for Road Safety Research, 2002.52. Parker D et al. Determinants of intenti<strong>on</strong> to commitdriving violati<strong>on</strong>s. Accident Analysis and Preventi<strong>on</strong>,1992, 24:117–131.53. McKenna FP, Crick JL. Developments in hazard percepti<strong>on</strong>.Final <str<strong>on</strong>g>report</str<strong>on</strong>g>. L<strong>on</strong>d<strong>on</strong>, Department for Transport, 1994.54. Stevens<strong>on</strong> M, Jamrozik KD, Spittle JA. A case-c<strong>on</strong>trolstudy of traffic risk factors and <strong>child</strong> pedestrian <strong>injury</strong>.Internati<strong>on</strong>al Journal of Epidemiology, 1995, 24:957–964.55. Traffic safety facts. Child restraint use in 2007: overallresults. Washingt<strong>on</strong>, DC, Nati<strong>on</strong>al Highway Traffic SafetyAdministrati<strong>on</strong>, 2008.56. Survey. Salim and Salimah, Safe and Sound web site(http://www.salimandsalimah.org/survey.htm, accessed28 April 2008).57. Karwacki JJ Jr, Baker SP. Children in motor vehicles:never too young to die. Journal of the American MedicalAssociati<strong>on</strong>, 1979, 242:2848–2851.52 WORLD REPORT ON CHILD INJURY PREVENTION
58. Durbin D, Elliott M, Winst<strong>on</strong> F. Belt-positi<strong>on</strong>ing boosterseats and reducti<strong>on</strong> in risk of <strong>injury</strong> am<strong>on</strong>g <strong>child</strong>renin vehicle crashes. Journal of the American MedicalAssociati<strong>on</strong>, 2003, 289:2835–2840.59. American Academy of Pediatrics, Committee <strong>on</strong> Injuryand Pois<strong>on</strong> Preventi<strong>on</strong>. Selecting and using the mostappropriate car safety seats for growing <strong>child</strong>ren: guidelinesfor counseling parents. Pediatrics, 2002, 109:550–553.60. Everett SA et al. Trends and subgroup differences intransportati<strong>on</strong> related <strong>injury</strong> risk and safety behaviorsam<strong>on</strong>g high school students, 1991–1997. Journal ofAdolescent Health, 2001, 28:228–234.61. Shope JT. Influences <strong>on</strong> youthful driving behavior andtheir potential for guiding interventi<strong>on</strong>s to reduce crashes.Injury Preventi<strong>on</strong>, 2006, 12:i9–i14.62. Carlin JB, Taylor P, Nolan T. A case-c<strong>on</strong>trol study of <strong>child</strong>bicycle injuries: relati<strong>on</strong>ship of risk to exposure. AccidentAnalysis and Preventi<strong>on</strong>, 1995, 27:839–844.63. Traffic safety facts: bicyclists and other cyclists. Washingt<strong>on</strong>,DC, Nati<strong>on</strong>al Highway Traffic Safety Administrati<strong>on</strong>, 2006.64. Thomps<strong>on</strong> DC, Rivara FP, Thomps<strong>on</strong> R. Helmets forpreventing head and facial injuries in bicyclists. CochraneDatabase of Systematic Reviews, 2005, (4):CD001855.65. Senturia YD et al. Bicycle-riding circumstances andinjuries in school-aged <strong>child</strong>ren: a case-c<strong>on</strong>trol study.Archives of Pediatrics and Adolescent Medicine, 1997,151:485–489.66. Rivara FP, Thomps<strong>on</strong> DC, Thomps<strong>on</strong> RS. Epidemiologyof bicycle injuries and risk factors of serious <strong>injury</strong>. InjuryPreventi<strong>on</strong>, 1997, 3:110–114.67. Puranik S, L<strong>on</strong>g J, Coffman S. Profile of pediatric bicycleinjuries. South Medical Journal, 1998, 91:1033–1037.68. Shafi S et al. Impact of bicycle helmet safety legislati<strong>on</strong> <strong>on</strong><strong>child</strong>ren admitted to a regi<strong>on</strong>al pediatric trauma center.Journal of Pediatric Surgery, 1998, 33:317–321.69. Lin M-R et al. Factors associated with severity ofmotorcycle injuries and young adult riders. Annals ofEmergency Medicine, 2003, 41:783–791.70. Liu BC et al. Helmets for preventing <strong>injury</strong> in motorcycleriders. Cochrane Database of Systematic Reviews, 2007,(4):CD004333.71. Hung DV, Stevens<strong>on</strong> M, Ivers R. Barriers to, and factorsassociated with, observed motorcycle helmet use inVietnam. Accident Analysis and Preventi<strong>on</strong>, 2008,40:1627–1633.72. Chen L et al. Carrying passengers as a risk factor forcrashes fatal to 16– and 17–year old drivers. Journal of theAmerican Medical Associati<strong>on</strong>, 2000, 283:1578–1582.73. Williams AF. Teenage passengers in motor vehicle crashes:a summary of current research. Arlingt<strong>on</strong>, VA, InsuranceInstitute for Highway Safety, 2001.74. Huber JC, Carozza SE, Gorman DM. Underage driving asan indicator of risky behavior in <strong>child</strong>ren and adolescents.Journal of Adolescent Health, 2006, 38:612–616.75. Maycock G. Novice driver accidents and the driving test.Crowthorne, Transport Research Laboratory, 2002 (TRLReport 527).76. Fatality facts: teenagers 2005. Arlingt<strong>on</strong>, VA, InsuranceInstitute for Highway Safety, 2006 (www.iihs.org/research/fatality_facts/teenagers.html, accessed 13 May 2008).77. Mayhew DR, Simps<strong>on</strong> HM, Pak A. Changes in the collisi<strong>on</strong>rate am<strong>on</strong>g novice drivers during the first m<strong>on</strong>ths ofdriving. Accident Analysis and Preventi<strong>on</strong>, 2003, 35:683–691.78. Nati<strong>on</strong>al Research Council and Institute of Medicine. Astudy of interacti<strong>on</strong>s: emerging rapporteurs. Washingt<strong>on</strong>,DC, The Nati<strong>on</strong>al Academies Press, 2006.79. Keall M, Frith W, Patters<strong>on</strong> T. The influence of alcohol,age and number of passengers <strong>on</strong> the night-time risk ofdriver fatal <strong>injury</strong> in New Zealand. Accident Analysis andPreventi<strong>on</strong>, 2004, 36:49–61.80. McAnally K, Kypri K. Alcohol and road safety behaviouram<strong>on</strong>g New Zealand tertiary students. Internati<strong>on</strong>alJournal of Adolescent Medical Health, 2004, 16:229–237.81. Youth risk behavior surveillance: United States, 2005.Atlanta, GA, Nati<strong>on</strong>al Center for Chr<strong>on</strong>ic DiseasePreventi<strong>on</strong> and Health Promoti<strong>on</strong>, Centers for DiseaseC<strong>on</strong>trol and Preventi<strong>on</strong>, 2006 (http://apps.nccd.cdc.gov/yrbss/CategoryQuesti<strong>on</strong>s.asp?cat=1&desc=Unintenti<strong>on</strong>alInjuries and Violence, accessed 28 April 2008).82. Sim<strong>on</strong>s-Mort<strong>on</strong> B, Lerner N, Singer J. The observed effectsof teenage passengers <strong>on</strong> the risky driving behavior ofteenage drivers. Accident Analysis and Preventi<strong>on</strong>, 2005,37:973–982.83. Blows S et al. Risky driving habits and motor vehicledriver <strong>injury</strong>. Accident Analysis and Preventi<strong>on</strong>, 2005,37:619–624.84. Hendrick JL, Switzer JR. Hands-free versus hand-heldcell ph<strong>on</strong>e c<strong>on</strong>versati<strong>on</strong> <strong>on</strong> a braking resp<strong>on</strong>se by youngdrivers. Percepti<strong>on</strong> and Motor Skills, 2007, 105:514–522.85. McEnvoy SP, Stevens<strong>on</strong> MR, Woodward M. Thec<strong>on</strong>tributi<strong>on</strong> of passengers versus mobile ph<strong>on</strong>e use tomotor vehicle crashes resulting in hospital attendanceby the driver. Accident Analysis and Preventi<strong>on</strong>, 2007,39:1170–1176.86. Lam LT et al. Passenger carriage and car crash <strong>injury</strong>: acomparis<strong>on</strong> between younger and older drivers. AccidentAnalysis and Preventi<strong>on</strong>, 2003, 35:861–867.87. Fergus<strong>on</strong> SA. Other high-risk factors for young drivers:how graduated licensing does, doesn’t, or could addressthem. Journal of Safety Research, 2003, 34:71–77.88. Braitman KA et al. Crashes of novice teenage drivers:characteristics and c<strong>on</strong>tributing factors. Journal of SafetyResearch, 2008, 39:27–54.89. Chen IG et al. Teen drivers and the risk of <strong>injury</strong> to <strong>child</strong>passengers in motor vehicle crashes. Injury Preventi<strong>on</strong>,2005, 11:12–17.WORLD REPORT ON CHILD INJURY PREVENTION 53
90. Padlo P, Aultman-Hall L, Stamatiadis N. Passengers andother factors affecting the safety of young and older drivers.Transportati<strong>on</strong> Research Records, 2006, 1937:7–13.91. Williams AF. Teenage drivers: patterns of risk. Journal ofSafety Research, 2003, 34:5–15.92. Maycock G. Drinking and driving in Great Britain: areview. Crowthorne, Transport Research Laboratory, 1997(TRL Report 232).93. Dand<strong>on</strong>a R, Kumar GA, Dand<strong>on</strong>a L. Risky behaviorof drivers of motorized two wheeled vehicles in India.Journal of Safety Research, 2006, 37:149–158.94. Towner E et al. Injuries in <strong>child</strong>ren aged 0–14 years andinequalities. L<strong>on</strong>d<strong>on</strong>, Health Development Agency, 2005(http://www.nice.org.uk/niceMedia/pdf/injuries_in_<strong>child</strong>ren_inequalities.pdf, accessed 22 January 2008).95. Fatimah M et al. The risk of road traffic accidents am<strong>on</strong>gprimary school <strong>child</strong>ren in Kuala Terengganu. MedicalJournal of Malaysia, 1997, 52:402–408.96. Pless IB, Verreault R, Tenina S. A case-c<strong>on</strong>trol study ofpedestrian and bicyclist injuries in <strong>child</strong>hood. AmericanJournal of Public Health, 1989, 79:995–998.97. Joly MF, Foggin PM, Pless IB. A case-c<strong>on</strong>trol study oftraffic accidents am<strong>on</strong>g <strong>child</strong> pedestrians. In: Proceedingsof the Internati<strong>on</strong>al C<strong>on</strong>ference <strong>on</strong> Traffic Safety. NewDelhi, 1991.98. La Flamme L. Social inequality in <strong>injury</strong> risks: knowledgeaccumulated and plans for the future. Stockholm, Nati<strong>on</strong>alInstitute of Public Health, 1998.99. Hasselberg M, Laflamme L, Weitoft GR. Socioec<strong>on</strong>omicdifferences in road traffic injuries during <strong>child</strong>hood andyouth: a closer look at different kinds of road user. Journalof Epidemiology and Community Health, 2001, 55:858–862.100. Hippisley-Cox J et al. Cross-secti<strong>on</strong>al survey ofsocioec<strong>on</strong>omic variati<strong>on</strong>s in severity and mechanismof <strong>child</strong>hood injuries in Trent 1992–7. British MedicalJournal, 2002, 324:1132–1134.101. Nantulya WM, Reich M. The neglected epidemic: roadtraffic injuries in developing countries. British MedicalJournal, 2002, 324:1139–1141.102. Celis A et al. Family characteristics and pedestrian <strong>injury</strong>risk in Mexican <strong>child</strong>ren. Injury Preventi<strong>on</strong>, 2003, 9:58–61.103. Mizuno K, Kajzer J. Head injuries in vehicle-pedestrianimpact. In: Proceedings of the Society of AutomotiveEngineers <str<strong>on</strong>g>World</str<strong>on</strong>g> C<strong>on</strong>gress, 6–9 March 2000, Detroit,Michigan. Warrendale, PA, Society of AutomotiveEngineers, 2000 (http://www.sae.org/servlets/productDetail?PROD_TYP=PAPER&PROD_CD=2000-01-0157, accessed 22 April 2008).104. Crandall JR, Bhalla KS, Madeley NJ. Designing roadvehicles for pedestrian protecti<strong>on</strong>. British Medical Journal,2002, 324:1145–1148.105. Holland A et al. Driveway motor vehicle injuries in <strong>child</strong>ren.The Medical Journal of Australia, 2000, 173:192–195.106. Fent<strong>on</strong> SJ et al. The prevalence of driveway back-overinjuries in the area of sports utility vehicles. Journal ofPediatric Surgery, 2005, 40:1964–1968.107. Lovette B. Back-up detecti<strong>on</strong> devices: what do we all needto know? Dangerous blind z<strong>on</strong>es. Journal of PediatricHealth Care, 2007, 21:123–128.108. Scho<strong>on</strong> CC. Invloed kwaliteit fiets op <strong>on</strong>gevallen. [Theinfluence of cycle quality <strong>on</strong> crashes]. Leidschendam,Institute for Road Safety Research, 1996 (SWOV ReportR-96-32).109. Mohan D, Tiwari G. Road safety in low-income countries:issues and c<strong>on</strong>cerns regarding technology transfer fromhigh-income countries. In: Reflecti<strong>on</strong>s <strong>on</strong> the transfer oftraffic safety knowledge to motorizing nati<strong>on</strong>s. Melbourne,Global Traffic Safety Trust, 1998:27–56.110. Clift<strong>on</strong> KJ, Kreamer-Fults K. An examinati<strong>on</strong> of theenvir<strong>on</strong>mental attributes associated with pedestrianvehicular crashes near public schools. Accident Analysisand Preventi<strong>on</strong>, 2007, 39:708–715.111. Bly P, Dix M, Stephens<strong>on</strong> C. Comparative study ofEuropean <strong>child</strong> pedestrian exposure and accidents.L<strong>on</strong>d<strong>on</strong>, Departments of the Envir<strong>on</strong>ment, Transport andthe Regi<strong>on</strong>s, 1999.112. Kwe<strong>on</strong> SS, Shin MH. [An epidemiological study for <strong>child</strong>pedestrian traffic injuries that occurred in school-z<strong>on</strong>e](article in Korean). Journal of Preventive Medicine andPublic Health, 2005, 38:163–169.113. Roberts I et al. Effect of envir<strong>on</strong>mental factors <strong>on</strong> riskof <strong>injury</strong> of <strong>child</strong> pedestrians by motor vehicles: a casec<strong>on</strong>trolstudy. British Medical Journal, 1995, 310:91–94.114. Mueller BA et al. Envir<strong>on</strong>mental factors and the risk for<strong>child</strong>hood pedestrian-motor vehicle collisi<strong>on</strong> occurrence.American Journal of Epidemiology, 1990, 132:550–560.115. Stevens<strong>on</strong> M. Childhood pedestrian injuries: what canchanges to the road envir<strong>on</strong>ment achieve? Australia NewZealand Journal of Public Health, 1997, 21:33–37.116. Gururaj G, Reddi MN, Aer<strong>on</strong>-Thomas A. Epidemiology ofroad traffic injuries in Bangalore. In: Proceedings of the 5th<str<strong>on</strong>g>World</str<strong>on</strong>g> C<strong>on</strong>ference <strong>on</strong> Injury Preventi<strong>on</strong> and C<strong>on</strong>trol. NewDelhi, Macmillan India, 2000.117. Joshipura MK et al. Trauma care systems in India. Injury,2003, 34:686–692.118. Mohan D. Traffic safety and city structure: less<strong>on</strong>s for thefuture. Salud Pública de México, 2008, 50:S93–S100.119. Tingvall C, Haworth N. Visi<strong>on</strong> Zero: an ethical approachto safety and mobility. Paper presented to the 6th Instituteof Transport Engineers’ Internati<strong>on</strong>al C<strong>on</strong>ference <strong>on</strong> RoadSafety and Traffic Enforcement: Bey<strong>on</strong>d 2000, Melbourne,6–7 September 1999 (http://www.m<strong>on</strong>ash.edu.au/muarc/<str<strong>on</strong>g>report</str<strong>on</strong>g>s/papers/visi<strong>on</strong>zero.html, accessed 23 January 2008).120. Advancing sustainable safety in brief. Leidschendam,Netherlands, Institute for Road Safety Research, 2006(http://www.swov.nl/rapport/DMDV/Advancing_Sustainable_Safety_brief.pdf, accessed 23 January 2008).54 WORLD REPORT ON CHILD INJURY PREVENTION
121. Retting RA et al. A review of evidence-based trafficengineering measures designed to reduce pedestrian–vehicle crashes. American Journal of Public Health, 2003,93:1456–1463.122. Elvik R, Vaa T, eds. The handbook of road safety measures.Amsterdam, Elsevier Science Ltd, 2004.123. Bunn F et al. Area-wide traffic calming for preventingtraffic related injuries. Cochrane Database of SystematicReviews, 2003, (1):CD003110.124. Afukaar FK, Antwi P, Ofosu-Amaah S. Pattern of roadinjuries in Ghana: implicati<strong>on</strong>s for c<strong>on</strong>trol. Injury C<strong>on</strong>troland Safety Promoti<strong>on</strong>, 2003, 10:69–76.125. Dominican Republic: <strong>child</strong> friendly municipalities.Internati<strong>on</strong>al Secretariat for Child Friendly Cities website. Florence, UNICEF (http://www.<strong>child</strong>friendlycities.org/networking/dominican_republic.html, accessed 8May 2008).126. Steps to creating a safe routes to school program. Safe Routesto School Online Guide. Chapel Hill, NC, University ofNorth Carolina Highway Safety Research Center (http://www.saferoutesinfo.org/guide/steps/index.cfm, accessed5 July 2008).127. Mackett RL et al. A methodology for evaluating walkingbuses as an instrument of urban transport policy. TransportPolicy, 2003, 10:179–186.128. Rowland D et al. Randomised c<strong>on</strong>trolled trial of sitespecific advice <strong>on</strong> school travel patterns. Archives ofDiseases in Children, 2003, 88:6–11.129. GRSP in Bangalore. Global Road Safety Partnership web site(http://www.grsproadsafety.org/?pageid=27#GRSP%20in%20Bangalore, accessed 5 July 2008).130. Safety of vulnerable road users. Paris, Organisati<strong>on</strong> forEc<strong>on</strong>omic Co-operati<strong>on</strong> and Development, 1998 (http://www.oecd.org/dataoecd/24/4/2103492.pdf, accessed 23January 2008).131. Vulnerable road users in the Asian and Pacific regi<strong>on</strong>s.Manila, Asian Development Bank, 2003 (http://www.adb.org/Documents/Books/Road-Safety-Guidelines/vulnerable-road-users.pdf, accessed 23 January 2008).132. Test procedures: <strong>child</strong> protecti<strong>on</strong>. EuroNCAP web site (http://www.eur<strong>on</strong>cap.com/C<strong>on</strong>tent-Web-Page/cec92835-f082-4bd4-b4a3-2958ec66cbee/<strong>child</strong>-protecti<strong>on</strong>.aspx, accessed5 July 2008).133. Zaza S et al. Reviews of evidence regarding interventi<strong>on</strong>sto increase use of <strong>child</strong> safety seats. American Journal ofPreventive Medicine, 2001, 21:31–47.134. Anund A et al. Child safety in cars: literature review.Stockholm, Swedish Nati<strong>on</strong>al Road and TransportResearch Institute, 2003 (VTI <str<strong>on</strong>g>report</str<strong>on</strong>g> 489A).135. Tsoumakas K et al. Parents’ knowledge and attitudes aboutpreventing injuries in motor vehicle accidents in <strong>child</strong>renin Greece. Traffic Injury Preventi<strong>on</strong>, 2008, 9:129–134.136. Ehiri JE et al. Interventi<strong>on</strong>s for promoting boosterseat use in four to eight year olds traveling in motorvehicles. Cochrane Database of Systematic Reviews, 2006,(1):CD004334.137. Motor vehicle occupant <strong>injury</strong>: strategies for increasinguse of <strong>child</strong> safety seats, increasing use of safety beltsand reducing alcohol impaired driving. Mortality andMorbidity Weekly Report, 2001, 50:1 (http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5007a1.htm, accessed 22January 2008).138. Kedikoglou S et al. A maternity hospital-based infantcar-restraint loan scheme: public health and ec<strong>on</strong>omicevaluati<strong>on</strong> of an interventi<strong>on</strong> for the reducti<strong>on</strong> of roadtraffic injuries. Scandinavian Journal of Public Health,2005, 33:42–49.139. Dellinger A et al. Interventi<strong>on</strong>s to prevent motor vehicleinjuries. In: Doll L et al., eds. Handbook of <strong>injury</strong> andviolence preventi<strong>on</strong>. New York, NY, Springer, 2007:55–79.140. Kallan MJ, Durbin DR, Arbogast KB. Seating patternsand corresp<strong>on</strong>ding risk of <strong>injury</strong> am<strong>on</strong>g 0- to 3-yearold<strong>child</strong>ren in <strong>child</strong> safety seats. Pediatrics, 2008,121:e1342–e1347.141. Lund UJ. The effect of seating locati<strong>on</strong> <strong>on</strong> the <strong>injury</strong> ofproperly restrained <strong>child</strong>ren in <strong>child</strong> safety seats. AccidentAnalysis and Preventi<strong>on</strong>, 2005, 37:435–439.142. Hertz E. Revised estimates of <strong>child</strong> restraint effectiveness[research note]. Washingt<strong>on</strong>, DC, Nati<strong>on</strong>al HighwayTraffic Safety Administrati<strong>on</strong>, 1996.143. Johnst<strong>on</strong> C, Rivara FP, Soderberg R. Children in carcrashes: analysis of data for <strong>injury</strong> and use of restraints.Pediatrics, 1994, 6:960–965.144. Traffic safety facts 2004: occupant protecti<strong>on</strong>. Washingt<strong>on</strong>,DC, Nati<strong>on</strong>al Highway Traffic Safety Administrati<strong>on</strong>, 2004.145. Helmets: a road safety manual for decisi<strong>on</strong> makers andpractiti<strong>on</strong>ers. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>,2006 (http://www.who.int/violence_<strong>injury</strong>_preventi<strong>on</strong>/publicati<strong>on</strong>s/road_traffic/helmet_manual.pdf, accessed22 January 2008).146. Hendrie D et al. Child and family safety device affordabilityby country income level: a comparis<strong>on</strong> of 18 countries.Injury Preventi<strong>on</strong>, 2004, 10:338–343.147. Liberatti CLB et al. Helmet use by motorcyclists injuredin traffic accidents in L<strong>on</strong>drina, southern Brazil. PanAmerican Journal of Public Health, 2003, 13:33–38.148. Kwan I, Mapst<strong>on</strong>e J. Interventi<strong>on</strong>s for increasingpedestrian and cyclist visibility for the preventi<strong>on</strong> of deathand injuries. Cochrane Database of Systematic Reviews,2002, (2):CD003438.149. Van Niekerk EC. Pedestrian visibility: final <str<strong>on</strong>g>report</str<strong>on</strong>g>. Pretoria,Centre for Scientific and Industrial Research, 2003 (CR2002/78).150. Thornly SJ et al. C<strong>on</strong>spicuity and bicycle crashes:preliminary findings of the Taupo Bicycle Study. InjuryPreventi<strong>on</strong>, 2008, 14:11–18.151. Kobusingye O, Tumwesigye NM, Atuyambe L. Protectingvulnerable road users through visibility improvement: aWORLD REPORT ON CHILD INJURY PREVENTION 55
pilot study. Sydney, Road Traffic Injury Research Network,2004 (http://www.rtirn.net/PDFs/RTIRN%20Facsheet_Uganda.pdf, accessed 8 July 2008).152. Umar RS. Helmet initiatives in Malaysia. In: Proceedings ofthe 2nd <str<strong>on</strong>g>World</str<strong>on</strong>g> Engineering C<strong>on</strong>gress, Kuching, 22–25 July2002. Kuching, Instituti<strong>on</strong> of Engineers, 2002:93–101.153. Yuan W. The effectiveness of the “ride bright” legislati<strong>on</strong>in Singapore. Accident Analysis and Preventi<strong>on</strong>, 2000,32:559–563.154. Wells S et al. Motorcycle rider c<strong>on</strong>spicuity and crashrelated <strong>injury</strong>: case-c<strong>on</strong>trol study. British Medical Journal,2004, 328:857.155. Police enforcement strategies to reduce traffic casualtiesin Europe. Brussels, European Transport Safety Council,Working Party <strong>on</strong> Traffic Regulati<strong>on</strong> Enforcement, 1999(http://www.etsc.be/oldsite/strategies.pdf, accessed 29April 2008).156. Norghani M et al. Use of exposure c<strong>on</strong>trol methods totackle motorcycle accidents in Malaysia. Serdang, RoadSafety Research Centre, Universiti Putra Malaysia, 1998(Research Report 3/98).157. Scho<strong>on</strong> CC, Goldenbeld C. J<strong>on</strong>ge brom- en snorfietsers:kan hun <strong>on</strong>gevalskans sterk omlaag? Effecten van maatregelenen draagvlak daarvoor <strong>on</strong>der j<strong>on</strong>geren en organisaties.[Young mopedists and light-mopedists: can theiraccident chance be greatly reduced? Effects of measuresand support for them am<strong>on</strong>g the young and organizati<strong>on</strong>s].Leidschendam, Institute for Road Safety Research,2003 (SWOV Report R-2003-13) (http://www.swov.nl/rapport/R-2003-13.pdf, accessed 22 January 2008).158. Shults R et al. Review of evidence regarding interventi<strong>on</strong>sto reduce alcohol-impaired driving. American Journal ofPreventive Medicine, 2001, 21:66–84.159. Elder RW et al. Effectiveness of sobriety checkpoints forreducing alcohol involved. Traffic Injury Preventi<strong>on</strong>, 2002,3:266–274.160. Barbar T et al. Alcohol: no ordinary commodity. Oxford,Oxford University Press, 2003.161. Henstridge J, Homel R, Mackay P. The l<strong>on</strong>g-term effectsof random breath testing in four Australian states: a timeseries analysis. Canberra, Federal Office of Road Safety,1997.162. Hings<strong>on</strong> RW, Assailly J-P, Williams AF. Underage drinking:frequency, c<strong>on</strong>sequences, and interventi<strong>on</strong>s. Traffic InjuryPreventi<strong>on</strong>, 2004, 5:228–236.163. Hedlund J, Shults R, Compt<strong>on</strong> R. What we know, what wed<strong>on</strong>’t know, and what we need to know about graduateddriver licensing. Journal of Safety Research, 2003, 34:107–115.164. Hedlund J, Compt<strong>on</strong> R. Graduated driver licensingresearch in 2004 and 2005. Journal of Safety Research,2005, 36:4–14.165. Preusser DF, Tis<strong>on</strong> J. GDL then and now. Journal of SafetyResearch, 2007, 28:159–163.166. Desapriya EBR et al. Child motor vehicle occupant andpedestrian casualties before and after enactment of <strong>child</strong>restraint seats legislati<strong>on</strong> in Japan. Injury C<strong>on</strong>trol andSafety Promoti<strong>on</strong>, 2004, 11:225–230.167. Duperrex O et al. Safety educati<strong>on</strong> of pedestrians for<strong>injury</strong> preventi<strong>on</strong>: a systematic review of randomisedc<strong>on</strong>trol trials. British Medical Journal, 2002, 324:1129.168. Roberts<strong>on</strong> L. Injury epidemiology, 3rd ed. New York, NY,Oxford University Press, 2007.169. Gielen A, Sleet DA, DiClemente R, eds. Injury and violencepreventi<strong>on</strong>: behavioral science theories, methods andapplicati<strong>on</strong>s. San Francisco, CA, Jossey Bass, 2006.170. Thoms<strong>on</strong> JK, Whelan KM. A community approach to roadsafety educati<strong>on</strong> using practical training methods. L<strong>on</strong>d<strong>on</strong>,Department for Transport, 1997 (Road Safety ResearchReport No. 3).171. Rivara F, Metrik J. Training programs for bicycle safety.Seattle, WA, Traffic Safety Commissi<strong>on</strong>, 1998 (http://safety.fhwa.dot.gov/ped_bike/docs/b_training.pdf,accessed 22 January 2008).172. Towner E et al. What works in preventing unintenti<strong>on</strong>alinjuries in <strong>child</strong>ren and young adolescents? An updatedsystematic review. L<strong>on</strong>d<strong>on</strong>, Health Development Agency,2001.173. Soul City Institute: health and development communicati<strong>on</strong>.Soul City web site (http://www.soulcity.org.za/, accessed28 April 2008).174. Scheepers E et al. Evaluating health communicati<strong>on</strong>: aholistic overview of the impact of Soul City IV. HealthPromoti<strong>on</strong> Journal of Australia, 2004, 15:121−133.175. Vernick JS et al. Effects of high school driver educati<strong>on</strong> <strong>on</strong>motor vehicle crashes, violati<strong>on</strong>s, and licensure. AmericanJournal of Preventive Medicine, 1999, 16(1 Suppl.):40–46.176. Roberts I et al. School based driver educati<strong>on</strong> for thepreventi<strong>on</strong> of traffic crashes. Cochrane Database ofSystematic Reviews, 2001, (3):CD003201.177. Ker K et al. Post-licence driver educati<strong>on</strong> for the preventi<strong>on</strong>of road traffic crashes: a systematic review of randomizedc<strong>on</strong>trolled trials. Accident Analysis and Preventi<strong>on</strong>, 2005,37:205–213.178. Sasser S et al. Prehospital trauma care systems. Geneva,<str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2005 (http://www.who.int/entity/violence_<strong>injury</strong>_preventi<strong>on</strong>/publicati<strong>on</strong>s/services/39162_oms_new.pdf, accessed 14 May 2008).179. Mock C et al. Guidelines for essential trauma care. Geneva,<str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2004 (http://whqlibdoc.who.int/publicati<strong>on</strong>s/2004/9241546409.pdf, accessed22 January 2008).180. Cummings P et al. Air bags and passenger fatality accordingto passenger age and restraint use. Epidemiology, 2002,13:525–532.181. Braver et al. Deaths am<strong>on</strong>g drivers and right-fr<strong>on</strong>t passengersin fr<strong>on</strong>tal collisi<strong>on</strong>s: redesigned air bags relative to firstgenerati<strong>on</strong>air bags. Traffic Injury Preventi<strong>on</strong>, 2008, 9:48–58.56 WORLD REPORT ON CHILD INJURY PREVENTION
WORLD REPORT ON CHILD INJURY PREVENTION 57
DROWNINGRUBY’S STORY© S. CooperChristmas is a joyous time for most, but for parents Scott andAmanda and older sister Abby, Christmas Eve 2006 was theday they found their 14-m<strong>on</strong>th-old daughter Ruby face down intheir home pool grey, lifeless and without a heartbeat. The familywas preparing for Christmas when Scott and Amanda realizedRuby was missing. Scott’s first instinct was to check the poolwhich had a makeshift fence while they were landscaping, buthe couldn’t see her and returned inside to c<strong>on</strong>tinue looking.Unknown to them, <strong>child</strong>ren sink when they drown and Ruby was actually at thebottom of the pool. It wasn’t until Amanda re-checked the pool from a differentangle that she discovered every parent’s worst nightmare. Ruby was pulled fromthe water and Scott began CPR while Amanda frantically called an ambulancewhich took 40 minutes to reach their house. Fortunately Amanda had her GP’shome number and she and her husband – both doctors – rushed to assist. Rubywas given CPR but still remained unresp<strong>on</strong>sive and without a heartbeat. As alast resort the lifesaving decisi<strong>on</strong> was made to give her an adrenalin injecti<strong>on</strong>straight to the heart. To every<strong>on</strong>e’s relief her heart began to beat and she wasrushed to hospital.Ruby was given a 10% chance of survival and Scott and Amanda were warned thatif she did survive l<strong>on</strong>g-term brain damage was highly likely. But after spendingChristmas day in an induced coma and a total of three weeks in the PaediatricIntensive Care Unit and Neurological ward, against all odds, Ruby made amiraculous recovery.Ruby slowly regained her strength and learned to crawl and walk again and hasbegun to talk. Her fine motor skills were affected so she visits with an occupati<strong>on</strong>altherapist and physiotherapist every two weeks. The family have been told that it isnow a matter of ensuring Ruby meets milest<strong>on</strong>es and that if there is any l<strong>on</strong>g-termneurological damage it is likely to become evident when Ruby starts school.Although Ruby’s survival and miraculous progress are not typical of <strong>child</strong>ren whohave experienced a n<strong>on</strong>-fatal drowning, the circumstances in which it occurredare very comm<strong>on</strong>. A lapse in adult supervisi<strong>on</strong> even for very short periods oftime is a major c<strong>on</strong>tributing factor to<strong>child</strong>ren drowning. Big sister Abby wasalso deeply affected by the incident andAmanda says that she is an extremelyanxious mother now, and so much moreaware of potential hazards. Amandasays: “Before this happened I wasvery relaxed as a mum, maybe toomuch so, and thought that nothingwould ever happen to my <strong>child</strong>. It’sterrifying how quickly things canhappen. I d<strong>on</strong>’t even want to dwell<strong>on</strong> what could’ve been, we areamazingly lucky. So many peoplehave stories that d<strong>on</strong>’t all turn outas well as ours.”Safe Kids New ZealandMedia Release, 10 October 2007http://www.safekids.org.nz/.
CHAPTER 3 – DROWNINGChapter 3DrowningIntroducti<strong>on</strong>Water touches every aspect of <strong>child</strong>ren’s lives. They needit to grow, they are comforted by it, they are cleaned andcooled by it – and without it they cannot survive. Water tomost <strong>child</strong>ren means fun, play and adventure – in a pool,p<strong>on</strong>d, lake or simply in the road following a rain storm.Water, though, can be a dangerous medium. A small <strong>child</strong>can drown in a few centimetres of water at the bottom ofa bucket, in the bath, or in a rice field. Drowning is an<strong>injury</strong> that displays epidemiological patterns that changeaccording to age group, body of water and activity. Inmost countries around the world, drowning ranks am<strong>on</strong>gthe top three causes of death from unintenti<strong>on</strong>al <strong>injury</strong>,with the rates highest am<strong>on</strong>g <strong>child</strong>ren under five yearsof age.This chapter describes the magnitude of thephenomen<strong>on</strong> of <strong>child</strong>hood drowning around the world,in terms of deaths, morbidity and disability – pointingto the likelihood that the true size of the problem hasbeen substantially underestimated. It summarizes therisk and protective factors, with the Hadd<strong>on</strong> matrix as aframework, and sets out the various preventi<strong>on</strong> strategies,both proven and promising. The chapter c<strong>on</strong>cludeswith recommendati<strong>on</strong>s, urging that c<strong>on</strong>fr<strong>on</strong>ting thispreventable <strong>injury</strong> should be made a priority and givenproper resources for research and preventi<strong>on</strong> efforts.For the purpose of this chapter, drowning refers to anevent in which a <strong>child</strong>’s airway is immersed in a liquidmedium, leading to difficulty in breathing (1). This eventmay result in death or survival. The definiti<strong>on</strong> used in this<str<strong>on</strong>g>report</str<strong>on</strong>g> – the process of experiencing respiratory impairmentfrom submersi<strong>on</strong>/immersi<strong>on</strong> in liquid (2) – is <strong>on</strong>e agreedup<strong>on</strong> by experts at a recent world c<strong>on</strong>ference <strong>on</strong> drowning.This definiti<strong>on</strong> is simple and comprehensive, encompassingcases that result in either death, a certain level of morbidityor no morbidity (2).High-income countries, such as Australia and UnitedStates, have seen dramatic reducti<strong>on</strong>s in death rates fromdrowning, which have most likely come about as a result ofboth changes in exposure to risk and the implementati<strong>on</strong> ofspecific interventi<strong>on</strong>s (3, 4). The less<strong>on</strong>s learned from thesecountries may be applicable to other countries around theworld in helping to develop preventi<strong>on</strong> programmes.Epidemiology of drowningAccording to the WHO Global Burden of Disease estimates,388 000 people died in 2004 as a result of drowning aroundthe world, of whom 45% were under the age of 20 years(see Statistical Annex, Table A.1). Fatal drowning ranked13th as the overall cause of death am<strong>on</strong>g <strong>child</strong>ren under15 years old, with the 1–4 year age group appearing atgreatest risk. The overall global rate for drowning am<strong>on</strong>g<strong>child</strong>ren is 7.2 deaths per 100 000 populati<strong>on</strong>, thoughwith significant regi<strong>on</strong>al variati<strong>on</strong>s. The drowning ratein low-income and middle-income countries is six timeshigher than in high-income countries (with rates of 7.8 per100 000 and 1.2 per 100 000, respectively).For those <strong>child</strong>ren who survive drowning, many areleft with l<strong>on</strong>g-term c<strong>on</strong>sequences and disability that createenormous difficulties for families, with prohibitively highcosts of health care. Global data show that approximately28% of all unintenti<strong>on</strong>al <strong>injury</strong> deaths am<strong>on</strong>g <strong>child</strong>ren aredue to drowning and 1.1% of all disability-adjusted lifeyears (DALYs) lost for <strong>child</strong>ren under 15 years of age inlow-income and middle-income countries are from n<strong>on</strong>fataldrowning (see Statistical Annex, Table A.2).Available data show that there are substantial differencesin drowning fatality rates across the globe.Comparis<strong>on</strong>s, though, are difficult because of the use ofdifferent definiti<strong>on</strong>s, different categories counted or excludedin the data, the frequent lack of comprehensivenati<strong>on</strong>al data and the variable quality of data. For somecountries, mostly high-income <strong>on</strong>es, the pattern of fataldrowning is well documented. It now appears that therecan be c<strong>on</strong>siderable differences both within and betweencountries and regi<strong>on</strong>s with regard to the nature and scaleof <strong>child</strong>hood drowning. Although drowning rates havedeclined significantly in recent decades in some highincomecountries, there are few established risk factorsal<strong>on</strong>g with proven preventive strategies. This highlightsthe need for well-designed research to study the causesand origins of drowning injuries and to evaluate preventi<strong>on</strong>measures.MortalityIn 2004, approximately 175 000 <strong>child</strong>ren and youth underthe age of 20 years died as a result of drowning around theworld. The overwhelming majority, 98.1% of these deaths,occurred in low-income and middle-income countries(see Statistical Annex, Table A.1). The low-income andmiddle-income countries of the WHO Western PacificRegi<strong>on</strong> have the highest rate of drowning deaths (13.9 per100 000 populati<strong>on</strong>), followed by the African Regi<strong>on</strong> (7.2 per100 000), the low-income and middle-income countries ofthe Eastern Mediterranean Regi<strong>on</strong> (6.8 per 100 000) and theSouth-East Asia Regi<strong>on</strong> (6.2 per 100 000) (see Figure 3.1).WORLD REPORT ON CHILD INJURY PREVENTION 59
FIGURE 3.1Fatal drowning rates per 100 000 <strong>child</strong>ren a by WHO regi<strong>on</strong> and counry income level, <str<strong>on</strong>g>World</str<strong>on</strong>g>, 200410.0+6.0–9.92.0–5.9
FIGURE 3.2Fatal <strong>injury</strong> rates per 100 000 <strong>child</strong>ren aged 0–17 years in five aAsian countriesaDrowningRoad traffic injuriesSuffocati<strong>on</strong>Animal bitesSuicideElectrocuti<strong>on</strong>Sharp objectsPois<strong>on</strong>ingBlunt objectsBurnsFalling objectsBangladesh, China (Beijing, Jiangxi), Philippines, Thailand, Viet NamSource: reference 6.Falls0 5 10 15 20 25 30Rate per 100 000 <strong>child</strong>renFIGURE 3.3Fatal drowning rates per 100 000 <strong>child</strong>ren by age and countryincome level, <str<strong>on</strong>g>World</str<strong>on</strong>g>, 2004Rate per 100 000 populati<strong>on</strong>121086420HIC = High-income countries; LMIC = low-income and middle-income countries.Source: WHO (2008), Global Burden of Disease: 2004 update.HICLMICUnder 1 1–4 5–9 10–14 15–19Age (years)AgeThe death rates for drowning, by age group, for <strong>child</strong>renand young people less than 20 years old show a ratherhigher rate in <strong>child</strong>ren in the 0–4-year age bracket, ascompared with the rates for the other five-year age groups(see Figure 3.3).Data from the studies c<strong>on</strong>ducted in South and East Asiashow that drowning accounted for 90% of all <strong>injury</strong> deathsfor <strong>child</strong>ren aged 1–4 years and over 50% of <strong>injury</strong> deathsfor <strong>child</strong>ren aged 5–9 years (6). In Bangladesh, 26% of alldeaths in <strong>child</strong>ren between the ages of 1 and 4 years aredue to drowning (12).Drowning is the leading cause of <strong>injury</strong> death in <strong>child</strong>renaged 1 to 2 years in the United States (13) and am<strong>on</strong>g1–14-year-olds in China (14, 15). In Brazil, drowning isthe leading cause of <strong>injury</strong> death in 1–4-year-olds, and26% of all unintenti<strong>on</strong>al <strong>injury</strong> deaths in <strong>child</strong>ren aged 0to 14 years are from drowning (16).GenderBoys are overrepresented in every regi<strong>on</strong> of the world withregard to drowning death rates (see Table 3.1). In 2004, theoverall fatality rate for boys under the age of 20 years was9 per 100 000 populati<strong>on</strong>, nearly twice as high as the ratefor girls (5.2 per 100 000 populati<strong>on</strong>). A similar skewingtowards boys was found in the South and East Asiansurveys (see Statistical Annex, Table B.1).Locati<strong>on</strong>Every year 70 Member States – mainly middle-income andhigh-income countries –submit to WHO mortality data thatinclude the fourth digit of the Internati<strong>on</strong>al Classificati<strong>on</strong>of Disease codes, which allows disaggregati<strong>on</strong> intosubtypes of drowning. Analysis of these data show thateven in these relatively better-off countries, informati<strong>on</strong><strong>on</strong> where the drowning occurs is poorly documented. Inmore than 50% of cases the place is given as “unspecified”,making analysis of place of drowning difficult (17).Some countries, however, do have alternative sources ofdata. In Brazil, for instance, more than 60% of drowningoccurs in natural bodies of water (16), while in SouthAfrica the locati<strong>on</strong> of drowning is str<strong>on</strong>gly related tosocioec<strong>on</strong>omic status. Am<strong>on</strong>g wealthier communitiesTABLE 3.1Fatal drowning rates per 100 000 <strong>child</strong>ren a by sex, country income level and WHO regi<strong>on</strong>, <str<strong>on</strong>g>World</str<strong>on</strong>g>, 2004Africa Americas South-East Asia Europe Eastern Mediterranean Western PacificLMIC HIC LMIC LMIC HIC LMIC HIC LMIC HIC LMICBoys 9.0 1.8 5.0 7.1 0.8 5.5 10.7 9.0 1.7 17.5Girls 5.4 0.7 1.8 5.2 0.3 2.4 1.6 4.5 0.7 9.9aThese data refer to those under 20 years of age.HIC = High-income countries; LMIC = low-income and middle-income countries.Source: WHO (2008), Global Burden of Disease: 2004 update.WORLD REPORT ON CHILD INJURY PREVENTION 61
in South Africa, swimming pools and the sea are themajor sites of drowning, while for poorer communitiesthe majority of drowning am<strong>on</strong>g <strong>child</strong>ren occurs in ruralareas, typically in rivers, lakes and dams (18).The place of drowning is also related to age. In theUnited States, infants most comm<strong>on</strong>ly drown in baths andbuckets, 1–4-year-olds in swimming pools, and <strong>child</strong>renover 5 years of age most often in pools, rivers and lakes(19, 20). Most young <strong>child</strong>ren who drowned in pools werelast seen in the home, had been out of sight for less thanfive minutes, and were in the care of <strong>on</strong>e or both parentsat the time (21).In some industrialized countries such as the UnitedKingdom, despite a reducti<strong>on</strong> in overall drowning ratesam<strong>on</strong>g <strong>child</strong>ren, the number of <strong>child</strong>ren dying in gardenp<strong>on</strong>ds or other ornamental water features has increasedover the past decade (22).MorbidityEstimates of the number of serious n<strong>on</strong>-fatal cases ofdrowning are more difficult to obtain. Reporting of n<strong>on</strong>fatalcases is generally less standardized and <str<strong>on</strong>g>report</str<strong>on</strong>g>ing to acentral health statistics system is often not mandatory. Thisis true of most countries, regardless of income, althoughsome countries are able to provide estimates from hospitaldata. Nevertheless, for <strong>child</strong>ren aged 0–14 years, WHOglobal estimates for n<strong>on</strong>-fatal drowning range between 2and 3 milli<strong>on</strong>.Am<strong>on</strong>g <str<strong>on</strong>g>report</str<strong>on</strong>g>ed drowning cases, case fatality rates arehigh. Once a drowning is significant enough to warrant<str<strong>on</strong>g>report</str<strong>on</strong>g>ing, there is a high likelihood that the event hasresulted in death or significant disability. For each fatality,it is estimated that there are between <strong>on</strong>e and four n<strong>on</strong>fatalevents serious enough to result in hospitalizati<strong>on</strong> (23).Improvements in medical treatment are unlikely to changethis pattern significantly in the near future. There is thusa need to focus <strong>on</strong> primary preventi<strong>on</strong>, rapid and effectiverescue, and immediate resuscitati<strong>on</strong> in cases of drowning.C<strong>on</strong>sequences of n<strong>on</strong>-fatal drowningThe l<strong>on</strong>g-term health c<strong>on</strong>sequences of n<strong>on</strong>-fatal <strong>child</strong>hooddrowning are not well known, as few studies have assessedfuncti<strong>on</strong>al outcome after drowning (23–25).An Australian study <strong>on</strong> drowning for the five-yearperiod 1999–2000 to 2003–2004, for hospital admissi<strong>on</strong>sof all ages, showed <strong>on</strong> average that 22.3% of cases wereleft with severe or persistent respiratory or neurologicalc<strong>on</strong>sequences (26). The study also indicated that at least 5%of <strong>child</strong> survivors from drowning who had been admitted tohospital were discharged with severe neurological deficits(meaning that they would survive in a vegetative state).In the early 1990s, a British study <str<strong>on</strong>g>report</str<strong>on</strong>g>ed that am<strong>on</strong>gall drowning cases in <strong>child</strong>ren younger than 14 years ofage who were admitted to hospital, 8% died and 5% hada severe neurological deficit (27). Similar findings were<str<strong>on</strong>g>report</str<strong>on</strong>g>ed from a South African study, which found that12% of <strong>child</strong>ren admitted for drowning subsequently diedand 6% suffered from a severe neurological deficit (28).In studies in both the United States (23) and the UnitedKingdom (27), all <strong>child</strong>ren who had suffered drowningand who were alert <strong>on</strong> admissi<strong>on</strong> to hospital fullyrecovered. In the United States review, half of all <strong>child</strong>renwho were c<strong>on</strong>fused or comatose <strong>on</strong> admissi<strong>on</strong> had a pooroutcome, 35% died and 15% had a severe neurologicaldeficit (23). A high proporti<strong>on</strong> of <strong>child</strong> drowning caseswith poor outcomes has also been observed in a paediatricrespiratory care unit in Thailand, where the mortality ratewas 26% and 36% suffered from neurological l<strong>on</strong>g-termc<strong>on</strong>sequences (29).Due to differences in patient populati<strong>on</strong>s and studydesigns, the figures <strong>on</strong> the health c<strong>on</strong>sequences of n<strong>on</strong>fatal<strong>child</strong>hood drowning are not properly comparableacross countries. Moreover, many studies lack detailedinformati<strong>on</strong> <strong>on</strong> functi<strong>on</strong>al outcomes. There is a needfor studies measuring the c<strong>on</strong>sequences of drowning in<strong>child</strong>hood – and n<strong>on</strong>-fatal drowning in particular – usingcomparable methodologies and internati<strong>on</strong>al guidelines(30). This would allow for sound estimates of the prevalenceof brain damage and other permanent disabilities resultingfrom n<strong>on</strong>-fatal drowning in <strong>child</strong>hood.Impact <strong>on</strong> families and communitiesThe lifel<strong>on</strong>g health c<strong>on</strong>sequences of n<strong>on</strong>-fatal drowninghave a great impact <strong>on</strong> families, and include psychosocialc<strong>on</strong>sequences for those who have suffered drowning, theirsiblings, parents and other caregivers.Disability-adjusted life years (DALYs) lost for drowningvary widely (see Statistical Annex, Table A.2). For <strong>child</strong>renyounger than 15 years, the higher figures come from lowincomeand middle-income countries of the WHO WesternPacific Regi<strong>on</strong>, where drowning is resp<strong>on</strong>sible for 4% ofDALYs, from all causes (see Statistical Annex, Table A.2).The impact of drowning <strong>on</strong> communities can be furtherestimated in terms of potential years of productive life lostand valued years of potential life lost. Both these measuresestimate the loss of productivity due to premature deathbefore the usual age of retirement at 65 years. The cases ofBangladesh, China and Viet Nam provide good examplesof the huge impact <strong>on</strong> the ec<strong>on</strong>omy of drowning (6). Astudy in China showed that <strong>injury</strong> death by far exceededother major diseases – such as heart disease, cancerand infectious diseases – as a c<strong>on</strong>tributor to losses inproducti<strong>on</strong>. The study also found that drowning rankedsec<strong>on</strong>d, after motor vehicle traffic injuries, am<strong>on</strong>g all causesof <strong>injury</strong>, in terms of both potential years of productive lifelost and valued years of potential life lost (31).Ec<strong>on</strong>omic impact of drowningStudies to assess the costs of <strong>injury</strong> in several parts ofthe world (32–36) have up to now largely neglected or62 WORLD REPORT ON CHILD INJURY PREVENTION
else underestimated the ec<strong>on</strong>omic impact of drowning.In spite of the scarcity of accurate and comparable data,available estimates indicate that n<strong>on</strong>-fatal drowning mayhave serious ec<strong>on</strong>omic c<strong>on</strong>sequences. Specific studies intothe costs of hospitalizati<strong>on</strong>s for n<strong>on</strong>-fatal drowning inthe United States (34, 36, 37) have shown that while mostcases can be discharged <strong>on</strong> the same day or after a singlenight’s stay, a small proporti<strong>on</strong> need to receive intensivetreatment for very l<strong>on</strong>g periods. For this reas<strong>on</strong>, the meandirect costs associated with hospitalizati<strong>on</strong> have been<str<strong>on</strong>g>report</str<strong>on</strong>g>ed at $US 13 000 to $US 14 000 per case (36, 37). Forcases with severe l<strong>on</strong>g-term c<strong>on</strong>sequences, such as braindamage, treatment costs al<strong>on</strong>e can exceed $US 100 000. Ina cost of <strong>injury</strong> study undertaken in Australia, n<strong>on</strong>-fataldrowning was found to have the highest average lifetimecost – an estimate that includes direct and indirect costs –per patient of any <strong>injury</strong> type (38). Studies of the impact of<strong>child</strong>hood drowning <strong>on</strong> families and communities showthat the cost is highest for those low-income and middleincomecountries in which families rely <strong>on</strong> older <strong>child</strong>renfor income (39).Limitati<strong>on</strong>s of dataStatistics <strong>on</strong> drowning are based <strong>on</strong> a broad range of datasources. Although much progress has been made aroundthe world in collecting data, the availability and qualityof data <strong>on</strong> drowning varies greatly between countries,depending <strong>on</strong> the surveillance systems in place and theavailability and quality of other statistical resources. Data<strong>on</strong> drowning deaths are lacking or unreliable in many lowincomeand middle-income countries, despite periodicsurveys or local data that suggest that these countries havethe highest rates of fatal drowning (40).Even in countries where counts of drowning deathsappear relatively complete, important basic details aboutthe event are often lacking, including informati<strong>on</strong> <strong>on</strong> thelocati<strong>on</strong> of drowning, the intent and the circumstances.There are two main reas<strong>on</strong>s for this lack of informati<strong>on</strong>.First, the data collecti<strong>on</strong> systems employed may notcapture all the relevant informati<strong>on</strong> – such as the age ofthe pers<strong>on</strong> c<strong>on</strong>cerned and their swimming ability, thetype of water in which the drowning occurred, the causeof immersi<strong>on</strong>, whether there were immediate attempts atresuscitati<strong>on</strong>, and the presence of any barriers. Sec<strong>on</strong>d,the informati<strong>on</strong> may not be available at source. Manyincidents are not witnessed and it is not always possibleto rec<strong>on</strong>struct the specific circumstances around theevent (41).Both lack of informati<strong>on</strong> and misclassificati<strong>on</strong> have aneffect <strong>on</strong> overall estimates of the impact of drowning. Incases where a pers<strong>on</strong> survives drowning for a period of timein hospital, but dies some days later, the primary cause ofdeath may be coded as something other than drowning – forexample, as respiratory failure. Under<str<strong>on</strong>g>report</str<strong>on</strong>g>ing also occursbecause of the ways that intent can be classified (42).Many countries classify deaths according to theInternati<strong>on</strong>al Classificati<strong>on</strong> of Disease (ICD) E-codes.These data are then used to characterize drowning inthe regi<strong>on</strong>. The most recent (tenth) revisi<strong>on</strong> of the ICDis an improvement over previous editi<strong>on</strong>s of the ICD inthat the newer codes are more specific as to the locati<strong>on</strong>of drowning. However, most countries do not use thefourth character of the ICD code which details where thedrowning occurred.Risk factorsKnowledge of risk factors is a critical prerequisite for theeffective preventi<strong>on</strong> of drowning (see Table 3.2). Availablestudies <strong>on</strong> drowning suggest that people living in countries– particularly countries that are densely populated –with a large amount of open water are at a higher riskof drowning. Other risk factors, such as gender and age,appear to be almost universal.Child-related factorsAge and developmentAs already stated, <strong>child</strong>ren under five years of age appearto have the highest drowning mortality rates worldwide,with rates am<strong>on</strong>g all age groups peaking in 1–4-yearolds.In late adolescences another, smaller peak is seen.This pattern is generally c<strong>on</strong>sistent across the world. Thelikely explanati<strong>on</strong>s for these peaks relate to developmentalprocesses in young <strong>child</strong>ren and experimentati<strong>on</strong> am<strong>on</strong>gadolescents, especially with substances such as alcohol.With <strong>child</strong> drowning, risk and circumstances aregenerally related to the developmental stage of the <strong>child</strong>.Because infants under <strong>on</strong>e year of age are usually unableto access water by themselves, unintenti<strong>on</strong>al drowning atthis age is mostly the result of a <strong>child</strong> being left al<strong>on</strong>e orwith an unqualified caregiver – such as a young sibling – inor near water. By c<strong>on</strong>trast, <strong>child</strong>ren who are more mobileand inquisitive, but still too young to have developed anawareness of hazards or avoidance skills, often wanderaway from the supervising adult and fall or climb intoa nearby body of water (3, 43–45). Often the parent orcaregiver is unaware that the <strong>child</strong> has approached or hasfallen into the water (46).The increased risk during adolescence is possibly asa result of less supervisi<strong>on</strong> and increased independence,increased risk-taking and greater exposure to open waterduring work or leisure (6, 26).GenderBased <strong>on</strong> global data, rates of fatal drowning are higherin males than females. This is true in all age groups withthe excepti<strong>on</strong> of infants less than <strong>on</strong>e, where rates am<strong>on</strong>gfemales are higher than males (see Table 3.3). Infanticidesof females, misclassified as unintenti<strong>on</strong>al events, may bea factor here. Am<strong>on</strong>g males, drowning death rates peakWORLD REPORT ON CHILD INJURY PREVENTION 63
TABLE 3.2Hadd<strong>on</strong> Matrix applied to the risk factors for <strong>child</strong>hood drowningPhasesPre-eventEventPost-eventFactorsChild Agent Physical envir<strong>on</strong>ment Socioec<strong>on</strong>omic envir<strong>on</strong>mentDevelopmental issues; gender; vulnerability;underlying medical c<strong>on</strong>diti<strong>on</strong>,e.g. epilepsy; lack of supervisi<strong>on</strong>;lack of knowledge about water risks;need to access water for functi<strong>on</strong>alpurposes, e.g. drinking, washing orfishing; transport <strong>on</strong> water; recreati<strong>on</strong>aluse of water; alcohol c<strong>on</strong>sumpti<strong>on</strong>by adolescent swimmers or caregiversChild not wearing pers<strong>on</strong>al flotati<strong>on</strong>device; rescuer unable to swim; lack ofswimming and/or water survival skills;overestimati<strong>on</strong> of swimming ability;lack of strength; lack of comprehensi<strong>on</strong>of situati<strong>on</strong>; panic resp<strong>on</strong>se; swimmingal<strong>on</strong>e; lack of pers<strong>on</strong>al alerting devicesor knowledge of emergency signals(such as waving arms)Delay in rescue; inaccessible first-aidkits; lack of knowledge by caregiverabout what to do immediately; lack ofalerting mechanisms (such as mobileph<strong>on</strong>e, flares)Unprotected water hazards;unsafe watercraft; overloadedwatercraftDeep water; str<strong>on</strong>g riverwater current; ocean ripcurrent; very cold water;big waves; lack of pers<strong>on</strong>alflotati<strong>on</strong> devices or otherlife-saving devices in boat;lack of lifeguardsVictim carried away fromshore by currentLack of barriers; unfamiliar envir<strong>on</strong>ment;slippery, uneven, unstableor steep surfaces near or in water;weather c<strong>on</strong>diti<strong>on</strong>s, e.g. floods;str<strong>on</strong>g sea currents; inadequatephysical infrastructure, such asbridges or safe crossings; lack ofsafe water supplies; lack of warningof severe weatherVariable water depth; unstablefooting; lack of escape mechanism,e.g. ladder, ropes, flotati<strong>on</strong> device;snags in waterL<strong>on</strong>g emergency or fire departmentresp<strong>on</strong>se time; inadequate rescueand treatment skills; poor accessto water; inadequate transport forprompt medical careLack of supervisi<strong>on</strong> or<strong>child</strong> care; reliance <strong>on</strong>peer or older <strong>child</strong> supervisi<strong>on</strong>;poverty; largefamilies; unemployed orilliterate parents; failureof authorities to removeor protect hazards; lack ofpool-fencing legislati<strong>on</strong>;lack of water safety instructi<strong>on</strong>and communityawareness programmesPoor access to informati<strong>on</strong>and resources for minimizingrisk; inadequatecommunicati<strong>on</strong>s or infrastructureto call for emergencyhealth servicesInadequate care; pooraccess to acute care hospitalsand rehabilitati<strong>on</strong>services; little communitysupport for victims andfamiliesin the 1–4-year age group. In females, rates are highest ininfants and decline thereafter. The greatest difference indrowning death rates by gender occurs in adolescents aged15–19 years, where rates am<strong>on</strong>g males are 2.4 times greaterthan rates am<strong>on</strong>g females.This gender pattern is seen across the world, irrespectiveof a country’s wealth (4, 47, 48). Males in the WHO Africanand Western Pacific Regi<strong>on</strong>s have the highest drowningrelatedmortality rates worldwide (39). In most regi<strong>on</strong>s,with the excepti<strong>on</strong> of the Americas and the EasternMediterranean, males’ death rates from drowning areroughly double those of females.TABLE 3.3Fatal drowning rates per 100 000 <strong>child</strong>ren by age and sex, <str<strong>on</strong>g>World</str<strong>on</strong>g>,2004Age ranges (in years)Under 1 1–4 5–9 10–14 15–19 Under 20Boys 6.4 11.8 7.8 8.3 9.3 9.0Girls 9.8 7.6 4.9 4.0 3.8 5.2Source: WHO (2008), Global Burden of Disease: 2004 update.The reas<strong>on</strong> for this may be that boys are more involvedthan girls in work that takes place in or near open bodiesof water, and that they indulge to a greater extent inrecreati<strong>on</strong>al aquatic activities. This is illustrated by thehigh number of young males who drown in Uganda whileworking <strong>on</strong> fishing boats (49). There is some evidence fromhigh-income countries that greater risk-taking behaviouralso c<strong>on</strong>tributes to higher drowning rates am<strong>on</strong>g boys.There is also evidence that, during aquatic activities, theyare more likely than girls to swim al<strong>on</strong>e, to swim at nightand to c<strong>on</strong>sume alcohol when swimming or boating (47,50–53).PovertyAs previously noted, even within a given regi<strong>on</strong> of theworld, there are c<strong>on</strong>siderable differences in drowningmortality rates between high-income and low-incomecountries. This is also the case within certain countries. Alack of educati<strong>on</strong>al opportunity, associated with poverty,may be <strong>on</strong>e factor involved. There is some evidence tosuggest that drowning in <strong>child</strong>ren is affected by the levelof educati<strong>on</strong> of the family head or the caregiver. A studyin Guadalajara, Mexico, for example, found that the risk ofa <strong>child</strong> aged 1 to 4 years dying from drowning was higher64 WORLD REPORT ON CHILD INJURY PREVENTION
am<strong>on</strong>g those <strong>child</strong>ren from households where the head ofthe family had not completed elementary school (54). InBangladesh, <strong>child</strong>ren whose mothers had <strong>on</strong>ly primaryeducati<strong>on</strong> were at significantly greater risk of drowningcompared to <strong>child</strong>ren whose mothers had sec<strong>on</strong>daryor higher educati<strong>on</strong> (9). Against this, the study of <strong>child</strong>drowning in Xiamen, China found that the educati<strong>on</strong>allevel of the father or mother was not a risk factor fordrowning mortality (55).Within countries, social and demographic factors alsoappear to affect the risk of drowning. Evidence from <strong>child</strong>drowning studies in low-income and middle-incomecountries such as China (6, 11, 55) Uganda (24) andBangladesh (9, 12) c<strong>on</strong>sistently show that rural <strong>child</strong>renhave much higher drowning rates than those in urban areas.Many of these deaths occur in fishing communities wherewater transport takes place in n<strong>on</strong>-motorized watercraft(49). In Bangladesh, the annual drowning rates in <strong>child</strong>renaged 1–4 years are 136.9 per 100 000 in rural areas and 18.9per 100 000 in urban areas (7, 9, 12). Case-c<strong>on</strong>trol studiesc<strong>on</strong>ducted in this country (9, 12) also found that <strong>child</strong>drowning risk increased as maternal age and family sizeincreased. This pattern, though, was not observed in thestudy of <strong>child</strong> drowning in Xiamen, China (55).Within high-income countries, there are suggesti<strong>on</strong>sof large discrepancies in fatal drowning rates betweenpopulati<strong>on</strong> subgroups, with an increased risk of betweentwo and four times for <strong>child</strong>ren and young people fromracial or ethnic minority groups (13, 56, 57). In the UnitedStates, ethnic minorities and foreign-born young menhave higher rates of drowning compared with their whitecounterparts (56, 58). In the Netherlands, ethnic minoritiesexperience a nearly three-fold higher risk of drowningdeath than the native Dutch populati<strong>on</strong> (57). The factorsthat c<strong>on</strong>tribute to disparities in risk of drowning am<strong>on</strong>gdifferent ethnic groups are not well understood. Suggestedexplanati<strong>on</strong>s include differences in swimming ability andexperience in the water, lack of opportunities to learn toswim, and lack of supervisi<strong>on</strong> in envir<strong>on</strong>ments wherepopulati<strong>on</strong> groups are at high-risk swim (58, 59).Underlying c<strong>on</strong>diti<strong>on</strong>sEpilepsy is known to increase the risk of drowning deathin all sources of water, including baths, swimming pools,p<strong>on</strong>ds and other natural bodies of water (60, 61). A casec<strong>on</strong>trolstudy c<strong>on</strong>ducted in Norway found that <strong>child</strong>renwith epilepsy were significantly more at risk of submersi<strong>on</strong>and drowning than <strong>child</strong>ren who did not have epilepsy,in both baths and swimming pools (62). In this study,though, it was found that no <strong>child</strong> died of submersi<strong>on</strong>if an adult was present. In Sweden, 10% of those with ahistory of epilepsy died from drowning over the period1975–1995 (63). Other c<strong>on</strong>diti<strong>on</strong>s that are likely to increasethe risk of drowning are autism (22, 64) and certaincardiac arrhythmias, although the latter are less frequentin <strong>child</strong>ren (65).Agent factorsLack of safety equipmentThe lack of availability or accessibility of safety equipmentin water transportati<strong>on</strong> vessels are additi<strong>on</strong>al risk factors.Flotati<strong>on</strong> devices such as life jackets are indispensable<strong>on</strong> all vessels, whether used for transportati<strong>on</strong> or forpleasure. In the United States, for example, in 2005 theCoast Guard received <str<strong>on</strong>g>report</str<strong>on</strong>g>s for 4969 boating incidents.In these incidents, 3451 participants were <str<strong>on</strong>g>report</str<strong>on</strong>g>ed injuredand 697 died. Am<strong>on</strong>g those who drowned, 87% were notwearing life jackets (66). In additi<strong>on</strong> to the lack of flotati<strong>on</strong>devices, the poor maintenance of such equipment is anadditi<strong>on</strong>al risk.Safety equipment used by <strong>child</strong>ren while swimmingshould meet minimum safety standards. Items such assupporting rings or “water wings” may give parents afalse feeling of safety, resulting in lapses in supervisi<strong>on</strong>with devastating c<strong>on</strong>sequences. The use of blow-up toys,rafts and air mattresses has also been recognized as beingunsafe (67).Unsafe vessels <strong>on</strong> waterThere are regular media <str<strong>on</strong>g>report</str<strong>on</strong>g>s of the deaths of adultsand <strong>child</strong>ren as a result of being transported in unsafe orovercrowded boats. Many of these boats are unseaworthyand will have been further compromised by turbulentweather c<strong>on</strong>diti<strong>on</strong>s. These incidents account for unknownnumbers of drowning deaths every year. In low-incomecountries, the capsizing of boats, launches and ferries issadly comm<strong>on</strong>place, especially during the rainy seas<strong>on</strong>and at periods, such as nati<strong>on</strong>al holidays, when there arehigh levels of mobility.Alcohol c<strong>on</strong>sumpti<strong>on</strong>Risk-taking behaviour figures str<strong>on</strong>gly in unintenti<strong>on</strong>aldrowning cases, particularly am<strong>on</strong>g adolescents. Alcoholuse has been linked to between 25% and 50% of adolescentand adult deaths associated with water recreati<strong>on</strong>(68). Alcohol influences balance, coordinati<strong>on</strong> andjudgement, and its effects are heightened by exposure tothe sun and heat (69). Alcohol c<strong>on</strong>sumpti<strong>on</strong> by parentsand other caretakers while supervising <strong>child</strong>ren inwater should also be c<strong>on</strong>sidered. While many studieshave investigated the direct c<strong>on</strong>tributi<strong>on</strong> of alcohol todrowning, little work has been d<strong>on</strong>e to estimate the riskto <strong>child</strong>ren of alcohol c<strong>on</strong>sumpti<strong>on</strong> by those supervisingthem (40).Estimates of the extent of alcohol involvement indrowning vary widely. This is because of differences inrecording age groups or incomplete testing. Apart fromaffecting judgement and performance, alcohol is believedto have direct physiological effects that may affect survival<strong>on</strong>ce submersi<strong>on</strong> has occurred – through mechanisms suchas increasing hypothermia and retarding the protectiveWORLD REPORT ON CHILD INJURY PREVENTION 65
involuntary muscular c<strong>on</strong>tracti<strong>on</strong> of the laryngeal cords(70).Envir<strong>on</strong>mental factorsType of body of waterPerhaps the str<strong>on</strong>gest risk factor for <strong>child</strong> drowningmortality is exposure to a “risky” body of water.Patterns of <strong>child</strong> drowning across countries generallyreflect the type of water to which the <strong>child</strong> is exposed.In low-income and middle-income countries, mostdrowning deaths happen during daily activities thatinvolve playing, working, washing, collecting water andcrossing water – for instance, to reach school. The bodiesof water involved include p<strong>on</strong>ds, ditches, lakes, riversand water collecting systems, both above and belowground, such as buckets, barrels, wells and cisterns (24,54, 71). By c<strong>on</strong>trast, in high-income countries, most<strong>child</strong>hood drowning occurs in recreati<strong>on</strong>al settings. Foryounger <strong>child</strong>ren this is often a swimming pool and forolder <strong>child</strong>ren a lake or river used for swimming. Whileapproaches to preventi<strong>on</strong> are transferable, specificpreventi<strong>on</strong> strategies and measures should be tailoredfor specific types of exposure.In general, most <strong>child</strong>ren drown in or around the home.The younger the <strong>child</strong>, the closer to home the event islikely to occur. Baths are a very comm<strong>on</strong> locati<strong>on</strong>, though<strong>child</strong>ren mostly drown in them <strong>on</strong>ly when left unattended(72). For young <strong>child</strong>ren in high-income countries, thepresence of a residential pool, particularly <strong>on</strong>e that isinadequately fenced, is the str<strong>on</strong>gest exposure factor (51),while in many low-income countries, the presence ofopen bodies of water or a well is str<strong>on</strong>gly related to therisk of drowning. For instance, a study in a metropolitanarea of Mexico found that <strong>child</strong>ren living in homes with awell experienced a seven-fold increased risk of drowningas compared with those in homes without a well (54). InBangladesh, most young <strong>child</strong>ren aged 12–23 m<strong>on</strong>thswho died from drowning did so in ditches and p<strong>on</strong>ds,reflecting the fact that they were highly exposed to thesewater sources (71). A study of Australian farm injuriesfound that 78% of drownings in <strong>child</strong>ren under 5 years ofage living <strong>on</strong> farms occurred in farm dams and irrigati<strong>on</strong>channels (73).Climate<str<strong>on</strong>g>World</str<strong>on</strong>g>wide, large numbers of drowning deaths areassociated with cataclysmic floods and ocean waves, which,in a single event, can leave thousands dead. Childrenaccounted for about <strong>on</strong>e third of those who died duringthe Indian Ocean tsunami in 2004 (74).Holiday activitiesA number of studies have found an increased risk of fataldrowning am<strong>on</strong>g both adults and <strong>child</strong>ren <strong>on</strong> holiday intheir own country or abroad. In Australia, between 1992and 1997, 4.7% of all n<strong>on</strong>-boating drowning cases, 18% ofsurf and ocean drowning cases and 25% of scuba drowningcases were am<strong>on</strong>g foreigners (75). Another Australianstudy, covering the period mid-2001 to mid-2005, showedthat almost 25% of drowning deaths were am<strong>on</strong>g foreigntourists, including <strong>child</strong>ren (76). It has been <str<strong>on</strong>g>report</str<strong>on</strong>g>ed thatmany more <strong>child</strong>ren from the United Kingdom drown inswimming pools abroad than in swimming pools in theirhome country. This finding is presumably related bothto the increased exposure to water when <strong>on</strong> holiday andexposure to a new situati<strong>on</strong> (77).Access to treatment and rehabilitati<strong>on</strong>Several studies have c<strong>on</strong>firmed that most lives are saved bythe immediate acti<strong>on</strong> of bystanders at the scene, either laypeople or professi<strong>on</strong>al rescuers. Without such immediatefirst aid – including basic cardiopulm<strong>on</strong>ary resuscitati<strong>on</strong> –subsequent advanced and invasive life support techniquesappear to be of little value in most cases (78).Following the initial attempts at resuscitati<strong>on</strong>, rapiddeployment to an emergency department of a hospitalis essential to prevent further neurological damage ordeath. The initial management of n<strong>on</strong>-fatal drowningshould involve c<strong>on</strong>tinued resuscitati<strong>on</strong> and treatmentof respiratory failure, after which the <strong>child</strong> should begradually rewarmed.Outcome studies have shown that submersi<strong>on</strong> for l<strong>on</strong>gerthan 25 minutes, a c<strong>on</strong>tinued need for cardiopulm<strong>on</strong>aryresuscitati<strong>on</strong> for more than 25 minutes, and lack of pulses<strong>on</strong> arrival at the emergency room are all predictors ofsevere l<strong>on</strong>g-term neurological c<strong>on</strong>sequences or death(1, 79, 80). However, the existence of case <str<strong>on</strong>g>report</str<strong>on</strong>g>s of<strong>child</strong>ren surviving neurologically intact after prol<strong>on</strong>gedsubmersi<strong>on</strong> in icy water suggests that more aggressiveinterventi<strong>on</strong>s can be helpful in these cases (1).Interventi<strong>on</strong>sGiven the complexity of drowning events, strategiesfor preventi<strong>on</strong> require a holistic approach, based <strong>on</strong>the particular pattern of drowning observed in a givenlocati<strong>on</strong>. Passive preventi<strong>on</strong> strategies – such as improvingsafety design – that require no acti<strong>on</strong> or else <strong>on</strong>ly a singleacti<strong>on</strong> <strong>on</strong> the part of the individual, are generally regardedas more effective than active strategies, such as adoptingsafer behaviours, requiring repeated acti<strong>on</strong>s. However, formany types of drowning there are a limited number ofpassive strategies – or even n<strong>on</strong>e at all.Most drowning deaths could be prevented by a sustained effortto implement safety interventi<strong>on</strong>s. The task ahead is clear - totranslate what is now known into acti<strong>on</strong> <strong>on</strong> the ground (UNICEFBangladesh).66 WORLD REPORT ON CHILD INJURY PREVENTION
Engineering measuresEliminating hazardsEliminating a hazard – where this is possible – is themost effective preventi<strong>on</strong> method, since it does not rely<strong>on</strong> barriers or other protective measures which may beineffective. Buckets and baths, for example, should be leftempty when not in use, as <strong>child</strong>ren could drown in themif they c<strong>on</strong>tained a liquid. Similarly, holes in the ground,dug for building purposes, should be drained of rainwateror filled in to prevent water collecting. Small c<strong>on</strong>tainers,such as washing tubs, should be safely stored so that theywill not fill with rainwater (81).Passive strategies relating to the creati<strong>on</strong> of infrastructureinclude the building of safe bridges and theinstallati<strong>on</strong> of piped water systems, both of which havehistorically been factors in reducing drowning rates indeveloping countries. Having piped water to hand meansthat people can avoid open bodies of water to bathe orwash clothes in or to collect drinking water from. It alsomakes exposure to stored rainwater and wells less likely,both of which are potential hazards (81).Providing safe venues for recreati<strong>on</strong>al swimming canalso help prevent drowning. Natural bodies of waterc<strong>on</strong>tain a number of associated hazards for swimmers. Thedepth of water in them may be unknown and there may beunderwater obstacles, sudden and unseen changes of depthor deep holes. Str<strong>on</strong>g currents and a low temperature ofwater can create further problems. The provisi<strong>on</strong> of suitablydesigned pools, whose depth is known at each point and inwhich obstacles and currents are absent, makes it possiblefor <strong>child</strong>ren to learn to swim in an envir<strong>on</strong>ment withc<strong>on</strong>siderably fewer hazards.Envir<strong>on</strong>mental measuresPool fencingAnother passive interventi<strong>on</strong> is the creati<strong>on</strong> of an effectivebarrier between <strong>child</strong> and hazard (see Box 3.1). In highincomecountries it has been found that surroundingprivate swimming pools and spas with safety barriersthat prevent unsupervised young <strong>child</strong>ren enteringsignificantly reduces their risk of drowning (82–86). Ameta-analysis of three case–c<strong>on</strong>trol studies showed asignificantly decreased risk of drowning in a fenced pool,as compared to an unfenced <strong>on</strong>e (87). Furthermore, thestudy found that a barrier isolating the pool from all otherstructures – a four-sided fence – was shown to be far moreprotective than perimeter fencing, a three-sided fencewhere the house or another structure forms the fourth sideof the barrier (87).Research in the United States and Australia has found thatlaws and regulati<strong>on</strong>s requiring pool fencing are insufficientif perimeter fencing is not accompanied by adequateenforcement to ensure the self-closing system of the gate andthe latching system are functi<strong>on</strong>ing properly (83, 88).Covering wellsIn low-income and middle-income countries, creatingbarriers between young <strong>child</strong>ren and the bodies of waterto which they are exposed can be an effective measureto prevent drowning. Covering wells or open barrelswith grills, creating an embankment or fenced barriernear p<strong>on</strong>ds and riverbanks, and building flood-c<strong>on</strong>trolembankments, are all effective in preventing drowning(54) (see Box 3.1). Similarly, creating fencing around adwelling where there is a hazard of open water outside thehouse can also provide protecti<strong>on</strong>.© M. Peden/WHOBOX 3.1Covering wells in MexicoWells and underground cisterns are important sources of householdwater. The former are comm<strong>on</strong> in rural areas, while the latter areused in some cities without a reliable community water source. Acomm<strong>on</strong> characteristic of both is an opening large enough to allowaccess. This can create a major drowning risk for <strong>child</strong>ren, especiallyin developing countries. One study found that the presence of wellsin homes increased the risk of drowning in the home by a factor ofnearly seven, while cisterns increased the risk two-fold (54).Using accepted strategies as well as the experience of swimmingpool fencing, a <strong>child</strong>’s risk of drowning could be substantially reducedif the opening to these household water sources was closed by a lockedhatch. This preventive strategy is familiar to the Mexican public, whohave a popular saying, “close the well after the drowned <strong>child</strong>.”Because water must be drawn daily, wells and underground cisternscannot be sealed the whole time. The most hazardous methodof obtaining water would be through a hatch or lid large enough to admita bucket – and therefore also large enough to let a small <strong>child</strong> passthrough. A more effective preventive measure would be to draw waterusing a manual or electric pump. This would make it easier to obtainhousehold water and would eliminate the risk of <strong>child</strong>ren drowning.WORLD REPORT ON CHILD INJURY PREVENTION 67
In Australia, farm safety researchers are investigating thefeasibility of a “virtual fence”. The technology for an alarmsystem signalling that a <strong>child</strong> under adult supervisi<strong>on</strong> haswandered bey<strong>on</strong>d predetermined limits from the homealready exists. The researchers are examining whetherthis technology can be applied effectively to increase <strong>child</strong>safety in low-income countries, especially in relati<strong>on</strong> tothe risk of drowning in bodies of water such as dams.Legislati<strong>on</strong> and standardsPool fencing laws and their enforcementIn many high-income countries, legislati<strong>on</strong> requiringisolati<strong>on</strong> pool fencing for all swimming pools (includingprivate <strong>on</strong>es) has been recommended and sometimes alsoenacted and enforced. Such legislati<strong>on</strong> has proved effectivein decreasing drowning rates, though not to the extent thathad been anticipated (86, 89, 90). This may be due to a lackof knowledge of the law and its inadequate enforcement.Pers<strong>on</strong>al flotati<strong>on</strong> devicesAlthough not yet thoroughly evaluated, wearing aproperly-fitted pers<strong>on</strong>al flotati<strong>on</strong> device, such as a lifejacket, is a promising strategy to prevent drowning (91).This is particularly the case with regard to swimmerswho are unskilled or tired or who panic. If a young <strong>child</strong>wearing a properly-designed pers<strong>on</strong>al flotati<strong>on</strong> devicefalls into the water, the device should keep the <strong>child</strong>afloat l<strong>on</strong>g enough to be rescued. Only certain types ofpers<strong>on</strong>al flotati<strong>on</strong> device will ensure that the <strong>child</strong> floatsface-up. These devices should therefore be seen as shorttermsoluti<strong>on</strong>s and not as a substitute for supervisi<strong>on</strong>. Theprovisi<strong>on</strong> of pers<strong>on</strong>al flotati<strong>on</strong> devices for all occupantsof ferries and other vessels has the potential to save manylives (see Box 3.2).Laws <strong>on</strong> alcoholGeneral minimum-age drinking laws and loweringthe alcohol level do not appear to be associated with areducti<strong>on</strong> in drowning rates am<strong>on</strong>g adolescents (96).However, it is known that c<strong>on</strong>suming alcohol before orduring activities in bodies of water increases the risk ofdrowning. Adolescents should therefore be encouragednot to drink and swim. In additi<strong>on</strong>, advertising thatencourages alcohol use during boating and the saleof alcohol at water recreati<strong>on</strong>al facilities should berestricted.BOX 3.2Pers<strong>on</strong>al flotati<strong>on</strong> devices and drowningLifejackets were developed to prevent drowning in emergencies at sea. In the water, they turn wearers to a positi<strong>on</strong> where the face points up, andwith the head supported and the mouth out of the water. Buoyancy material is c<strong>on</strong>centrated in fr<strong>on</strong>t of the wearer, which makes the jacket bulky,uncomfortable and restrictive. Newer buoyancy devices are designed to keep the wearer afloat but do not meet the high performance requirementsfor lifejackets, with regard to buoyancy and keeping the face up. They are c<strong>on</strong>sidered appropriate, though, for use by <strong>child</strong>ren, recreati<strong>on</strong>al boatersand water sports participants, who are undertaking activities in calm waters, close to the shore or close to help from rescuers.The broader term “pers<strong>on</strong>al flotati<strong>on</strong> device” is now used in many countries to cover all these new flotati<strong>on</strong> devices as well as the lifejacket. Manygovernments now require all recreati<strong>on</strong>al vessels to carry <strong>on</strong>e wearable pers<strong>on</strong>al flotati<strong>on</strong> device, of a specified type, for each pers<strong>on</strong> <strong>on</strong> board. However,since drowning during recreati<strong>on</strong>al boating usually occurs suddenly or unexpectedly, lifejackets stored <strong>on</strong> board offer little protecti<strong>on</strong> unlessthey are actually worn. Various studies have shown that up to 50% of drownings resulting from boating-related incidents could have been preventedif the pers<strong>on</strong> had been wearing an appropriate pers<strong>on</strong>al flotati<strong>on</strong> device (92).Two main strategies – educati<strong>on</strong> and, to a lesser extent, regulati<strong>on</strong>– have been employed by governments to try to increase the wearing ofpers<strong>on</strong>al flotati<strong>on</strong> devices am<strong>on</strong>g recreati<strong>on</strong>al boaters, including watersports participants. Only two evaluati<strong>on</strong>s of educati<strong>on</strong>al campaigns <strong>on</strong>pers<strong>on</strong>al flotati<strong>on</strong> devices have been published, both <str<strong>on</strong>g>report</str<strong>on</strong>g>ing modest effectiveness(93, 94). Although the use of pers<strong>on</strong>al flotati<strong>on</strong> devices am<strong>on</strong>gall boaters increased, the impact of the campaign <strong>on</strong> <strong>child</strong>hood drowningwas undetermined.Some countries have made the wearing of pers<strong>on</strong>al flotati<strong>on</strong> devicesmandatory. Preliminary data from an Australian study, which evaluatesboth the wearing rates and the effectiveness of regulati<strong>on</strong>s, shows promisingresults (95).The available evidence therefore suggests that the use of pers<strong>on</strong>al flotati<strong>on</strong>devices is potentially a str<strong>on</strong>g measure to prevent drowning am<strong>on</strong>grecreati<strong>on</strong>al boaters, including <strong>child</strong>ren, and that regulati<strong>on</strong> is more effectivethan educati<strong>on</strong> in increasing the use of these devices and preventingdrowning.© Marine Safety Victoria68 WORLD REPORT ON CHILD INJURY PREVENTION
Developing educati<strong>on</strong> and skillsTeaching swimming and improving skillsMost studies show that swimming instructi<strong>on</strong> improvesswimming ability, but no c<strong>on</strong>clusive evidence exists thatswimming ability c<strong>on</strong>fers protecti<strong>on</strong> against the risk ofdrowning. There are, however, indicati<strong>on</strong>s that swimminginstructi<strong>on</strong> and the c<strong>on</strong>sequent increased ability atswimming, as well as greater survival skills, do providesome protecti<strong>on</strong>, even at relatively young ages.L<strong>on</strong>gitudinal studies of <strong>child</strong> drowning are hamperedby the lack of data regarding the proporti<strong>on</strong> of <strong>child</strong>renwho can swim and the level of swimming ability of thosewho drown. A study c<strong>on</strong>ducted in the United States (seeBox 3.3), a recent study in rural China of <strong>child</strong> drowning(46) and research in Bangladesh (7) all suggest thatswimming less<strong>on</strong>s may be protective.Even in the face of this preliminary evidence, thereshould be cauti<strong>on</strong> in recommending swimming less<strong>on</strong>s asa protective strategy for young <strong>child</strong>ren. Several studiesshow <strong>child</strong>ren as young as 24 m<strong>on</strong>ths can improve theirskills, but their learning period is much l<strong>on</strong>ger than thatof older <strong>child</strong>ren (98).C<strong>on</strong>cern has been voiced that mass training inswimming skills for <strong>child</strong>ren could lead to more<strong>child</strong>ren, especially young <strong>on</strong>es, being exposed to waterand becoming overc<strong>on</strong>fident in it. Ultimately, accordingto this view, drowning rates in <strong>child</strong>ren could increaserather than decrease (99). A study in Australia, however,suggested a link between swimming less<strong>on</strong>s and decreaseddrowning rates in <strong>child</strong>ren (100). However, this may havealso been because more safe places for swimming wereopened, including large numbers of public pools (seeBox 3.4).BOX 3.3Teaching <strong>child</strong>ren to swimOne possible strategy to prevent drowning is to improve <strong>child</strong>ren’s swimming skills through formal instructi<strong>on</strong>. Few studies have examined theassociati<strong>on</strong> between either swimming skills or swimming instructi<strong>on</strong> and drowning risk. While it seems intuitive that more skilled swimmers wouldbe less likely to drown, it is also the case that skilled swimmers drown. Am<strong>on</strong>g older <strong>child</strong>ren especially, it is possible that those who are comfortablein water or who perceive themselves to be good swimmers might seek out water-related activities. These activities might occur in more risky settings– such as in deeper water or at locati<strong>on</strong>s without lifeguards or other appropriate supervisi<strong>on</strong>.Preliminary results of a study in the United States (97) found that past participati<strong>on</strong> in formal swimming less<strong>on</strong>s offered a protective effect fordrowning. In this study, the families of <strong>child</strong>ren who had drowned and the families of matched c<strong>on</strong>trols were asked about their <strong>child</strong>’s past participati<strong>on</strong>in formal swimming less<strong>on</strong>s. For <strong>child</strong>ren aged 1–4 years, interviews were c<strong>on</strong>ducted with 61 families of <strong>child</strong>ren who had drowned andthe families of 134 matched c<strong>on</strong>trols. In the 5–19-year age group, interviews were c<strong>on</strong>ducted with 27 families of drowning cases and 79 matchedc<strong>on</strong>trols.For the younger age group, 3% of those who drowned had participated in formal swimming less<strong>on</strong>s, against 26% in the matched c<strong>on</strong>trols. Thisrepresents a 90% reducti<strong>on</strong> in drowning risk am<strong>on</strong>g those who had swimming less<strong>on</strong>s. Am<strong>on</strong>g older <strong>child</strong>ren, 27% of the drowning cases had takenformal swimming less<strong>on</strong>s against 53% of the c<strong>on</strong>trols – an associati<strong>on</strong> that was not statistically significant.In general, increased swimming skills also appear protective with respect to drowning risk. This is particularly true in <strong>child</strong>ren over 5 years ofage, with several of the skills showing a protective effect in adjusted analyses, despite the small sample size. For example, in the older age group,drowning cases were less likely to be able to swim <strong>on</strong> the stomach for a distance of 5 metres. However, am<strong>on</strong>g those aged 5–19 years, many of thosewho drowned were relatively skilled swimmers. Of those who drowned in this group, 58% were <str<strong>on</strong>g>report</str<strong>on</strong>g>ed to be able to swim c<strong>on</strong>tinuously for at leasta minute and 48% to be able to swim at least 15 metres.This study had a number of limitati<strong>on</strong>s, including the relatively smallsample sizes in both age groups and a reliance <strong>on</strong> <str<strong>on</strong>g>report</str<strong>on</strong>g>s, rather than <strong>on</strong>observati<strong>on</strong>, of swimming skills. In additi<strong>on</strong>, it is quite possible that parentswho enroll young <strong>child</strong>ren in swimming less<strong>on</strong>s could differ fromparents who do not do so. These differences are difficult to measure andcould have an effect <strong>on</strong> a <strong>child</strong>’s risk of drowning.In spite of these shortcomings, these early results, together with a previousstudy in rural China (46) that also identified a protective associati<strong>on</strong>between swimming instructi<strong>on</strong> and drowning risk, suggest that formalinstructi<strong>on</strong> in swimming ought to be a comp<strong>on</strong>ent of a strategy to preventdrowning. However, those designing preventi<strong>on</strong> programmes, and thosetargeted by them, must be aware that even the most skilled swimmers candrown. Swimming less<strong>on</strong>s and the teaching of water survival skills shouldtherefore be regarded as <strong>on</strong>e important comp<strong>on</strong>ent of a multiple approachto preventi<strong>on</strong>.© Naser UNICEFWORLD REPORT ON CHILD INJURY PREVENTION 69
More good interventi<strong>on</strong> studies are needed to evaluatethe effectiveness of swimming less<strong>on</strong>s in preventingdrowning in young <strong>child</strong>ren, and to specify what sort ofswimming and survival skills should be taught. Impartingknowledge and skills bey<strong>on</strong>d the basic swimming strokesis certainly necessary. This includes teaching <strong>child</strong>rento swim safely in open water, to identify hazards such asrocks, currents and dangerous weather c<strong>on</strong>diti<strong>on</strong>s, andto recognize, avoid and – if necessary – escape from ripcurrents.Supervisi<strong>on</strong> by lifeguardsLifeguards (also known in Australia, New Zealand andSouth Africa as lifesavers) – both voluntary and paid– have provided protecti<strong>on</strong> at swimming pools andnatural bodies of water in various parts of the worldsince the 19th century. Voluntary lifeguarding still exists,particularly around natural bodies of water. At the sametime, paid lifeguards are increasingly being employed inpublic and commercial swimming venues.There have been no published studies formallyevaluating the effectiveness of lifeguarding as a primarypreventi<strong>on</strong> measure. Australian studies, based <strong>on</strong> rescueand resuscitati<strong>on</strong> data from associati<strong>on</strong>s of lifeguards, do,however, point to some effectiveness (101, 102). Trainedlifeguards <strong>on</strong> beaches and at public swimming pools arelikely to decrease the risk of drowning by being models forsafe behaviour, actively c<strong>on</strong>trolling the risk-taking acti<strong>on</strong>sof swimmers, m<strong>on</strong>itoring water and weather c<strong>on</strong>diti<strong>on</strong>s,and prohibiting or restricting swimming in the seaif behaviour or c<strong>on</strong>diti<strong>on</strong>s pose a hazard. Lifeguards,furthermore, provide rescue and resuscitati<strong>on</strong> to limitcases of drowning resulting in death or brain damage(103). For their work to be effective, though, they require<strong>on</strong>going training and need to adhere to high standards ofperformance, particularly as regards surveillance (104).Supervisi<strong>on</strong> by parent or caregiverEducating parents and caregivers about the risks fordrowning is an important step for changing knowledge,beliefs and attitudes which in turn determine behaviour.People often underestimate the risk of drowning andare unaware of who is particularly at risk (6). A study ofAmericans of Vietnamese origin found that both parentsand adolescents often attributed drowning to fate (105).Parents and caregivers need to understand that young<strong>child</strong>ren should never be left al<strong>on</strong>e or with another young<strong>child</strong> in or around any body of water (see Box 3.5). Theyalso need to learn basic life-saving and first-aid skills.Numerous studies have shown that inadequatesupervisi<strong>on</strong> is an important c<strong>on</strong>tributory factor forpaediatric drowning of all types, especially drowning inthe bath (106). However, the effectiveness of supervisi<strong>on</strong>as a drowning preventi<strong>on</strong> measure has not been formallyBOX 3.4A mass primary school swimming instructi<strong>on</strong> campaignFrom the 1950s <strong>on</strong>wards, a major collaborative swimming instructi<strong>on</strong> campaign was implemented across the state of Victoria, Australia. The programmewas named after a daily newspaper, The Herald, which had launched it and gave it publicity. Supported by the Educati<strong>on</strong> Department and thelocal government and champi<strong>on</strong>ed by an ex-olympic swimmer, the campaign also coincided with the Olympic Games held in Melbourne in 1956.The campaign was aimed at the later years of primary school <strong>child</strong>ren. These <strong>child</strong>ren received a “Herald Certificate” when they swam thetarget distance of 23 metres, and the annual award rates were published by the newspaper. By the summer of 1962–63, over a milli<strong>on</strong> <strong>child</strong>renhad participated in the Herald campaign. All <strong>child</strong>ren aged 10–12 years were covered by this programme, which was associated with a reducti<strong>on</strong> inthe drowning rate. This mass swimming campaign, together with an increase in the number of safe places to swim and other drowning preventi<strong>on</strong>strategies, resulted in a significant reducti<strong>on</strong> in the drowning rate (see accompanying figure).Number of certificates awarded90 00080 00070 00060 00050 00040 00030 00020 00010 0000CertificatesRatesP# # # # # # P#1935 1937 1939 1941 1943 1945 1947 1949 1951 1953 1955 1957 1959 1961 19639876543210Drowning deaths per 100 000 populati<strong>on</strong>Year70 WORLD REPORT ON CHILD INJURY PREVENTION
BOX 3.5Adult supervisi<strong>on</strong> and swimmingtraining for very young <strong>child</strong>renIn New Zealand, <strong>child</strong>ren under five years of age have the highestdeath rate from drowning of any age group in the country. In an attemptto prevent such deaths, a number of organizati<strong>on</strong>s have promotedswimming less<strong>on</strong>s for very young <strong>child</strong>ren, despite a lack ofevidence that swimming instructi<strong>on</strong> in this age group is effective inteaching protective skills. Some experts have warned that swimmingless<strong>on</strong>s at this age may actually be harmful, making young <strong>child</strong>renless fearful of water and giving parents a false sense of security. Astudy to examine the beliefs of adults about the benefit of swimminginstructi<strong>on</strong> was c<strong>on</strong>ducted, with 555 parents who had enrolledtheir preschool <strong>child</strong>ren in swimming less<strong>on</strong>s, together with ac<strong>on</strong>trol group of 327 parents of similar <strong>child</strong>ren who had not (107).The study found that parents believed that <strong>child</strong>ren as young as twoyears could learn to swim, and that a sizable proporti<strong>on</strong> thoughtthat swimming classes were the best way to prevent small <strong>child</strong>renfrom drowning. A third of parents c<strong>on</strong>sidered it better to develop theswimming ability of their <strong>child</strong>ren than to rely <strong>on</strong> adult supervisi<strong>on</strong>in order to prevent drowning.The study brought out parents’ misc<strong>on</strong>cepti<strong>on</strong>s over their young<strong>child</strong>ren’s ability to be safe. Parents often place their <strong>child</strong>ren in situati<strong>on</strong>swhere there is a mismatch between the <strong>child</strong>’s skills <strong>on</strong> the<strong>on</strong>e hand, and the demands of the tasks required for safety <strong>on</strong> theother. This has been shown not <strong>on</strong>ly for drowning, but also for pedestriansafety, driving skills and safety with firearms. Such misc<strong>on</strong>cepti<strong>on</strong>sneed be combatted with a range of educati<strong>on</strong>al, regulatoryand other interventi<strong>on</strong>s so as to reduce the risk of inadvertent <strong>injury</strong>to <strong>child</strong>ren.evaluated. What c<strong>on</strong>stitutes adequate adult supervisi<strong>on</strong> forbathing and water safety has <strong>on</strong>ly recently been studied.Those who supervise <strong>child</strong>ren in and around water shouldreceive appropriate training in rescue and resuscitati<strong>on</strong>skills.Infants and other <strong>child</strong>ren who lack mobility requirec<strong>on</strong>tinuous supervisi<strong>on</strong> <strong>on</strong> the site while in the bath. Theage up to which <strong>child</strong>ren need such supervisi<strong>on</strong> has notbeen determined but is likely to extend to at least fiveyears. Bey<strong>on</strong>d this age, <str<strong>on</strong>g>report</str<strong>on</strong>g>ed drownings in a bath arealmost always related to seizures (62). For <strong>child</strong>ren andadolescents with epilepsy, being in a bath poses the highestrisk for unintenti<strong>on</strong>al death. Children with epilepsyshould therefore always use a shower rather than a bathand adhere strictly to other seizure c<strong>on</strong>trol measures (62).In some communities it is comm<strong>on</strong> to rely <strong>on</strong> other<strong>child</strong>ren of the same age or older to protect a young <strong>child</strong>.In the case of drowning, such a form of care appears toprovide insufficient protecti<strong>on</strong>. A historical review ofdrowning in Australia found that throughout the 19thand 20th centuries many <strong>child</strong> drowning deaths occurredin the company of other <strong>child</strong>ren (81). Because drowninghappens rapidly, compani<strong>on</strong>s are often unable to rescuethe drowning <strong>child</strong> and may themselves drown in theprocess.Interventi<strong>on</strong>s for adolescentsAdolescent drowning usually occurs in open water whileswimming, boating or undertaking other leisure activities.Those who drown have generally been swimming with <strong>on</strong>eor more friends of a similar age who do not recognize theyare in trouble or cannot rescue them. Adults are usuallyabsent, and there may be peer pressure to indulge in riskbehaviours, such as c<strong>on</strong>suming alcohol. With alcoholc<strong>on</strong>sumpti<strong>on</strong>, the risk of drowning increases as bloodalcohol c<strong>on</strong>centrati<strong>on</strong> levels rise. Measures to preventthe use of alcohol and recreati<strong>on</strong>al drugs around wateractivities are therefore likely to reduce the rate of adolescentdrownings (108, 109).From early adolescence <strong>on</strong>wards, preventiveinterventi<strong>on</strong>s for drowning should increase a pers<strong>on</strong>’scognitive skills around water. These skills include:– better recogniti<strong>on</strong> of hazards;– recogniti<strong>on</strong> of pers<strong>on</strong>al limits, including knowledge of<strong>on</strong>e’s swimming ability;– the ability to resist peer pressure to take part in activitiesfor which skills are lacking.Such interventi<strong>on</strong>s, though, have not been properlydeveloped or tested. For <strong>child</strong>ren and adolescents, aparticular problem is to provide safe sites for swimmingthat are also attractive. To this end, trained and equippedlifeguards need to be present at places and at times thatadolescents are most likely to c<strong>on</strong>gregate. In rural areas,safe settings for swimming need to be made available.Otherwise, <strong>child</strong>ren and adolescents are likely to gather atunsafe places such as irrigati<strong>on</strong> ditches, quarries and otheropen water sites.Managing drowningDrowning injuries arise because a pers<strong>on</strong> cannotadequately breathe and obtain oxygen. Even if a pers<strong>on</strong>is quickly retrieved from the water while drowning, theymay have stopped breathing, and suffer brain damageas a result of a lack of oxygen. A sec<strong>on</strong>dary preventi<strong>on</strong>strategy, therefore, for all age groups, is training inresuscitati<strong>on</strong> techniques. The str<strong>on</strong>gest predictor ofoutcome following drowning is the mental status of thepers<strong>on</strong> being rescued (110).Support from bystandersStudies have shown that <strong>child</strong>ren who receive immediateresuscitati<strong>on</strong> from bystanders – before the arrival ofmedical pers<strong>on</strong>nel – have improved outcomes (111, 112).Attempts by bystanders to provide “mouth-to-mouth”resuscitati<strong>on</strong> to the <strong>child</strong> may stimulate the return ofthe <strong>child</strong>’s sp<strong>on</strong>taneous breathing. If the <strong>child</strong> does notbegin to breathe, providing such resuscitati<strong>on</strong> is criticalfor survival. Advanced life support provided by medicalpers<strong>on</strong>nel may save a <strong>child</strong> who has deteriorated to a stateof cardiac arrest. However, even in high-income countriesWORLD REPORT ON CHILD INJURY PREVENTION 71
with local paediatric intensive care facilities, the windowof opportunity for interventi<strong>on</strong> is at the scene of thedrowning (113, 114).Psychosocial supportCoping with a sudden unexpected death, such as occurswith drowning, is always difficult. When the pers<strong>on</strong>in questi<strong>on</strong> is a <strong>child</strong>, the loss is generally even moredevastating and <strong>on</strong>e over which the parents frequentlyexperience feelings of guilt. Childhood death is alsostressful for health care providers. There needs to be greatersupport for families in which a <strong>child</strong>hood drowning hasoccurred, as well as for the health care providers. Greaterattenti<strong>on</strong> should also be devoted to the l<strong>on</strong>g-term careof <strong>child</strong>ren who have become neurologically damagedthrough drowning (78).Adapting interventi<strong>on</strong>sTo maximize their effectiveness, preventi<strong>on</strong> strategies andmeasures against drowning should be appropriate to the<strong>child</strong>’s developmental stage. While a barrier, for example,might be effective in preventing drowning in young<strong>child</strong>ren, this measure is not in general likely to keepolder <strong>child</strong>ren and adolescents from accessing water. Thecultural acceptability to <strong>child</strong>ren and parents of possibleinterventi<strong>on</strong>s also needs to be borne in mind.Affordability and availability are further factors thatmay determine whether interventi<strong>on</strong>s are implemented.Fencing works well for swimming pools, for instance, butit may not be the soluti<strong>on</strong> in regi<strong>on</strong>s where canals andirrigati<strong>on</strong> ditches are ubiquitous.As another examples, items such as pers<strong>on</strong>al flotati<strong>on</strong>devices may not be locally available. Measures to overcomethis obstacle include the setting up of local loan schemesfor such devices.Potentially harmful interventi<strong>on</strong>sBaby bath seats and flexible solar pool covers are notdesigned to prevent drowning, though they are sometimesused for that purpose. Several small studies havedocumented drowning am<strong>on</strong>g infants who were leftunattended in a baby bath seat (115, 116). While in mostcases it was not the bath seat itself that was unsafe, its usetended to make parents feel more comfortable aboutleaving their young <strong>child</strong> unattended. Similarly, flexiblesolar pool covers do not prevent drowning fromoccurring. There have been cases where unsupervised<strong>child</strong>ren drowned, having become trapped in them or hiddenfrom view (117). More rigid, heavier devices may offerprotecti<strong>on</strong>, though these have not been tested for effectivenessand are c<strong>on</strong>siderably more expensive, although theyare sometimes used <strong>on</strong> public swimming pools.Further research <strong>on</strong> interventi<strong>on</strong>sFor all interventi<strong>on</strong>s to prevent drowning, accurateand comprehensive data are vital for evaluating theireffectiveness. Many interventi<strong>on</strong>s still require rigorousevaluati<strong>on</strong>. Above all, the debate around whether <strong>child</strong>renunder the age of five years should be taught to swim needsto be resolved, so that an unequivocal message can begiven to parents. Research is also needed as to why poolfencing laws do not live up to expectati<strong>on</strong>s, includingan examinati<strong>on</strong> of both the knowledge of users as wellas their attitude to newer fencing. For young <strong>child</strong>ren,close supervisi<strong>on</strong> is a vital strategy for preventi<strong>on</strong>. Suchsupervisi<strong>on</strong> includes safe play areas for <strong>child</strong>ren whichhave been proposed but not evaluated (118). What qualifiesas “adequate” supervisi<strong>on</strong>, though, needs defining andevaluating.C<strong>on</strong>clusi<strong>on</strong>s and recommendati<strong>on</strong>sDrowning is a public health issue calling for worldwideattenti<strong>on</strong>. Recent community-based surveys indicate thatthe problem of drowning is likely to be much greater thanpresent global estimates would suggest. This relativelyneglected <strong>injury</strong> problem should be given a much higherpriority by policy-makers and d<strong>on</strong>ors.In 1997, drowning was described as “the final fr<strong>on</strong>tierof <strong>injury</strong> preventi<strong>on</strong>” (119), because of the scarcity ofevidence for the effectiveness of interventi<strong>on</strong> strategies.Since that time, though, a certain amount of progress hasbeen made. This chapter has described the many effectiveand promising interventi<strong>on</strong>s now available to reduce<strong>child</strong>hood drowning (see Table 3.4). More scientificinvestigati<strong>on</strong>, though, is still required to identifysignificant risk and protective factors in drowning.Recommendati<strong>on</strong>s An agenda to address drowning, with targets appropriateto the local situati<strong>on</strong>, should be set up by every country.Because of the high rates of drowning fatalities, the mainfocus needs to be <strong>on</strong> primary preventi<strong>on</strong> strategies. Partnerships between governments, communities,industry, private sector bodies and public healthagencies should be created to address drowning. Whilethe type of strategies to prevent drowning and treat<strong>child</strong>ren and adolescents will vary greatly betweencountries and regi<strong>on</strong>s, cooperative efforts at every level– including at the global level – are essential. To enable countries to compare data and shareexperiences and interventi<strong>on</strong> strategies more effectively(120), the following need to be d<strong>on</strong>e:– the collecti<strong>on</strong> of c<strong>on</strong>sistent epidemiologic data;– the use of standard definiti<strong>on</strong>s;– the use of coding schemes. Further research to evaluate protective factors is urgentlycalled for, using large interventi<strong>on</strong> trials, examiningthe effect of measures such as providing instructi<strong>on</strong> inswimming and survival skills. The design and evaluati<strong>on</strong> of interventi<strong>on</strong>s in specificsettings needs <strong>on</strong>going research.72 WORLD REPORT ON CHILD INJURY PREVENTION
TABLE 3.4Evidence for key strategies to prevent drowning am<strong>on</strong>g <strong>child</strong>renStrategyEffectivePromisingInsufficient evidenceIneffectivePotentially harmfulRemoving (or covering) water hazardsRequiring isolati<strong>on</strong> fencing (4-sided) around swimming poolsWearing pers<strong>on</strong>al flotati<strong>on</strong> devicesEnsuring immediate resuscitati<strong>on</strong>Ensuring the presence of lifeguards at swimming areasC<strong>on</strong>ducting targeted awareness-raising <strong>on</strong> drowningTeaching <strong>child</strong>ren older than 5 years to swimIntroducing laws <strong>on</strong> pool fencingIntroducing a law <strong>on</strong> the use of pers<strong>on</strong>al flotati<strong>on</strong> devicesPromoting drowning preventi<strong>on</strong> through doctorsRestricting access to areas unsafe for swimmingTeaching <strong>child</strong>ren younger than 5 years to swimIntroducing laws <strong>on</strong> blood alcohol c<strong>on</strong>tent for swimmersC<strong>on</strong>ducting preventi<strong>on</strong> campaigns, such as <strong>on</strong> advertising hoardings, for drowningPromoting solar pool covers aUsing baby bath seats aaThese are not primarily designed as drowning preventi<strong>on</strong> interventi<strong>on</strong>s.Source: references 121, 122. Proven interventi<strong>on</strong>s should be implemented wheretheir relevance has been dem<strong>on</strong>strated. These include:– the eliminati<strong>on</strong> of water hazards;– the creati<strong>on</strong> of barriers between <strong>child</strong>ren andhazards;– the use by <strong>child</strong>ren of pers<strong>on</strong>al flotati<strong>on</strong> devices. Immediate resuscitati<strong>on</strong>, prior to the arrival ofparamedical pers<strong>on</strong>nel, should be promotedeverywhere. Such resuscitati<strong>on</strong> significantly increasesthe likelihood of a good outcome – irrespective of age,gender, durati<strong>on</strong> of submersi<strong>on</strong> or the presence ofhypothermia.References1. Idris AH et al. Recommended guideline for uniform<str<strong>on</strong>g>report</str<strong>on</strong>g>ing of data from drowning: the “Utstein style”.Resuscitati<strong>on</strong>, 2003, 59:45–57.2. Van Beeck EF et al. A new definiti<strong>on</strong> of drowning: towardsdocumentati<strong>on</strong> and preventi<strong>on</strong> of a global public healthproblem. Bulletin of the <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2005,83:853–856.3. Cass DT, Ross F, Lam LT. Childhood drowning in NewSouth Wales 1990–1995: a populati<strong>on</strong>-based study. TheMedical Journal of Australia, 1996, 165:610–612.4. Brenner RA, Smith GS, Overpeck MD. Divergent trends in<strong>child</strong>hood drowning rates, 1971 through 1988. Journal ofthe American Medical Associati<strong>on</strong>, 1994, 271:1606–1608.“C<strong>on</strong>sidering that drowing is the sec<strong>on</strong>d leading cause of unintenti<strong>on</strong>al<strong>injury</strong> death worldwide and the single leading cause of <strong>child</strong> death (includingdisease) in some countries, the focus this critical <str<strong>on</strong>g>report</str<strong>on</strong>g> bringsto the problem and viable preventive measures is immensely valuable.Now comes the time for acti<strong>on</strong>.” Alan Whelpt<strong>on</strong>, <str<strong>on</strong>g>World</str<strong>on</strong>g> President,Internati<strong>on</strong>al Wife Saving Federati<strong>on</strong>.5. <str<strong>on</strong>g>World</str<strong>on</strong>g> Drowning Report, 2007 editi<strong>on</strong>. Brussels,Internati<strong>on</strong>al Lifesaving Federati<strong>on</strong>, 2007.6. Linnan M et al. Child mortality and <strong>injury</strong> in Asia:survey results and evidence. Florence, UNICEF InnocentiResearch Centre, 2007 (http://www.unicef-irc.org/publicati<strong>on</strong>s/pdf/iwp_2007_06.pdf, accessed 21 January2008). (Innocenti Working Paper 2007-06, Special Series<strong>on</strong> Child Injury No. 3).WORLD REPORT ON CHILD INJURY PREVENTION 73
7. Rahman A et al. Bangladesh health and <strong>injury</strong> survey:<str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> <strong>child</strong>ren. Dhaka, Government of the People’sRepublic of Bangladesh, ICMH, UNICEF and TASC,2005.8. Sitthi-amorn C et al. Child <strong>injury</strong> in Thailand: a <str<strong>on</strong>g>report</str<strong>on</strong>g><strong>on</strong> the Thai Nati<strong>on</strong>al Injury Survey. Bangkok, Institute ofHealth Research, 2006.9. Rahman A et al. Drowning – a major but neglected <strong>child</strong>health problem in rural Bangladesh: implicati<strong>on</strong>s for lowincome countries. Internati<strong>on</strong>al Journal of Injury C<strong>on</strong>troland Safety Promoti<strong>on</strong>, 2006, 13:101–105.10. Jing RW et al., eds. Beijing <strong>injury</strong> survey, <strong>child</strong> <strong>injury</strong> <str<strong>on</strong>g>report</str<strong>on</strong>g>.Beijing, Chinese Field Epidemiology Training Program,China Centers for Disease C<strong>on</strong>trol, 2004.11. Yang L et al. Epidemiological profile of mortality due toinjuries in three cities in the Guangxi Province, China.Accident Analysis and Preventi<strong>on</strong>, 2005, 37:137–141.12. Ahmed MK, Rahman M, Ginneken JV. Epidemiologyof <strong>child</strong> deaths due to drowning in Matlab, Bangladesh.Internati<strong>on</strong>al Journal of Epidemiology, 1999, 28:306–311.13. Brenner R. Preventi<strong>on</strong> of drowning in infants, <strong>child</strong>ren,and adolescents. Pediatrics, 2003, 112:440–445.14. Annual Statistics Book. Beijing, Ministry of Health, 2001.15. Zhang P, Chen R, Deng J. [A prospective study <strong>on</strong>accidental deaths am<strong>on</strong>g 0–14 year old <strong>child</strong>ren in Jiangsu,1994–1995] (article in Chinese). Zh<strong>on</strong>ghua LiuxingbingxueZazhi, 1998, 19:290–293.16. Afogamentos [Drownings]. São Paulo, Criança SeguraBrasil (http://www.criancasegura.org.br/dados_acidentes_afogamentos.asp,accessed 20 April 2008).17. WHO mortality database: tables. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g>Health Organizati<strong>on</strong> (http://www.who.int/healthinfo/morttables/en/index.html, accessed 21 April 2008).18. Matzopoulos R, ed. A profile of fatal injuries in SouthAfrica: third annual <str<strong>on</strong>g>report</str<strong>on</strong>g> of the Nati<strong>on</strong>al MortalitySurveillance System. Cape Town, Medical ResearchCouncil, 2001 (http://www.sahealthinfo.org/violence/nimssannual2001.htm, accessed 20 April 2008).19. Brenner, RA et al. Where <strong>child</strong>ren drown, United States,1995. Pediatrics, 2001, 108:85–89.20. Hyder AA et al. Childhood drowning in low- and middleincomecountries: Urgent need for interventi<strong>on</strong> trials.Journal of Paediatrics and Child Health, 2008, 44:221–227.21. Present P. Child drowning study. A <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> theepidemiology of drowning in residential pools to <strong>child</strong>renunder age five. Washingt<strong>on</strong>, DC, United States C<strong>on</strong>sumerProduct Safety Commissi<strong>on</strong>, 1987.22. Silbert J et al. Preventing deaths by drowning in <strong>child</strong>renin the United Kingdom: have we made progress in 10years? Populati<strong>on</strong> based incidence study. British MedicalJournal, 2002, 324:1070–1071.23. Meyer RJ, Theodorou AA, Berg RA. Childhood drowning.Pediatrics in Review, 2006, 27:163–169.24. Kobusingye O, Guwatudde D, Lett R. Injury patterns inrural and urban Uganda. Injury Preventi<strong>on</strong>, 2001, 7:46–50.25. Polinder S et al. Prevalence and prognostic factorsof disability after <strong>child</strong>hood <strong>injury</strong>. Pediatrics,2005,116:e810–e817.26. Kreisfeld R, Henley G. Deaths and hospitalizati<strong>on</strong>s due todrowning, Australia 1999–2000 to 2003–2004. Adelaide,Australian Institute for Health and Welfare, 2008 (Deathsand Hospitalisati<strong>on</strong>s Injury Research and Statistics Series,No. 39).27. Kemp AM, Sibert JR. Outcome in <strong>child</strong>ren who nearlydrown: a British Isles study. British Medical Journal, 1991,302:931–933.28. Kibel SM et al. Childhood near-drowning: a 12-yearretrospective review. South African Medical Journal, 1990,78:418–421.29. Susiva C, Bo<strong>on</strong>r<strong>on</strong>g T. Near-drowning in PediatricRespiratory Intensive Care Unit, Siriraj Hospital. Journalof the Medical Associati<strong>on</strong> of Thailand, 2005, 88(Suppl.8):S44–S47.30. Van Beeck EF et al. Guidelines for the c<strong>on</strong>ducti<strong>on</strong> offollow-up studies measuring <strong>injury</strong>-related disability.Journal of Trauma, 2007, 62:534–550.31. Lam LT et al. Different quantitative measures of theimpact of <strong>injury</strong> deaths <strong>on</strong> the community in the GuangxiProvince, China. Accident Analysis and Preventi<strong>on</strong>, 2005,37:761–766.32. Lindqvist KS, Brodin H. One-year ec<strong>on</strong>omic c<strong>on</strong>sequencesof accidents in a Swedish municipality. Accident Analysisand Preventi<strong>on</strong>, 1996, 28:209–219.33. Thanh NX et al. The ec<strong>on</strong>omic burden of unintenti<strong>on</strong>alinjuries: a community-based cost analysis in Bavi,Vietnam. Scandinavian Journal of Public Health, 2003,62(Suppl.):S45–S51.34. Corso P et al. Incidence and lifetime costs of injuries in theUnited States. Injury Preventi<strong>on</strong>, 2006, 12:212–218.35. Meerding WJ, Mulder S, van Beeck EF. Incidence andcosts of injuries in the Netherlands. European Journal ofPublic Health, 2006, 16:272–278.36. Ellis AA, Trent RB. Hospitalizati<strong>on</strong>s for near drowningin California: incidence and costs. American Journal ofPublic Health, 1995, 85:1115–1118.37. Joseph MM, King WD. Epidemiology of hospitalizati<strong>on</strong>for near-drowning. Southern Medical Journal, 1998,91:253–255.38. Wats<strong>on</strong> W, Ozanne-Smith J. The cost of <strong>injury</strong> to Victoria.Clayt<strong>on</strong>, M<strong>on</strong>ash University, 1997 (M<strong>on</strong>ash UniversityAccident Research Centre Report 124).39. Peden M, McGee K. The epidemiology of drowningworldwide. Injury C<strong>on</strong>trol and Safety Promoti<strong>on</strong>, 2003,10:195–199.74 WORLD REPORT ON CHILD INJURY PREVENTION
40. Smith GS. The global burden of drowning. In: BierensJJLM, ed. Handbook <strong>on</strong> drowning; preventi<strong>on</strong>, rescue,treatment. Germany, Springer-Verlag, 2006:56–61.41. Quan L, Cummings P. Characteristics of drowning bydifferent age groups. Injury Preventi<strong>on</strong>, 2003, 9:163–168.42. Smith GS, Langley JD. Drowning surveillance: how well doE codes identify submersi<strong>on</strong> fatalities. Injury Preventi<strong>on</strong>,1998, 4:135–139.43. Blum C, Shield J. Toddler drowning in domestic swimmingpools. Injury Preventi<strong>on</strong>, 2000, 6:288–290.44. Agran PF et al. Rates of pediatric injuries by 3-m<strong>on</strong>thintervals for <strong>child</strong>ren 0 to 3 years of age. Pediatrics, 2003,111:e683–e692.45. Rowntree G. Accidents am<strong>on</strong>g <strong>child</strong>ren under two yearsof age in Great Britian. Injury Preventi<strong>on</strong>, 1998, 4:69–76.46. Yang L et al. Risk factors for <strong>child</strong>hood drowning in ruralregi<strong>on</strong>s of a developing country: a case–c<strong>on</strong>trol study.Injury Preventi<strong>on</strong>, 2007, 13:178–182.47. Howland J et al. Why are most drowning victims men?Sex differences in aquatic skills and behaviours. AmericanJournal of Public Health, 1996, 86:93–96.48. Rahman A et al. Pattern and determinants of <strong>child</strong> deathsdue to drowning in rural Bangladesh [Published abstract].In: Proceedings of the 6th <str<strong>on</strong>g>World</str<strong>on</strong>g> C<strong>on</strong>ference <strong>on</strong> InjuryC<strong>on</strong>trol and Preventi<strong>on</strong>, M<strong>on</strong>treal, Canada, 12–15 May2002. M<strong>on</strong>treal, University of M<strong>on</strong>treal Press, 2002:477–478.49. Kobusingye OC. The global burden of drowning: anAfrican perspective. In: Bierens JJLM, ed. Handbook <strong>on</strong>drowning: preventi<strong>on</strong>, rescue and treatment. Germany,Springer-Verlag, 2006:61–62.50. Wintemute GJ et al. Alcohol and drowning: an analysis ofc<strong>on</strong>tributing factors and a discussi<strong>on</strong> of criteria for caseselecti<strong>on</strong>. Accident Analysis and Preventi<strong>on</strong>, 1990, 22:291–296.51. Recommendati<strong>on</strong>s: <str<strong>on</strong>g>World</str<strong>on</strong>g> C<strong>on</strong>gress <strong>on</strong> Drowning,Amsterdam, Netherlands, 26–28 June 2002. Amsterdam,<str<strong>on</strong>g>World</str<strong>on</strong>g> C<strong>on</strong>gress <strong>on</strong> Drowning, 2002. (http://www.drowning.nl/pdf/Recommendati<strong>on</strong>s.pdf, accessed 20 April2008).52. Morgan D, Ozanne-Smith J, Triggs T. Measurement bydirect observati<strong>on</strong> of drowning risk exposure for surfbeach bathers. Journal of Science and Medicine in Sport,2008 (in press).53. Morgan D, Ozanne-Smith J, Triggs T. Self <str<strong>on</strong>g>report</str<strong>on</strong>g>ed waterand drowning risk exposure at surf beaches. Australianand New Zealand Journal of Public Health (in press).54. Celis, A. Home drowning am<strong>on</strong>g preschool age Mexican<strong>child</strong>ren. Injury Preventi<strong>on</strong>, 1997, 3:252–256.55. Fang Y et al. Child drowning deaths in Xiamen city andsuburbs, People’s Republic of China. Injury Preventi<strong>on</strong>,2007, 13:339–343.56. Karr CJ, Rivara FP, Cummings P. Severe <strong>injury</strong> am<strong>on</strong>gHispanic and n<strong>on</strong>-Hispanic <strong>child</strong>ren in Washingt<strong>on</strong> state.Public Health Reports, 2005, 120:19–24.57. Stirbu I et al. Injury mortality am<strong>on</strong>g ethnic minoritygroups in the Netherlands. Journal of Epidemiology andCommunity Health, 2006, 60:249–255.58. Saluja G et al. Swimming pool drownings am<strong>on</strong>g USresidents aged 5–24 years: understanding racial/ethnicdisparities. American Journal of Public Health, 2006,96:728–733.59. Mael FA. Staying afloat: within-group swimmingproficiency for Whites and Blacks. Journal of AppliedPsychology, 1995, 80:479–490.60. Besag FMC. T<strong>on</strong>ic seizures are a particular risk factor fordrowning in people with epilepsy. British Medical Journal,2001, 321:975–976.61. Nei M, Bagla R. Seizure-related <strong>injury</strong> and death. CurrentNeurology and Neuroscience Reports, 2007, 7:335–341.62. Diekema DS, Quan L, Holt VL. Epilepsy as a risk factor forsubmersi<strong>on</strong> <strong>injury</strong> in <strong>child</strong>ren. Pediatrics, 1993, 91:612–616.63. Janss<strong>on</strong> B, Ahmed N. Epilepsy and <strong>injury</strong> mortality inSweden–the importance of changes in coding practice.Seizure, 2002, 11:361–370.64. Shavelle RM, Strauss DJ, Pickett J. Causes of death inautism. Journal of Autism and Developmental Disorders,2001, 31:569–576.65. Ackerman MJ et al. A novel mutati<strong>on</strong> in KVLQT1 isthe molecular basis of inherited l<strong>on</strong>g QT syndrome in anear-drowning patient’s family. Pediatric Research, 1998,44:148–153.66. Boating Statistics – 2005. United States Coast Guard,Department of Homeland Security, 2006 (http://www.uscgboating.org/statistics/Boating_Statistics_2005.pdf,accessed 21 April 2008).67. Life jackets and life preservers. Chicago, IL, AmericanAcademy of Pediatrics (http://www.aap.org/family/tippslip.htm, accessed 23 April 2008).68. Howland J, Hings<strong>on</strong> R. Alcohol as a risk factor fordrownings: A review of the literature (1950–1985).Accident Analysis and Preventi<strong>on</strong>, 1988, 20:19–25.69. Smith GS, Kraus JF. Alcohol and residential, recreati<strong>on</strong>al,and occupati<strong>on</strong>al injuries: a review of the epidemiologicevidence. Annual Reviews of Public Health, 1988, 9:99–121.70. Smith GS, Brenner RA. The changing risks of drowningfor adolescents in the US and effective c<strong>on</strong>trol strategies.Adolescent Medicine, 1995, 6:153–170.71. Hyder AA et al. Death from drowning: defining a newchallenge for <strong>child</strong> survival in Bangladesh. Injury C<strong>on</strong>troland Safety Promoti<strong>on</strong>, 2003, 10:205–210.72. Drownings and other water-related injuries in Canada1991–2000. Ottawa, Canadian Red Cross, 2003 (http://WORLD REPORT ON CHILD INJURY PREVENTION 75
www.redcross.ca/cmslib/general/10drwn_english.pdf,accessed 20 April 2008).73. Mitchell RJ et al. Farm-related fatalities involving <strong>child</strong>renin Australia, 1989–1992. Australian and New ZealandJournal of Public Health, 2001, 25:307–314.74. Tsunami disaster: UN relief efforts. UNICEF, 2004 (http://www.un.org/events/UNART/tsunami_disaster.pdf,accessed 20 April 2008).75. Mackie IJ. Patterns of drowning in Australia, 1992–1997.Medical Journal of Australia, 1999, 171:587–590.76. Morgan D, Ozanne-Smith J, Triggs T. Descriptiveepidemiology of drowning deaths in a surf beach swimmerand surfer populati<strong>on</strong>. Injury Preventi<strong>on</strong>, 2008, 14:62–65.77. Lunetta P et al. How well does a nati<strong>on</strong>al newspaper<str<strong>on</strong>g>report</str<strong>on</strong>g>ing system profile drowning? Internati<strong>on</strong>al Journalof Injury C<strong>on</strong>trol and Safety Promoti<strong>on</strong>, 2006, 13:35–41.78. Bierens JJLM, ed. Handbook <strong>on</strong> drowning. Germany,Springer-Verlag, 2006.79. DeNicola LK et al. Submersi<strong>on</strong> injuries in <strong>child</strong>ren andadults. Critical Care Clinics, 1997, 13:477–502.80. Causey AL, Tilelli JA, Swans<strong>on</strong> ME. Predicting dischargein uncomplicated near-drowning. American Journal ofEmergency Medicine, 1995, 18:9–11.81. Staines C, Ozanne-Smith J, Davis<strong>on</strong> G. Child and earlyadolescent drowning in developing communities: Victoria,a case study. Melbourne, M<strong>on</strong>ash University AccidentResearch Centre, 2008.82. Pitt WR, Cass DT. Preventing <strong>child</strong>ren drowning inAustralia. Medical Journal of Australia, 2001, 175:603–604.83. Pitt WR, Balanda KP. Toddler drowning in domesticswimming pools in Queensland since uniform fencingrequirements. Medical Journal of Australia, 1998, 169:557–558.84. Ferguss<strong>on</strong> DM, Horwood LJ. Risks of drowning in fencedand unfenced domestic swimming pools. New ZealandJournal of Medicine, 1984, 97:777–779.85. Stevens<strong>on</strong> MR et al. Childhood drowning: barrierssurrounding private swimming pools. Pediatrics, 2003,111:E115–E119.86. Logan P et al. Childhood drowning and fencing of outdoorpools in the United States, 1994. Pediatrics, 1998, 101:E3.87. Thomps<strong>on</strong> DC, Rivara FP. Pool fencing for preventingdrowning in <strong>child</strong>ren. Cochrane Database of SystematicReviews, 2000, (2):CD001047.88. Morgenstern H, Bingham T, Reza A. Effects of pool-fencingordinances and other factors <strong>on</strong> <strong>child</strong>hood drowning inLos Angeles County, 1990–1994. American Journal ofPublic Health, 2000, 90:595–601.89. Ferguss<strong>on</strong> DM, Horwood LJ, Shann<strong>on</strong> FT. The safetystandards of domestic swimming pools 1980–1982. NewZealand Medical Journal, 1983, 96:93–95.90. Morris<strong>on</strong> L et al. Achieving compliance with poolfencing legislati<strong>on</strong> in New Zealand: a survey of regulatoryauthorities. Injury Preventi<strong>on</strong>, 1999, 5:114–118.91. Pers<strong>on</strong>al flotati<strong>on</strong> devices. Seattle, WA, Harborview InjuryPreventi<strong>on</strong> and Research Center (http://depts.washingt<strong>on</strong>.edu/hiprc/practices/topic/drowning/flotati<strong>on</strong>.html,accessed 20 April 2008).92. O’C<strong>on</strong>nor P. Nati<strong>on</strong>al assessment of boating fatalities inAustralia 1992–1998. Rozelle, NSW, Nati<strong>on</strong>al MarineSafety Committee, 2004 (http://www.nmsc.gov.au/documents/Fatal%20Report_screen.pdf, accessed 29 January2007).93. Treser CD, Trusty MN, Yang PP. Pers<strong>on</strong>al floatati<strong>on</strong> deviceusage: do educati<strong>on</strong>al efforts have an impact? Journal ofPublic Health Policy, 1997, 18:346–356.94. Bennett E et al. Evaluati<strong>on</strong> of a drowning preventi<strong>on</strong>campaign in King County, Washingt<strong>on</strong>. Injury Preventi<strong>on</strong>,1999, 5:109–113.95. Cassell E et al. Evaluati<strong>on</strong> of the effectiveness of the 2005Victorian pers<strong>on</strong>al flotati<strong>on</strong> device (PFD) wear regulati<strong>on</strong>s:a pre- and post-observati<strong>on</strong>al study (Report to MarineSafety Victoria). Melbourne, MUARC, 2007.96. Howland J et al. Did changes in minimum age drinkinglaws affect adolescent drowning (1970–90)? InjuryPreventi<strong>on</strong>, 1998, 4:288–291.97. Brenner RA et al. The associati<strong>on</strong> between swimmingless<strong>on</strong>s and drowning in <strong>child</strong>hood: a case-c<strong>on</strong>trol study.Archives of Pediatrics and Adolescent Medicine, (in press).98. Asher KN et al. Water safety training as a potential meansof reducing risk of young <strong>child</strong>ren’s drowning. InjuryPreventi<strong>on</strong>, 1995, 1:228–233.99. Smith GS, Howland JH. Declines in drowning: exploringthe epidemiology of favorable trends. Journal of theAmerican Medical Associati<strong>on</strong>, 1999, 281:2245–2247.100. Ozanne-Smith J, Wigglesworth E, Staines C. Swimminginstructi<strong>on</strong> and drowning [Abstract]. In: <str<strong>on</strong>g>World</str<strong>on</strong>g> C<strong>on</strong>gress<strong>on</strong> Drowning, Amsterdam, 26–28 June 2002. Amsterdam,C<strong>on</strong>sumer Safety Institute, 2002.101. Manolios N, Mackie I. Drowning and near-drowning<strong>on</strong> Australian beaches patrolled by life-savers: a 10-yearstudy, 1973–1983. Medical Journal of Australia, 1988,148:170–171.102. Fenner PJ et al. Success of surf lifesaving resuscitati<strong>on</strong>sin Queensland, 1973–1992. Medical Journal of Australia,1985, 164:580–583.103. Branche CM, Stewart S, eds. Lifeguard effectiveness: a<str<strong>on</strong>g>report</str<strong>on</strong>g> of the working group. Atlanta, GA, Centers forDisease C<strong>on</strong>trol and Preventi<strong>on</strong>, Nati<strong>on</strong>al Center forInjury Preventi<strong>on</strong> and C<strong>on</strong>trol, 2001 (http://www.cdc.gov/ncipc/lifeguard/08_ec<strong>on</strong>omic_costs.htm, accessed19 April 2008).104. Schwebel DC, Simps<strong>on</strong> J, Lindsay S. Ecology of drowningrisk at a public swimming pool. Journal of Safety Research,2007, 38:367–372.76 WORLD REPORT ON CHILD INJURY PREVENTION
105. Quan L et al. Beliefs and practices to prevent drowningam<strong>on</strong>g Vietnamese-American adolescents. InjuryPreventi<strong>on</strong>, 2006, 12:427–429.106. Lee LK, Thomps<strong>on</strong> KM. Parental survey of beliefs andpractices about bathing and water safety and their <strong>child</strong>ren:guidance for drowning preventi<strong>on</strong>. Accident Analysis andPreventi<strong>on</strong>, 2007, 39:58–62.107. Moran K, Stanley T. Parental percepti<strong>on</strong>s of toddlerwater safety, swimming ability and swimming less<strong>on</strong>s.Internati<strong>on</strong>al Journal of Injury C<strong>on</strong>trol and SafetyPromoti<strong>on</strong>, 2006, 13:139–143.108. Lunetta P, Penttilä A, Sarna S. Water traffic accidents,drowning and alcohol in Finland, 1969–1995. Internati<strong>on</strong>alJournal of Epidemiology, 1998, 27:1038–1043.109. Cummings P, Quan L. Trends in unintenti<strong>on</strong>al drowning:the role of alcohol and medical care. Journal of theAmerican Medical Associati<strong>on</strong>, 1999, 281:2198–2202.110. Graf WD et al. Predicting outcome in pediatric submersi<strong>on</strong>victims. Annals of Emergency Medicine, 1995, 26:312–319.111. Kyriacou DN et al. Effect of immediate resuscitati<strong>on</strong> <strong>on</strong><strong>child</strong>ren with submersi<strong>on</strong> <strong>injury</strong>. Pediatrics, 1994, 94:137–142.112. Wiggint<strong>on</strong> J. The key role of laypers<strong>on</strong> acti<strong>on</strong>s in drowningincidents. In: <str<strong>on</strong>g>World</str<strong>on</strong>g> C<strong>on</strong>gress <strong>on</strong> Drowning, Amsterdam, 26–28 June 2002. Amsterdam, C<strong>on</strong>sumer Safety Institute, 2002.113. Quan L, Kinder D. Pediatric submersi<strong>on</strong>s: prehospitalpredictors of outcome. Pediatrics, 1992, 90:909–913.114. Suominen et al. Does water temperature affect outcome ofnearly drowned <strong>child</strong>ren. Resuscitati<strong>on</strong>, 1997, 35:111–115.115. Byard RW, D<strong>on</strong>ald T. Infant bath seats, drowning andnear-drowning. Journal of Paediatrics and Child Health,2004, 40:305–307.116. Rauchschwalbe R, Brenner RA, Smith GS. The role ofbathtub seats and rings in infant drowning deaths. Pediatrics,1997, 100:E1.117. Sulkes SB, van der Jagt EW. Solar pool blankets: anotherwater hazard. Pediatrics, 1990, 85:1114–1117.118. Bugeja L, Franklin R. Drowning deaths of zero- tofive-year-old <strong>child</strong>ren in Victorian dams, 1989–2001.Australian Journal of Rural Health, 2005, 13:300–308.119. Pless IB. The challenge of drowning preventi<strong>on</strong>. InjuryPreventi<strong>on</strong>, 1997, 3:237–238.120. Passmore JW, Smith JO, Clappert<strong>on</strong> A. True burden ofdrowning: compiling data to meet the new definiti<strong>on</strong>.Internati<strong>on</strong>al Journal of Injury C<strong>on</strong>trol and SafetyPromoti<strong>on</strong>, 2007, 14:1–3.121. Quan L, Bennett EE, Branche CM. Interventi<strong>on</strong>s to preventdrowning. In: Doll LS et al., eds. Handbook of <strong>injury</strong> andviolence preventi<strong>on</strong>. Atlanta, GA, Springer, 2007:81–96.122. Nort<strong>on</strong> R et al. Unintenti<strong>on</strong>al injuries. In: Jamis<strong>on</strong> DT etal., eds. Disease c<strong>on</strong>trol priorities in developing countries(2nd editi<strong>on</strong>). New York, Oxford University Press and the<str<strong>on</strong>g>World</str<strong>on</strong>g> Bank, 2006:737–753 (http://www.dcp2.org/pubs/DCP/39/, accessed 14 February 2008).WORLD REPORT ON CHILD INJURY PREVENTION 77
© Children of FireFive years ago, when he was 13 yearsold, Vusi suffered serious burns.He woke up <strong>on</strong>e night to find hisblanket and bedroom ablaze froma candle that had fallen over. Theflames injured his face, handsand feet.B U RNSVUSI’S STORYAfter many m<strong>on</strong>ths in hospital, he left wearing a brown elasticized pressure garmentaround his face and hands so that his scars would not become thick and raised, asoften happens.From the start, Vusi was very sensitive about his appearance. People <strong>on</strong> the streetsand at school used to tease him about the mask-like pressure garment, comparinghim to a masked televisi<strong>on</strong> entertainer. The l<strong>on</strong>g hospital stay and the psychologicalstress led to problems at school and his educati<strong>on</strong> was delayed. Despite all he wentthrough, though, Vusi has become a charming, friendly pers<strong>on</strong> with an engagingsmile. He loves music and voluntarily spends time with blind <strong>child</strong>ren and otherswith disabilities, encouraging them to exercise more.Africa’s fi rst burns charity, “Children of Fire”, has, for the past twelve years, beenhelping severely burned <strong>child</strong>ren to obtain complex surgery, therapy and educati<strong>on</strong>.They now also work <strong>on</strong> community safety, teaching those at risk how to preventfi re burns, as well as imparting fi rst aid and fi re-fi ghting skills. The organizati<strong>on</strong> alsohelps inventors of safer paraffi n or biofuel stoves to publicize their inventi<strong>on</strong>s morewidely, and in a similar way promotes the use of safer candlesticks.In June 2007, 15 teenaged burns survivors, al<strong>on</strong>g with other young volunteers,climbed Mount Kilimanjaro in a campaign to raise awareness of burn injuries and howto prevent them, and to increase tolerance of disability and disfigurement. Vusi was<strong>on</strong>e of those who climbed to above 5000 metres and 12 others reached the summit.Adapted from the Children of Fire web site (http://www.fire<strong>child</strong>ren.org, accessed 9 June 2008).
CHAPTER 4 – BURNSChapter 4BurnsIntroducti<strong>on</strong>Children are naturally curious. As so<strong>on</strong> as they are mobile,they begin to explore their surroundings and play with newobjects. In this way, they acquire the skills they need tosurvive in the world. At the same time, though, they comeinto c<strong>on</strong>tact with objects that can cause severe injuries.Playing with fire or touching hot objects can result inburns. This is a debilitating c<strong>on</strong>diti<strong>on</strong> accompanied byintense pain and often by l<strong>on</strong>ger-term illness that createssuffering not <strong>on</strong>ly for the <strong>child</strong> but for the wider familyand community. Fortunately, the preventi<strong>on</strong>, acute careand rehabilitati<strong>on</strong> of burns have improved greatly overthe past few decades. There is now ample evidence thata number of measures are effective in preventing burns.These include the introducti<strong>on</strong> and enforcement of itemssuch as smoke alarms, residential sprinklers and fire-safelighters, and laws regulating the temperature of hot-watertaps. N<strong>on</strong>etheless, c<strong>on</strong>siderable disparities exist betweencountries in the extent of their preventi<strong>on</strong>, care andrehabilitati<strong>on</strong> of burns.BOX 4.1Classificati<strong>on</strong> of burnsThere are several ways of classifying burns. The following are threecomm<strong>on</strong>ly used typologies, based respectively <strong>on</strong> the cause, extent andseverity of the burn.Classificati<strong>on</strong> by mechanism or causeCausally, burns may be classified as thermal or inhalati<strong>on</strong>al.Thermal burns involve the skin and may present as:– scalds – caused by hot liquid or steam;– c<strong>on</strong>tact burns – caused by hot solids or items such as hot pressingir<strong>on</strong>s and cooking utensils, as well as lighted cigarettes;– flame burns – caused by flames or incandescent fires, such asthose started by lighted cigarettes, candles, lamps or stoves;– chemical burns – caused by exposure to reactive chemical substancessuch as str<strong>on</strong>g acids or alkalis;– electrical burns – caused by an electrical current passing from anelectrical outlet, cord or appliance through the body.Inhalati<strong>on</strong>al burns are the result of breathing in superheated gases,steam, hot liquids or noxious products of incomplete combusti<strong>on</strong>.They cause thermal or chemical <strong>injury</strong> to the airways and lungs (2)and accompany a skin burn in approximately 20% to 35% of cases.Inhalati<strong>on</strong>al burns are the most comm<strong>on</strong> cause of death am<strong>on</strong>g peoplesuffering fire-related burn (3).This chapter describes what is currently known about<strong>child</strong>hood burns and how to prevent and manage them.In doing so, it summarizes the epidemiology of burnsin <strong>child</strong>ren and the risk factors and discusses in detailboth proven and promising interventi<strong>on</strong>s. The chapterc<strong>on</strong>cludes with a set of recommended interventi<strong>on</strong>s and adescripti<strong>on</strong> of areas where further research is required.For the purpose of this chapter, a burn is defined asan <strong>injury</strong> to the skin or other organic tissue caused bythermal trauma. It occurs when some or all of the cellsin the skin or other tissues are destroyed by hot liquids(scalds), hot solids (c<strong>on</strong>tact burns), or flames (flameburns). Injuries to the skin or other organic tissues due toradiati<strong>on</strong>, radioactivity, electricity, fricti<strong>on</strong> or c<strong>on</strong>tact withchemicals are also c<strong>on</strong>sidered as burns (1).Burns may be distinguished and classified by theirmechanism or cause, the degree or depth of the burn, thearea of body surface that is burned, the regi<strong>on</strong> or part ofthe body affected, as well as the extent. Box 4.1 summarizesthree of the most comm<strong>on</strong>ly used classificati<strong>on</strong>s.Classificati<strong>on</strong> by the degree and depth of a burnBurns may also be classified by depth or thickness:First-degree or superficial burns are defined as burns to the epidermisthat result in a simple inflammatory resp<strong>on</strong>se. They are typicallycaused by exposure of the unprotected skin to solar radiati<strong>on</strong> (sunburn)or to brief c<strong>on</strong>tact with hot substances, liquids or flash flames(scalds). First-degree burns heal within a week with no permanentchanges in skin colour, texture, or thickness.Sec<strong>on</strong>d-degree or partial-thickness burns result when damage to theskin extends beneath the epidermis into the dermis. The damage doesnot, however, lead to the destructi<strong>on</strong> of all elements of the skin.– Superficial sec<strong>on</strong>d-degree burns are those that take less thanthree weeks to heal.– Deep sec<strong>on</strong>d-degree burns take more than three weeks to closeand are likely to form hypertrophic scars.Third-degree or full-thickness burns are those where there is damageto all epidermal elements – including epidermis, dermis, subcutaneoustissue layer and deep hair follicles. As a result of the extensivedestructi<strong>on</strong> of the skin layers, third-degree burn wounds cannot regeneratethemselves without grafting.In adults, a full-thickness burn will occur within 60 sec<strong>on</strong>ds if the skin isexposed to hot water at a temperature of 53° C (4). If, though, the temperatureis increased to 61° C, then <strong>on</strong>ly 5 sec<strong>on</strong>ds are needed for sucha burn. In <strong>child</strong>ren, burns occur in around a quarter to a half of the timeneeded for an adult to burn.Classificati<strong>on</strong> by extent of burnThe extent of burn, clinically referred to as the total body surface areaburned, is defined as the proporti<strong>on</strong> of the body burned (5). Severalmethods are used to determine this measurement, the most comm<strong>on</strong>being the so-called “rule of nines”. This method assigns 9% to the headand neck regi<strong>on</strong>, 9% to each arm (including the hand), 18% to each leg(including the foot) and 18% to each side of the trunk (back, chest andabdomen). The “rule of nines” is used for adults and <strong>child</strong>ren older than10 years, while the Lund and Browder Chart is used for <strong>child</strong>ren youngerthan 10 years (6). The calculati<strong>on</strong> assumes that the size of a <strong>child</strong>’s palmis roughly 1% of the total body surface area (7).WORLD REPORT ON CHILD INJURY PREVENTION 79
Epidemiology of burnsAccording to the WHO Global Burden of Disease estimatesfor 2004, just over 310 000 people died as a result of firerelatedburns, of whom 30% were under the age of 20 years(see Statistical Annex, Table A.1). Fire-related burns arethe 11th leading cause of death for <strong>child</strong>ren between theages of 1 and 9 years. Overall, <strong>child</strong>ren are at high riskfor death from burns, with a global rate of 3.9 deaths per100 000 populati<strong>on</strong>. Am<strong>on</strong>g all people globally, infantshave the highest death rates from burns. The rate thenslowly declines with age, but increases again in elderlyadults.The l<strong>on</strong>g-term c<strong>on</strong>sequences and the disability thatcan result from burns place a c<strong>on</strong>siderable strain <strong>on</strong>individuals and their families, as well as <strong>on</strong> health-carefacilities. According to WHO data, approximately 10% ofall unintenti<strong>on</strong>al <strong>injury</strong> deaths are due to fire-related burns(see Statistical Annex Table A.1). In additi<strong>on</strong>, fire-relatedburns are am<strong>on</strong>g the leading causes of disability-adjustedlife years (DALYs) lost in low-income and middle-incomecountries (see Statistical Annex A.2).MortalityGlobally, nearly 96 000 <strong>child</strong>ren under the age of 20 yearswere estimated to have been fatally injured as a result ofa fire-related burn in 2004. The death rate in low-incomeand middle-income countries was eleven times higherthan that in high-income countries, 4.3 per 100 000 asagainst 0.4 per 100 000 (see Statistical Annex, Table A.1).However, as can be seen in Figure 4.1, burn-related deathsshow great regi<strong>on</strong>al variability. Most of the deaths occurin poorer regi<strong>on</strong>s of the world – am<strong>on</strong>g the WHO regi<strong>on</strong>sof Africa and South-East Asia, and the low-income andmiddle-income countries of the Eastern MediterraneanRegi<strong>on</strong>. The death rates in the Americas and the highincomecountries of the Europe and the Western Pacificregi<strong>on</strong>s are am<strong>on</strong>g the lowest in the world.Every year 70 Member States – mainly middle-incomeand high-income countries –submit to WHO mortalitydata that include the fourth digit of the Internati<strong>on</strong>alClassificati<strong>on</strong> of Disease codes, which allows disaggregati<strong>on</strong>into subtypes of burns. Analysis of these data showthat, in 2002, fire-related burns made up 93.0% of all burndeaths, scalds c<strong>on</strong>tributed 5.4% and the rest, 1.6%, were asa result of c<strong>on</strong>tact, chemical or electrical burns (8).Studies from high-income countries suggest that smokeinhalati<strong>on</strong> is the str<strong>on</strong>gest determinant of mortality fromburns, mostly from house fires or other c<strong>on</strong>flagrati<strong>on</strong>s.For <strong>child</strong>ren over three years of age, smoke inhalati<strong>on</strong> isstr<strong>on</strong>gly associated with mortality, despite improvementsin the care of burns (9).FIGURE 4.1Mortality rates due to fire-related burns per 100 000 <strong>child</strong>ren a by WHO regi<strong>on</strong> and country income level, 20044+0.5–3.9
AgeFigure 4.2 shows <strong>child</strong> death rates from burns by age group.Infants have the highest rates, while those aged between 10and 14 years have the lowest rates. The death rate climbs againin the 15–19-year age range, possibly as a result of greaterexposure, experimentati<strong>on</strong> and risk-taking, as well as thefact that many in that group are beginning employment.FIGURE 4.2Fatal fire-related burn rates per 100 000 <strong>child</strong>ren by age andcountry income level, <str<strong>on</strong>g>World</str<strong>on</strong>g>, 2004Rate per 100 000 populati<strong>on</strong>121086420HIC = High-income countries; LMIC = low-income and middle-income countries.Source: WHO (2008), Global Burden of Disease: 2004 update.GenderHICLMICUnder 1 1–4 5–9 10–14 15–19 under 20Age (years)Burns are the <strong>on</strong>ly type of unintenti<strong>on</strong>al <strong>injury</strong> wherefemales have a higher rate of <strong>injury</strong> than males. The firerelateddeath rate for girls is 4.9 per 100 000 populati<strong>on</strong>,as against 3.0 per 100 000 for boys. The difference isparticularly pr<strong>on</strong>ounced in infants and also in adolescentsbetween the ages of 15 and 19 years (see Figure 4.3).The greatest gender discrepancies are found in theWHO South-East Asia Regi<strong>on</strong> and in the low-income andmiddle-income countries of the Eastern MediterraneanRegi<strong>on</strong>. In these regi<strong>on</strong>s, girls in the 15–19-year age brackethave death rates that are substantially higher than ratesfor the same age group in any other regi<strong>on</strong> (see StatisticalAnnex, Table A.1).FIGURE 4.3Fatal fire-related burn rates per 100 000 <strong>child</strong>ren by age and sex,<str<strong>on</strong>g>World</str<strong>on</strong>g>, 2004Rate per 100 000 populati<strong>on</strong>14121086420Source: WHO (2008), Global Burden of Disease: 2004 update.BoysGirlsUnder 1 1–4 5–9 10–14 15–19Age (years)MorbidityGlobal data <strong>on</strong> n<strong>on</strong>-fatal outcomes from burns is not readilyavailable. However, the WHO Global Burden of Diseaseproject for 2004 makes it clear that burns are an importantc<strong>on</strong>tributor to the overall disease toll in <strong>child</strong>ren in thelow-income and middle-income countries of the African,South-East Asia and the Eastern Mediterranean regi<strong>on</strong>s(see Statistical Annex, Table A.2).While burns from fire c<strong>on</strong>tribute to the majority of burnrelateddeaths in <strong>child</strong>ren, scalds and c<strong>on</strong>tact burns arean important factor in overall morbidity from burns anda significant cause of disability. Chemical and electricalburns am<strong>on</strong>g <strong>child</strong>ren, though, are relatively rare (10–12).AgeIn high-income countries, <strong>child</strong>ren under the age of fiveyears old are at the highest risk of hospitalizati<strong>on</strong> fromburns, although 15–19-year-olds, as already stated, are alsoa group at high risk. Nearly 75% of burns in young <strong>child</strong>renare from hot liquid, hot tap water or steam. Infants underthe age of <strong>on</strong>e year are still at significant risk for burns,even in developed countries. The burns they suffer are mostcomm<strong>on</strong>ly the result of scalds from cups c<strong>on</strong>taining hotdrinks or c<strong>on</strong>tact burns from radiators or hot-water pipes(13).The following give an indicati<strong>on</strong> of the situati<strong>on</strong> insome high-income countries:In Canada, in a single year, there were over 6000 visitsto emergency departments in the province of Ontario(whose populati<strong>on</strong> is about 12 milli<strong>on</strong>) due to burns(14). Almost half the cases of burns are am<strong>on</strong>g <strong>child</strong>renunder five years of age (15).In Finland, an 11-year study found that scalds wereresp<strong>on</strong>sible for 42.2% of <strong>child</strong>ren being admitted totwo paediatric burns units. Am<strong>on</strong>g <strong>child</strong>ren underthree years of age, 100% of burns were the result of hotwater. In the 11–16-year group, 50% of burns were dueto electricity, with the other 50% resulting from fire andflames (16).In Kuwait, the incidence of burns in <strong>child</strong>ren under15 years of age was 17.5 per 100 000 populati<strong>on</strong>. Scalds(67%), followed by flames (23%), were the leading causesof burns (17).In the United States, <strong>on</strong>e of the leading causes of <strong>injury</strong>from scalding in <strong>child</strong>ren is hot soup, particularlyprepackaged instant soup (18).In low-income and middle-income countries, <strong>child</strong>renunder the age of five years have been shown to have adisproporti<strong>on</strong>ately higher rate of burns than is the case inhigh-income countries. In Kenya, for example, 48.6% of<strong>child</strong>ren presenting to the Kenyatta Nati<strong>on</strong>al Hospital wereunder the age of five years. Although scalds were the mostcomm<strong>on</strong> type of burn, those caused by open flames werealso prominent (19). Other examples from low-incomeWORLD REPORT ON CHILD INJURY PREVENTION 81
and middle-income countries show rather different agepatterns and leading causes.In Shand<strong>on</strong>g Province, China, a 5-year review of datafrom the burns unit revealed that <strong>child</strong>ren under theage of 10 years were admitted in the greatest numbers,followed by adults aged between 20 and 30 years. Scaldsand fire-related burns were seen in roughly similarnumbers (20).Burns from boiling liquids, most frequently water boiledfor bathing, were am<strong>on</strong>g the leading causes of injuriesto <strong>child</strong>ren under the age of 10 years in Cuernavaca,Mexico (21).In Maiduguri, north-east Nigeria, the comm<strong>on</strong>est causeof burns was scalds (64.4%). Children under the age ofthree years were disproporti<strong>on</strong>ately represented (22).In Brazil, Côte d’Ivoire and India, infants account fornearly half of all <strong>child</strong>hood burns (23–25).In Fars Province in the Islamic Republic of Iran, theannual hospitalizati<strong>on</strong> rate for <strong>child</strong>ren under 15 yearswas 11.8 per 100 000 populati<strong>on</strong>. Scalds accountedfor 46.2% of the burns, whereas flames accounted for42.8%. Most burns occurred at home (26).Similar results have been found in a recent study infour low-income countries. In this study, 53% of burns in<strong>child</strong>ren under 12 years of age were the result of a hot liquid,followed by fire and flame in 19% of cases and electricity in14% of cases (see Statistical Annex, Table C.1).Infants in Africa under <strong>on</strong>e year of age have an annualincidence of fire-related burns of 35 per 100 000 – more thanthree times the world average for this age group (27).GenderThe gender distributi<strong>on</strong> of n<strong>on</strong>-fatal burns differs betweencountries – a fact that may be related to cultural practices,particularly with regard to cooking. Some African andAsian countries – including Angola, Bangladesh, China,Côte d’Ivoire, Kenya and Nigeria – <str<strong>on</strong>g>report</str<strong>on</strong>g> a higher numberof cases am<strong>on</strong>g males (19, 20, 22, 24, 28, 29). Others, suchas Egypt and India, have a greater proporti<strong>on</strong> am<strong>on</strong>g girls,particularly teenage girls (30–32).The increasing proporti<strong>on</strong> of burn injuries recorded ingirls as they grow older might be explained by the changingactivities of the two genders. While girls are increasinglyinvolved in the kitchen, helping their mothers – and thereforemore exposed to fire, and hot liquids and other substances– boys tend to stay more outdoors (see Box 4.2). In somecultures, “bride burning” is still practised and may be linkedto a higher incidence of burns in adolescent females (33).BOX 4.2Burns to young working females in work and home settingsBurns are the leading cause of deaths from <strong>injury</strong> in many developing countries. Work-related burn injuries are relatively rare in <strong>child</strong>ren. N<strong>on</strong>etheless,they are an important public health problem for young people employed in the catering industry and <strong>child</strong>ren working in residential kitchens.Work-related <strong>child</strong>hood burn injuries – in whatever setting – often go un<str<strong>on</strong>g>report</str<strong>on</strong>g>ed, especially in developing countries, either because safety regulati<strong>on</strong>sare not being enforced, or because of a lack of regulati<strong>on</strong> and supervisi<strong>on</strong>. Three types of workplaces are typically involved in employmentrelatedburn injuries in <strong>child</strong>ren.Catering and restaurant industry: The most comm<strong>on</strong> sources of burn injuries in restaurants and kitchens are cooking oils, hot water, steamand heating equipment. A study in the state of Washingt<strong>on</strong>, United States for the period 1989–1993, found that 2076 workers under 18 years of agesuffered burn injuries, representing 7.6% of all work-related burn injuries. The most comm<strong>on</strong> sector in which they occurred was the food servicesindustry. Young people working in fast-food outlets and restaurants made up 62% of these cases – as against <strong>on</strong>ly 32% of burn injuries in 125 otheroccupati<strong>on</strong>s combined (34). Similar findings for the state were also found for the period 1994–1998 (35).Other industrial settings, including metal industries: Children have the lowest rates of burns in large-scale industrial settings, presumably becausethey are generally unsuitable for this work and therefore have little exposure to its risks. Where they are involved and suffer burns, though, their burns are <strong>on</strong>the whole more severe than in other settings. In both industrial settings and in food services, males are more affected than females by burns.House kitchens: Unlike the situati<strong>on</strong> in other workplace settings, employment-related injuries in house kitchens principally involve girls. Girls workingas house maids are generally resp<strong>on</strong>sible for cooking as well as other household tasks. They often work without c<strong>on</strong>tracts and may be deprived of legalsupport. Due to their young age, they are <strong>on</strong> average less skilful and more pr<strong>on</strong>e to burns than adults. In additi<strong>on</strong>, their work c<strong>on</strong>diti<strong>on</strong>s are frequentlyunsafe. Some young females are employed in households that are not their own, while others are obliged to work in their home as family members. Theflammable and loose clothing often worn by young women in developing countries further increases the risk of burn injuries (36).In the Islamic Republic of Iran, burn injuries are the most comm<strong>on</strong> unintenti<strong>on</strong>al home-related <strong>injury</strong> (37). Iranian <strong>injury</strong> registry databases showthat during the period 1999–2001, 58% of all <str<strong>on</strong>g>report</str<strong>on</strong>g>ed burn injuries were in <strong>child</strong>ren. In the Ardabil province of Iran, a recent study found that 65%of <strong>child</strong>ren suffering burns in the kitchen were girls, and that girls aged 16–17 years were three times as likely to be burned in the kitchen as wereboys. The study also found that <strong>child</strong>ren younger than 12 years were having to help in cooking-related work in kitchens, with an average startingage of 8 years (see Table).Children helping in household kitchen jobs, Ardabil province, Islamic Republic of Iran, 2006Kitchen jobs Proporti<strong>on</strong> of <strong>child</strong>ren helping in kitchen (%) Mean age of starting to help in kitchen (years)Cooking 21.2 8.7Preparing tea 37.2 8.0Carrying hot food 37.5 7.9Lighting the oven 24.0 –82 WORLD REPORT ON CHILD INJURY PREVENTION
Locati<strong>on</strong>Most studies suggest that burns in <strong>child</strong>ren occur mostfrequently in the home, or else – am<strong>on</strong>g older <strong>child</strong>ren – inthe workplace. A study in four low-income countries foundthat 65% of <strong>child</strong>hood burns had occurred in and aroundthe home (Statistical Annex, Table C.1). The kitchen isusually the most comm<strong>on</strong> part of the house. In this room,<strong>child</strong>ren may upset receptacles with hot liquids, be injuredby exploding stoves, stand <strong>on</strong> hot coals or be splashed withhot cooking oil.Most burns occur in urban areas. Those burns thattake place in rural areas with inadequate prehospitalcare, though, can lead to greater volumes of illness anddisabilities.Nature and severity of burnsFew empirical studies have described burn injuries by thebody part affected. Am<strong>on</strong>g those that have, though, themost comm<strong>on</strong> sites are <str<strong>on</strong>g>report</str<strong>on</strong>g>ed to be the following:– from scalds: the trunk and upper extremities (24, 38);– from flame-related burns: the lower extremities (38, 39);– from c<strong>on</strong>tact burns: the hands (40);– from electrical burns: there may be little externalevidence of the burn but extensive internal damage.Small <strong>child</strong>ren who bite or suck <strong>on</strong> extensi<strong>on</strong> cordscan burn their mouth and lips. Such burns may causecosmetic deformities and impair growth of the teeth,mandibles and maxilla (41).– from chemical burns: the site depends <strong>on</strong> whether thechemical is ingested, splashed or inhaled.The total surface area of the body that is affected depends<strong>on</strong> the cause of burn, the mechanism of <strong>injury</strong> and the ageof the <strong>child</strong>. In general, scalds and c<strong>on</strong>tact burns are lesssevere than fire-related burns. Lung damage, as a result ofinhalati<strong>on</strong> injuries, is the most frequent cause of death andis largely unpreventable (42).C<strong>on</strong>sequences of n<strong>on</strong>-fatal burnsThe study already menti<strong>on</strong>ed that was c<strong>on</strong>ducted infour low-income countries found that the average <strong>injury</strong>severity score for <strong>child</strong>ren who had been burned was 5. Inadditi<strong>on</strong>, 49% of affected <strong>child</strong>ren suffered some form ofdisability after a burn, with 8% being left with a permanentphysical disability (see Table 1.5 in Chapter 1). Therewere similar results in Bangladesh, where a communitybasedsurvey revealed an annual disability rate of 5.7 per100 000 <strong>child</strong>ren as a result of burns (29).Burns can result in significant l<strong>on</strong>g-term c<strong>on</strong>sequenceswhich – in the absence of a comprehensive and coordinatedrehabilitati<strong>on</strong> programme – can leave <strong>child</strong>ren scarred,physically and psychologically, for the rest of their lives.Most rehabilitati<strong>on</strong> programmes seek to prevent l<strong>on</strong>gtermproblems – such as scarring, c<strong>on</strong>tractures andother physical problems that limit functi<strong>on</strong>ing. However,attenti<strong>on</strong> should also be paid to managing pain as well aspsychological issues such as anxiety, post-traumatic stress,phobias and isolati<strong>on</strong> (43, 44).The most comm<strong>on</strong> physical l<strong>on</strong>g-term c<strong>on</strong>sequencesfollowing a burn include hypertrophic scarring, extensivec<strong>on</strong>tractures, the formati<strong>on</strong> of keloids and the need toamputate an extremity (43). Hypertrophic scarring inparticular has been found to be <strong>on</strong>e of the most significantl<strong>on</strong>g-term c<strong>on</strong>sequences of <strong>child</strong>hood burns, occurringin almost half of severe cases (45). Keloid formati<strong>on</strong> isrelatively more comm<strong>on</strong> am<strong>on</strong>g <strong>child</strong>ren of Africandescent (46).“My worst experience took place <strong>on</strong> a crowded bus. Other passengerskept looking at me so I took my jacket off and covered my head.I just wanted to be invisible and I wanted them all to disappeartoo.” (Michael, aged 17, Changing Faces – a United Kingdom n<strong>on</strong>governmentalorganizati<strong>on</strong> for people with disfigurements)The outcome following a burn depends <strong>on</strong> a number ofinterrelated factors. These include:– the <strong>child</strong>’s age;– the body part affected;– the proporti<strong>on</strong> of body surface area burned;– the length of time from <strong>injury</strong> to care;– the type of care applied – such as dressings ordebridement (the removal of damaged tissue from awound);– post-burn complicati<strong>on</strong>s.Burns to the face resulting in gross disfigurati<strong>on</strong> canlead to poor self-esteem in <strong>child</strong>ren and adolescents (47).Children suffering burns when they are young, though,appear to be very resilient, adapting to their disfigurati<strong>on</strong>with greater ease than those similarly affected duringadolescence. A recent study from India showed that<strong>on</strong>ly adolescents in the study required psychosocialrehabilitati<strong>on</strong> (48).As <strong>on</strong>e of the factors in the <strong>child</strong>’s l<strong>on</strong>g-term socialadjustment is that of self-esteem (49), social supportnetworks may help the process. This is the case not <strong>on</strong>lyfor the <strong>child</strong>, but also for parents, and in particularmothers, who often experience post-traumatic stressdisorder after their <strong>child</strong> has suffered a large burn (50, 51).N<strong>on</strong>governmental organizati<strong>on</strong>s can play an importantrole in providing such support. So can “burn camps”for <strong>child</strong>ren, that were first set up in 1983 (52). Siblingsof a <strong>child</strong> who has suffered burns should also be takeninto c<strong>on</strong>siderati<strong>on</strong>, as overprotecting the <strong>child</strong> can havean adverse behavioural impact <strong>on</strong> other <strong>child</strong>ren in thefamily (53).Impact <strong>on</strong> families and communitiesEvaluating the cost of burns and their treatment is difficult.It is certain, though, that burns create a heavy ec<strong>on</strong>omicWORLD REPORT ON CHILD INJURY PREVENTION 83
load <strong>on</strong> health-care services. A study of hospitalizati<strong>on</strong>s inBangkok, for example, found that the cost of burn injurieswas not sufficiently reimbursed to the hospitals. As aresult, the hospitals had to divert resources from otherareas of care (54).The cost of treating burns is dependent <strong>on</strong> the typeand severity of the burn. In the United Kingdom, a recentstudy found the average cost of an uncomplicated minorpaediatric scald to be £1850 (US$ 3618) (55). Anotherstudy from the United States found that the cost ofhospitalizati<strong>on</strong>s from burns ranged from US$ 1187 forscalds to US$ 4102 for those resulting from fires (56).In additi<strong>on</strong> there are also costs to the families of<strong>child</strong>ren associated with hospitalizati<strong>on</strong>, the need forl<strong>on</strong>g-term rehabilitati<strong>on</strong>, lost school days and educati<strong>on</strong>,possible future unemployment, social rejecti<strong>on</strong> and otherpsychosocial issues (51, 57).The potential to reduce individual and societal costsby carrying out effective burn preventi<strong>on</strong> interventi<strong>on</strong>s ishuge. A recent study in Ontario, Canada (58), for instance,found that – through a combinati<strong>on</strong> of educati<strong>on</strong>al andlegislative measures – preventing scald burns could save531 Canadian dollars (US$ 507) per scald.Limitati<strong>on</strong>s of dataThere are wide differences between countries in data <strong>on</strong><strong>child</strong>hood burns – as regards their availability, quality andreliability. The WHO Global Burden of Disease projectdata used in this chapter relies <strong>on</strong>ly <strong>on</strong> fire-related burns.Although these account for nearly 97% of fatal burns in<strong>child</strong>ren, the data still underestimate the total numberof burns cases. This could be rectified if more countriessubmitted data that included the 4th digit of the ICDcoding.While there is no global morbidity database, therenow exist many studies from both high-income and lowincomecountries <strong>on</strong> the epidemiology and risk factorsfor burns. Using these hospital-based studies researchershave tried to estimate the global extent of n<strong>on</strong>-fatal burns.However, these attempts have been hampered by the lackof populati<strong>on</strong>-based informati<strong>on</strong> and also by the differingdefiniti<strong>on</strong>s of the age range of <strong>child</strong>hood (59).Risk factorsVarious studies, using descriptive and case-c<strong>on</strong>trol designs,have found a range of risk factors for <strong>child</strong>hood burns.However, because of the way in which burns are codedin many countries, it is often impossible to distinguishbetween the different mechanisms that lead to burns. Forexample, the risk factors for burns caused by chemicalagents, and the populati<strong>on</strong> most frequently affected bysuch burns, are both very different from the risk factorsfor and populati<strong>on</strong>s affected by scalds from boiling fluids.Thus, while the existing data identify <strong>child</strong>ren and youngpeople as a high-risk populati<strong>on</strong> for burns, informati<strong>on</strong><strong>on</strong> mechanisms and causal factors is largely missing. Thissecti<strong>on</strong> makes use of the Hadd<strong>on</strong> matrix (60) to highlightthe <strong>child</strong>, agent and envir<strong>on</strong>mental risk factors. Some riskfactors are applicable, of course, <strong>on</strong>ly to certain types ofburns (see Table 4.1).TABLE 4.1Hadd<strong>on</strong> Matrix applied to the risk factors for fire-related burns am<strong>on</strong>g <strong>child</strong>renPhasesPre-eventEventPost-eventFactorsChild Agent Physical envir<strong>on</strong>ment Socioec<strong>on</strong>omic envir<strong>on</strong>mentDevelopmental issues, includingexperimentati<strong>on</strong>; gender;vulnerability – including disabled<strong>child</strong>ren, refugees, street<strong>child</strong>ren; lack of supervisi<strong>on</strong>;parents smoking in the home orin bed; lack of knowledge aboutrisks of fire in the home.Unmaintained smoke alarmsand sprinkler systems; <strong>child</strong>not wearing flame-retardantclothing; poor knowledge aboutevacuati<strong>on</strong> procedures.Inaccessible first-aid kits; lackof knowledge by caregivers andcommunity about what to doimmediately after a burn.Storage of flammablesubstances in the house;combustibles, matchesor lighters accessible to<strong>child</strong>ren; unsafe stovesor lamps; fireworks.Lack of sprinklersystems; lack of firehydrants or other accessto a supply of water.Flammability ofhousehold materialsand <strong>child</strong>ren’s clothing;toxicity of smoke andburning householdmaterials.Housing in slums or c<strong>on</strong>gestedareas; overcrowdedhouseholds; no separati<strong>on</strong>between cooking area andother areas; absence offlame-retardant householdmaterials.Lack of functi<strong>on</strong>ing smokealarms; lack of clear andeasily accessible escaperoutes; lack of access toteleph<strong>on</strong>e to call for help.Poor emergency or firedepartment resp<strong>on</strong>se time;poor rescue and treatmentskills; lack of access towater; inability to transportto medical care promptly.Poverty; unemployment, illiteracy am<strong>on</strong>gparents; sibling who died of burns; lackof fire-related building codes and theirenforcement; lack of policies or laws <strong>on</strong>smoke alarms, sprinkler systems, accessto hydrants; lack of policies or laws <strong>on</strong>flammability standards.Poor access to informati<strong>on</strong> and resourcesto minimize risk; inadequate communicati<strong>on</strong>sinfrastructure for calling emergencyhealth services.Inadequate burns care; inadequate accessto burn centres and rehabilitati<strong>on</strong> services;insufficient community support for thosewho have suffered burns.84 WORLD REPORT ON CHILD INJURY PREVENTION
Child-related factorsAge and developmentBurns in very young <strong>child</strong>ren often occur from a mixtureof curiosity and awkwardness. In <strong>child</strong>ren under the age offour years, the level of motor development does not matchthe <strong>child</strong>’s cognitive and intellectual development andinjuries can thus occur more easily (61).Infants under the age of <strong>on</strong>e year are in a particularcategory, as their mobility starts to develop and theyreach out to touch objects (13). C<strong>on</strong>sequently, burns to thepalms of the hands are particularly comm<strong>on</strong>, as a resultof touching heaters or hot-water pipes. Because a <strong>child</strong>has thinner skin <strong>on</strong> the palms and slower withdrawalreflexes, such c<strong>on</strong>tact burns may be deep and thus requireprol<strong>on</strong>ged and careful therapy during the healing phase toprevent flexure c<strong>on</strong>tractures of the hand (40).Scald burns are the most frequent type of burn am<strong>on</strong>g<strong>child</strong>ren under the age of six years – an observati<strong>on</strong> thatappears to cut across geographic and ec<strong>on</strong>omic groups.Typical scald burns occur when a <strong>child</strong> pulls down ac<strong>on</strong>tainer of hot fluid, such as a cup of coffee, <strong>on</strong>to his orher face, upper extremities and trunk. These are typicallysuperficial sec<strong>on</strong>d-degree burns. Apart from the painthey cause the <strong>child</strong> and the distress for the parents, theseburns will typically heal within weeks, leaving little or nopermanent damage.As <strong>child</strong>ren grow older, they become less likely to beinjured by comm<strong>on</strong> household objects and more interestedin the world outside. There is then an increased likelihoodthat they will be involved in serious fires. In particular,boys older than 6 or 8 years of age often become curiousabout fire, leading to experimentati<strong>on</strong> with matches,lighters or fireworks. In some cases, younger siblings areinjured while watching the experimentati<strong>on</strong> of an olderbrother or sister (62).GenderAs already menti<strong>on</strong>ed, burns are the <strong>on</strong>ly type of fatal<strong>injury</strong> that occurs more frequently am<strong>on</strong>g girls than boysin three WHO regi<strong>on</strong>s (see Table 4.2). For n<strong>on</strong>-fatal burns,the pattern is not quite as clear, and in some settings boysmay be at a greater risk of burns than girls, perhaps asa result of the more inquisitive nature of boys and theirgreater risk-taking behaviours (63, 64).Local customs of using open fires for cooking andheating, together with the wearing of loose-fitting clothing,particularly am<strong>on</strong>g teenage girls in the South-East Asiaand Eastern Mediterranean regi<strong>on</strong>s (30), are associatedwith an increased rate of burns am<strong>on</strong>g young women (1).VulnerabilitySome <strong>child</strong>ren are more vulnerable to burns than others.Disabled <strong>child</strong>ren have a significantly higher incidence ofburn injuries than n<strong>on</strong>-disabled <strong>child</strong>ren (65). Althoughnot specific to <strong>child</strong>ren, those who suffer from unc<strong>on</strong>trolledepilepsy appear to be at greater risk for burn injuries. Suchinjuries are often severe enough to require admissi<strong>on</strong> tohospital (66).Other vulnerable groups – such as <strong>child</strong>ren of asylumseekers (67), those living in high-income countries butborn to foreign parents (68), as well as <strong>child</strong>ren in ruralareas distant from medical care – have higher incidencesof burns and of their c<strong>on</strong>sequences (69).Am<strong>on</strong>g street <strong>child</strong>ren, there have been numerousjournalistic <str<strong>on</strong>g>report</str<strong>on</strong>g>s, though few scientific studies, <strong>on</strong> howthey may be burned while sleeping in derelict buildings,underground sewers or close to open fires. Apart from thedanger from flames, the inhalati<strong>on</strong> of hydrocarb<strong>on</strong>s or thesniffing of glue am<strong>on</strong>g street <strong>child</strong>ren can lead to burns ofthe trachea (70).Studies have also found that the <strong>child</strong>ren of parents whosmoke while in bed are at higher risk of burns than thosewho do not have parents who smoke (71).PovertyMortality and morbidity from burns are str<strong>on</strong>gly associatedwith poverty. In additi<strong>on</strong> to the markedly higher incidenceof burns am<strong>on</strong>g <strong>child</strong>ren in low-income and middle-incomecountries, there are also differences by socioec<strong>on</strong>omic classwithin high-income countries, with studies from Swedenand the United Kingdom showing an increased risk of burnsam<strong>on</strong>g poorer <strong>child</strong>ren (72, 73). In Sweden, the relative riskof being hospitalized for a burn was 2.3 times higher for<strong>child</strong>ren in the poorest socioec<strong>on</strong>omic group than am<strong>on</strong>gthose in the most prosperous group. Furthermore, withinTABLE 4.2Fatal fire-related burn rates per 100 000 <strong>child</strong>ren a by sex, WHO regi<strong>on</strong> and country income level, <str<strong>on</strong>g>World</str<strong>on</strong>g>, 2004Africa Americas South- East Asia Europe Eastern Mediterranean Western PacificLMIC HIC LMIC LMIC HIC LMIC HIC LMIC HIC LMICBoys 8.9 0.7 0.7 3.3 0.2 1.3 0.6 3.6 0.3 0.4Girls 8.5 0.6 0.6 9.1 0.2 1.0 0.1 5.8 0.3 0.8aThese data refer to those under 20 years of age.HIC = High-income countries; LMIC = low-income and middle-income countries.Source: WHO (2008), Global Burden of Disease: 2004 update.WORLD REPORT ON CHILD INJURY PREVENTION 85
the poorest group, the risk for burns was greater than forany other <strong>child</strong>hood <strong>injury</strong> (73). In Australia, too, the riskof fire-related burns and scalds requiring a hospital stay wasfound by <strong>on</strong>e study to increase as income decreases (74).This finding was c<strong>on</strong>firmed by a systematic review of therisk factors for <strong>injury</strong> in a house fire. The review found thatthose in the lowest quintile of income were 2.4 times morelikely to die in a house fire than those in the highest twoincome quintiles (71).Agent factorsUnsafe equipmentHeat, light sources and cooking equipment – especiallythose relying <strong>on</strong> fossil fuels – all carry inherent risks (75).In particular, heating or cooking <strong>on</strong> open fires that are notenclosed or that stand at ground level pose significant dangersto <strong>child</strong>ren. There are similar dangers in the use of smallkerosene stoves or lanterns, candles for lighting, and othervolatile or highly flammable fuels within the house (75–78).Easy access for <strong>child</strong>ren to cooking appliances or pots withboiling liquids is a further risk factor for burns (76, 79, 80).Unsafe electrical appliances, plugs, wires and otherc<strong>on</strong>necti<strong>on</strong>s all increase the risk of electrical burns for<strong>child</strong>ren (21, 80).Flammable substancesFlammable substances such as kerosene and paraffinshould not be stored in the house. However, for practicalreas<strong>on</strong>s, they are not usually stored in this way. Apart fromthe obvious danger of fire, they are also a pois<strong>on</strong>ing risk forsmall <strong>child</strong>ren, being frequently kept in c<strong>on</strong>tainers lacking<strong>child</strong>-resistant closures (see Chapter 6).FireworksMany countries celebrate religious or nati<strong>on</strong>al festivalsby setting off fireworks and many burn injuries regularlyoccur around these holidays (75, 81, 82). Fireworks pose asignificant risk for <strong>child</strong>ren, particularly adolescent boys.In Greece, 70% of firework burn injuries recorded by thecountry’s <strong>injury</strong> surveillance system involved boys aged 10to 14 years, usually as a result of setting off the fireworksthemselves. Girls who were injured by fireworks wereusually bystanders (81). In Australia, 50% of those injuredby fireworks were boys under 18 years of age (83).Fireworks have been banned in many high-incomecountries unless they are safely set off by professi<strong>on</strong>als aspart of a public display. In most low-income and middleincomecountries, there are no laws restricting the use offireworks. However, in some countries that ban the privateuse of fireworks, injuries from them nevertheless occur,usually in adolescent males (62, 83, 84). In the state ofMinnesota in the United States, after a law banning privatefireworks had been repealed, there was an increase in thenumber of <strong>child</strong>ren suffering burns (85).Envir<strong>on</strong>mental factorsCooking and living areasThe overwhelming majority of <strong>child</strong>hood burns occur in thehome, and in particular in the kitchen. It has been suggestedthat the locati<strong>on</strong> within the home of the heating equipmentand the structure of the kitchen may present significantrisks to <strong>child</strong>ren (86). In South Africa, for example, manyhomes c<strong>on</strong>sist of <strong>on</strong>e or two main rooms, that are divided bytemporary internal divisi<strong>on</strong>s made of curtains or cardboard.These rooms are utilized for functi<strong>on</strong>s such as sleeping,washing, cooking and eating, depending <strong>on</strong> the time of dayand the requirements of the family (86, 87), or else as a workspace (88). This type of domestic arrangement may greatlyincrease the exposure of a <strong>child</strong> to domestic equipment andsources of heat (89, 90).Socioec<strong>on</strong>omic envir<strong>on</strong>mentA number of case-c<strong>on</strong>trol and descriptive studies c<strong>on</strong>ductedin different parts of the world have identified severalsocioec<strong>on</strong>omic factors that increase the risk of <strong>child</strong>hoodburns (74, 75, 77, 79, 91–93). These factors include:– a low rate of literacy within the family;– living in overcrowded dwellings or with cluttered areasin the home;– a failure of proper supervisi<strong>on</strong> of <strong>child</strong>ren;– a history of burns am<strong>on</strong>g siblings;– the absence of laws and regulati<strong>on</strong>s relating to buildingcodes, smoke detectors and flammable clothing.Time of incidentTwo peak times of the day have been <str<strong>on</strong>g>report</str<strong>on</strong>g>ed for incidentsinvolving burns – the late morning, when domestic tasksare being d<strong>on</strong>e, and around the time for the evening meal(29, 94). There have also been peaks noted, in some regi<strong>on</strong>sof the world, by seas<strong>on</strong> of the year. In tropical climates,where heating, even in winter, is not generally required,there is a fairly even distributi<strong>on</strong> of cases of burnsthroughout the year (28, 38). In places where the wintersare cold, though, an increased incidence of burns tendsto be recorded during winter (94–97). The associati<strong>on</strong>,in many countries, of incidence of burns with public orreligious holidays has already been noted.Lack of access to waterInadequate access to a good supply of water – in the form ofa tap, hosepipe or sprinkler system – to douse flames or stopthe flames spreading, is a str<strong>on</strong>g risk factor (74). Similarly, alack of smoke detectors or the presence of n<strong>on</strong>-functi<strong>on</strong>ingsmoke detectors appears to be related, in some developedcountries, to an increased risk for <strong>child</strong>hood burns (98).Protective factorsSeveral protective factors have been shown to reduce therisk of burns or to minimize their c<strong>on</strong>sequences (74, 75,77, 99), including:86 WORLD REPORT ON CHILD INJURY PREVENTION
– literacy, particularly am<strong>on</strong>g mothers;– knowledge of the risk of burns and of health-careservices;– ownership of the house;– having living rooms separate from the kitchen;– the use of fire-retardant fabrics for clothes;– the installati<strong>on</strong> of smoke detectors and water sprinklers;– appropriate first-aid and emergency resp<strong>on</strong>se systems;– the existence of good quality health-care services.Interventi<strong>on</strong>sThis secti<strong>on</strong> summarizes some of the interventi<strong>on</strong>s to preventvarious types of burn injuries am<strong>on</strong>g <strong>child</strong>ren. The mainprotective factors for burns are briefly listed, and three broadapproaches for preventi<strong>on</strong> are described, namely:– engineering, design and envir<strong>on</strong>mental measures;– the introducti<strong>on</strong> of legislati<strong>on</strong> and standards;– educati<strong>on</strong>al measures.A fourth, and effective, approach c<strong>on</strong>sists of acombinati<strong>on</strong> of the three earlier <strong>on</strong>es. The managementof burns, in particular first aid, and the value of dedicatedtrauma centres and of proper rehabilitati<strong>on</strong> are discussedin a separate secti<strong>on</strong>.Engineering measuresSafer lamps and stovesIn many low-income and middle-income countries,the lamps and stoves for lighting and heating use fossilfuels. These lamps and stoves are comm<strong>on</strong>ly linked to<strong>child</strong>hood burns. Developing safe stoves and movingthem out of doors and off the ground would not <strong>on</strong>lyreduce the number of burns sustained by <strong>child</strong>ren butalso reduce their exposure to indoor fumes. A trial inrural Guatemala of an improved wooden stove produceda decrease in both acute lower respiratory infecti<strong>on</strong>s andfire-related burns. Rigorous evaluati<strong>on</strong> of this trial is stillin progress (100).In Sri Lanka, an interventi<strong>on</strong> using safe lamps forlighting is being implemented (see Box 4.3). Although thisproject too is awaiting evaluati<strong>on</strong>, the initial results appearpromising.BOX 4.3Cheap and safe alternatives to traditi<strong>on</strong>al paraffin lampsParaffin oil (also known as kerosene) is a flammable fuel, used widely in some countries for lamps. According to the <str<strong>on</strong>g>World</str<strong>on</strong>g> Bank Global Data M<strong>on</strong>itoringInformati<strong>on</strong> System 1 , <strong>on</strong>ly 29% of households in sub-Saharan Africa are electrified, while in most countries in South Asia two out of three houseshave electricity. While there are efforts in all these countries to provide more homes with electricity, progress is often slow. The global use of paraffinis therefore likely to c<strong>on</strong>tinue for many years. At the same time, there is an urgent need for cheap and safe paraffin lamps.A properly designed paraffin lamp it is not by itself unsafe for use in the home, even though it carries a flame. Like the kitchen knife, it is safeif well-designed and used with the proper basic safeguards. Unfortunately, paraffin lamps designed with safety in mind are relatively expensive.Around the world, milli<strong>on</strong>s of families use makeshift paraffin lamps that are very cheap – but unsafe. Poverty is the main factor here, though ignoranceof the fact that their lamps pose a serious danger also plays a part.In Mozambique, people use a lamp known as a xiphefo, c<strong>on</strong>sisting of a tall bottle with a wick-carrier placed <strong>on</strong> its top. In Sri Lanka, some lampsare made out of discarded medicine bottles, while others are burnt-out light bulbs fitted with a wire frame and metal base. Both types are light inweight and could easily topple, igniting the clothes of a <strong>child</strong> sitting or sleeping nearby.People in these places have been accustomed to their traditi<strong>on</strong>al lamps from <strong>child</strong>hood. Marketing a safe alternative that is radically differentwould be difficult to accomplish. A str<strong>on</strong>g promoti<strong>on</strong>al campaign <strong>on</strong> safety is therefore needed. People should be told how to use paraffin lampssafely, and, am<strong>on</strong>g other things:– not to add paraffin to burning lamps;– not to place lamps at the edge of a table or other raised surface;– not to hang the lamps <strong>on</strong> walls;– not to use c<strong>on</strong>tainers for paraffin that previously c<strong>on</strong>tained petrol.The unsafe, makeshift lamps that are used by poor people cost very little. Therefore any alternative that is proposed has to be as cheap as possible.There are two opti<strong>on</strong>s. The first is the use of a safer oil, in place of the paraffin in the existing lamps. Vegetable oils such as those of coc<strong>on</strong>ut,sesame, neem and mustard are safe, but their disadvantage is that they do not rise in the wick-carrier.The sec<strong>on</strong>d opti<strong>on</strong> is for a lamp that is safe, even with paraffin. Such a lamp is, in fact, currently being marketed in Sri Lanka to good effect. Itsprincipal features are:It is short and heavy, so that it does not easily tip over.It has two flat sides, so that even if it tipped over, it would not roll.It has a screw-<strong>on</strong> metal lid, to prevent oil spilling if it tips over.Its design is simple and it can be mass-produced at low cost.It has a near-globular shape and is made of thick glass, so that it does not crack if it falls.There are no delicate or moving parts, so that it can be used for several years.The use of such a lamp, with appropriate basic care being exercised, could prevent the many paraffin burns that occur around the world each year,though its efficacy has yet to be subjected to rigorous evaluati<strong>on</strong>.1Available at web site: http://ddp-ext.worldbank.org/ext/GMIS/gdmis.do?siteId=1&menuId=IDA14RMS10WORLD REPORT ON CHILD INJURY PREVENTION 87
Families in many developing countries will c<strong>on</strong>tinue touse fossil fuels for heating and cooking, until such time asthe cost of electricity and of essential electrical appliancesbecomes affordable (101).Smoke alarmsEvidence for the effectiveness of interventi<strong>on</strong>s existsmost markedly in the case of smoke detectors, whichhave been found to reduce the risk of deaths by over 70%(102). The problem, though, is to make sure that all homeshave working smoke alarms <strong>on</strong> all levels of the residence,including in the sleeping areas. People often remove thebatteries from their smoke detectors to avoid the nuisanceof false alarms, or else do not check the batteries regularly.For optimum protecti<strong>on</strong>, most smoke detectors requirethat they be tested m<strong>on</strong>thly and that their battery bechanged twice a year. However, there are new devices,which – while more expensive – make use of a 10-yearbattery. Fully integrated, hard-wired smoke alarms oftennow come with the new types of residential c<strong>on</strong>structi<strong>on</strong>,at least in some developed countries.A systematic review of c<strong>on</strong>trolled trials of interventi<strong>on</strong>spromoting smoke alarms found that approaches thatused <strong>on</strong>ly educati<strong>on</strong> produced <strong>on</strong>ly modest benefits.Programmes that provided and installed smoke alarmsappeared to reduce fire-related injuries (103). However,programmes that combined legislati<strong>on</strong> <strong>on</strong> smoke alarmswith installati<strong>on</strong> and educati<strong>on</strong> seemed to result in thegreatest benefit (104).A study in the United States (105) evaluated the costeffectivenessof smoke detectors and found the ratio of thecost of detectors to the saving in health-care costs to be1:26.Residential sprinklersFire sprinkler systems have been proved to be effective (106)and can now be found widely in public and commercialproperty in many countries. Home sprinkler systems, <strong>on</strong>the other hand, are recommended but not widely used,though in some countries governments require them tobe installed in the c<strong>on</strong>structi<strong>on</strong> of new homes.Fire-retardant household materialsModifying products associated with fire-related burnsis a promising approach. Following the introducti<strong>on</strong>in Australia of fire-retardant material for <strong>child</strong>ren’sbedclothes in 1979, the annual number of burns relatedto clothing dropped from around 300 to 30 (107). Inthe United States, <strong>child</strong>ren’s bedclothes are regulated bythe United States Product Safety Commissi<strong>on</strong>. Certaintypes and sizes of clothes need to pass a flammabilitytest or else be tight-fitting, so as to reduce the risk ofburns (108). In additi<strong>on</strong>, many countries require thatbedding, mattresses and upholstered furniture be fireretardant.Envir<strong>on</strong>mental measuresPromising envir<strong>on</strong>ment modificati<strong>on</strong>s that may reducethe incidence of burns include, am<strong>on</strong>g others:– introducing new or stricter building codes andstandards;– modifying or improving c<strong>on</strong>structi<strong>on</strong> materials;– improving heating and lighting equipment in homes;– raising cooking facilities off the ground;– separating cooking areas from living areas.Unfortunately, although promising, such preventi<strong>on</strong>measures have not been well evaluated, particularly inlow-income and middle-income countries.A Cochrane review of interventi<strong>on</strong>s that altered thehome envir<strong>on</strong>ment to reduce all types of <strong>injury</strong>, includingburns, c<strong>on</strong>cluded that there is still insufficient evidence todetermine their effectiveness (109).Laws and regulati<strong>on</strong>sLaws and regulati<strong>on</strong>s are <strong>on</strong>e of the most efficient waysto get people to adopt safe behaviours. In additi<strong>on</strong> tolegislati<strong>on</strong> enforcing smoke detectors, which has proveneffective in many high-income countries, three othermeasures appear to be effective – laws <strong>on</strong> the temperatureof hot-water taps, banning fireworks and standards for<strong>child</strong>-resistant lighters.Temperature of hot-water tapsInterventi<strong>on</strong>s to prevent scald burns focus primarily<strong>on</strong> educati<strong>on</strong> together with laws and their enforcementregulating the temperature of hot water from householdtaps (110). In the United States, the c<strong>on</strong>trol of hot-watertemperature in taps in the state of Washingt<strong>on</strong> reducedthe number of domestic hot-water scalds by combining aneducati<strong>on</strong>al programme with laws cutting the temperaturein preset water heaters from 60°C to 49°C (111, 112). Asa result, 84% of homes changed to lower temperature.Other educati<strong>on</strong>al interventi<strong>on</strong>s in Norway (113) and NewZealand (114) aimed at reducing the hot-water temperaturewere also successful in reducing burns. A Canadian studyevaluated the effectiveness of a combined educati<strong>on</strong>al andlegislative approach to reduce thermostat settings andfound a 56% reducti<strong>on</strong> in scald burns (58).Child-resistant lightersA survey in the United States in 1985 showed that <strong>child</strong>renplaying with lighters were the cause of residential firesresulting in 170 deaths and 1150 injuries annually in thecountry (115). As a result, the United States C<strong>on</strong>sumerProduct Safety Commissi<strong>on</strong> developed a standard forcigarette lighters that applied to all products manufacturedor imported into the country. A study after this standardwas introduced found that fires, deaths and injuries causedby young <strong>child</strong>ren playing with lighters had been reducedby as much as 58%, saving over half a billi<strong>on</strong> US dollars in88 WORLD REPORT ON CHILD INJURY PREVENTION
societal costs in 1998 al<strong>on</strong>e (116). Other countries followedthe United States example. In 2007, the European Uni<strong>on</strong>introduced laws requiring manufacturers and importersto comply with the European standard for <strong>child</strong>-resistantlighters (117). Although <strong>child</strong>-resistant lighters are not asubstitute for parental supervisi<strong>on</strong>, c<strong>on</strong>siderable savings tothe health sector and society could be made if all countriesadopted similar standards.Banning of fireworksMany high-income countries have banned fireworkpurchase or ownership by <strong>child</strong>ren. A recent review in theUnited Kingdom revealed that since the introducti<strong>on</strong> ofthe Fireworks Act in 2003 and the Fireworks regulati<strong>on</strong>in 2004 which limited the sale of fireworks to the threeweeks surrounding B<strong>on</strong>fire Night, and banned the sale orpossessi<strong>on</strong> of fireworks by under 18 year olds, more than80% of <strong>child</strong>ren’s firework injuries were seen in the threeweeks surrounding B<strong>on</strong>fire Night. They c<strong>on</strong>cluded thatthe law had a definite impact <strong>on</strong> reducing n<strong>on</strong>-B<strong>on</strong>firerelated firework injuries, but that stricter enforcement wasrequired (118).Educati<strong>on</strong>al approachesIncreased knowledge about burns am<strong>on</strong>g young <strong>child</strong>renhas been shown to result from educati<strong>on</strong>al programmesin schools and communities (119). It is unclear, though,whether these programmes have any effect in reducing theincidence of burns, as they lack a rigorous evaluati<strong>on</strong> ofthe l<strong>on</strong>g-term outcomes of burn injuries (120).Community programmes to ensure good supervisi<strong>on</strong>of <strong>child</strong>ren, particularly those with disabilities, to educateparents about burns and to advise against the storageof flammable substances in the home, have all beenproposed as primary preventi<strong>on</strong> strategies for burns (92).A programme in Bangladesh involves <strong>child</strong>ren beingplaced in nurseries for a number of hours each day. Thepurpose is to give the mothers free time for their domestictasks, so that they can be more attentive when the <strong>child</strong>renreturn home. The programme has yet to be evaluated forits effectiveness in preventing burns or drowning.Educating parents about the use of safety equipmenthas been shown to result in increased knowledge, butagain it has not been possible so far to dem<strong>on</strong>strate that asa result there is better use of such equipment (121, 122). Theeffectiveness of home visitati<strong>on</strong> programmes is similarlyuncertain. In general, educati<strong>on</strong>al programmes appearmore successful when coupled with increasing access tosafety products or with changes in the law.Combined strategiesStrategies which combine legislati<strong>on</strong> and standards,product modificati<strong>on</strong> and educati<strong>on</strong> appear to have themost far-reaching effects in reducing the incidence ofburns (see Box 4.4).BOX 4.4“Hot water burns like fire”In 1992, the Australian state of New South Wales launched the country’sfirst state-wide preventi<strong>on</strong> campaign for scalds in <strong>child</strong>ren, entitled“Hot Water Burns Like Fire”. This followed a <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> injuriesin emergency departments that showed scalds as the fourth-leadingcause of hospitalizati<strong>on</strong> am<strong>on</strong>g young <strong>child</strong>ren. The main agentsof scalds identified were: hot tap water, hot beverages, kettles andsaucepans. As a result of this campaign, the whole of Australia nowhas laws mandating a maximum temperature of 50° C for hot watertaps in bathrooms – for new installati<strong>on</strong>s fitted and old <strong>on</strong>es thatare replaced.The first phase of the campaign aimed to raise awareness aboutthe causes of scalds to <strong>child</strong>ren, the most serious and preventable<strong>on</strong>e being hot tap water. This phase involved community heath-carestaff, health promoti<strong>on</strong> pers<strong>on</strong>nel, retailers, plumbers and the membersof the hot-water heating industry.The sec<strong>on</strong>d phase, beginning in 1994, focused <strong>on</strong> how to modifytemperatures of hot-water taps in bathrooms. Following meetingsinvolving experts in infecti<strong>on</strong> c<strong>on</strong>trol and manufacturers of hot-waterheating, an amendment to the nati<strong>on</strong>al standards <strong>on</strong> hot waterdelivery for pers<strong>on</strong>al purposes was introduced. Each state was thenobliged to change its plumbing code so that the delivery of hot waterin homes was capped at 50° C. This involved the use of a temperaturetesting card and a brochure with instructi<strong>on</strong>s <strong>on</strong> how to test andmodify the temperature.Between 1989 and 1996, the rate of hospitalizati<strong>on</strong>s for scaldsinvolving young <strong>child</strong>ren aged 0–4 years fell by 13%. In the same period,the durati<strong>on</strong> length of hospital stay dropped by 18%. The combinedeffect of the reduced number and severity of cases resulted ina net 27% fall in the total number of hospital beds utilized. Rates forthe most serious scalds (involving a stay of 10 days or more) showedthe greatest decline – a reducti<strong>on</strong> of 30% for the two years followingthe sec<strong>on</strong>d stage of the campaign. In all, there was an annual savingto the health care system of between 3.8 and 6.5 milli<strong>on</strong> Australiandollars, based <strong>on</strong> an average cost of treating a serious scald.© K McGeeWORLD REPORT ON CHILD INJURY PREVENTION 89
Managing burnsAccess to treatment and rehabilitati<strong>on</strong>Although the care of burns depends largely <strong>on</strong> theavailability of financial and human resources, manycountries still manage to deliver good quality care despitelimited health budgets. A number of cheaper opti<strong>on</strong>s forburns management are currently being evaluated. Theseinclude:– open, as against closed techniques to manage wounds(123);– less costly grafting techniques (124).In additi<strong>on</strong>, practical guides for managing paediatricburns are being promoted in developing countries (125).In many places the cost of treatment is high and <strong>on</strong>lythose who are well-off can afford to take their <strong>child</strong>rento hospital (38). This can result in delayed healing,c<strong>on</strong>tractures and superimposed infecti<strong>on</strong>s.Families frequently resort to using traditi<strong>on</strong>al methodsof healing before attempting to access modern medicine,because of the difficulty of accessing such health care (27,126).First aid for burnsFollowing a burn, the <strong>child</strong> should be stabilized beforebeing transported to hospital. This is usually d<strong>on</strong>e byfamily, bystanders or first resp<strong>on</strong>ders and should followthe basic rules of what should and should not be d<strong>on</strong>e inthese circumstances (see Table 4.3). The overall aim mustbe to cool the burn, prevent <strong>on</strong>going burning and preventc<strong>on</strong>taminati<strong>on</strong>.There are many studies assessing the first aid of burns inhigh-income countries, and from these, examples of goodpractices – such as to “cool the burn” – are drawn. Coolingthe burn surface is <strong>on</strong>e of the oldest methods of treatment(127). However, <strong>on</strong>ly a handful of studies have examinedburn interventi<strong>on</strong>s in low-income and middle-incomecountries. A survey in India found that <strong>on</strong>ly 22.8% ofpatients had received appropriate first aid for their burns.The remainder had either received no first aid or elseinappropriate treatment – such as raw eggs, toothpaste,mashed potato or oil being rubbed into the burn (32). InViet Nam, a study compared <strong>child</strong>ren who had receivedimmediate cooling with water after a burn with thosewho had not. It turned out that those who had receivedproper first aid needed 32% less subsequent grafting (128).Educati<strong>on</strong> <strong>on</strong> the effect of immediate applicati<strong>on</strong> of cool(not ice cold) water to burns should be promoted widely asan effective first-aid treatment.Acute management of burnsMedical care for burns has markedly improved survival.In the United States in 1940, 50% of <strong>child</strong>ren with burnsinvolving 30% or more of their total body surface died.In 2000, a study in the same country found no deaths in<strong>child</strong>ren with burns involving as much as 59% of bodysurface area (129). In Pakistan, <strong>on</strong> the other hand, burnsof over 40% in <strong>child</strong>ren are still often fatal (see Box 4.5).Once a <strong>child</strong> suffering burns has been transported toan acute care facility, assessment and stabilizati<strong>on</strong> initiallyfocus <strong>on</strong> a survey of airway, breathing and circulati<strong>on</strong>.There should also be a careful examinati<strong>on</strong> of the <strong>child</strong>from head to toe, looking for other signs of trauma.Children with sec<strong>on</strong>d-degree burns usually presentwith intense pain and typically hold the affected limbsimmobile in a positi<strong>on</strong> of comfort. The site of the burnshould immediately be assessed to determine its severity.Pain management in such cases is essential.For reas<strong>on</strong>s that are not yet understood, when the sizeof a burn exceeds 15% to 20% of body surface area of theaffected <strong>child</strong>, the inflammatory resp<strong>on</strong>se extends bey<strong>on</strong>dthe local site of <strong>injury</strong>. Blood pressure becomes dangerouslylow, and if fluids are not given fast enough, the <strong>child</strong> willgo into shock and die. If the <strong>child</strong> does survive the first48 hours, there is still a risk of death from infectiouscomplicati<strong>on</strong>s, since the barrier to bacteria is broken andthe immune system suppressed.The overall aim of managing burn wounds is to closethe wound as quickly as possible, either by allowing theTABLE 4.3First aid for burnsWhat not to doDo not commence first aid before ensuring your own safety(switch off electrical current, wear gloves for chemicals, etc.).Do not apply paste, oil, kumkum (a paste made from turmeric) –or raw cott<strong>on</strong> to the burned area.Do not apply ice.Do not open the blisters with a needle or pin.Do not apply any material directly to the wound as it mightbecome infected.Avoid applicati<strong>on</strong> of topical medicati<strong>on</strong> until the patient has beenplaced under appropriate medical care.What to doStop the burning process by removing clothing and irrigating thewounds.Apply cold water or allow the burnt area to remain in c<strong>on</strong>tact with coldwater for some time.In flame injuries, extinguish the flames by allowing the patient to roll<strong>on</strong> the ground, or by applying a blanket, or using water or other fireextinguishingliquids.In chemical burns, remove or dilute the chemical agent by copiouslyirrigating the wound with water.Obtain medical care.Source: reference 1.90 WORLD REPORT ON CHILD INJURY PREVENTION
BOX 4.5Managing burns in PakistanBurns are <strong>on</strong>e of the most neglected areas of health care in developing countries. These countries have 90% of global burn injuries, with 70% ofthese injuries occuring in <strong>child</strong>ren. While there have been major improvements in burn care in many high-income countries, making it quite possiblefor patients with burns of more than 90% of body surface area to survive, in countries such as Pakistan, burns of over 40% are frequently fatal. Evenminor burns can lead to significant illness as a result of recurrent wound infecti<strong>on</strong>s, delayed wound healing and the formati<strong>on</strong> of c<strong>on</strong>tractures.There are various reas<strong>on</strong>s for this poor outcome. Access to care may be impeded by difficult terrain, as well as by a lack of pre-hospital services andinefficient chains of referral. Even if the patient manages to reach a health-care facility, initial resuscitati<strong>on</strong> procedures are frequently inadequate.Appropriate airway management, mechanical ventilati<strong>on</strong> and aggressive fluid resuscitati<strong>on</strong> are often not provided in the first few hours.Burn care has become highly specialized and is performed at dedicated centres. These specialized instituti<strong>on</strong>s not <strong>on</strong>ly provide comprehensiveclinical care but also serve as important research centres. In several developed countries, burn centres have existed for more than 60 years.Today, the United States has 70 burn centres. In Pakistan, there are <strong>on</strong>ly eight specialized burns units for a populati<strong>on</strong> of 150 milli<strong>on</strong> people.Their standards of care vary c<strong>on</strong>siderably, depending <strong>on</strong> the workload,the availability of funding and the quality of management. There are n<strong>on</strong>ati<strong>on</strong>ally-agreed standards or ways in which to enforce standards. Inthe whole of Pakistan, there are currently <strong>on</strong>ly 15 to 20 surge<strong>on</strong>s whoare burn care specialists.The ability of health-care specialists to manage sepsis and inhalati<strong>on</strong>al<strong>injury</strong> often defines the eventual outcome in patients with burns. Managingsepsis requires meticulous aseptic wound treatment and surgical debridement,and the early recogniti<strong>on</strong> and aggressive treatment of sepsisand septic shock, as well as nutriti<strong>on</strong>al support. Similarly, inhalati<strong>on</strong>al<strong>injury</strong> often requires l<strong>on</strong>g periods of mechanical ventilati<strong>on</strong> under the supervisi<strong>on</strong>of an experienced critical care worker.Burn care is also expensive. In Karachi, the daily average cost of treatinga patient with a major burn of 25% or more of body surface area isaround US$120, and a hospital stay can last as l<strong>on</strong>g as 8 to 10 weeks. Theec<strong>on</strong>omics of burn care discourages the creati<strong>on</strong> of burns centres in theprivate sector and fails to attract committed staff.© A. Harry/AFROskin to heal by sec<strong>on</strong>dary intenti<strong>on</strong> (allowing the wound toheal over <strong>on</strong> its own) or through surgical closure (grafting).The management of small, deep sec<strong>on</strong>d-degree burns hasevolved into an efficient and effective plan of treatmentthat nowadays produces highly satisfactory cosmetic andfuncti<strong>on</strong>al results with minimal morbidity. The treatmentplan has two comp<strong>on</strong>ents: excising the burn wound beforesuppurati<strong>on</strong> occurs; and covering the excised wound withsynthetic or biological wound coverings. However, large,deep sec<strong>on</strong>d-degree or third-degree burns, particularly in<strong>child</strong>ren, c<strong>on</strong>tinue to pose a significant problem for theburn surge<strong>on</strong>.The surgical approach to early excisi<strong>on</strong> and graftingof burn wounds involves trained pers<strong>on</strong>nel and safeand effective resources. As removing the burn woundis a procedure associated with a high volume of bloodloss, the operati<strong>on</strong> cannot be performed unless there arefacilities in the hospital to provide blood for transfusi<strong>on</strong>s.The management of <strong>child</strong>ren around the time of such anoperati<strong>on</strong> is very complicated and requires collaborati<strong>on</strong>with experienced anaesthesiologists (125). The postoperativecare of the grafted wounds and the areas fromwhich skin has been taken for the grafts calls for a team oftrained nurses and occupati<strong>on</strong>al and physical therapists.For these reas<strong>on</strong>s, early excisi<strong>on</strong> and grafting may not bean appropriate course to be taken in some low-incomecountries.Sadly, the usual fate of a <strong>child</strong> with an extensive thirddegreeburn in a low-income country is death. The riskof mortality from burns covering over 30% of total bodysurface area is roughly 50%. The risk of burns coveringmore than 50% of total body surface area is nearly 100%(56). For those <strong>child</strong>ren who survive such severe burns,most are left with unsightly scarring, resulting in bothphysical and psychological disability.Dedicated trauma centresNot all <strong>child</strong>ren require treatment from a dedicatedtrauma centre. A large number of countries now have suchcentres and criteria exist for deciding which patients aretransferred to them. The American College of Surge<strong>on</strong>sand the American Burn Associati<strong>on</strong> recommend that<strong>child</strong>ren with the following c<strong>on</strong>diti<strong>on</strong>s should be treatedin a burns centre (130):– partial thickness (sec<strong>on</strong>d-degree) burns greater than10% of the total surface area of the body;– burns involving the face, hands, feet, genitalia, perineumor major joints;– full-thickness (third-degree) burns;WORLD REPORT ON CHILD INJURY PREVENTION 91
– electrical burns, including injuries from lightning;– chemical burns;– injuries from inhaling smoke;– pre-existing medical disorders that could complicatethe management of burns, prol<strong>on</strong>g recovery or affectsurvival;– accompanying trauma, where the burn <strong>injury</strong> poses thegreater risk of morbidity or mortality.While it is well established that trauma systems preventunnecessary deaths in patients with blunt or penetratinginjuries (131), there are few data to sustain this argument inthe care of burn patients (132). N<strong>on</strong>etheless, expert opini<strong>on</strong>supports the claim that patients with serious burns willhave better outcomes and with less costly management ifthey are in a dedicated burn centre (133).Rehabilitati<strong>on</strong> facilitiesChildren who sustain burns deserve the best rehabilitati<strong>on</strong>facilities available, so that they are able to return toproductive and meaningful roles within their community.The requirements for rehabilitati<strong>on</strong> should be discussedduring the acute phase and should involve not <strong>on</strong>ly physicalbut also psychological therapy (see Box 4.6). Inadequaterehabilitati<strong>on</strong> can result in physical and psychologicaldamage with a serious lifel<strong>on</strong>g effect.BOX 4.6Rehabilitati<strong>on</strong> for paediatric burn survivors in South AfricaBurn injuries are tragic, largely preventable and frequently have lifel<strong>on</strong>g c<strong>on</strong>sequences for the young patient. In South Africa these injuries are <strong>on</strong>the increase. This is due to factors such as poverty, illiteracy, a lack of resources, urban migrati<strong>on</strong> and the c<strong>on</strong>sequent rising number of makeshifthousing settlements.New developments and improvements in burn care generally have led to increased survival rates and a fall in the death rate. However, paediatricburn survivors need more than excellence in wound care, surgery and nursing. They also require in-depth rehabilitati<strong>on</strong>, c<strong>on</strong>sisting not <strong>on</strong>ly of physiotherapyand occupati<strong>on</strong>al therapy, but also of emoti<strong>on</strong>al support and reintegrati<strong>on</strong> into the community.An estimated 90% of <strong>child</strong>ren who have survived burns are not followed up. Once a <strong>child</strong> is discharged from hospital, the parents often do notrecognize that follow-up rehabilitati<strong>on</strong> or l<strong>on</strong>g-term rec<strong>on</strong>structive surgery may be needed. For those who do receive rehabilitati<strong>on</strong> services, theemphasis is largely <strong>on</strong> physical rehabilitati<strong>on</strong>, rather than emoti<strong>on</strong>al support and community reintegrati<strong>on</strong>. South Africa has an acute shortage ofappropriately-trained professi<strong>on</strong>als to provide for the complex rehabilitati<strong>on</strong> needs of burn survivors.At Cape Town’s Red Cross Hospital burns unit, up to 96% of <strong>child</strong>ren admitted are from disadvantaged communities. A study at this hospital inthe late 1970s found that up to 70% of severely burned <strong>child</strong>ren either attempted or actually committed suicide. In 2002, health professi<strong>on</strong>als at thehospital set up a three-tiered pilot rehabilitati<strong>on</strong> project for burned <strong>child</strong>ren and their families.The first phase of rehabilitati<strong>on</strong> starts as so<strong>on</strong> as possible during the admissi<strong>on</strong> stage. At this point individual physiotherapy, occupati<strong>on</strong>al therapyand the management of pain is arranged. A community worker will also become involved, resp<strong>on</strong>sible for parental support during this firstphase and for l<strong>on</strong>g-term follow-up of disfigured <strong>child</strong>ren during the final phase of rehabilitati<strong>on</strong>. The Red Cross Hospital is unique in including touchtherapies – such as reflexology and aromatherapy – in the management of burns, al<strong>on</strong>g with more traditi<strong>on</strong>al treatments such as music and arttherapy. This holistic approach thus attempts to deal with stress and anxiety, as well as with the general emoti<strong>on</strong>al well-being of the <strong>child</strong>.The sec<strong>on</strong>d phase is <strong>on</strong> an out-patient basis and c<strong>on</strong>tinues what was started in the first phase. The previous therapies are again offered, al<strong>on</strong>gwith such things as <strong>child</strong>ren’s yoga and creative play. The use of the African drum (jembe) has been found to be particularly successful in musictherapy.The third and final phase of rehabilitati<strong>on</strong> focuses mainly <strong>on</strong> communityand school reintegrati<strong>on</strong>. Informati<strong>on</strong> is disseminated through the massmedia <strong>on</strong> the situati<strong>on</strong> of disfigured <strong>child</strong>ren and their needs. Teachersfrom 63 township schools have received training around the preventi<strong>on</strong> ofburns and the reintegrati<strong>on</strong> into the educati<strong>on</strong> system of <strong>child</strong>ren disfiguredby burn injuries. C<strong>on</strong>tinuous educati<strong>on</strong> for <strong>child</strong>ren is the single mostimportant outcome of their successful rehabilitati<strong>on</strong>. Disfigured <strong>child</strong>renare often reluctant to return to school for fear of being ostracized. If theystay uneducated they are more likely to be unemployable. In South Africa,this could lead to the <strong>child</strong>’s ending up <strong>on</strong> the streets or in pris<strong>on</strong>.Through this programme, the Red Cross Hospital aims to provide forthe emoti<strong>on</strong>al needs of <strong>child</strong>ren who have suffered burns and help thembecome fully reintegrated into society. For financial reas<strong>on</strong>s, <strong>on</strong>ly the firstphase of the three-phase programme is being offered at present. Communityreintegrati<strong>on</strong> of burned <strong>child</strong>ren can be achieved, even in thedeveloping world. However, this requires dedicated, trained staff and thesubstantial financial resources which are sadly lacking.© R. Albertyn, RXH92 WORLD REPORT ON CHILD INJURY PREVENTION
Adapting interventi<strong>on</strong>sThe extent to which interventi<strong>on</strong>s that work in <strong>on</strong>esocioec<strong>on</strong>omic setting can be effectively transferredto another depends <strong>on</strong> several factors. The advantageof transferring an established interventi<strong>on</strong> – if that ispossible – is that resources are c<strong>on</strong>served. A decisi<strong>on</strong>,though, to implement a particular interventi<strong>on</strong> measure ina particular place should always be based <strong>on</strong> solid scientificevidence, c<strong>on</strong>siderati<strong>on</strong>s of cost, cultural appropriatenessand sustainability (134).Potentially harmful interventi<strong>on</strong>sFirst-aid treatment for burn injuries is best accomplishedwith cool water (127, 135). Traditi<strong>on</strong>al treatments, though,c<strong>on</strong>tinue to be practised. These include putting butter oroil <strong>on</strong> sunburn, and ice, aloe, sugar water, toothpaste orother household products <strong>on</strong> a sec<strong>on</strong>d-degree burn. Allthese traditi<strong>on</strong>al practices can be harmful, as they cancause the skin to slough away, leaving the tender lowerlayers susceptible to infecti<strong>on</strong>. Although some agents– such as h<strong>on</strong>ey or commercially available cold packs –may indeed have some beneficial effects, they are betteravoided. Instead, people should be advised to use <strong>on</strong>lycool, clean water.Evaluating interventi<strong>on</strong>sA number of evaluati<strong>on</strong> studies have been c<strong>on</strong>ductedin high-income countries. These include an ec<strong>on</strong>omicanalysis of 1990 that found that three quarters of<strong>child</strong>hood fire-related deaths in the home could beprevented if there were working smoke alarms, sprinklersystems, anti-scald devices, slow-burning cigarettes and<strong>child</strong>proof lighters (136).There are no systematic evaluati<strong>on</strong>s, though, of burnpreventi<strong>on</strong> strategies in low-income and middle-incomecountries. Nevertheless, a number of interventi<strong>on</strong>s appearpromising. Am<strong>on</strong>g them are: separating cooking areasfrom living areas; eliminating the storage of flammablesubstances in the house; placing cooking surfaces higherthan ground level; introducing smoke alarms; makingfirst aid available; and increasing awareness about burnsand their preventi<strong>on</strong> (137). At the same time, others, suchas community-based interventi<strong>on</strong>s and campaigns (138)and home visitati<strong>on</strong> programmes for at-risk families(139), have insufficient evidence for them to be promotedas good practices.Further research in these areas is needed so thatmodel interventi<strong>on</strong> programmes can be developed forimplementati<strong>on</strong> in countries that share a similar patternof <strong>child</strong>hood burns.C<strong>on</strong>clusi<strong>on</strong>s and recommendati<strong>on</strong>sThere is overwhelming evidence that <strong>child</strong>hood burnsare largely envir<strong>on</strong>mentally c<strong>on</strong>diti<strong>on</strong>ed and preventable(93). It would therefore seem natural that the preventi<strong>on</strong>of burns should focus <strong>on</strong> a mixture of envir<strong>on</strong>mentalmodificati<strong>on</strong>s, parental educati<strong>on</strong> and product safety (seeTable 4.4).Special attenti<strong>on</strong> needs to be paid to the kitchen, thescene of the majority of burns. Programmes are neededto ensure proper supervisi<strong>on</strong> of <strong>child</strong>ren and their generalwell-being, particularly of those with disabilities. Parentsshould receive better informati<strong>on</strong> about all types of burns.There must be much greater awareness everywhere aboutthe dangers of storing flammable substances in the home.Recommendati<strong>on</strong>sA range of measures to prevent burns have been discussedin this chapter. Many of these still require rigorousevaluati<strong>on</strong>, particularly in low-income and middle-incomecountries.Those preventi<strong>on</strong> interventi<strong>on</strong>s that have provedeffective include:– laws and enforcement for the installati<strong>on</strong> of smokealarms;– <strong>child</strong>-resistant lighter standards;– laws to regulate hot-water temperature.A number of other preventi<strong>on</strong> interventi<strong>on</strong>s arec<strong>on</strong>sidered highly promising. These include:– the use of safe lamps;– the separati<strong>on</strong> of cooking areas from living areas;– the development of safer stoves.As regards measures taken after the event, two firerelated measures are str<strong>on</strong>gly recommended:– smoke alarms;– residential sprinkler system.The management of burns, from first aid torehabilitati<strong>on</strong>, is an essential comp<strong>on</strong>ent of sec<strong>on</strong>daryand tertiary preventi<strong>on</strong> strategies. Children who sufferburns require the best care available so as to minimizethe potentially serious physical and psychological l<strong>on</strong>gtermc<strong>on</strong>sequences of this type of <strong>injury</strong>.Educati<strong>on</strong>al programmes c<strong>on</strong>vey knowledge to <strong>child</strong>renand parents. They are useful for creating a climatein which campaigns for changes in behaviour and inproducts will be supported. For preventi<strong>on</strong> purposes,educati<strong>on</strong>al programmes are often combined withprogrammes involving legislati<strong>on</strong> and standards andproduct modificati<strong>on</strong>s. Educati<strong>on</strong> and counselling <strong>on</strong>their own, though, whether at the individual level orwithin schools, appear to be ineffective in reducing theincidence of burns.“Thermal burns are a comm<strong>on</strong> cause of accidental death in <strong>child</strong>renworldwide. Despite various methods of preventi<strong>on</strong> and care, suchinjuries are <strong>on</strong> the rise. Only through a deeper understanding of theunderlying causes can we develop truly viable alternative soluti<strong>on</strong>s. Ifthe proposals outlined in this <str<strong>on</strong>g>report</str<strong>on</strong>g> are implemented correctly, theycan bring about the necessary changes.” Mehmet Haberal, President,Internati<strong>on</strong>al Society for Burn Injuries.WORLD REPORT ON CHILD INJURY PREVENTION 93
TABLE 4.4Key strategies to prevent burns am<strong>on</strong>g <strong>child</strong>renStrategyEffectivePromisingInsufficientevidenceIneffectiveHarmfulSetting (and enforcing) laws <strong>on</strong> smoke alarmsDeveloping a standard for <strong>child</strong>-resistant lightersSetting (and enforcing) laws <strong>on</strong> hot-water tap temperature and educating the publicTreating patients at dedicated burns centresSeparating cooking areas from living areasDeveloping standards and codes for fire-retardant garmentsBanning the manufacture and sale of fireworksPromoting the use of safe lamps and stovesProviding first-aid for scalds – “cool the burn”C<strong>on</strong>ducting home visitati<strong>on</strong> programmes for at-risk familiesInstalling residential sprinklersDistributing smoke alarms <strong>on</strong> their own (without accompanying laws)C<strong>on</strong>ducting community-based campaigns and interventi<strong>on</strong>sStoring flammable substances correctlyModifying the envir<strong>on</strong>ment, e.g. home alterati<strong>on</strong>sC<strong>on</strong>ducting school-based burns preventi<strong>on</strong> programmesUsing traditi<strong>on</strong>al remedies <strong>on</strong> burnsSource: references 120, 137, 138.References1. Facts about injuries: burns. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>and Internati<strong>on</strong>al Society for Burn Injuries, 2006(http://www.who.int/entity/violence_<strong>injury</strong>_preventi<strong>on</strong>/publicati<strong>on</strong>s/other_<strong>injury</strong>/en/burns_factsheet.pdf, accessed17 April 2008).2. Davies JW. Toxic chemicals versus lung tissue: an aspectof inhalati<strong>on</strong> <strong>injury</strong> revisited. Journal of Burn Care andRehabilitati<strong>on</strong>, 1986, 7:213–222.3. Saffle JR, Davis B, Williams P. Recent outcomes in thetreatment of burn <strong>injury</strong> in the United States: a <str<strong>on</strong>g>report</str<strong>on</strong>g> fromthe American Burn Associati<strong>on</strong> patient registry. Journalof Burn Care and Rehabilitati<strong>on</strong>, 1995, 16:219–232.4. Moritz AR, Henriques FC. Studies of thermal <strong>injury</strong> II:the relative importance of time and surface temperaturein the causati<strong>on</strong> of cutaneous burns. American Journal ofPathology, 1947, 23:695–720.5. Lund C, Browder N. The estimati<strong>on</strong> of areas of burns.Surgical Gynecology and Obstetrics, 1944, 79:352–358.6. MacLennan N, Heimbach D, Cullen FB. Anesthesia formajor thermal <strong>injury</strong>. Anesthesiology, 1998, 89:749–770.7. Walt<strong>on</strong> J, Mandara AR. Burns and smoke inhalati<strong>on</strong>.Anesthesia and Intensive Care Medicine, 2005, 6:317–321.8. WHO mortality database: tables. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g>Health Organizati<strong>on</strong> (http://www.who.int/healthinfo/morttables/en/index.html, accessed 21 April 2008).9. Barrow RE et al. Influence of demographics and inhalati<strong>on</strong><strong>injury</strong> <strong>on</strong> burn mortality in <strong>child</strong>ren. Burns, 2004, 30:72–77.10. Achebe UJ, Akpuaka FC. Chemical burns in Enugu. WestAfrican Journal of Medicine, 1989, 8:205–208.11. Chuang SS, Yang JY, Tsai FC. Electric water heaters: a newhazard for pediatric burns. Burns, 2003, 29:589–591.12. Nursal TZ et al. Burns in southern Turkey: electricalburns remain a major problem. Journal of Burn Care andRehabilitati<strong>on</strong>, 2003, 24:309–314.13. Nguyen DQ et al. Infants under 1 year of age have asignificant risk of burn <strong>injury</strong>. Burns, 2008 34: 873–877.14. Child and youth unintenti<strong>on</strong>al <strong>injury</strong>: 10 years in review,1994–2003. Tor<strong>on</strong>to, ON, Safe Kids Canada, 2007(http://www.sickkids.ca/SKCForPartners/custom/Nati<strong>on</strong>alReportUpdatedENG.pdf, accessed 18 April2008).15. Nati<strong>on</strong>al Ambulatory Care Reporting System. CanadianInstitute for Health Informati<strong>on</strong> (http://secure.cihi.ca/cihiweb/dispPage.jsp?cw_page=services_nacrs_e,accessed 9 April 2008).94 WORLD REPORT ON CHILD INJURY PREVENTION
16. Papp A et al. Paediatric ICU burns in Finland 1994–2004.Burns, 2008, 34:339–344.17. Sharma PN et al. Paediatric burns in Kuwait: incidence,causes and mortality. Burns, 2006, 32:104–111.18. Palmieri RL et al. Pediatric soup scald burn <strong>injury</strong>: etiologyand preventi<strong>on</strong>. Journal of Burn Care and Research, 2008,29:114–118.19. Ndiritu S, Ngumi ZW, Ngaim O. Burns: the epidemiologicalpattern, risk and safety awareness at Kenyatta Nati<strong>on</strong>alHospital, Nairobi. East African Medical Journal, 2006,83:455–460.20. Y<strong>on</strong>gqiang F et al. Epidemiology of hospitalized burnpatients in Shand<strong>on</strong>g Province, 2001–2005. Journal ofBurn Care and Research, 2007, 28:468–473.21. Hijar-Medina MC et al. Accidentes en el hogar en niñosmenores de 10 años: causas y c<strong>on</strong>secuencias [Homeaccidents in <strong>child</strong>ren less than 10 years of age: causes andc<strong>on</strong>sequences]. Salud Pública de México, 1992, 34:615–625.22. Gali BM, Madziga AG, Naaya HU. Epidemiology of<strong>child</strong>hood burns in Maiduguri, north-eastern Nigeria.Nigerian Journal of Medicine, 2004, 13:144–147.23. Rossi LA et al. Childhood burn injuries: circumstancesof occurrences and their preventi<strong>on</strong> in Ribeirão Preto,Brazil. Burns, 1998, 24:416–419.24. Vilasco B, B<strong>on</strong>durand A. Burns in Abidjan, Côte d’Ivoire.Burns, 1995, 21:291–296.25. Gupta M, Gupta OK, Goil P. Paediatric burns in Jaipur,India: an epidemiological study. Burns, 1992, 18:63–67.26. Lari AR et al. Epidemiology of <strong>child</strong>hood burns in Farsprovince, Iran. Journal of Burn Care and Rehabilitati<strong>on</strong>,2002, 23:39–45.27. Hyder AA et al. Review <strong>on</strong> <strong>child</strong>hood burn injuries inSub Saharan Africa: a forgotten public health challenge.African Safety Promoti<strong>on</strong>: A Journal of Injury and ViolencePreventi<strong>on</strong>, 2004, 2:43–49.28. Adamo C et al. Epidemiological data <strong>on</strong> burn injuriesin Angola: a retrospective study of 7230 patients. Burns,1995, 21:536–538.29. Mashreky SR et al. Epidemiology of <strong>child</strong>hood burn: yieldof largest community based <strong>injury</strong> survey in Bangladesh.Burns, 2008 34: 856–862.30. Bawa Bhalla S, Kale SR, Mohan D. Burn properties offabrics and garments worn in India. Accident Analysis andPreventi<strong>on</strong>, 2000, 32:407–420.31. Hemeda M, Maher A, Mabrouk A. Epidemiology of burnsadmitted to Ain Shams University Burns Unit, Cairo,Egypt. Burns, 2003, 29:353–358.32. Ghosh A, Bharat R. Domestic burns preventi<strong>on</strong> and firstaid awareness in and around Jamshedpur, India: strategiesand impact. Burns, 2000, 26:605–608.33. Gupta RK, Srivastava AK. Study of fatal burn cases inKanpur (India). Forensic Science Internati<strong>on</strong>al, 1988,37:81–89.34. McCullough JE, Henders<strong>on</strong> AK, Kaufman JD.Occupati<strong>on</strong>al burns in Washingt<strong>on</strong> State, 1989–1993.Journal of Occupati<strong>on</strong>al and Envir<strong>on</strong>mental Medicine,1998, 40:1083–1089.35. Baggs J, Curwick C, Silverstein B. Work-related burns inWashingt<strong>on</strong> State, 1994 to 1998. Journal of Occupati<strong>on</strong>aland Envir<strong>on</strong>mental Medicine, 2002, 44:692–699.36. Arshi S et al. Preventi<strong>on</strong> oriented epidemiologic study ofaccidental burns in rural areas of Ardabil, Iran. Burns,2006, 32:366–371.37. Mohammadi R et al. Unintenti<strong>on</strong>al home-related injuries inthe Islamic Republic of Iran: findings from the first year of anati<strong>on</strong>al programme. Public Health, 2005, 119:919–924.38. Forjuoh SN, Guyer B, Smith GS. Childhood burns inGhana: Epidemiological characteristics and home-basedtreatment. Burns, 1995, 21:24–28.39. Kalayi GD, Muhammad I. Clothing burns in Zaria. Burns,1994, 20:356–359.40. Argirova M, Hadzhiyski O. Treatment of palm burns in<strong>child</strong>ren. Annals of Burns and Fire Disasters, 2005, 18:190–193.41. Electrical injuries. The Merck Manuals Online MedicalLibrary, 2005 (http://www.merck.com/mmpe/sec21/ch316/ch316b.html?qt=electrical%20burns&alt=sh,accessed 17 April 2008).42. Gore DC et al. Assessment of adverse events in the demiseof pediatric burn patients. Journal of Trauma, 2007,63:814–818.43. Esselman PC. Burn rehabilitati<strong>on</strong>: an overview. Archivesof Physical and Medical Rehabilitati<strong>on</strong>, 2007, 88(Suppl.2):S3–S6.44. Smith JS, Smith KR, Rainey SL. The psychology of burncare. Journal of Trauma Nursing, 2006, 13:105–106.45. Spurr ED, Shakespeare PG. Incidence of hypertrophicscarring in burn-injured <strong>child</strong>ren. Burns, 1990, 16:179–181.46. Taylor SC. Epidemiology of skin diseases in people ofcolor. Cutis, 2003, 71:271–275.47. Clark A. Psychosocial aspects of facial disfigurement:problems, management and the role of a lay-ledorganizati<strong>on</strong>. Psychology, Health and Medicine, 1999,4:127–142.48. Mathangi Ramakrishnan K et al. Paediatric rehabilitati<strong>on</strong>in a developing country, India, in relati<strong>on</strong> to aetiology,c<strong>on</strong>sequences and outcome in a group of 459 burnt<strong>child</strong>ren. Pediatric Rehabilitati<strong>on</strong>¸ 2004, 7:145–149.49. Gilboa D. L<strong>on</strong>g-term psychosocial adjustment after burninjuries. Burns, 2001, 27:335–341.50. Rizz<strong>on</strong>e LP et al. Posttraumatic stress disorder in mothersof <strong>child</strong>ren and adolescents with burns. Journal of BurnCare and Rehabilitati<strong>on</strong>, 1994, 15:158–163.51. Kent L, King H, Cochrane R. Maternal and <strong>child</strong>psychological sequelae in pediatric burn injuries. Burns,2000, 26:317–322.WORLD REPORT ON CHILD INJURY PREVENTION 95
52. Doctor ME. Burn camps and community aspects ofburn care. Journal of Burn Care and Rehabilitati<strong>on</strong>, 1992,13:68–76.53. Mancuso MG et al. Impact <strong>on</strong> the family: psychosocialadjustment of siblings of <strong>child</strong>ren who survive seriousburns. Journal of Burn Care and Research, 2003, 24:2.54. Sirit<strong>on</strong>gtaworn P, Peunchompoo N. Ec<strong>on</strong>omic problem ofreferred trauma cases in Siriraj Hospital. Journal of theMedical Associati<strong>on</strong> of Thailand, 2006, 89:1621–1629.55. Griffiths HR et al. The cost of a hot drink scald. Burns,2006, 32:372–374.56. Forjuoh SN. The mechanisms, intensity of treatment, andoutcomes of hospitalized burns: issues for preventi<strong>on</strong>.Journal of Burn Care and Rehabilitati<strong>on</strong>, 1998, 19:456–460.57. Joseph KE et al. Parental correlates of unintenti<strong>on</strong>al burninjuries in infancy and <strong>child</strong>hood burns. Burns, 2002,28:455–463.58. Han RK, Ungar WJ, Macarthur C. Cost-effectivenessanalysis of a proposed public health legislative/educati<strong>on</strong>alstrategy to reduce tap water scald injuries in <strong>child</strong>ren.Injury Preventi<strong>on</strong>, 2007, 13:248–253.59. Burd A, Yuen C. A global study of hospitalized pediatricburn patients. Burns, 2005, 31:432–438.60. Runyan CW. Using the Hadd<strong>on</strong> matrix: introducing thethird dimensi<strong>on</strong>. Injury Preventi<strong>on</strong>, 1998, 4:302–307.61. Chung ECH et al. Burn injuries in China: a <strong>on</strong>e year surveyat the United Christian Hospital. H<strong>on</strong>g K<strong>on</strong>g Practice,1996, 18:631–636.62. Ying SY, Ho WS. Playing with fire: a significant cause ofburn <strong>injury</strong> in <strong>child</strong>ren. Burns, 2001, 27:39–41.63. Chan KYO et al. A review of burns patients admitted tothe burns unit of hospital universiti Kebangsaan Malaysia.Medical Journal of Malaysia, 2002, 57:418–425.64. Zhu ZX, Yang H, Meng FZ. The epidemiology of <strong>child</strong>hoodburns in Jiamusi, China. Burns, 1988, 14:394–396.65. Chen G et al. Incidence and pattern of burn injuriesam<strong>on</strong>g <strong>child</strong>ren with disabilities. Journal of Trauma, 2007,62:682–686.66. Spitz MC. Injuries and death as a c<strong>on</strong>sequence of seizuresin people with epilepsy. Epilepsia, 1998, 39:904–907.67. Dempsey MP, Orr DJ. Are paediatric burns more comm<strong>on</strong>in asylum seekers? An analysis of paediatric burnadmissi<strong>on</strong>s. Burns, 2006, 32:242–245.68. Carlss<strong>on</strong> A et al. Burn injuries in small <strong>child</strong>ren: apopulati<strong>on</strong>-based study in Sweden. Journal of ClinicalNursing, 2006, 15:129–134.69. Soori H, Naghavi M. Childhood deaths from unintenti<strong>on</strong>alinjuries in rural areas of Iran. Injury Preventi<strong>on</strong>, 1998,4:222–224.70. Kane JM, Nazarian EB, C<strong>on</strong>nolly H. Hydrocarb<strong>on</strong>inhalati<strong>on</strong> <strong>injury</strong>. eMedicine, 2006 (http://www.emedicine.com/PED/topic2790.htm, accessed 10 April 2008).71. Warda L, Tenenbein M, Moffat MEK. House fire preventi<strong>on</strong>update (Part 1): a review of risk factors for fatal and n<strong>on</strong>fatalhouse fires. Injury Preventi<strong>on</strong>, 1999, 5:145–150.72. Hippisley-Cox J et al. Cross secti<strong>on</strong>al survey of socioec<strong>on</strong>omicvariati<strong>on</strong>s in severity and mechanism of<strong>child</strong>hood injuries in Trent 1992–7. British MedicalJournal, 2002, 324:1132–1134.73. Reimers A, Laflamme L. Neighbourhood socio-ec<strong>on</strong>omiccompositi<strong>on</strong> and <strong>injury</strong> risks. Acta Paediatrica, 2005,94:1488–1494.74. Poulos R et al. Area socioec<strong>on</strong>omic status and <strong>child</strong>hood<strong>injury</strong> morbidity in New South Wales, Australia. InjuryPreventi<strong>on</strong>, 2007, 13:322–327.75. Delgado J et al. Risk factors for burns in <strong>child</strong>ren: crowding,poverty, and poor maternal educati<strong>on</strong>. Injury Preventi<strong>on</strong>,2002, 8:38–41.76. Daisy S et al. Socioec<strong>on</strong>omic and cultural influence in thecausati<strong>on</strong> of burns in the urban <strong>child</strong>ren of Bangladesh.Journal of Burn Care and Rehabilitati<strong>on</strong>, 2001, 22:269–273.77. Forjuoh SN et al. Risk factors for <strong>child</strong>hood burns: acase-c<strong>on</strong>trol study of Ghanaian <strong>child</strong>ren. Journal ofEpidemiology and Community Health, 1995, 49:189–193.78. Werneck GL, Reichenheim ME. Paediatric burns andassociated risk factors in Rio de Janeiro, Brazil. Burns,1997, 23:478–83.79. Katcher ML. Tap water scald preventi<strong>on</strong>: it’s time for aworldwide effort. Injury Preventi<strong>on</strong>, 1998, 4:167–168.80. Munro S-A, van Niekerk A, Seedat M. Childhoodunintenti<strong>on</strong>al injuries: the perceived impact of theenvir<strong>on</strong>ment, lack of supervisi<strong>on</strong> and <strong>child</strong> characteristics.Child: Care, Health and Development, 2006, 32:269–279.81. Vassilia K, Eleni P, Dimitrios T. Firework-related<strong>child</strong>hood injuries in Greece: a nati<strong>on</strong>al problem. Burns,2004, 30:151–153.82. Mohan D, Varghese M. Fireworks cast a shadow <strong>on</strong> India’sfestival of lights. <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Forum, 1990, 11:323–326.83. Abdulwadud O, Ozanne-Smith J. Injuries associated withfireworks in Victoria: an epidemiological review. InjuryPreventi<strong>on</strong>, 1998, 4:272–275.84. Witsaman RJ, Comstock RD, Smith GA. Pediatricfireworks-related injuries in the United States, 1990–2003.Pediatrics, 2006, 118:296–303.85. Roesler JS, Day H. Sparklers, smoke bombs, and snakes,oh my! Effect of legislati<strong>on</strong> <strong>on</strong> fireworks-related injuries inMinnesota, 1999–2005. Minnesota Medical Journal, 2007,90:46–47.86. Van Niekerk A et al. Caregiver experiences,c<strong>on</strong>textualisati<strong>on</strong>s and understandings of the burn <strong>injury</strong>to their <strong>child</strong>: accounts from low-income settings inSouth Africa. Child: Care, Health and Development, 2007,33:236–245.87. Seedat M et al. The applicati<strong>on</strong> of still photography inmarshalling data for community-based initiatives. AfricanJournal of Psychology, 2006, 2:303–314.96 WORLD REPORT ON CHILD INJURY PREVENTION
88. Kellet P, Tipple AG. The home as workplace: a study ofincome-generating activities within the domestic setting.Envir<strong>on</strong>ment and Urbanizati<strong>on</strong>, 2000, 12:203–213.89. Godwin Y, Huds<strong>on</strong> DA, Bloch CE. Shack fires: ac<strong>on</strong>sequence of urban migrati<strong>on</strong>. Burns, 1996, 23:151–153.90. Zwi KJ et al. Patterns of <strong>injury</strong> in <strong>child</strong>ren and adolescentspresenting to a South African township health centre.Injury Preventi<strong>on</strong>, 1995, 1:26–30.91. Van Rijn OJ et al. Aetiology of burn injuries am<strong>on</strong>g<strong>child</strong>ren aged 0–4 years: results of a case-c<strong>on</strong>trol study.Burns, 1991, 17:213–219.92. Forjuoh SN. Burns in low- and middle-income countries: areview of available literature <strong>on</strong> descriptive epidemiology,risk factors, treatment, and preventi<strong>on</strong>. Burns, 2006,32:529–537.93. Petridou E et al. Risk factors for <strong>child</strong>hood burn injuries:a case-c<strong>on</strong>trol study from Greece. Burns, 1998, 24:123–128.94. Davies JWL. The problem of burns in India. Burns, 1990,16(Suppl. 1):S1–S24.95. Cheng JCY et al. An analysis of 1704 burn injuries in H<strong>on</strong>gK<strong>on</strong>g <strong>child</strong>ren. Burns, 1990, 16:182–184.96. Van Niekerk A, Rode H, Laflamme L. Incidence andpatterns of <strong>child</strong>hood burn injuries in the Western Cape,South Africa. Burns, 2004, 30:341–347.97. El-Badawy A, Mabrouk AR. Epidemiology of <strong>child</strong> burnsin the burn unit of Ain Shams University in Cairo, Egypt.Burns, 1998, 24:728–732.98. LeBlank JC et al. Home safety measures and the risk ofunintenti<strong>on</strong>al <strong>injury</strong> am<strong>on</strong>g young <strong>child</strong>ren: a multicentrecase-c<strong>on</strong>trol study. Canadian Medical Associati<strong>on</strong> Journal,2006, 175:883–887.99. Koupil J et al. Special features of burn injuries in elderlypatients. Acta Chirurgiae Plasticae, 2001, 43:57–60.100. Bruce N et al. Preventi<strong>on</strong> of burns am<strong>on</strong>g <strong>child</strong>ren in woodfuel using homes in rural Guatemala (Poster presentati<strong>on</strong>).16th Annual C<strong>on</strong>ference of the Internati<strong>on</strong>al Societyfor Envir<strong>on</strong>mental Epidemiology, New York, NY, 1–4August 2004 (http://ehs.sph.berkeley.edu/heh/guat/pubs/Burns%20poster%20ISEE%202004%20v230704.pdf,accessed 17 April 2008).101. Madubansi M, Schacklet<strong>on</strong> CM. Changes in fuelwooduse and selecti<strong>on</strong> following electrificati<strong>on</strong> in theBushbuckridge lowveld, South Africa. Journal ofEnvir<strong>on</strong>mental Management, 2007, 83:416–426.102. Runyan CW et al. Risk factors for fatal residential fires.New England Journal of Medicine, 1992, 327:859–863.103. DiGuiseppi C, Higgins JPR. Systematic review of c<strong>on</strong>trolledtrials of interventi<strong>on</strong>s to promote smoke alarms. Archivesof Diseases in Children, 2000, 82:341–348.104. Ballesteros MF, Jacks<strong>on</strong> ML, Martin MW. Workingtowards the eliminati<strong>on</strong> of residential fire deaths: TheCenter for Disease C<strong>on</strong>trol and Preventi<strong>on</strong>’s smoke alarminstallati<strong>on</strong> and fire safety (SAIFE) program. Journal ofBurn Care and Rehabilitati<strong>on</strong>, 2005, 26:434–439.105. Working to prevent and c<strong>on</strong>trol <strong>injury</strong> in the UnitedStates: fact book for the year 2000. Atlanta, GA, Centersfor Disease C<strong>on</strong>trol and Preventi<strong>on</strong>, Nati<strong>on</strong>al Center forInjury Preventi<strong>on</strong> and C<strong>on</strong>trol, 2000.106. Home fire protecti<strong>on</strong>: residential fire sprinkler systems.Emmitsburg, MD, Federal Emergency ManagementAgency, United States Fire Administrati<strong>on</strong>, 2004 (https://www.usfa.dhs.gov/downloads/pdf/publicati<strong>on</strong>s/fa-43.pdf, accessed 1 June 2008).107. Fires and burns fact sheet. Brisbane, Kidsafe Australia(http://www.gtp.com.au/kidsafeqld/inewsfiles/inews.25847.1.pdf, accessed 16 June 2008).108. Children’s sleepwear regulati<strong>on</strong>s. Washingt<strong>on</strong>, DC, UnitedStates C<strong>on</strong>sumer Product Safety Commissi<strong>on</strong>, 2001.109. Ly<strong>on</strong>s R et al. Modificati<strong>on</strong> of the home envir<strong>on</strong>ment forthe reducti<strong>on</strong> of injuries. Cochrane Database SystematicReviews, 2003, 4:CD003600:1–33.110. MacArthur C. Evaluati<strong>on</strong> of Safe Kids Week 2001:preventi<strong>on</strong> of scald and burn injuries in young <strong>child</strong>ren.Injury Preventi<strong>on</strong>, 2003, 9:112–116.111. Feldman KW et al. Tap water scald burns in <strong>child</strong>ren.Injury Preventi<strong>on</strong>, 1997, 4:238–242.112. Rivara CF. Hot water scald burns in <strong>child</strong>ren. Pediatrics,1998, 102:256–258.113. Ytterstad B, Sogaard AJ. The Harstad <strong>injury</strong> preventi<strong>on</strong>study: preventi<strong>on</strong> of burns in small <strong>child</strong>ren by acommunity-based interventi<strong>on</strong>. Burns, 1995, 21:259–266.114. Waller AE, Clarke JA, Langley JD. An evaluati<strong>on</strong> of aprogram to reduce home hot tap water temperatures.Australian Journal of Public Health, 1993, 17:116–123.115. Smith L, Smith C, Ray D. Lighters and matches: anassessment of risk associated with household ownership anduse. Washingt<strong>on</strong>, DC, United States C<strong>on</strong>sumer ProductSafety Commissi<strong>on</strong>, 1991.116. Smith LE, Greene MA, Singh HA. Study of the effectivenessof the US safety standard for <strong>child</strong>-resistant cigarettelighters. Injury Preventi<strong>on</strong>¸ 2002, 8:192–196.117. EU requires cigarette lighters to be <strong>child</strong>-resistant. EUROPAPress Releases, 14 March 2007 (http://europa.eu/rapid/pressReleasesActi<strong>on</strong>.do?reference=IP/07/325, accessed 1June 2008).118. Edwin AF, Cubis<strong>on</strong> TC, Pape SA. The impact of recentlegislati<strong>on</strong> <strong>on</strong> paediatric fireworks injuries in the Newcastleup<strong>on</strong> Tyne regi<strong>on</strong>. Burns, 2008, May 26 [epub ahead ofprint].119. Kendrick D et al. “Risk Watch”: cluster randomizedc<strong>on</strong>trolled trial evaluating an <strong>injury</strong> preventi<strong>on</strong> program.Injury Preventi<strong>on</strong>, 2007, 13:93–99.120. Warda LJ, Ballesteros MF. Interventi<strong>on</strong>s to preventresidential fire <strong>injury</strong>. In: Doll L et al., eds. Handbook of<strong>injury</strong> and violence preventi<strong>on</strong>. Atlanta, GA, Springer,2007:97–115.WORLD REPORT ON CHILD INJURY PREVENTION 97
121. Gielen AC et al. A randomized trial of enhancedanticipatory guidance for <strong>injury</strong> preventi<strong>on</strong>. Archives ofPediatric and Adolescent Medicine, 2001, 155:42–49.122. Gielen AC et al. The effects of improved access to safetycounseling, products and home visits <strong>on</strong> parents’ safetypractices. Archives of Pediatric and Adolescent Medicine,2002, 156:33–40.123. Gosselin RA, Kuppers G. Open versus closed managementof burn wounds in a low-income developing country.Burns, 2008 (in press).124. Hernd<strong>on</strong> DN. Total burn care (2nd ed.). Philadelphia, PA,Harcourt, 2002.125. Thomas J, Rode H. A practical guide to paediatric burns.Cape Town, SAMA Health and Medical Publishing Group,2006.126. Albertyn R, Bickler S, Rode H. Paediatric burn in injuriesin Sub Sahara Africa: an overview. Burns, 2006, 32:605–612.127. Davies JWL. Prompt cooling of burned areas: a review ofbenefits and the effector mechanisms. Burns, 1982, 9:1–6.128. Nguyen NL et al. The importance of immediate cooling:a case series of <strong>child</strong>hood burns in Vietnam. Burns, 2002,28:173–176.129. Sheridan RL et al. Current expectati<strong>on</strong>s for survival inpediatric burns. Archives of Pediatric and AdolescentMedicine, 2000, 154:245–249.130. Resources of optimal care of the injured patient. Chicago,IL, American College of Surge<strong>on</strong>s, Committee <strong>on</strong> Trauma,1999.131. Cooper DJ et al. Quality assessment of the management ofroad traffic fatalities at a level I trauma center comparedwith other hospitals in Victoria, Australia. Journal ofTrauma, 1998, 45:772–799.132. Sheridan RL et al. Early burn center transfer shortens thelength of hospitalizati<strong>on</strong> and reduces complicati<strong>on</strong>s in<strong>child</strong>ren with serious burn injuries. Journal of Burn Careand Rehabilitati<strong>on</strong>, 1999, 20:347–50.133. Organizati<strong>on</strong> and delivery of burn care. Practice Guidelinesof the American Burn Associati<strong>on</strong>, 2001 (http://www.ameriburn.org/PracticeGuidelines2001.pdf, accessed15 April 2008).134. Forjuoh SN, Li G. A review of successful transport andhome <strong>injury</strong> interventi<strong>on</strong>s to guide developing countries.Social Science and Medicine, 1996, 43:1551–1560.135. Yuan J et al. Assessment of cooling <strong>on</strong> an acute scald burn<strong>injury</strong> in a porcine model. Journal of Burn Care Research,2007, 28:514–520.136. McLoughlin E, MacGuire A. The causes, cost andpreventi<strong>on</strong> of <strong>child</strong>hood burn injuries. American Journalof Diseases of Children, 1990, 166:677–683.137. Nort<strong>on</strong> R et al. Unintenti<strong>on</strong>al injuries. In: Jamis<strong>on</strong> DT etal., eds. Disease c<strong>on</strong>trol priorities in developing countries(2nd ed.). New York, NY, Oxford University Press and<str<strong>on</strong>g>World</str<strong>on</strong>g> Bank, 2006:737–753 (http://www.dcp2.org/pubs/DCP/39/, accessed 14 February 2008).138. Turner C et al. Community-based interventi<strong>on</strong>s for thepreventi<strong>on</strong> of burns and scalds in <strong>child</strong>ren. CochraneDatabase Systematic Reviews, 2004, 3:CD004335.139. Kenrick D, Mulvaney C, Wats<strong>on</strong> M. Does targeting <strong>injury</strong>preventi<strong>on</strong> towards families in disadvantaged areas reduceinequalities in safety practice? Health Educati<strong>on</strong> Research,2008 (http://her.oxfordjournals.org/cgi/c<strong>on</strong>tent/full/cym083, accessed 14 August 2008).98 WORLD REPORT ON CHILD INJURY PREVENTION
WORLD REPORT ON CHILD INJURY PREVENTION 99
© C. KhasnabisSohel, a boy of 14 years,was the main breadwinnerin his family of four. He livedin the village of Krishnapur,in Narsingdi district inBangladesh. At the age of 7years, Sohel lost his father,Fazlur, who had slipped inthe bathroom and suffereda severe head <strong>injury</strong>.FALLSSOHEL’S STORYThe father left behind a small plot of land and a poor dwelling. The mother, Jharna,a 38-year-old widow, did household work for neighbours to earn a minute income.As a result of their circumstances, Sohel dropped out of school when he was in theseventh grade, and began to cultivate their small piece of land. He grew rice andother crops, which mostly went for their own c<strong>on</strong>sumpti<strong>on</strong>. Sohel and his friendsused to go to the river to fi sh, to earn a bit of extra m<strong>on</strong>ey for their daily living.It was the rainy seas<strong>on</strong>, in July 2004. One afterno<strong>on</strong> Sohel went out to the river tofi sh with his two friends. After failing for two hours to catch anything, they returneddesp<strong>on</strong>dently to the village. There was an old mosque there, <strong>on</strong> which the villagershad started some renovati<strong>on</strong> work. Keen to see what had been d<strong>on</strong>e and inquisitiveby nature, Sohel climbed <strong>on</strong>to the roof of the mosque. No c<strong>on</strong>structi<strong>on</strong> workers orany<strong>on</strong>e else were around at the time. Sohel’s friends wouldn’t follow him and pleadedwith him not to climb. Sohel ignored them and walked around the roof, movingtowards the edge.The roof, littered with c<strong>on</strong>structi<strong>on</strong> materials, was very wet. Suddenly Sohel stumbledover some materials, lost c<strong>on</strong>trol and fell from the roof. His head, which was badlyinjured, bled profusely, his right hand was broken and he lost c<strong>on</strong>sciousness. Somenearby people, alerted by the cries of his friends, took him to the nearest healthcentre, 15 kilometres from the village. So severe were his injuries that the paramediccould not help him. Within half an hour, he was dead.Sohel’s tragic case is not unique in Bangladesh. The Bangladesh Health and InjurySurvey showed that each year more than a thousand <strong>child</strong>ren under 18 years of agedie in the country as a result of unintenti<strong>on</strong>al falls. Each year fi ve thousand <strong>child</strong>renare injured from rooftop falls al<strong>on</strong>e. Over 5% of these become permanently disabledwhile the others suffer from varying degrees of illness. More than half the <strong>child</strong>hoodinjuries are am<strong>on</strong>g 10–14-year-olds, with more boys than girls suffering (1).To stop more <strong>child</strong>ren like Sohel needlessly dying from what are preventable injuries,acti<strong>on</strong> must be taken now.
CHAPTER 5 – FALLSChapter 5FallsIntroducti<strong>on</strong>Falling is a normal part of the way a <strong>child</strong> develops– learning to walk, climb, run, jump and explore thephysical envir<strong>on</strong>ment. Fortunately, most falls are of littlec<strong>on</strong>sequence and most <strong>child</strong>ren fall many times in theirlives without incurring damage, other than a few cutsand bruises. All the same, some falls are bey<strong>on</strong>d both theresilience of the human body and the capacity of the c<strong>on</strong>tactsurface to absorb the energy transferred. Falls are thus animportant cause of <strong>child</strong>hood injuries, including thoseresulting in permanent disability or death. Falls of thisdegree of seriousness are not randomly distributed, eitherglobally or within single countries. To understand whythis should be <strong>on</strong>e needs to examine the built envir<strong>on</strong>mentand the social c<strong>on</strong>diti<strong>on</strong>s in which <strong>child</strong>ren live.This chapter focuses <strong>on</strong> the main ideas underlying thepreventi<strong>on</strong> of unintenti<strong>on</strong>al falls in <strong>child</strong>hood, using apublic health approach. The extent and characteristics ofthe problem are first identified and after that the types ofexposure that are linked to a risk of <strong>injury</strong>. Interventi<strong>on</strong>strategies to prevent such injuries and their disablingc<strong>on</strong>sequences are examined for their effectiveness andcost-effectiveness. Finally, c<strong>on</strong>siderati<strong>on</strong> is given as tohow the most promising strategies can be successfullyimplemented <strong>on</strong> a wider scale.Falls have been defined and recorded in several ways. Thischapter adopts the <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>’s definiti<strong>on</strong>,according to which falls are “an event which results in apers<strong>on</strong> coming to rest inadvertently <strong>on</strong> the ground or flooror other lower level” (2). In the WHO database of injuries,fall-related deaths and n<strong>on</strong>-fatal injuries exclude those dueto assault and intenti<strong>on</strong>al self-harm. Injuries and deathsresulting from falls from animals, burning buildings andvehicles, as well as falls into water and machinery, are als<strong>on</strong>ot coded as falls. Instead, they are recorded, respectively,as injuries due to animals, fire, transport, submersi<strong>on</strong> andmachinery.An expert group c<strong>on</strong>vened by the Nati<strong>on</strong>al Instituteof Child Health and Human Development defined fallsas an external cause or type of exposure, the impact ofwhich is “to come down by force of gravity suddenly; totumble, topple, and forcibly lose balance” (3). The grouplisted the main factors relating to falls in <strong>child</strong>hood. Theseincluded:– social and demographic factors, such as the <strong>child</strong>’s age,gender, ethnicity and socioec<strong>on</strong>omic status;– the physical development of the <strong>child</strong>;– activity taking place before the fall – such as running,walking or climbing;– the locati<strong>on</strong> of the fall;– the height from which the fall occurs;– characteristics of the surfaces with which c<strong>on</strong>tact is made– such as texture, smoothness and deformability.All this informati<strong>on</strong>, if available, taken together withinformati<strong>on</strong> <strong>on</strong> risk factors, can provide valuable clues asto how and why fall-related injuries occur, and greatly helpefforts to prevent them.Epidemiology of fallsAccording to the WHO Global Burden of Disease projectfor 2004, an estimated 424 000 people of all ages diedfrom falls worldwide. Although the majority of fallrelateddeaths were am<strong>on</strong>g adults, they ranked as thetwelfth leading cause of death am<strong>on</strong>g 5 to 9-year-olds and15 to 19-year-olds (see Table 1.1 in Chapter 1). Morbidityfrom falls is much more comm<strong>on</strong> and represents asignificant burden <strong>on</strong> health-care facilities around theworld. Am<strong>on</strong>g <strong>child</strong>ren under 15 years, n<strong>on</strong>-fatal fallswere the 13th leading cause of disability-adjusted lifeyears (DALYs) lost. In most countries, falls are the mostcomm<strong>on</strong> type of <strong>child</strong>hood <strong>injury</strong> seen in emergencydepartments, accounting for between 25% and 52% ofassessments (4, 5).The published literature <strong>on</strong> the incidence and patternsof fall-related injuries am<strong>on</strong>g <strong>child</strong>ren relates largely tohigh-income countries, where just 10% of the world’s<strong>child</strong>ren live. In many of these countries, deaths from alltypes of <strong>injury</strong> are estimated to have dropped by over 50%over the past three decades (6, 7).A systematic review of the literature from mainlylow-income and middle-income countries in Africa,Asia and Central and South America <strong>on</strong> the incidenceof unintenti<strong>on</strong>al <strong>child</strong>hood falls resulting in death orneeding medical care, found the following.In Africa, the median incidence of falls am<strong>on</strong>g <strong>child</strong>renand youth aged less than 22 years was 41 per 100 000populati<strong>on</strong> (8).In Central and South America, the rate varied from1378 to 2700 per 100 000 populati<strong>on</strong> aged less than20 years (9, 10).In Asia, the median incidence was 170 per 100 000populati<strong>on</strong> aged less than 18 years (43% of allinjuries).The highest rate <strong>on</strong> the Asian c<strong>on</strong>tinent was recordedin the United Arab Emirates with an incidence of some1923 per 100 000 populati<strong>on</strong> (11–14).WORLD REPORT ON CHILD INJURY PREVENTION 101
The UNICEF–TASC surveys have also found falls tobe a leading cause of morbidity and disability in <strong>child</strong>ren,resulting in high social and ec<strong>on</strong>omic costs (15).The studies reviewed suggest a substantial variabilityin the incidence of falls between regi<strong>on</strong>s – and sometimeswithin regi<strong>on</strong>s. In the absence of a comm<strong>on</strong> methodologyand standard definiti<strong>on</strong>, however, data from differentstudies and settings cannot be compared directly andare potentially misleading. Less than a fifth of the studiesdocumented deaths due to falls, <strong>on</strong>ly 12% used standardizedor formal definiti<strong>on</strong>s for falls, and n<strong>on</strong>e provided reliabledata <strong>on</strong> the severity of injuries or c<strong>on</strong>sequent disabilityresulting.MortalityIn 2004, nearly 47 000 <strong>child</strong>ren and youth under the ageof 20 years died as a result of a fall. Fall-related mortalitydata compiled by WHO reveal important differencesbetween regi<strong>on</strong>s, and between countries within regi<strong>on</strong>s(see Figure 5.1). High-income countries in the Americas,Europe and Western Pacific regi<strong>on</strong>s had average mortalityrates of between 0.2 and 1.0 per 100 000 <strong>child</strong>ren aged lessthan 20 years. However, low-income and middle-incomecountries in the same regi<strong>on</strong>s <str<strong>on</strong>g>report</str<strong>on</strong>g>ed rates up to threetimes higher. Low-income and middle-income countriesin South-East Asia and the Eastern Mediterranean regi<strong>on</strong>shad the highest average rates – of 2.7 per 100 000 and 2.9per 100 000, respectively. While it is quite possible that thelevels are so much higher in some places, it is also possiblethat some misclassificati<strong>on</strong> of data has occurred. Childabuse, for instance, is sometimes wr<strong>on</strong>gly classified in thecategory of falls (16, 17).AgeIn high-income countries, the average fall mortality rates,by age, are similar over the first 20 years of life. However,in low-income and middle-income countries, infants lessthan <strong>on</strong>e year of age have very high rates (see Figure 5.2).FIGURE 5.2Fatal fall-related <strong>injury</strong> rates per 100 000 <strong>child</strong>ren by age andcountry income level, <str<strong>on</strong>g>World</str<strong>on</strong>g>, 2004Rate per 100 000 populati<strong>on</strong>6420HIC = High-income countries; LMIC = low-income and middle-income countries.Source: WHO (2008), Global Burden of Disease: 2004 update.HICLMICUnder 1 1–4 5–9 10–14 15–19 under 20Age (years)FIGURE 5.1Fatal fall-related <strong>injury</strong> rates per 100 000 <strong>child</strong>ren a by WHO regi<strong>on</strong> and country income level, 20042+0.5–1.9
Community surveys c<strong>on</strong>ducted in Asia highlight thehigh incidence of fall deaths in the regi<strong>on</strong>. In Bangladesh,the overall fall mortality rate for the 0–17-year age groupwas 2.8 per 100 000 (1), and falls were the sec<strong>on</strong>d leadingcause of death through <strong>injury</strong> am<strong>on</strong>g infants aged less than<strong>on</strong>e year (24.7 per 100 000 populati<strong>on</strong>). In Viet Nam, fallswere the sixth leading cause of <strong>child</strong>hood death (4.7 per100 000 aged 0–17 years) (18). In Jiangxi province in China,falls were the fourth leading cause of death (3.1 per 100 000aged 0–17 years). Higher rates were <str<strong>on</strong>g>report</str<strong>on</strong>g>ed in rural areasthan in urban areas (19).Falls are still an important cause of death in <strong>child</strong>ren inhigh-income countries, even though the incidence rates arec<strong>on</strong>siderably less than in low-income and middle-incomecountries. Falls are the fourth leading cause of traumadeaths in <strong>child</strong>hood in the United States (20) and the sixthleading external cause of death am<strong>on</strong>g Australian <strong>child</strong>renaged 0–14 years (21).GenderBoys are overrepresented in fall mortality statistics (seeTable 5.1), with the male-to-female ratio varying from1.2:1 (in low-income and middle-income countries inSouth-East Asia) to 12:1 (in high-income countries in theEastern Mediterranean regi<strong>on</strong>).Type of fallBased <strong>on</strong> data from the Global Burden of Disease project,which includes the fourth ICD coding digit from 70 mainlymiddle-income and high-income Member States, 66% offatal falls am<strong>on</strong>g <strong>child</strong>ren occurred from a height, while8% resulted from falls <strong>on</strong> the same level. Unfortunately,the relevant informati<strong>on</strong> was unavailable for a quarter ofthe <str<strong>on</strong>g>report</str<strong>on</strong>g>ed falls (22).MorbidityExtent of the problemGlobal statistics <strong>on</strong> n<strong>on</strong>-fatal <strong>injury</strong> are not readilyavailable, though the incidence of n<strong>on</strong>-fatal falls isclearly much higher than that of fatal cases. Data that areavailable indicate that falls are a leading, if not in fact themost comm<strong>on</strong>, type of <strong>injury</strong> resulting in hospitalizati<strong>on</strong>or emergency room attendance in most high-incomecountries (20, 23–28). Falls were also cited as the leadingcause of <strong>injury</strong> am<strong>on</strong>g 13–15-year-olds in the GlobalSchool Health Survey, covering 26 countries (see StatisticalAnnex, Table A.3).Most published studies of n<strong>on</strong>-fatal <strong>injury</strong> in low-incomeand middle-income countries are hospital-based and mayfail to capture data <strong>on</strong> <strong>child</strong>ren who are unable to accessmedical care (29, 30). Community-based studies suggestthat there are many more significant fall-related injuriesthan just those seen at health-care facilities (14, 31).The Asian community surveys recorded <strong>injury</strong> eventsthat were serious enough to warrant seeking medicalattenti<strong>on</strong> or that resulted in school days missed. Injuriesnot meeting these criteria were deemed insignificant interms of health-care costs and social costs (29, 31). In the<strong>injury</strong> survey in Jiangxi province, China (19), for every<strong>on</strong>e death due to a fall, there were 4 cases of permanentdisability, 13 cases requiring hospitalizati<strong>on</strong> for 10 ormore days, 24 cases requiring hospitalizati<strong>on</strong> for between1 and 9 days, and 690 cases where care was sought orwhere at least 1 day of work or school was missed (seeFigure 5.3). The survey highlighted the substantial costof n<strong>on</strong>-fatal injuries due to falls and the small proporti<strong>on</strong>of cases seen in hospital settings – cases which, takentogether, must c<strong>on</strong>tribute c<strong>on</strong>siderably to the overall costof falls.FIGURE 5.3Inury pyramid for falls am<strong>on</strong>g <strong>child</strong>ren 0–17 years, Jiangxiprovince, ChinaSource: Reference 19.Death(1)Permanent disability(4)Hospitalizati<strong>on</strong> (10+ days)(13)Hospitalizati<strong>on</strong> (1–9 days)(24)Missed work or school or sought treatment(690)TABLE 5.1Fatal fall <strong>injury</strong> rates per 100 000 <strong>child</strong>ren a by sex, country income level and WHO regi<strong>on</strong>, 2004Africa Americas South-East Asia Europe Eastern Mediterranean Western PacificLMIC HIC LMIC LMIC HIC LMIC HIC LMIC HIC LMICBoys 1.8 0.3 1.0 3.0 0.5 1.3 4.0 3.5 0.5 2.5Girls 1.1 0.1 0.4 2.4 0.2 0.6 0.3 2.3 0.3 1.9aThese data refer to those under 20 years of age.HIC = High-income countries; LMIC = low- and middle-income countries.Source: WHO (2008), Global Burden of Disease: 2004 update.WORLD REPORT ON CHILD INJURY PREVENTION 103
Similar patterns of <strong>injury</strong> were observed in Uganda,where there were higher rates of falls am<strong>on</strong>g <strong>child</strong>ren inrural than in urban areas (32). Data from various countriesin Latin America and from Pakistan also reveal that fallsare a comm<strong>on</strong> cause of n<strong>on</strong>-fatal <strong>injury</strong> am<strong>on</strong>g <strong>child</strong>ren(9, 33–36).Globally, 50% of the total number of DALYs lost due tofalls occur in <strong>child</strong>ren less than 15 years of age. However,the burden of <strong>child</strong>hood falls is largely explained by themorbidity and disabilities that may persist for life. Theskewed distributi<strong>on</strong> of this burden geographically andthe relative scarcity of statistics <strong>on</strong> n<strong>on</strong>-fatal <strong>injury</strong> eventsmake it more difficult to describe and address the problemof <strong>child</strong>hood falls.Severity of fallsThe severity of a fall-related <strong>injury</strong> is determined by theanatomy of the human body and the impact force towhich the body is subjected – in the absence of any specialprotecti<strong>on</strong> <strong>on</strong> the body or impact-absorbing materialsin the landing or c<strong>on</strong>tact surfaces (37–41). The impactforce itself depends, am<strong>on</strong>g other things, <strong>on</strong> the heightfrom which the fall occurs. These relati<strong>on</strong>ships are welldescribed in high-income countries in relati<strong>on</strong> to fallsfrom playground equipment (42–46) and from windowsand roofs (47–49).The proporti<strong>on</strong>s of injuries due to falls, as well as thepat terns of injur y f rom fa l ls genera l ly, ca n di ffer c<strong>on</strong>siderablyin developing countries from those in developed countries(50). For instance, a recent study c<strong>on</strong>ducted in four lowincomeand middle-income countries found that falls werethe leading cause of unintenti<strong>on</strong>al <strong>injury</strong> am<strong>on</strong>g <strong>child</strong>renunder the age of 12 years. The types of injuries sustainedwere largely cuts and scrapes, fractures of the upper andlower extremities and c<strong>on</strong>tusi<strong>on</strong>s. In half of all cases, the<strong>child</strong>ren were left with some form of disability – in 41% ofcases with a temporary disability of less than six weeks (seeStatistical Annex, Table C.1).Generally, the greater the height from which a <strong>child</strong>falls, the more severe the <strong>injury</strong> (51). The Jiangxi surveyfound that about 18% of falls were from heights of fivemetres or more and two thirds involved heights of between<strong>on</strong>e and five metres (19). The Jiangxi and Beijing surveys(19, 52) revealed that as <strong>child</strong>ren grew older, an increasingproporti<strong>on</strong> of falls were from greater heights – such astrees and rooftops, frequently, in the case of adolescents.A Nigerian study, <strong>on</strong> the other hand, found that <strong>on</strong>ly 25%of falls in <strong>child</strong>hood leading to hospitalizati<strong>on</strong> were fromheights, the remainder occurring at ground level (53).Injuries from falls from heights of more than two storeystypically involve falls from windows, balc<strong>on</strong>ies and roofs(41, 51). Falls from stairs and trees are also comm<strong>on</strong>, asare falls into ditches, wells, shafts and other holes in theground (19). Trees are particularly hazardous, especiallyin some tropical countries where <strong>child</strong>ren are employedto harvest high tree crops (50) (see Box 5.1).BOX 5.1Falls from trees in MozambiqueIn 2006, an <strong>injury</strong> and violence survey was c<strong>on</strong>ducted in Mozambique.The study covered 179 households from the urban district ofMatola and 162 from the rural district of Boane, both areas in thesouthernmost part of the country.Falls were the leading cause (31.7%) of <strong>injury</strong> in Boane district,while they accounted for 23.8% of injuries in Matola district, surpassed<strong>on</strong>ly by road traffic injuries, accounting for 34.7% of all injuries.Twenty-eight per cent of all the falls involved <strong>child</strong>ren and adolescentsunder the age of 20 years. Many of the falls were from trees, acomm<strong>on</strong> occurrence in developing countries.In <strong>on</strong>e of the most rural parts of Boane district, a widowed motherwith seven <strong>child</strong>ren is in tears as she tells the story of her eldests<strong>on</strong>, José. José broke his leg after falling from a coc<strong>on</strong>ut tree whilecollecting fruit for the family’s breakfast. Now aged 17 years, he ispermanently disabled. One of his legs had to be amputated becausehe did not receive immediate care. His mother recalls that neighbourstried to help so<strong>on</strong> after the fall, but that it took many hours toget him to the nearest health-care facility. On arrival there it wasapparent that the fracture was compound and the facility lacked thenecessary equipment to handle his case. He was c<strong>on</strong>sequently referredto Maputo Central Hospital, a further three hours’ drive away. Itwas 17 hours before José was seen by an orthopaedic surge<strong>on</strong>. José’smother has now lost her primary breadwinner. She reflects <strong>on</strong> theirexperience, saying “these are the realities of the day-to-day life wehave to deal with in Mozambique.”José’s case is not an isolated <strong>on</strong>e. Data from the emergency departmentsurveillance system in Maputo Central Hospital show thatfalls account for 40% of those presenting to the emergency department,with <strong>child</strong>ren under 18 years of age making up almost twothirds of these cases. Seventy-five per cent of the serious fall injuriesam<strong>on</strong>g <strong>child</strong>ren are the result of their falling from trees, usuallyaround the home.© WHO104 WORLD REPORT ON CHILD INJURY PREVENTION
In the United States, many of the fall fatalities am<strong>on</strong>g<strong>child</strong>ren involve falls from poor-quality housing in lowincomeurban areas, typically from the sec<strong>on</strong>d flooror higher (51). Falls from greater heights tend to occurmore in the summer m<strong>on</strong>ths. This is presumably becausewindows – the usual site for falls of pre-school-age <strong>child</strong>ren– are more likely to be open at that time of year, and older<strong>child</strong>ren are more likely to be outdoors playing <strong>on</strong> fireescapes, roofs and balc<strong>on</strong>ies (47–49).A case–c<strong>on</strong>trol study from New Zealand has shownthat the risk of <strong>injury</strong> in a fall from playground equipmentincreases dramatically for heights of over 1.5 metres (54).After adjusting for various factors such as the <strong>child</strong>’s ageand weight and the presence of impact absorbing surfaces,<strong>child</strong>ren falling from over 1.5 metres were found to havefour times the risk of <strong>injury</strong> compared to those falling frombelow that height. The risk of <strong>injury</strong> rose with increasingfall height, with <strong>child</strong>ren who fell from over 2.25 metreshaving 13 times the risk of <strong>injury</strong> compared to those whofell from 0.75 metres or below.The extent to which falls from low heights result in lifethreateninginjuries, especially head injuries, has generatedc<strong>on</strong>siderable c<strong>on</strong>troversy, largely in relati<strong>on</strong> to suspected<strong>child</strong> abuse (55–57). What evidence there is <strong>on</strong> this doestend to point in the directi<strong>on</strong> of possible abuse. Reportedfatalities following short or minor falls are more comm<strong>on</strong>in situati<strong>on</strong>s where there are no unrelated witnesses whocan c<strong>on</strong>firm the history of events (55–57). When makingclinical decisi<strong>on</strong>s, therefore, the height of a fall should notbe the <strong>on</strong>ly criteri<strong>on</strong> used to determine the threat to lifethat a particular <strong>injury</strong> poses (58).C<strong>on</strong>sequences of fallsFalls are the leading cause of traumatic brain <strong>injury</strong>,especially in young <strong>child</strong>ren, with a significant risk of l<strong>on</strong>gtermc<strong>on</strong>sequences (20, 59–61). In the United States, about<strong>on</strong>e third of the 1.4 milli<strong>on</strong> people suffering traumaticbrain injuries are <strong>child</strong>ren aged 0 to 14 years, who havedisproporti<strong>on</strong>ately high rates of falls compared with otherage groups (62).A Canadian study noted that 36% of infants aged lessthan <strong>on</strong>e year presenting to an emergency departmentfollowing a fall had significant head injuries, and thatfalls were resp<strong>on</strong>sible for 90% of all head injuries seen inthe emergency department (20). Falls are also the mostcomm<strong>on</strong> cause of fatal and serious head injuries am<strong>on</strong>g<strong>child</strong>ren in France and the United Kingdom (63–65).While the incidence of spinal-cord injuries following afall is generally low, most spinal-cord injuries, resulting inquadriplegia or paraplegia, are attributed to falls (66–68).A case study from Nigeria describes the lifel<strong>on</strong>g disabilityresulting from such injuries, often the result of falls fromtall palm trees (69).Children tend to use their arms to protect their headswhen falling from a height. Limb fractures, particularlyof the forearm, are therefore the most comm<strong>on</strong> type offall-related <strong>injury</strong> in <strong>child</strong>ren bey<strong>on</strong>d the age of infancy(37, 70–73). An analysis in Australia of <strong>child</strong>ren fallingfrom playground equipment showed that fracturesaccounted for 85% of playground injuries (74). Therehave been suggesti<strong>on</strong>s that the incidence of upper limbfractures has increased in recent years, while that ofserious head injuries has declined. This claim needs tobe investigated further in relati<strong>on</strong> to safety standards inplaygrounds (75, 76).Even after incurring open or complex fractures, <strong>child</strong>renin low-income countries can make a good recovery ifthey receive proper care (77). All the same, permanentdisfigurement and functi<strong>on</strong>al impairment from suchfractures are frequently seen in poorer settings (5, 9, 78,79). Growth-plate fractures are particularly liable to resultin permanent disability (79). Abdominal and chest injuriesare uncomm<strong>on</strong> in falls from <strong>on</strong>e or two storeys, but morefrequent in falls from greater heights (47, 72, 80).The UNICEF–TASC survey in Jiangxi province, China,found that falls were the leading cause of permanentdisability in young people aged 0–17 years, primarily dueto the l<strong>on</strong>g-term c<strong>on</strong>sequences of brain and cervical spine<strong>injury</strong>. Such disability was estimated to be 3.5 times morefrequent in boys than in girls (19). A study in Nicaraguaalso found that falls were the leading cause of permanentdisability in young people less than 15 years of age (33).In Thailand (81) and Viet Nam (18), falls accounted for1% and 4% of the total burden of permanent disability,respectively. Permanent disability in these surveysreferred to the loss of a physical sense – such as sight orhearing – loss of mobility or loss of the ability to speak.However, emoti<strong>on</strong>al, psychological and cognitive l<strong>on</strong>gtermc<strong>on</strong>sequences were not included because of thedifficulty in measuring them (19). As a result, the overallamount of permanent disability is likely to be c<strong>on</strong>siderablygreater than the survey estimates suggest.Cost of fall-related <strong>injury</strong>In Canada, annual injuries from <strong>child</strong>hood falls wereestimated in 1995 to cost 630 milli<strong>on</strong> Canadian dollars (82).Implementing strategies known to be effective is expectedto result in a 20% reducti<strong>on</strong> in the incidence of falls am<strong>on</strong>g<strong>child</strong>ren aged 0–9 years, 1500 fewer hospitalizati<strong>on</strong>s,13 000 fewer n<strong>on</strong>-hospitalized injuries, 54 fewer injuriesleading to permanent disability and net savings of overC$ 126 milli<strong>on</strong> (US$ 120 milli<strong>on</strong>) every year (82).In the United States, falls account for the largest shareof the cost of deaths and injuries in <strong>child</strong>ren under 15 yearsof age – more than a quarter of all <strong>child</strong>hood unintenti<strong>on</strong>al<strong>injury</strong>-related costs, and costing almost US$ 95 billi<strong>on</strong> in2004 (83). For <strong>child</strong>ren aged 0–19 years, hospital data from36 states suggest that the total expenditure for a case ofacute care following a fall was sec<strong>on</strong>d <strong>on</strong>ly to that of roadtraffic <strong>injury</strong> (84).WORLD REPORT ON CHILD INJURY PREVENTION 105
In Australia, the annual direct health-care cost of fallsin <strong>child</strong>ren is estimated to be over 130 milli<strong>on</strong> Australiandollars, of which 28 milli<strong>on</strong> dollars is attributable tohospital inpatient care (21).While sufficient data are not available from low-incomeand middle-income countries to obtain an estimate of thecost of fall-related injuries, it is clear that cost is substantial.In Lil<strong>on</strong>gwe, Malawi, almost 10% of paediatric admissi<strong>on</strong>swere related to unintenti<strong>on</strong>al injuries, a third of whichwere as a result of fractures, generally from falls (85). Anemergency department study in Turkey noted that fallsaccounted for 41% of <strong>injury</strong> admissi<strong>on</strong>s and c<strong>on</strong>tributedto a major part of the overall budget for paediatric traumacases (86). The high risk of wounds becoming c<strong>on</strong>taminatedand of complicati<strong>on</strong>s such as b<strong>on</strong>e and joint infecti<strong>on</strong>s,together with the scarcity of powerful antibiotics andmicrosurgical techniques, create significant problems forhealth-care services (77, 85, 87, 88). The length of paediatrichospital admissi<strong>on</strong>s involving osteomyelitis in a Gambianhospital, for instance, was found to be sec<strong>on</strong>d <strong>on</strong>ly to thatof admissi<strong>on</strong>s as a result of burns (88).Limitati<strong>on</strong>s of dataRates of fatalities resulting from falls are relatively low.Much of the estimated global burden of falls am<strong>on</strong>g<strong>child</strong>ren stems from subsequent disability. The lack ofreliable data, in much of the world, <strong>on</strong> n<strong>on</strong>-fatal outcomesis therefore a significant deficiency.The mechanisms and patterns of fall-related <strong>injury</strong>am<strong>on</strong>g <strong>child</strong>ren are highly dependent <strong>on</strong> the c<strong>on</strong>text.Again, this informati<strong>on</strong> is generally not available for mostlow-income and middle-income countries – countries inwhich the burden of falls is the heaviest. In high-incomecountries, studies gathering data specifically related tothe c<strong>on</strong>text and circumstances surrounding falls – anddeparting from the standard Internati<strong>on</strong>al Classificati<strong>on</strong>of Disease codes – have provided valuable informati<strong>on</strong> tohelp develop preventi<strong>on</strong> measures.Risk factorsAs already menti<strong>on</strong>ed, the incidence and patterns offall injuries am<strong>on</strong>g <strong>child</strong>ren depend to a great extent <strong>on</strong>c<strong>on</strong>textual factors. A systematic review of the publishedliterature <strong>on</strong> risk factors for unintenti<strong>on</strong>al injuries dueto falls in <strong>child</strong>ren identified age, sex and poverty asc<strong>on</strong>sistent independent risk factors (4). Other major riskfactors influencing the incidence and severity of fallinjuries were: the height of the fall; the type of surface;the mechanism (whether dropped, falling down stairs orfalling using a baby walker); and the setting (whether daycare or home care).Drawing <strong>on</strong> these studies and other epidemiologicalfindings, Table 5.2 shows the major factors influencingthe incidence of unintenti<strong>on</strong>al <strong>child</strong>hood falls and theirc<strong>on</strong>sequences.Child-related factorsAge and developmentChildren’s developmental stages – as well as the activitiesand envir<strong>on</strong>ments associated with these stages – have abearing <strong>on</strong> the incidence and characteristics of fall-relatedinjuries (89, 90). Research into the ways that infants andsmall <strong>child</strong>ren learn to climb stairs (91) has found complexinteracti<strong>on</strong>s between:– their evolving motor and cognitive skills;– the physical opportunities presented to them, such asaccess to stairs;– their social opportunities or lack of them, such as strictsupervisi<strong>on</strong> by caregivers.TABLE 5.2Hadd<strong>on</strong> Matrix applied to the risk factors for <strong>child</strong>hood fallsPhasesPre-eventEventPost-eventFactorsChild Agent Physical envir<strong>on</strong>ment Socioec<strong>on</strong>omic envir<strong>on</strong>mentAge; gender; level of activity;pre-existing disability.Size and physical developmentof <strong>child</strong>.Child’s general health; disability;post-<strong>injury</strong> complicati<strong>on</strong>s.Unsafe productor equipment;unprotectedrooftop, balc<strong>on</strong>yor staircase; tree.Lack of protectiveequipment or barriersthat reducethe severity of an<strong>injury</strong> in the eventof a fall.Sharp objects andothers hazardsthat increaserisk of cuts andinfecti<strong>on</strong>s.Lack of access to safe playspaces and opportunities;lack of preventive measuressuch as stair gates and guardrails.Height of fall; type of surface<strong>on</strong>to which <strong>child</strong> falls; lackof impact-absorbingsurfaces.Lack of adequate prehospitalcare, acute care orrehabilitati<strong>on</strong>.Poverty; single-parent family; family size;maternal educati<strong>on</strong>; awareness of fall risksam<strong>on</strong>g caregivers, <strong>child</strong>care providers andeducators.Lack of awareness of potentially serious injuriesassociated with falls, e.g. c<strong>on</strong>cussi<strong>on</strong>and brain <strong>injury</strong>.Lack of first-aid skills; lack of access tohealth care; lack of resources to managepost-<strong>injury</strong> outcomes.106 WORLD REPORT ON CHILD INJURY PREVENTION
Most of the falls young <strong>child</strong>ren have might bec<strong>on</strong>sidered a normal part of their development andlearning experience. However, their curiosity to exploretheir surroundings is generally not matched by theircapacity to gauge or resp<strong>on</strong>d to danger (5, 92). As theybecome older and increasingly independent, they haveaccess to a wider range of territory and are capable of agreater range of physical activity. They also often strive toperform more challenging and daring acts – a behaviourknown as “risk-taking”.In most high-income countries, <strong>child</strong>ren under <strong>on</strong>eyear of age are most likely to fall from furniture or carseats, or through being dropped. Between the ages of <strong>on</strong>eand three years, <strong>child</strong>ren are most likely to fall from stairsor steps, baby walkers, furniture or play equipment. Older<strong>child</strong>ren typically fall from playground equipment or frombeing pushed (89, 93–95).Evidence from low-income countries is less specific.However, a populati<strong>on</strong>-based study from Brazil, Chile,Cuba and Venezuela noted that falls involving young<strong>child</strong>ren occurred most comm<strong>on</strong>ly at home, though witholder <strong>child</strong>ren, instituti<strong>on</strong>s, such as schools, and publicplaces were the prime locati<strong>on</strong>s (9, 96). A study fromthree paediatric hospitals in Mexico found that falls fromstairways and beds accounted for a high proporti<strong>on</strong> ofadmissi<strong>on</strong>s of <strong>child</strong>ren under 10 years of age. The factorscreating particular <strong>injury</strong> risks for these <strong>child</strong>ren were (34,97): a lack of protective rails <strong>on</strong> beds (30%); unprotectedstaircases (48%); and easy access to roofs (40%). Falls fromunprotected rooftops – <strong>on</strong> which <strong>child</strong>ren play as well assleep – are comm<strong>on</strong> in countries such as Bangladesh, Indiaand Turkey (98, 99).GenderMales outnumber females for fall-related injuries – andindeed most types of <strong>injury</strong> – am<strong>on</strong>g <strong>child</strong>ren and youngpeople (6, 100). This is the case in most countries, and appliesto both fatal and n<strong>on</strong>-fatal falls (4, 37, 53, 101, 102).The nature of <strong>child</strong>hood falls and injuries can be partlyexplained by patterns of <strong>child</strong>-rearing, socializati<strong>on</strong> androle expectati<strong>on</strong>s. Risk-taking behaviour is also biologicallydetermined. Irrespective of culture boys engage in roughplay more frequently than do girls. Gender differences inthe extent to which <strong>child</strong>ren are exposed to hazards are alsocomm<strong>on</strong> in most societies (29). Some researchers attributepr<strong>on</strong>eness to <strong>injury</strong> in <strong>child</strong>ren to pers<strong>on</strong>ality traits suchas impulsiveness, hyperactivity, aggressi<strong>on</strong> and otherbehaviours more comm<strong>on</strong>ly ascribed to boys than girls (12,103). While many psychological characteristics are indeedassociated with increased risks of <strong>injury</strong>, a review of theliterature suggests that the c<strong>on</strong>tributi<strong>on</strong> of pers<strong>on</strong>ality traitsto <strong>child</strong>hood injuries is relatively small compared with thatof envir<strong>on</strong>mental and social factors (104).Differences in the way boys and girls are socializedby their parents were highlighted in a study examiningthe reacti<strong>on</strong>s of mothers to their <strong>child</strong>’s behaviour <strong>on</strong> theplayground. The study showed that mothers resp<strong>on</strong>dedless often and were slower to intervene in instances of riskybehaviour <strong>on</strong> the part of a s<strong>on</strong> than they did in the case ofa daughter (105). Parental practices have also been foundto foster greater exploratory behaviours am<strong>on</strong>g boys thanam<strong>on</strong>g girls and to impose fewer restricti<strong>on</strong>s <strong>on</strong> boys than<strong>on</strong> girls.PovertyA recent systematic review of risk factors for fall-relatedinjuries am<strong>on</strong>g <strong>child</strong>ren found a str<strong>on</strong>g relati<strong>on</strong>shipbetween social class and the incidence of <strong>child</strong>hood falls(4). The complex associati<strong>on</strong>s between social deprivati<strong>on</strong>and increased risks of <strong>child</strong>hood <strong>injury</strong> have severalunderlying factors (5, 106–111), including:– overcrowded housing c<strong>on</strong>diti<strong>on</strong>s;– hazardous envir<strong>on</strong>ments;– single-parenthood;– unemployment;– a relatively young maternal age;– a relatively low level of maternal educati<strong>on</strong>;– stress and mental health problems <strong>on</strong> the part ofcaregivers;– lack of access to health care.In some cases, poor-quality housing may be made morehazardous for falls as a result of its locati<strong>on</strong>. Examples ofthis are dwellings built <strong>on</strong> sloping sites in mountainousareas (112) and slum settlements c<strong>on</strong>structed <strong>on</strong> rockyterrain (113, 114).Underlying c<strong>on</strong>diti<strong>on</strong>sDespite the relative lack of data, there is evidence that<strong>child</strong>ren who are minimally mobile, but who are perceivedby a caregiver as immobile <strong>on</strong> account of their disability,are at increased risk for falling from a bed or otherelevated surface (92). The presence of mental disabilitycan increase the risk of unintenti<strong>on</strong>al <strong>injury</strong>, includingfalls, by a factor of up to eight (115–117). An emergencydepartmentstudy from Greece c<strong>on</strong>cluded that falls andc<strong>on</strong>cussi<strong>on</strong> were more comm<strong>on</strong> am<strong>on</strong>g <strong>child</strong>ren withpsychomotor or sensory disability than in <strong>child</strong>ren whowere not disabled (118). Children in wheelchairs areparticularly at risk, regardless of their cognitive ability,with falls estimated to account for 42% of the number ofinjuries am<strong>on</strong>g wheelchair users (92).Agent factorsC<strong>on</strong>sumer productsIn surveys of product safety in high-income countries,falls – generally involving infants in the first year of life –are am<strong>on</strong>g the most comm<strong>on</strong> n<strong>on</strong>-fatal injuries. Such fallsare associated with pushchairs (known as strollers in NorthAmerica), prams, baby walkers, high chairs, changingtables,cots (excluding portable cots) and baby exercisersWORLD REPORT ON CHILD INJURY PREVENTION 107
(119, 120). A study from the state of Victoria, Australia,suggests that baby bouncers (also called baby exercisers)are involved in the most severe n<strong>on</strong>-fatal injuries relatedto products, with almost <strong>on</strong>e in three injuries resultingin hospital admissi<strong>on</strong>. After baby bouncers, high chairsand pushchairs are the products linked to the most severeinjuries from falls (120, 121).A review of fall-related risk factors in the 0–6-year agegroup found that am<strong>on</strong>g <strong>child</strong>ren using bunk beds, therisk of a fall <strong>injury</strong> is greater for younger <strong>child</strong>ren, <strong>child</strong>renfrom poorer families, <strong>child</strong>ren in newer beds, and <strong>child</strong>renwho fall <strong>on</strong>to n<strong>on</strong>-carpeted floors (4, 122). Other <str<strong>on</strong>g>report</str<strong>on</strong>g>ssuggest that while bunk beds and c<strong>on</strong>venti<strong>on</strong>al beds maycause almost the same number of fall injuries am<strong>on</strong>g5–9-year-olds, injuries from bunk bed falls are more severethan those from c<strong>on</strong>venti<strong>on</strong>al bed falls as the fall is from agreater height (120).Many products for leisure activities – such asskateboards, in-line skates, Heelys (a popular brand ofshoes that c<strong>on</strong>vert from sports to roller shoes), ice-skates,swing ropes and trampolines – can result in fall-relatedinjuries, particularly limb fractures, sprains and headinjuries (123–129) (see Box 5.2). The European Uni<strong>on</strong>’s<strong>injury</strong> database has identified <strong>child</strong>ren’s bicycles, rollerskates and swings as the three leading c<strong>on</strong>sumer productsimplicated in home and leisure activity injuries, most ofwhich are from falls (130).Despite the virtual absence of data <strong>on</strong> the issue, productsafety is c<strong>on</strong>sidered to be a significant problem for <strong>child</strong>renin developing countries. In additi<strong>on</strong> to product-relatedrisks in occupati<strong>on</strong>al settings, globalizati<strong>on</strong> has led tothe widespread use in developing countries of potentiallydangerous products that are not always accompanied by thesafety features or regulati<strong>on</strong>s generally found in developedcountries. Heelys are <strong>on</strong>e such case of increasing c<strong>on</strong>cern,as falls involving their use can result in significant headand limb fractures (124, 131, 132).Playground equipmentFalls from playground equipment can lead to severeinjuries and are comm<strong>on</strong>ly seen in hospital admissi<strong>on</strong>statistics in high-income countries (120, 133–135). A studyfrom Victoria, Australia, found that falls from playgroundequipment accounted for 83% of emergency departmentadmissi<strong>on</strong>s. Of these cases, 39% were related to falls fromclimbing equipment, 18% from slides and 14% from swings(120).Several studies have discovered significant associati<strong>on</strong>sbetween certain structural features of playgrounds and fallinjuries (45, 54, 136–139). A New Zealand study has shownthat lowering the height of equipment to 1.5 metres couldreduce the risk of <strong>child</strong>ren having to attend emergencydepartments following playground falls by 45% (42).Studies from Canada (45) and Greece (138) have foundhigh risks of <strong>injury</strong>, particularly from falls, in playgroundslacking the proper safety standards – such as havingBOX 5.2Protective equipment to preventwrist fracturesFalls are a comm<strong>on</strong> form of sport and recreati<strong>on</strong>al <strong>injury</strong> in <strong>child</strong>renand adolescents. Activities that are associated with “outreach” falls –where the pers<strong>on</strong> falls forward and lands <strong>on</strong> an outstretched arm –have a significant likelihood of resulting in upper limb injuries. Such activitiesinclude snow and ice sports (such as skiing and ice skating) andsports involving wheels (such as roller skating and skateboarding).Fractures of the ulna and radius, particularly of the distal radius,as well as severe upper limb injuries, are comm<strong>on</strong> outcomes of outreachfall injuries. The usual sequence of events leading to thesewrist injuries is a loss of balance followed by a forward fall, with thepers<strong>on</strong> landing <strong>on</strong> an outstretched arm. The risk of <strong>injury</strong> is furtherincreased by factors such as:– high speed;– hard or irregular surfaces;– other physical hazards;– risky manoeuvres, such as aerial jumps in skateboarding.There is c<strong>on</strong>siderable evidence that the majority of distal radialfractures associated with sporting activities, particularly those insnow and those involving wheels, could be prevented by the use ofwrist guards (140). In fact, <strong>child</strong>ren and young people who do notwear wrist guards are up to ten times more likely to sustain severewrist injuries than those who wear them. This is the case, irrespectiveof the pers<strong>on</strong>’s level of skill in the sport (141). Despite this, fewparticipants wear them, with wearing rates estimated at less than60% for in-line skaters and less than 30% for snowboarders.Wrist guards are erg<strong>on</strong>omically designed devices that protect thepalm of the hand and support the wrist without compromising rangeof moti<strong>on</strong>. They reduce wrist fractures by absorbing impact energyand by sharing the load, so that the b<strong>on</strong>es in the wrist and forearmtake less of the strain of the fall (142). Fears that wrist guards mayexacerbate <strong>injury</strong> risk, or lead to more fractures further up the arm,are largely unfounded. Currently, there is no internati<strong>on</strong>al standardfor wrist guards and there are suggesti<strong>on</strong>s that not all models providefull protecti<strong>on</strong>. N<strong>on</strong>etheless, the overwhelming weight ofevidence is in favour of their effectiveness.The problem, as with other forms of protective equipment, ishow to encourage young people to wear wrist guards. A range of approachesis needed, combining educati<strong>on</strong>al measures with laws andtheir enforcement at the sites where <strong>child</strong>ren and young people arelikely to participate in these activities. These measures should be accompaniedby the use of prominent role models seen wearing wristguards, and advice as to their effectiveness at places where they aresold or rented out.appropriate and sufficiently thick surface materials, andadequate handrails or guardrails.AnimalsStudies from several developing countries point to theincreasing number of cases in recent years of <strong>child</strong>ren andyoung people presenting to hospital as a result of fallingfrom a horse. This may be due to the growing popularityof horse riding as a recreati<strong>on</strong>al sport, as well as to largernumbers of <strong>child</strong>ren working <strong>on</strong> farms (143–145). While108 WORLD REPORT ON CHILD INJURY PREVENTION
most injuries from falls from horses are minor <strong>on</strong>es, a studyfrom the Netherlands estimated that up to 40% of <strong>child</strong>renand adolescents treated in hospital after falling from ahorse still suffered a disability four years later (146).Animal racing also poses significant risks of <strong>child</strong>hoodfalls (147–150). Camel racing is a popular spectator sport,whose origins lie in the desert culture of West Asia andNorth Africa (150). Traditi<strong>on</strong>ally, race camels were riddenby young <strong>child</strong>ren from the family of the camel owner.In recent decades, though, migrant <strong>child</strong>ren as young asthree or four years of age have performed as camel jockeys,sometimes trafficked for that purpose (150, 151). Falls arethe comm<strong>on</strong>est type of <strong>injury</strong> in camel racing, frequentlyresulting in head injuries, including fractures of the skull(148, 149).Envir<strong>on</strong>mental factorsPhysical envir<strong>on</strong>mentThe “built envir<strong>on</strong>ment” is a vital resource for the healthydevelopment of <strong>child</strong>ren. At the same time, it is oftenthe source for their fall-related injuries (152). Structuralhazards in the built envir<strong>on</strong>ment stem from the presenceof dangerous or inappropriate features, or from the absenceof protective features. Specifically, such factors include:– a lack of building maintenance, particularly in lowincomerented housing;– design features in buildings and products that do not takeaccount of the changing capabilities of young <strong>child</strong>ren –such as a lack of window guards in high-rise buildings;– poor lighting in buildings and in streets.Socioec<strong>on</strong>omic envir<strong>on</strong>mentInadequate adult supervisi<strong>on</strong> is often cited as a majorc<strong>on</strong>tributor to <strong>child</strong>hood injuries (153, 154). The issuesinvolved, however, are complex and cut across many of theproblems facing the most vulnerable families. As describedin Chapter 1, the relative developmental immaturity of<strong>child</strong>ren leads to their having limited ability to recognizedanger and foresee the c<strong>on</strong>sequences of their acti<strong>on</strong>s ifleft unattended. It is therefore often regarded as axiomaticthat caregivers should supervise <strong>child</strong>ren and know whattype of injuries the <strong>child</strong>ren risk at different ages, so asto prevent them from incurring fall injuries (98). Parents,social workers and medical pers<strong>on</strong>nel are generally furtheragreed that pre-school-age <strong>child</strong>ren, in particular, shouldbe supervised c<strong>on</strong>stantly to minimize the risk of <strong>injury</strong> –with any unsupervised period lasting no l<strong>on</strong>ger than fiveminutes (154).However, despite these generally agreed “facts”, an overreliance<strong>on</strong> supervisi<strong>on</strong> as the <strong>on</strong>ly or primary approachto prevent falls am<strong>on</strong>g <strong>child</strong>ren is ill-advised, for severalreas<strong>on</strong>s, including the following (155–161):Falls can occur even with adult supervisi<strong>on</strong>, as has beenshown in several studies in high-income countries <strong>on</strong>injuries from baby walkers.What a caregiver c<strong>on</strong>siders an adequate levelof supervisi<strong>on</strong> may not be c<strong>on</strong>sistent with theepidemiological evidence.Ec<strong>on</strong>omic c<strong>on</strong>diti<strong>on</strong>s, such as poverty, unemploymentand the disrupti<strong>on</strong> of social networks, may seriouslyaffect the quality of supervisi<strong>on</strong>. In poor families,<strong>child</strong>ren may not <strong>on</strong>ly be left unsupervised, but findthemselves acting as caregivers to younger siblings.C<strong>on</strong>diti<strong>on</strong>s in which caregivers are under stress andhave c<strong>on</strong>flicting demands placed <strong>on</strong> their attenti<strong>on</strong> areoften the most hazardous. Other factors that increase<strong>child</strong>ren’s susceptibility to falls in poor households mayinclude mental health problems affecting caregivers(5, 90, 160–164).Illustrating the last point, a large urban slum in Rocinha,Brazil, was the site of a study of <strong>child</strong>hood injuries (90).Falls accounted for 66% of the injuries, an unsurprisingfinding given the steeply sloping terrain <strong>on</strong> which thesettlement was c<strong>on</strong>structed, its rocky outcrops and opendrains, as well as the high levels of stress exhibited by the<strong>child</strong>ren’s mothers.Several studies in high-income countries havesuggested that day-care facilities may pose significantrisks of <strong>injury</strong> (165, 166). A systematic review, though,found two studies that compared fall injuries in daycare with those in home care. These studies showedthat the risk of a fall <strong>injury</strong> am<strong>on</strong>g infants and young<strong>child</strong>ren in the home was twice the comparable risk inday-care settings (167, 168). N<strong>on</strong>etheless, there exist greatdifferences in c<strong>on</strong>diti<strong>on</strong>s within day-care centres – asindeed there are within home care. A more sophisticatedanalysis is therefore called for, that goes bey<strong>on</strong>d simplecategorizati<strong>on</strong> of care arrangements into “home care”and “day care”.Work envir<strong>on</strong>mentChild labour places <strong>child</strong>ren of both sexes at a significantrisk of falls. This is partly because the demands placed<strong>on</strong> the <strong>child</strong>ren usually exceed their ability to cope, interms of developmental skills, strength, stamina and size(169). Agriculture is also the most comm<strong>on</strong> setting forn<strong>on</strong>-fatal serious falls resulting in disabling head andlimb injuries. Particular dangers for <strong>child</strong>ren workingin this sector include unprotected platforms; laddersand tall trees used for reaching high-growing crops; pits,wells and unlit shafts; and barns, silos and deep drainageditches (50, 170).Children and adolescents <strong>on</strong> farms are an importantgroup at risk in high-income countries. Data fromCanadian and United States registries found that fallsaccounted for 41% of injuries am<strong>on</strong>g <strong>child</strong>ren in thissetting. In additi<strong>on</strong>, 61% of falls from heights occurredam<strong>on</strong>g <strong>child</strong>ren who were not working but who lived <strong>on</strong>the farms (143, 171, 172).WORLD REPORT ON CHILD INJURY PREVENTION 109
Studies from various low-income countries suggestthat falls are a comm<strong>on</strong> cause of serious <strong>injury</strong> for<strong>child</strong>ren working in the c<strong>on</strong>structi<strong>on</strong> industry, withsignificant risks posed by open building sites (173–175).Lack of treatment and rehabilitati<strong>on</strong>Community-based surveys in low-income and middleincomecountries show that a significant proporti<strong>on</strong> of<strong>child</strong>ren, including those with moderate to severe fallrelatedinjuries, do not receive medical care. The reas<strong>on</strong>sfor this include: the distance to the hospital; prohibitivetransport costs; and a lack of awareness <strong>on</strong> the part ofthe caregiver of the need for early attenti<strong>on</strong> (9, 19, 33,66, 176).The Jiangxi Injury Survey <str<strong>on</strong>g>report</str<strong>on</strong>g>ed that many <strong>child</strong>rensustaining fall injuries were either al<strong>on</strong>e or with another<strong>child</strong> at the time of the <strong>injury</strong> – rather than with acaregiver. The survey also found that adult caregiverswere generally unaware of basic first-aid proceduresand did not know how to reach high-quality medicalcare (19). A Nigerian study noted that it was relatives orneighbours who managed most <strong>child</strong>hood injuries, andthat less than 1% of injuries were seen by a health-careprofessi<strong>on</strong>al (177).The risks of late recogniti<strong>on</strong> of intracranial haemorrhage,inadequate care of the airway, poor managementof transfer between facilities, and inadequate acutetrauma and rehabilitati<strong>on</strong> care can profoundly influencethe probabilities of survival and disability (34, 176, 178,179). Rates of pre-hospital deaths are greater in placeswith less developed emergency medical services andl<strong>on</strong>ger periods of transfer to hospital (178). A study fromthe Islamic Republic of Iran found that 40% of fatalitiesfollowing <strong>child</strong>hood falls occurred in pre-hospitalsettings, while 30% occurred in emergency departmentsand 30% in hospitals (66).Interventi<strong>on</strong>sThe preventi<strong>on</strong> of fall-related injuries am<strong>on</strong>g <strong>child</strong>renis of paramount importance worldwide, given the largeamount of resulting morbidity, the high costs of healthcare and the significant risk of death, particularly fromhead injuries. The measures employed must strike acareful balance between, <strong>on</strong> the <strong>on</strong>e hand, promotingthe healthy development of <strong>child</strong>ren – allowing them toplay, explore and be physically active – and, <strong>on</strong> the otherhand, recognizing the vulnerability of <strong>child</strong>ren living inenvir<strong>on</strong>ments designed primarily for adults.The Child safety good practice guide (180) is <strong>on</strong>e ofseveral nati<strong>on</strong>al or regi<strong>on</strong>al policy documents describingpractical approaches for preventing fall-related injuriesam<strong>on</strong>g <strong>child</strong>ren. The following secti<strong>on</strong> c<strong>on</strong>siders the mostpromising such interventi<strong>on</strong>s in a global c<strong>on</strong>text.Engineering measuresIdentifying, replacing or modifying unsafe products hasbeen a leading strategy to prevent injuries from falls inmany high-income countries. Major reducti<strong>on</strong>s in theincidence of <strong>child</strong>hood fall injuries have been achievedby removing or redesigning nursery furniture (seeBox 5.3), playground equipment, sports and recreati<strong>on</strong>alequipment, and other items such as shopping carts andwheelchairs (180, 181). In some instances, a completeban <strong>on</strong> a product has ensued. In other cases, there hasbeen substantial modificati<strong>on</strong> of the original design –such as the introducti<strong>on</strong> of a new braking mechanismfor baby walkers (182). To be effective, such measuresgenerally require c<strong>on</strong>tinuous enforcement (180, 182,183).In some cases, sufficient evidence has accumulatedfrom other situati<strong>on</strong>s for devices to be recommended toprotect against fall-related injuries. Thus, despite a lackof interventi<strong>on</strong> studies relating to horse riding, helmetsare now recommended to reduce the risk of serious headinjuries am<strong>on</strong>g young riders (144). All the same, studiesfrom Australia, Canada, New Zealand and the UnitedStates suggest that rates of wearing helmets remainrelatively low in these countries (184–186). Helmets andwrist guards are also str<strong>on</strong>gly recommended for <strong>child</strong>renengaging in ice skating, in-line skating and roller skating(126).Envir<strong>on</strong>mental measuresModifying the envir<strong>on</strong>ment to make it more “<strong>child</strong>friendly”is a passive interventi<strong>on</strong> approach that benefitspeople of all ages. Major changes in the design andmaintenance of playgrounds have substantially reducedthe number of playground injuries in many high-incomecountries (180). Such modificati<strong>on</strong>s included layingrubber or bark ground surfacing of sufficient depth, andmaking equipment, such as slides, safer in terms of heightand structure.A community-based programme in the United Stateshas dem<strong>on</strong>strated how modifying buildings can achievesubstantial reducti<strong>on</strong>s in fall-related injuries am<strong>on</strong>g<strong>child</strong>ren. The “Children Can’t Fly” programme (49)(see Box 5.4), combining individual counselling and amass media campaign with the free distributi<strong>on</strong> andinstallati<strong>on</strong> of window guards, has proved effective incutting the incidence of falls from high-rise buildingsin low-income areas. How this strategy might betransferred to other settings depends <strong>on</strong> the structureof dwellings, the resources available and other factors.However, the use of window guards in many parts ofAfrica and other developing regi<strong>on</strong>s (187) suggeststhat this approach might be useful, if implementedal<strong>on</strong>g with other measures, such as the enforcement ofbuilding regulati<strong>on</strong>s.110 WORLD REPORT ON CHILD INJURY PREVENTION
BOX 5.3Product safety and falls from nursery furnitureMany countries have found injuries associated with nursery furniture to be an important issue in <strong>child</strong>ren under the age of five years. In the first year ofa <strong>child</strong>’s life, these injuries may represent almost 20% of injuries treated in hospital (188). The introducti<strong>on</strong> of <strong>injury</strong> surveillance systems and detailedsystematic analyses of deaths in young <strong>child</strong>ren led, in the last two decades of the twentieth century, to a greater awareness in developed countries ofinjuries related to nursery furniture, including cots, baby walkers, high chairs, prams, pushchairs, baby bouncers and changing-tables (121).While the overwhelming majority of n<strong>on</strong>-fatal, hospital-treated injuries associated with nursery furniture are due to falls, the types of <strong>injury</strong>involving nursery furniture leading to deaths are more varied. Such injuries include suffocati<strong>on</strong> and strangulati<strong>on</strong>, as well as asphyxiati<strong>on</strong> followinga fall – for example, following the tipping over of a pram.In 2002, the Internati<strong>on</strong>al Standardizati<strong>on</strong> Organizati<strong>on</strong> published guidelines for protecting <strong>child</strong>ren against <strong>injury</strong> from products (includingbuildings and installati<strong>on</strong>s), processes and services (189). These guidelines were aimed at those involved in setting or revising standards, as well asat designers, architects, manufacturers, service providers, communicators and policy-makers.Several countries have established standards – usually voluntary butsometimes mandatory – for the most frequently-used nursery products.These product-specific standards are known as “vertical standards”. Mandatoryvertical standards have been introduced in developed countries <strong>on</strong>a country-by-country basis, where voluntary measures have failed. TheEuropean Uni<strong>on</strong> has a Product Safety Directive that clearly sets out who isresp<strong>on</strong>sible for product safety at each stage – from design through manufacture,to importati<strong>on</strong>, wholesale and retail of products.Standards can also be based <strong>on</strong> the hazards, rather than the products,and these are known as “horiz<strong>on</strong>tal standards”. Australia, for instance, is inthe process of introducing horiz<strong>on</strong>tal standards, following a review of theproduct safety system and the way in which standards were made.Developing countries need now to adopt the best practices in productsafety. Several developing countries already manufacture products forexport, and follow safety standards set in the high-income countries importingthe products. A horiz<strong>on</strong>tal approach to safety standards is oftenthe most effective way to ensure safety for a wide range of existing, newand redesigned products.© WHOLaws and regulati<strong>on</strong>sLaws can be powerful tools to reinforce the use of existingtechnology and influence behaviour. In New York City,following the passage of legislati<strong>on</strong> requiring landlords toinstall window guards, a large decrease was observed inthe number of fatal falls of young <strong>child</strong>ren from high-risebuildings (41). Since the introducti<strong>on</strong> of both mandatoryand voluntary standards for baby walkers in Canadaand the United States, the tipping over of these itemsand structural failures in them appear to have becomeuncomm<strong>on</strong> (51, 190).Often, the potential effectiveness of promisingregulatory approaches remains unclear. For example, theeffectiveness of regulatory and enforcement proceduresin day-care centres is still uncertain, largely because ofmethodological shortcomings in the evaluative studiesc<strong>on</strong>ducted to date (139).Even where the effectiveness of laws or regulati<strong>on</strong>sis clearly established, a lack of adequate enforcementmay mean that a measure is not widely implemented.Despite the recognized benefits, for instance, of adoptingstandards for playgrounds, less than 5% of playgroundssurveyed in an Australian study were found to complywith the recommended guidelines <strong>on</strong> the depth of surfacematerial (191).Educati<strong>on</strong>al approachesEducati<strong>on</strong>al and awareness-raising campaigns –particularly those c<strong>on</strong>ducted in isolati<strong>on</strong> – have beencriticized in several quarters (5, 105, 189). These criticismshave centred <strong>on</strong> the relative lack of evidence that thesecampaigns reduce injuries, the difficulty in changinghuman behaviour, and human weaknesses – such asinattenti<strong>on</strong> and the ability to be distracted – that underminethe potential effectiveness of “active” interventi<strong>on</strong>s. Criticshave also pointed to the disproporti<strong>on</strong>ate burden of <strong>injury</strong>am<strong>on</strong>g poorer social groups, and the limited effect ofhealth messages aimed at these groups.Nevertheless, educating the parents of young <strong>child</strong>renabout falls is often regarded as an affordable and feasibleinterventi<strong>on</strong> measure. An attracti<strong>on</strong> of this strategy isthe relative ease with which programmes can be updatedwith new informati<strong>on</strong> – such as new guidance <strong>on</strong> babywalkers (189, 192–194). An intensive community-wideprogramme in the United States to educate the generalpublic and health-care workers about the dangers ofWORLD REPORT ON CHILD INJURY PREVENTION 111
BOX 5.4Children Can’t Fly“Children Can’t Fly” was a programme developed by the New YorkCity Department of Health in the early 1970s, to counter the highrates of death and <strong>injury</strong> am<strong>on</strong>g <strong>child</strong>ren following falls from windows.The programme involved persuading the city’s health board toamend the laws, so that all landlords were required to provide windowguards in high-rise apartments in which young <strong>child</strong>ren lived.This was the first such law of its kind in the United States.The programme c<strong>on</strong>tained three comp<strong>on</strong>ents.A voluntary <str<strong>on</strong>g>report</str<strong>on</strong>g>ing system. All falls am<strong>on</strong>g <strong>child</strong>ren under15 years had to be <str<strong>on</strong>g>report</str<strong>on</strong>g>ed by hospital emergency rooms andthe police. Home visits were made by nurses in the public healthsystem to the household where the fall had occurred.Educati<strong>on</strong>. Parents were counselled <strong>on</strong> a <strong>on</strong>e-to-<strong>on</strong>e basis <strong>on</strong> howto prevent falls. A mass media campaign was c<strong>on</strong>ducted <strong>on</strong> radioand televisi<strong>on</strong> and in the press, informing people of the risks of<strong>child</strong>ren falling from windows. This was accompanied by a communityeducati<strong>on</strong> programme, involving the disseminati<strong>on</strong> ofprinted material.Equipment. Easily-installable window guards were provided freeof charge, where required, to families with young <strong>child</strong>ren livingin areas of high risk.As a result of the programme, a significant reducti<strong>on</strong> in the incidenceof falls was recorded, particularly in the city’s Br<strong>on</strong>x district, wherethe number of <str<strong>on</strong>g>report</str<strong>on</strong>g>ed falls declined by 50%. Many other cities aroundthe world have since followed New York City’s lead. In additi<strong>on</strong> to thelives saved, this interventi<strong>on</strong> has been shown to be cost-effective interms of savings in hospitalizati<strong>on</strong>s, rehabilitati<strong>on</strong> and the costs ofmaintaining injured or permanently disabled <strong>child</strong>ren.Source: reference 49.infant walkers resulted in a 28% decline in the numberof <strong>child</strong>ren presenting to emergency departments withinjuries from falling down stairs related to the use ofthese walkers (195).Educati<strong>on</strong>al campaigns, though, are generally regardedto be more beneficial when combined with other strategies,such as legislati<strong>on</strong> or envir<strong>on</strong>mental modificati<strong>on</strong>. Suchcombined approaches often make the interventi<strong>on</strong>s easierto transfer to other settings, or indeed to implement inthe original setting (196). A review in 2007 showedthat educati<strong>on</strong> <strong>on</strong> safety in the home (with or withoutthe provisi<strong>on</strong> of safety equipment) resulted in a 26%increase in the proporti<strong>on</strong> of households with fitted stairgates. However, there was a lack of evidence that theseinterventi<strong>on</strong>s actually reduced <strong>injury</strong> rates (197). A moretargeted study published in 2008 has now shown somemodest reducti<strong>on</strong>s in fall rates (198).In settings where the technology and resources exist,there is increasing interest in employing electr<strong>on</strong>iccommunicati<strong>on</strong> to deliver safety messages, in the hope thatsuch an approach will overcome the problems encounteredby traditi<strong>on</strong>al methods of communicati<strong>on</strong>. One examplewas an early-<strong>child</strong>hood safety educati<strong>on</strong> programmedelivered through a stall c<strong>on</strong>taining computers in a busyemergency department. This emergency departmentserved a poor community with high levels of illiteracy. Arandomized c<strong>on</strong>trol trial suggested that the programmewas successful in increasing knowledge and several typesof safety behaviour. Its impact, however, <strong>on</strong> reducing<strong>injury</strong> rates is not as yet clear (199). An interesting findingwas the observati<strong>on</strong> that the benefits from more resourceintensiverecommendati<strong>on</strong>s – such as to install <strong>child</strong> safetyseats – depended <strong>on</strong> family income. As dem<strong>on</strong>strated inboth developed and developing countries (200, 201), unlessfinancial barriers and the particular situati<strong>on</strong>s of poorpopulati<strong>on</strong>s are addressed, “effective” interventi<strong>on</strong>s mayincrease, rather than decrease, disparities in the burden of<strong>injury</strong>, with the most vulnerable <strong>child</strong>ren being the leastlikely to benefit.Combining strategiesMany interventi<strong>on</strong> strategies combine several of themeasures outlined above.© T. Toroyan WHOHome visitati<strong>on</strong> programmesSupportive home visitati<strong>on</strong> programmes during early<strong>child</strong>hood have been used for a wide range of purposes.These include improvement of the home envir<strong>on</strong>ment,family support and the preventi<strong>on</strong> of behavioural problemsin the <strong>child</strong>ren. A Cochrane review and other morerecent studies have shown that home visits – includingmeasures directed at poorer families – are effective inimproving home safety and in reducing the risk of<strong>injury</strong> (202–206) and may result in modest reducti<strong>on</strong>s in<strong>injury</strong> rates (198, 202). More robust evaluati<strong>on</strong>, though,112 WORLD REPORT ON CHILD INJURY PREVENTION
is required in this area. The visits appear to be mosteffective when the informati<strong>on</strong> provided is targeted,age-appropriate and combined with the provisi<strong>on</strong> andinstallati<strong>on</strong> of safety equipment (204–207).Community interventi<strong>on</strong>sThe use of multiple strategies repeated in different formsand c<strong>on</strong>texts is a powerful means to foster a culture of safety(208). The preventi<strong>on</strong> of falls is comm<strong>on</strong>ly included am<strong>on</strong>gthe goals of community-based programmes for reducing<strong>child</strong>hood <strong>injury</strong> (209). Measures found to be particularlyeffective in this c<strong>on</strong>text include the installati<strong>on</strong> of windowguards in high-rise buildings, making playgrounds saferand removing baby walkers. In the “Children Can’tFly” programme in New York, important comp<strong>on</strong>entswere surveillance and follow-up, media campaigns andcommunity educati<strong>on</strong> – as well as the provisi<strong>on</strong> to familieswith young <strong>child</strong>ren of free, easily-installable windowguards (49).Some programmes in developing countries haveadopted the WHO Safe Communities model whichincludes safety audits of stairs and balc<strong>on</strong>y rails, andcampaigning for envir<strong>on</strong>mental improvements and saferecreati<strong>on</strong>al areas. However, good evaluati<strong>on</strong>s of theeffectiveness of these programmes, particularly withregard to their impact <strong>on</strong> the incidence of <strong>child</strong>hood fallinjuries, are still not available.Adapting interventi<strong>on</strong>sThere is little evaluative evidence <strong>on</strong> interventi<strong>on</strong>s thatcan reduce the rate of falls and their c<strong>on</strong>sequences indeveloping countries (210). Many measures that haveproved successful in reducing the incidence of fall injuriesin developed countries are limited with regard to theirfeasibility and acceptability in developing countries.Nevertheless, the experience of interventi<strong>on</strong> strategiesin developed countries can suggest suitable programmesin poorer settings. There now exists a range of promisingstrategies to reduce the incidence of <strong>child</strong>hood falls in lowincomeand middle-income countries.A recent overview of programmes in developedcountries to prevent injuries from falls found that –other than general recommendati<strong>on</strong>s about greatersupervisi<strong>on</strong> of <strong>child</strong>ren, interventi<strong>on</strong>s to reduce theheight of playground equipment and appropriate groundsurfacing in playgrounds – <strong>on</strong>ly <strong>on</strong>e proven interventi<strong>on</strong>was definitely transferable to developing countries (210).This was the “Children Can’t Fly” programme alreadymenti<strong>on</strong>ed, that was effective in reducing falls fromhigh-rise buildings in a low-income community in NewYork City. While the materials used and the c<strong>on</strong>text maydiffer, more widespread use in developing countries ofbarriers (such as the window guards in the “ChildrenCan’t Fly” programme) and safety equipment is likelynot <strong>on</strong>ly to be effective but also affordable, feasible andsustainable. Specifically, it is reas<strong>on</strong>able to assume thatreinforced c<strong>on</strong>structi<strong>on</strong> and protective barriers aroundthe periphery of roofs, as well as railings <strong>on</strong> stairs, canreduce the risk of falls am<strong>on</strong>g <strong>child</strong>ren. Furthermore,such measures can be strengthened by introducing andenforcing housing standards and building regulati<strong>on</strong>s(105, 189).As already noted, the most effective interventi<strong>on</strong>s toprevent injuries related to falls from playground equipmenthave focused <strong>on</strong> the use of impact-absorbing materials,height restricti<strong>on</strong>s <strong>on</strong> equipment and the overall designof playgrounds. While the materials may vary, the sameprinciples apply in all countries. A study in a township inJohannesburg, South Africa, found that creating safer andimproved recreati<strong>on</strong>al spaces and play areas for <strong>child</strong>renwas of prime importance for preventing <strong>injury</strong>, as well asviolence, to <strong>child</strong>ren (211).The effectiveness of home visitati<strong>on</strong> programmes inearly <strong>child</strong>hood in reducing the risk of falls and otherinjuries holds particular promise for low-income andmiddle-income countries. Many studies undertakenin high-income countries have focused <strong>on</strong> vulnerablefamilies and used n<strong>on</strong>-professi<strong>on</strong>al visitors (202). Anexploratory study in Jordan of <strong>child</strong>hood injuries,including those from falls, has highlighted the promisingnature of risk inventories prepared by health visitors(162).Several studies from developing countries havec<strong>on</strong>sidered the potential benefits of mass media andpamphlet campaigns (97). Others have examined homesafety and <strong>injury</strong> preventi<strong>on</strong> informati<strong>on</strong> targetedvariously at parents, health-care workers, law enforcementofficers, municipal officials, c<strong>on</strong>structi<strong>on</strong> workers andpolicy-makers (106, 162, 212–214). Features of some ofthese promising programmes include:– the inclusi<strong>on</strong> of public safety messages that corresp<strong>on</strong>dto <strong>child</strong>ren’s cognitive and developmental stages and totheir settings (97, 213);– the combinati<strong>on</strong> of educati<strong>on</strong> with specificenvir<strong>on</strong>mental modificati<strong>on</strong>s to achieve greater safety(90, 211);– the use of culturally appropriate modes of communicati<strong>on</strong>(97, 211);– the formulati<strong>on</strong> of messages that are relevant to thec<strong>on</strong>diti<strong>on</strong>s of poor or marginalized communities (90,211).As already noted, research has so far failed to providec<strong>on</strong>vincing evidence that educati<strong>on</strong>al and awarenessraisingcampaigns, in isolati<strong>on</strong>, are effective in reducingthe incidence of <strong>child</strong>hood fall injuries. It is possible thatthis reflects inadequate data and limitati<strong>on</strong>s in the designof evaluati<strong>on</strong>s (197). On the other hand, the lack of evidencemay be a result of the fact that changes in knowledge andattitudes do not necessarily create corresp<strong>on</strong>ding changesin <strong>injury</strong> rates. The Injury Preventi<strong>on</strong> Project SafetyWORLD REPORT ON CHILD INJURY PREVENTION 113
Survey (TIPP-SS) of the American Academy of Pediatricsis a widely used educati<strong>on</strong>al programme in the UnitedStates that seeks to assess changes in behaviour. A recentstudy of TIPP-SS suggests that rather than behaviour, it isknowledge and attitudes that the survey actually measures(215). Before countries start to invest scarce resources, itis therefore important that educati<strong>on</strong>al campaigns thatappear feasible are carefully evaluated for their ability tosignificantly reduce the rate of injuries.Involving a range of sectorsIt is always necessary to c<strong>on</strong>sider the broader socialdeterminants that affect the incidence of <strong>child</strong>hood falls.Given the different settings and types of <strong>child</strong>hood fall, itis not surprising that preventi<strong>on</strong> efforts cut across a rangeof sectors. For falls involving work in the agriculturalsector, for example, groups involved in preventi<strong>on</strong> includegovernmental and commercial bodies in that sector,landowners, farmers, manufacturers of equipment,occupati<strong>on</strong>al health workers, labour uni<strong>on</strong>s andcommunity groups. Efforts to prevent falls in the homebring in municipal authorities, architects, builders, townplanners, furniture designers, product manufacturers,health-care services, social services and n<strong>on</strong>governmentalorganizati<strong>on</strong>s.Children can incur injuries as a result of <strong>on</strong>e or moreof a range of factors relating to their caregivers. Suchfactors include poverty, ignorance, lack of c<strong>on</strong>trol overthe envir<strong>on</strong>ment, fatigue, depressi<strong>on</strong> and malevolence.Agencies that might address some of these factorsinclude those dealing with mental health and criminaljustice, social service agencies, and community andn<strong>on</strong>governmental organizati<strong>on</strong>s.C<strong>on</strong>clusi<strong>on</strong>s and recommendati<strong>on</strong>sFalls are the most comm<strong>on</strong> cause in many countries of<strong>injury</strong>-related hospital stays and emergency departmentvisits involving <strong>child</strong>ren. Limb fractures and head injuriesare comm<strong>on</strong> and traumatic brain injuries are most likelyto result in lifel<strong>on</strong>g disability. The predisposing factorsand the types of fall vary c<strong>on</strong>siderably across differentsettings. Developing countries have a disproporti<strong>on</strong>atelyhigh rate of fall-related injuries am<strong>on</strong>g <strong>child</strong>ren, andefforts to prevent these injuries are hampered by the lack ofevaluative evidence of interventi<strong>on</strong>s that have been tried inthese countries. Furthermore, although it is clear that thehealth-care sector has a pivotal role to play in preventing<strong>child</strong>hood <strong>injury</strong>, <strong>injury</strong> preventi<strong>on</strong> in many countriesoften does not figure am<strong>on</strong>g the priorities for health.Table 5.3 summarizes the main approaches toaddressing <strong>child</strong>hood falls. The most effective strategies, inall countries, are those that combine proven or promisingmeasures.Recommendati<strong>on</strong>sFrom the discussi<strong>on</strong> in this chapter, a number ofrecommendati<strong>on</strong>s stand out, including the following.Countries should, where possible, develop and promotelocally manufactured, cheap and effective measuresto protect against <strong>child</strong>hood falls – such as windowguards, roof railings and stair gates.Where building regulati<strong>on</strong>s exist, home modificati<strong>on</strong>s– such as the installati<strong>on</strong> of window guards – should beincorporated into the regulati<strong>on</strong>s and enforced.Local authorities should address structural hazards inthe built envir<strong>on</strong>ment that pose fall risks for <strong>child</strong>ren,such as open drains and wells.TABLE 5.3Key strategies to prevent falls am<strong>on</strong>g <strong>child</strong>renStrategyEffectivePromisingInsufficientevidenceIneffectiveHarmfulImplementing multifaceted community programmes such as “Children Can’t Fly”Redesigning nursery furniture and other productsEstablishing playground standards for the depth of appropriate surface material,height of equipment and maintenanceLegislating for window guardsUsing stair gates and guard railsC<strong>on</strong>ducting supportive home visitati<strong>on</strong> and educati<strong>on</strong> for at-risk familiesHolding mass media campaigns directed at parents, health workersProviding appropriate paediatric acute careRaising awareness through educati<strong>on</strong>al campaignsImplementing housing and building codesCovering wells and ditches and removing hazards114 WORLD REPORT ON CHILD INJURY PREVENTION
Local authorities should ensure that <strong>child</strong>ren haveaccess to safe playgrounds and recreati<strong>on</strong>al spaces –thereby encouraging physical activity while at the sametime reducing the risk of fall-related <strong>injury</strong>.Parental supervisi<strong>on</strong> is an important aspect ofpreventi<strong>on</strong>, particularly when combined with otherinterventi<strong>on</strong>s.Acute care and rehabilitati<strong>on</strong> should be available anddevised appropriately for <strong>child</strong>ren, so as to minimizethe l<strong>on</strong>g-term c<strong>on</strong>sequences of falls and prevent l<strong>on</strong>gtermdisability.Community-based <strong>injury</strong> surveys that extend bey<strong>on</strong>dassessments at health-care facilities are needed toobtain epidemiological data <strong>on</strong> fall injuries in lowincomeand middle-income countries. Data <strong>on</strong> thecharacteristics of injuries and the associated risk factorsare of special importance. This research should helpidentify, for a given setting, the five leading causes andtypes of <strong>child</strong>hood fall injuries and point to the mostcost-effective preventi<strong>on</strong> strategies.Large-scale evaluati<strong>on</strong> studies of interventi<strong>on</strong>s forreducing the incidence of <strong>child</strong>hood fall injuries andtheir c<strong>on</strong>sequences urgently need to be undertaken inlow-income and middle-income countries.References1. Rahman A et al. Bangladesh health and <strong>injury</strong> survey<str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> <strong>child</strong>ren. Dhaka, Institute of Child and MotherHealth, 2005.2. Falls. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, Violence andInjury Preventi<strong>on</strong> and Disability Department (http://www.who.int/violence_<strong>injury</strong>_preventi<strong>on</strong>/other_<strong>injury</strong>/falls/en/index.html, accessed 20 March 2008).3. Christoffel KK et al. Standard definiti<strong>on</strong>s for <strong>child</strong>hood<strong>injury</strong> research: excerpts of a c<strong>on</strong>ference <str<strong>on</strong>g>report</str<strong>on</strong>g>. Pediatrics,1992, 89:1027–1034.4. Khambalia A et al. Risk factors for unintenti<strong>on</strong>al injuriesdue to falls in <strong>child</strong>ren aged 0–6 years: a systematic review.Injury Preventi<strong>on</strong>, 2006, 12:378–385.5. Bartlett SN. The problem of <strong>child</strong>ren’s injuries in lowincomecountries: a review. Health Policy and Planning,2002, 17:1–13.6. Morris<strong>on</strong> A, St<strong>on</strong>e DH. Unintenti<strong>on</strong>al <strong>child</strong>hood <strong>injury</strong>mortality in Europe 1984–93: a <str<strong>on</strong>g>report</str<strong>on</strong>g> from the EURORISCWorking Group. Injury Preventi<strong>on</strong>, 1999, 5:171–176.7. A league table of <strong>child</strong> deaths by <strong>injury</strong> in rich countries(Innocenti Report Card No. 2). Florence, UNICEFInnocenti Research Centre, 2001 (http://www.unicef-icdc.org/publicati<strong>on</strong>s/pdf/repcard2e.pdf, accessed 22 January2008).8. Hyder AA et al. Falls am<strong>on</strong>g <strong>child</strong>ren in the developingworld: a gap in <strong>child</strong> health burden estimati<strong>on</strong>s? ActaPaediatrica, 2007, 96:1394–1398.9. Bangdiwala SI et al. The incidence of injuries in youngpeople: I. Methodology and results of a collaborativestudy in Brazil, Chile, Cuba and Venezuela. Internati<strong>on</strong>alJournal of Epidemiology, 1990, 19:115–124.10. Del Ciampo LA et al. Incidence of <strong>child</strong>hood accidentsdetermined in a study of home surveys. Annals of TropicalPaediatrics, 2001, 21:239–243.11. Savitsky B et al. Variability in pediatric <strong>injury</strong> patternsby age and ethnic groups in Israel. Ethnicity and Health,2007, 12:129–139.12. Bener A, Hyder AA, Schenk E. Trends in <strong>child</strong>hood <strong>injury</strong>mortality in a developing country: United Arab Emirates.Accident and Emergency Nursing, 2007, 15:228–233.13. Evbuomwan I. Paediatric trauma admissi<strong>on</strong>s in theSakaka Central Hospital, Al-Jouf Province, Saudi Arabia.Saudi Medical Journal, 1994, 15:435–437.14. Bener A et al. A retrospective descriptive study ofpediatric trauma in a desert country. Indian Pediatrics,1997, 34:1111–1114.15. Linnan M et al. Child mortality and <strong>injury</strong> in Asia:survey results and evidence. Florence, UNICEF InnocentiResearch Centre, 2007 (http://www.unicef-irc.org/publicati<strong>on</strong>s/pdf/iwp_2007_06.pdf, accessed 21 January2008).16. Overpeck MD, McLoughlin E. Did that <strong>injury</strong> happen<strong>on</strong> purpose? Does intent really matter? Injury Preventi<strong>on</strong>,1999, 5:11–12.17. Cheng TL et al. A new paradigm of <strong>injury</strong> intenti<strong>on</strong>ality.Injury Preventi<strong>on</strong>, 1999, 5:59–61.18. Linnan MJ et al. Vietnam multicentre <strong>injury</strong> survey. Hanoi,Hanoi School of Public Health, 2003.19. Jiangxi <strong>injury</strong> survey: <strong>child</strong> <strong>injury</strong> <str<strong>on</strong>g>report</str<strong>on</strong>g>. Jiangxi, JiangxiCenter for Disease C<strong>on</strong>trol, The Alliance for Safe Children,UNICEF–China, Jiangxi Provincial Health Bureau,Chinese Field Epidemiology Training Program, 2006.20. Pickett W et al. Injuries experienced by infant <strong>child</strong>ren:a populati<strong>on</strong>-based epidemiological analysis. Pediatrics,2003, 111:e365–370.21. Steenkamp M, Cripps R. Child injuries due to falls (InjuryResearch and Statistics Series, No. 7). Adelaide, AustralianInstitute of Health and Welfare, 2001.22. WHO mortality database: tables. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> HealthOrganizati<strong>on</strong> (http://www.who.int/healthinfo/morttables/en/index.html, accessed 21 April 2008).23. Pickett W, Hartling L, Bris<strong>on</strong> RJ. A populati<strong>on</strong>-based studyof hospitalized injuries in Kingst<strong>on</strong>, Ontario, identified viathe Canadian Hospitals Injury Reporting and Preventi<strong>on</strong>Program. Chr<strong>on</strong>ic Diseases in Canada, 1997, 18:61–69.24. Agran PF et al. Rates of pediatric injuries by 3-m<strong>on</strong>thintervals for <strong>child</strong>ren 0 to 3 years of age. Pediatrics, 2003,111:e683–692.25. Lam LT, Ross FI, Cass DT. Children at play: the deathand <strong>injury</strong> pattern in New South Wales, Australia, JulyWORLD REPORT ON CHILD INJURY PREVENTION 115
1990–June 1994. Journal of Paediatric Child Health, 1999,35:572–577.26. Warringt<strong>on</strong> SA, Wright CM, ALSPAC Study Team.Accidents and resulting injuries in premobile infants.Archives of Disease in Childhood, 2001, 85:104–107.27. Potoka DA, Schall LC, Ford HR. Improved functi<strong>on</strong>aloutcome for severely injured <strong>child</strong>ren treated at pediatrictrauma centers. Journal of Trauma, 2001, 51:824–834.28. Mo F et al. Adolescent injuries in Canada: findingsfrom the Canadian community health survey, 2000–2001. Internati<strong>on</strong>al Journal of Injury C<strong>on</strong>trol and SafetyPromoti<strong>on</strong>, 2006, 13:235–244.29. Linnan M, Peters<strong>on</strong> P. Child <strong>injury</strong> in Asia: time foracti<strong>on</strong>. Bangkok, The Alliance for Safe Children (TASC)and UNICEF East Asia and Pacific Regi<strong>on</strong>al Office, 2004(http://www.unicef.org/eapro/Child_<strong>injury</strong>_issue_paper.pdf, accessed 20 March 2008).30. El-Chemaly SY et al. Hospital admissi<strong>on</strong>s after paediatrictrauma in a developing country: from falls to landmines.Internati<strong>on</strong>al Journal of Injury C<strong>on</strong>trol and SafetyPromoti<strong>on</strong>, 2007, 14:131–134.31. Linnan M et al. Child mortality and <strong>injury</strong> in Asia: anoverview. Florence, UNICEF, Innocenti Research Centre,2007 (http://www.unicef-irc.org/publicati<strong>on</strong>s/pdf/iwp_2007_04.pdf, accessed 21 January 2008). (InnocentiWorking Paper 2007-04, Special Series <strong>on</strong> Child InjuryNo. 1).32. Kobusingye O, Guwatudde D, Lett R. Injury patterns inrural and urban Uganda. Injury Preventi<strong>on</strong>, 2001, 7:46–50.33. Tercero F et al. The epidemiology of moderate and severeinjuries in a Nicaraguan community: a household-basedsurvey. Public Health, 2006, 120:106–114.34. Hijar-Medina MC et al. Accidentes en el hogar en niñosmenores de 10 años: causas y c<strong>on</strong>secuencias [Homeaccidents in <strong>child</strong>ren less than 10 years of age: causes andc<strong>on</strong>sequences]. Salud Pública de México, 1992, 34:615–625.35. Fatmi Z et al. Incidence, patterns and severity of <str<strong>on</strong>g>report</str<strong>on</strong>g>edunintenti<strong>on</strong>al injuries in Pakistan for pers<strong>on</strong>s five yearsand older: results of the Nati<strong>on</strong>al Health Survey of Pakistan1990–94. BMC Public Health, 2007, 7:152.36. Bachani A et al. The burden of falls in Pakistan: the resultsof the 1st Nati<strong>on</strong>al Injury Survey. Baltimore, MD, JohnsHopkins University, 2007.37. Garretts<strong>on</strong> LK, Gallagher SS. Falls in <strong>child</strong>ren and youth.Pediatric Clinics of North America, 1985, 32:153–162.38. Mosenthal AC et al. Falls: epidemiology and strategiesfor preventi<strong>on</strong>. Journal of Trauma: Injury, Infecti<strong>on</strong>, andCritical Care, 1995, 38:753–756.39. Buckman RF, Buckman PD. Vertical decelerati<strong>on</strong> trauma:principles of management. Surgical Clinics of NorthAmerica, 1991, 71:331–344.40. Warner KG, Demling RH. The pathophysiology of freefall<strong>injury</strong>. Annals of Emergency Medicine, 1986, 15:1088–1093.41. Barlow B et al. Ten years of experience with falls froma height in <strong>child</strong>ren. Journal of Pediatric Surgery, 1983,18:509–511.42. Chalmers DJ et al. Height and surfacing as risk factors for<strong>injury</strong> in falls from playground equipment: a case-c<strong>on</strong>trolstudy. Injury Preventi<strong>on</strong>, 1996, 2:98–104.43. Macarthur C et al. Risk factors for severe injuries associatedwith falls from playground equipment. Accident Analysisand Preventi<strong>on</strong>, 2000, 32:377–382.44. Mott A et al. Safety of surfaces and equipment for <strong>child</strong>renin playgrounds. The Lancet, 1997, 349:1874–1876.45. Mowat DL et al. A case-c<strong>on</strong>trol study of risk factors forplayground injuries am<strong>on</strong>g <strong>child</strong>ren in Kingst<strong>on</strong> and area.Injury Preventi<strong>on</strong>, 1998, 4:39–43.46. Bertocci GE et al. Influence of fall height and impactsurface <strong>on</strong> biomechanics of feet-first free falls in <strong>child</strong>ren.Injury, 2004, 35:417–424.47. Sieben RL, Leavitt JD, French JH. Falls as <strong>child</strong>hoodaccidents: an increasing urban risk. Pediatrics, 1971,47:886–892.48. Bergner L, Mayer S, Harris D. Falls from heights: a<strong>child</strong>hood epidemic in an urban area. American Journalof Public Health, 1971, 61:90–96.49. Spiegel CN, Lindaman FC. Children can’t fly: a programto prevent <strong>child</strong>hood morbidity and mortality fromwindow falls. American Journal of Public Health, 1977,67:1143–1147.50. Barss P et al. Injury preventi<strong>on</strong>: an internati<strong>on</strong>al perspective.Epidemiology, surveillance and policy. L<strong>on</strong>d<strong>on</strong>, OxfordUniversity Press, 1998.51. American Academy of Paediatrics. Falls from heights:windows, roofs and balc<strong>on</strong>ies. Pediatrics, 2001, 107:1188–1191.52. Beijing <strong>injury</strong> survey: <strong>child</strong> <strong>injury</strong> <str<strong>on</strong>g>report</str<strong>on</strong>g>. Beijing, ChineseField Epidemiology Training Program, The Alliance forSafe Children, UNICEF–China, 2003.53. Adesunkanmi AR, Oseni SA, Badru OS. Severity andoutcome of falls in <strong>child</strong>ren. West African Journal ofMedicine, 1999, 18:281–285.54. Chalmers DJ, Langley JD. Epidemiology of playgroundequipment injuries resulting in hospitalizati<strong>on</strong>. Journal ofPaediatrics and Child Health, 1990, 26:329–334.55. Reiber GD. Fatal falls in <strong>child</strong>hood. How far must <strong>child</strong>renfall to sustain fatal head <strong>injury</strong>? Report of cases and reviewof the literature. American Journal of Forensic Medicineand Pathology, 1993, 14:201–207.56. Chadwick DL et al. Deaths from falls in <strong>child</strong>ren: how faris fatal? Journal of Trauma: Injury, Infecti<strong>on</strong>, and CriticalCare, 1991, 31:1353–1355.116 WORLD REPORT ON CHILD INJURY PREVENTION
57. Williams RA. Injuries in infants and small <strong>child</strong>renresulting from witnessed and corroborated free falls.Journal of Trauma, 1991, 31:1350–1352.58. Goodacre S et al. Can the distance fallen predict serious<strong>injury</strong> after a fall from a height? Journal of Trauma: Injury,Infecti<strong>on</strong>, and Critical Care, 1999, 46:1055–1058.59. Abdullah J et al. Persistence of cognitive deficits followingpaediatric head <strong>injury</strong> without professi<strong>on</strong>al rehabilitati<strong>on</strong>in rural East Coast Malaysia. Asian Journal of Surgery,2005, 28:163–167.60. Hyder AA et al. The impact of traumatic brain injuries: aglobal perspective. Neurorehabilitati<strong>on</strong>, 2007, 22:341.61. Ong L et al. Outcome of closed head <strong>injury</strong> in Malaysian<strong>child</strong>ren: neurocognitive and behavioural sequelae.Journal of Paediatrics and Child Health, 1998, 34:363–368.62. Langlois JA, Rutland-Brown W, Thomas KE. Traumaticbrain <strong>injury</strong> in the United States: emergency departmentvisits, hospitalizati<strong>on</strong>s, and deaths. Atlanta, GA, Centersfor Disease C<strong>on</strong>trol and Preventi<strong>on</strong>, Nati<strong>on</strong>al Center forInjury Preventi<strong>on</strong> and C<strong>on</strong>trol, 2006.63. Williams<strong>on</strong> LM, Morris<strong>on</strong> A, St<strong>on</strong>e DH. Trends in head<strong>injury</strong> mortality am<strong>on</strong>g 0–14 year olds in Scotland (1986–95). Journal of Epidemiology and Community Health,2002, 56:285–288.64. Brookes M et al. Head injuries in accident and emergencydepartments. How different are <strong>child</strong>ren from adults?Journal of Epidemiology and Community Health, 1990,44:147–151.65. Tiret L et al. The epidemiology of head trauma inAquitaine (France), 1986: a community-based study ofhospital admissi<strong>on</strong>s and deaths. Internati<strong>on</strong>al Journal ofEpidemiology, 1990, 19:133–140.66. Zargar M, Khaji A, Karbakhsh M. Injuries caused by fallsfrom trees in Tehran, Islamic Republic of Iran. EasternMediterranean Health Journal, 2005,11:235–239.67. Al-Jadid MS, Al-Asmari AK, Al-Moutaery KR. Quality oflife in males with spinal cord <strong>injury</strong> in Saudi Arabia. SaudiMedical Journal, 2004, 25:1979–1985.68. Cirak B et al. Spinal injuries in <strong>child</strong>ren. Journal ofPediatric Surgery, 2004, 39:607–612.69. Ok<strong>on</strong>kwo CA. Spinal cord injuries in Enugu, Nigeria:preventable accidents. Paraplegia, 1988, 26:12–18.70. Kopjar B, Wickizer TM. Fractures am<strong>on</strong>g <strong>child</strong>ren:incidence and impact <strong>on</strong> daily activities. Injury Preventi<strong>on</strong>,1998, 4:194–197.71. Rennie L et al. The epidemiology of fractures in <strong>child</strong>ren.Injury, 2007, 38:913–922.72. Smith MD, Burringt<strong>on</strong> JD, Woolf AD. Injuries in <strong>child</strong>rensustained in free falls: an analysis of 66 cases. Journal ofTrauma: Injury, Infecti<strong>on</strong>, and Critical Care, 1975, 15:987–991.73. Hansoti B, Beattie T. Can the height of a fall predict l<strong>on</strong>gb<strong>on</strong>e fracture in <strong>child</strong>ren under 24 m<strong>on</strong>ths? EuropeanJournal of Emergency Medicine, 2005, 12:285–286.74. Helps YLM, Pointer SC. Child <strong>injury</strong> due to falls fromplayground equipment, Australia 2002–04. Canberra,Australian Institute of Health and Welfare, 2006.75. Ball DJ. Trends in fall injuries associated with <strong>child</strong>ren’soutdoor climbing frames. Internati<strong>on</strong>al Journal of InjuryC<strong>on</strong>trol and Safety Promoti<strong>on</strong>, 2007, 14:49–53.76. Mitchell R et al. Falls from playground equipment: willthe new Australian playground safety standard make adifference and how will we tell? Health Promoti<strong>on</strong> Journalof Australia, 2007, 18:98–104.77. Bach O et al. Disability can be avoided after open fracturesin Africa: results from Malawi. Injury, 2004, 35:846–851.78. Mock CN. Injury in the developing world. Western Journalof Medicine, 2001, 175:372–374.79. Dhill<strong>on</strong> KS, Sengupta S, Singh BJ. Delayed management offracture of the lateral humeral c<strong>on</strong>dyle in <strong>child</strong>ren. ActaOrthopaedica Scandinavica, 1988, 59:419–424.80. Musemeche CA et al. Pediatric falls from heights. Journalof Trauma: Injury, Infecti<strong>on</strong>, and Critical Care, 1991,31:1347–1349.81. Thailand <strong>injury</strong> survey: Child <strong>injury</strong> <str<strong>on</strong>g>report</str<strong>on</strong>g>. Bangkok,Institute for Health Research, Chulal<strong>on</strong>gkorn University,The Alliance for Safe Children, UNICEF–Thailand, 2004.82. The ec<strong>on</strong>omic burden of unintenti<strong>on</strong>al <strong>injury</strong> in Canada.Tor<strong>on</strong>to, ON, Smartrisk; Emergency Health ServicesBranch, Ministry of Health, Ontario, 1998.83. Falls fact sheet. Washingt<strong>on</strong>, DC, Nati<strong>on</strong>al SAFE KIDSCampaign, 2004 (http://www.usa.safekids.org/tier3_cd.cfm?folder_id=540&c<strong>on</strong>tent_item_id=1050, accessed20 March 2008).84. Pressley JC et al. Nati<strong>on</strong>al <strong>injury</strong>-related hospitalizati<strong>on</strong>sin <strong>child</strong>ren: public versus private expenditures acrosspreventable <strong>injury</strong> mechanisms. Journal of Trauma: Injury,Infecti<strong>on</strong>, and Critical Care, 2007, 63(Suppl):S10–S19.85. Simm<strong>on</strong>s D. Accidents in Malawi. Archives of Disease inChildhood, 1985, 60:64–66.86. Gurses D et al. Cost factors in pediatric trauma. CanadianJournal of Surgery, 2003, 46:441–445.87. Bickler SW, Rode H. Surgical services for <strong>child</strong>renin developing countries. Bulletin of the <str<strong>on</strong>g>World</str<strong>on</strong>g> HealthOrganizati<strong>on</strong>, 2002, 80:829–835.88. Bickler SW, Sanno-Duanda B. Epidemiology of paediatricsurgical admissi<strong>on</strong>s to a government referral hospital inthe Gambia. Bulletin of the <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>,2000, 78:1330–1336.89. Flavin MP et al. Stages of development and <strong>injury</strong> patternsin the early years: a populati<strong>on</strong>-based analysis. BMC PublicHealth, 2006, 6:187.90. Towner E et al. Accidental falls: fatalities and injuries: anexaminati<strong>on</strong> of the data sources and review of the literatureWORLD REPORT ON CHILD INJURY PREVENTION 117
<strong>on</strong> preventive strategies. L<strong>on</strong>d<strong>on</strong>, Department of Tradeand Industry, 1999.91. Berger SE, Theuring C, Adolph KE. How and when infantslearn to climb stairs. Infant Behavior and Development,2007, 30:36–49.92. Matheny AP. Accidental injuries. In: Routh D, ed.Handbook of pediatric psychology. New York, NY, GuilfordPress, 1988.93. Needleman RD. Growth and development. In: BehrmanRE et al., eds. Nels<strong>on</strong> Textbook of Pediatrics, 17th ed.Philadelphia, PA, Saunders, 2003:23–66.94. Ozanne-Smith J et al. Community based <strong>injury</strong> preventi<strong>on</strong>evaluati<strong>on</strong> <str<strong>on</strong>g>report</str<strong>on</strong>g>: Shire of Bulla Safe Living Program.Canberra, M<strong>on</strong>ash University Accident Research Centre,1994 (Report No. 6).95. Schelp L, Ekman R, Fahl I. School accidents during athree school-year period in a Swedish municipality. PublicHealth, 1991, 105:113–120.96. Bangdiwala SI, Anzola-Perez E. The incidence of injuriesin young people: log-linear multivariable models for riskfactors in a collaborative study in Brazil, Chile, Cuba andVenezuela. Internati<strong>on</strong>al Journal of Epidemiology, 1990,19:125–132.97. Hijar-Medina MC et al. Factores de riesgo de accidentesen el hogar en niños. Estudio de casos y c<strong>on</strong>troles [Therisk factors for home accidents in <strong>child</strong>ren. A case-c<strong>on</strong>trolstudy]. Boletín Médico del Hospital Infantil de México,1993, 50:463–474.98. Mohan D. Childhood injuries in India: extent of theproblem and strategies for c<strong>on</strong>trol. Indian Journal ofPediatrics, 1986, 53:607–615.99. Yagmur Y et al. Falls from flat-roofed houses: a surgicalexperience of 1643 patients. Injury, 2004, 35:425–428.100. Krug EG, Sharma GK, Lozano R. The global burden ofinjuries. American Journal of Public Health, 2000, 90:523–526.101. Rivara FP et al. Populati<strong>on</strong>-based study of fall injuries in<strong>child</strong>ren and adolescents resulting in hospitalizati<strong>on</strong> ordeath. Pediatrics, 1993, 92:61–63.102. Roudsari BS, Shadman M, Ghodsi M. Childhood traumafatality and resource allocati<strong>on</strong> in <strong>injury</strong> c<strong>on</strong>trol programsin a developing country. BMC Public Health, 2006, 6:117.103. Iltus S. Parental ideologies in the home safety managementof <strong>on</strong>e to four year old <strong>child</strong>ren. New York, NY, GraduateSchool and University Center of the City University ofNew York, 1994.104. Wazana A. Are there <strong>injury</strong>-pr<strong>on</strong>e <strong>child</strong>ren? A criticalreview of the literature. Canadian Journal of Psychiatry,1997, 42:602–610.105. Morr<strong>on</strong>giello BA, Dawber T. Mothers’ resp<strong>on</strong>ses to s<strong>on</strong>sand daughters engaging in <strong>injury</strong>-risk behaviors <strong>on</strong> aplayground: implicati<strong>on</strong>s for sex differences in <strong>injury</strong>rates. Journal of Experimental Child Psychology, 2000,76:89–103.106. Reading R et al. Accidents to preschool <strong>child</strong>ren:comparing family and neighbourhood risk factors. SocialScience and Medicine, 1999, 48:321–330.107. Engstrom K, Diderichsen F, Laflamme L. Socioec<strong>on</strong>omicdifferences in <strong>injury</strong> risks in <strong>child</strong>hood and adolescence:a nati<strong>on</strong>-wide study of intenti<strong>on</strong>al and unintenti<strong>on</strong>alinjuries in Sweden. Injury Preventi<strong>on</strong>, 2002, 8:137–142.108. Faelker T, Pickett W, Bris<strong>on</strong> RJ. Socioec<strong>on</strong>omic differencesin <strong>child</strong>hood <strong>injury</strong>: a populati<strong>on</strong> based epidemiologicstudy in Ontario, Canada. Injury Preventi<strong>on</strong>, 2000, 6:203–208.109. Pensola TH, Valk<strong>on</strong>en T. Mortality differences by parentalsocial class from <strong>child</strong>hood to adulthood. Journal ofEpidemiology and Community Health, 2000, 54:525–529.110. Thanh NX et al. Does the “Injury poverty trap” exist? Al<strong>on</strong>gitudinal study from Bavi, Vietnam. Health Policy,2006, 78:249–257.111. Shenassa ED, Stubbendick A, Brown MJ. Social disparitiesin housing and related pediatric <strong>injury</strong>: a multilevel study.American Journal of Public Health, 2004, 94:633–639.112. Thanh NX et al. Does poverty lead to n<strong>on</strong>-fatalunintenti<strong>on</strong>al injuries in rural Vietnam? Internati<strong>on</strong>alJournal of Injury C<strong>on</strong>trol and Safety Promoti<strong>on</strong>, 2005,12:31–37.113. Reichenheim ME, Harpham T. Child accidents andassociated risk factors in a Brazilian squatter settlement.Health Policy and Planning, 1989, 4:162–167.114. Rizvi N et al. Distributi<strong>on</strong> and circumstances of injuriesin squatter settlements in Karachi, Pakistan. AccidentAnalysis and Preventi<strong>on</strong>, 2006, 38:526–531.115. Dunne RG, Asher KN, Rivara FP. Injuries in youngpeople with developmental disabilities: comparativeinvestigati<strong>on</strong> from the 1988 Nati<strong>on</strong>al Health InterviewSurvey. Mental Retardati<strong>on</strong>, 1993, 31:83–88.116. Sherrard J, T<strong>on</strong>ge BJ, Ozanne-Smith J. Injury inyoung people with intellectual disability: descriptiveepidemiology. Injury Preventi<strong>on</strong>, 2001, 7:56–61.117. Gallagher SS et al. The incidence of injuries am<strong>on</strong>g 87,000Massachusetts <strong>child</strong>ren and adolescents: results of the1980–81 Statewide Childhood Injury Preventi<strong>on</strong> ProgramSurveillance System. American Journal of Public Health,1984, 74:1340–1347.118. Petridou E et al. Injuries am<strong>on</strong>g disabled <strong>child</strong>ren: a studyfrom Greece. Injury Preventi<strong>on</strong>, 2003, 9:226–230.119. Ozanne-Smith J, Heffernan CJ. Child injuries associatedwith nursery furniture. Melbourne, M<strong>on</strong>ash UniversityAccident Research Centre, 1990:16.120. Wats<strong>on</strong> W, Ozanne-Smith J, Lough J. C<strong>on</strong>sumer productrelated <strong>injury</strong> to <strong>child</strong>ren. Melbourne, M<strong>on</strong>ash UniversityAccident Research Centre, 2000.121. Wats<strong>on</strong> W et al. Injuries associated with nursery furnitureand bunk beds. Melbourne, M<strong>on</strong>ash University AccidentResearch Centre, 1997.118 WORLD REPORT ON CHILD INJURY PREVENTION
122. Selbst SM, Baker MD, Shames M. Bunk bed injuries.American Journal of Diseases of Children, 1990, 144:721–723.123. Edwards DJ. Tarzan swings: a dangerous new epidemic.British Journal of Sports Medicine, 1991, 25:168–169.124. Vioreanu M et al. Heelys and street gliders injuries: a newtype of pediatric <strong>injury</strong>. Pediatrics, 2007, 119:e1294–1298.125. Brudvik C. Injuries caused by small wheel devices.Preventi<strong>on</strong> Science, 2006, 7:313–320.126. Knox CL, Comstock RD. Video analysis of falls experiencedby paediatric iceskaters and roller/inline skaters. BritishJournal of Sports Medicine, 2006, 40:268–271.127. Knox CL et al. Differences in the risk associated with head<strong>injury</strong> for pediatric ice skaters, roller skaters, and in-lineskaters. Pediatrics, 2006, 118:549–554.128. Linakis JG et al. Emergency department visits for pediatrictrampoline-related injuries: an update. AcademicEmergency Medicine, 2007, 14:539–544.129. Black GB, Amadeo R. Orthopedic injuries associated withbackyard trampoline use in <strong>child</strong>ren. Canadian Journal ofSurgery, 2003, 46:199–201.130. Zimmerman N, Bauer R. Injuries in the EuropeanUni<strong>on</strong>: statistics summary 2002–2004. Vienna, EuropeanAssociati<strong>on</strong> for Injury Preventi<strong>on</strong> and Safety Promoti<strong>on</strong>(EuroSafe), 2006.131. Oh D. Heelys injuries in <strong>child</strong>ren. Singapore MedicalJournal, 2006, 47:375.132. Lenehan B et al. Heely injuries: a new epidemic warrantinga government health warning! Injury, 2007, 38:923–925.133. Mott A et al. Patterns of injuries to <strong>child</strong>ren <strong>on</strong> publicplaygrounds. Archives of Disease in Childhood, 1994,71:328–330.134. Injury hospitalisati<strong>on</strong>s in Victoria 1991–92. A <str<strong>on</strong>g>report</str<strong>on</strong>g>focusing <strong>on</strong> the injuries of <strong>child</strong>ren and youth. Melbourne,Victorian Government Department of Health andCommunity Services, 1995.135. Nort<strong>on</strong> C, Nix<strong>on</strong> J, Sibert JR. Playground injuries to<strong>child</strong>ren. Archives of Disease in Childhood, 2004, 89:103–108.136. Briss PA et al. Injuries from falls <strong>on</strong> playgrounds: effectsof day care center regulati<strong>on</strong> and enforcement. Archives ofPediatrics and Adolescent Medicine, 1995, 149:906–911.137. Laforest S et al. Surface characteristics, equipment height,and the occurrence and severity of playground injuries.Injury Preventi<strong>on</strong>, 2001, 7:35–40.138. Petridou E et al. Injuries in public and private playgrounds:the relative c<strong>on</strong>tributi<strong>on</strong> of structural, equipment andhuman factors. Acta Paediatrica, 2002, 91:691–697.139. Sherker S et al. Out <strong>on</strong> a limb: risk factors for arm fracturein playground equipment falls. Injury Preventi<strong>on</strong>, 2005,11:120–124.140. Ly<strong>on</strong>s RA et al. Children’s fractures: a populati<strong>on</strong> basedstudy. Injury Preventi<strong>on</strong>, 1999, 5:129–132.141. Scheiber RA et al. Risk factors for injuries from in-lineskating and the effectiveness of safety gear. New EnglandJournal of Medicine, 1996, 335:1630–1635.142. Kim KJ et al. Shock attenuati<strong>on</strong> of various protectivedevices for preventi<strong>on</strong> of fall-related injuries of theforearm/hand complex. American Journal of SportsMedicine, 2006, 34:637–643.143. Hendricks KJ et al. Injuries to youth living <strong>on</strong> U.S. farmsin 2001 with comparis<strong>on</strong> to 1998. Journal of Agromedicine,2005, 10:19–26.144. Jagodzinski T, DeMuri GP. Horse-related injuries in<strong>child</strong>ren: a review. Wisc<strong>on</strong>sin Medical Journal, 2005,104:50–54.145. Smith GA et al. Pediatric farm-related injuries: a series of96 hospitalized patients. Clinical Pediatrics, 2004, 43:335–342.146. Dekker R et al. L<strong>on</strong>g-term outcome of equestrian injuriesin <strong>child</strong>ren. Disability and Rehabilitati<strong>on</strong>, 2004, 26:91–96.147. Ugboko VI et al. Facial injuries caused by animals innorthern Nigeria. British Journal of Oral and MaxillofacialSurgery, 2002, 40:433–437.148. Nawaz A et al. Camel-related injuries in the pediatric agegroup. Journal of Pediatric Surgery, 2005, 40:1248–1251.149. Bener A et al. Camel racing injuries am<strong>on</strong>g <strong>child</strong>ren.Clinical Journal of Sport Medicine, 2005, 15:290–293.150. Caine D, Caine C. Child camel jockeys: a present-daytragedy involving <strong>child</strong>ren and sport. Clinical Journal ofSport Medicine, 2005, 15:287–289.151. Khalaf S. Camel racing in the Gulf: notes <strong>on</strong> the evoluti<strong>on</strong>of a traditi<strong>on</strong>al sport. Anthropos, 1999, 94:85–105.152. Cummins SK, Jacks<strong>on</strong> RJ. The built envir<strong>on</strong>ment and<strong>child</strong>ren’s health. Pediatric Clinics of North America, 2001,48:1241–1252.153. Garbarino J. Preventing <strong>child</strong>hood <strong>injury</strong>: developmentaland mental health issues. American Journal ofOrthopsychiatry, 1988, 58:25–45.154. Peters<strong>on</strong> L, Ewigman B, Kivlahan C. Judgments regardingappropriate <strong>child</strong> supervisi<strong>on</strong> to prevent <strong>injury</strong>: the roleof envir<strong>on</strong>mental risk and <strong>child</strong> age. Child Development,1993, 64:934–950.155. Rieder MJ, Schwartz C, Newman J. Patterns of walker useand walker <strong>injury</strong>. Pediatrics, 1986, 78:488–493.156. Coats TJ, Allen M. Baby walker related injuries: ac<strong>on</strong>tinuing problem. Archives of Emergency Medicine,1991, 8:52–55.157. Partingt<strong>on</strong> MD, Swans<strong>on</strong> JA, Meyer FB. Head <strong>injury</strong> andthe use of baby walkers: a c<strong>on</strong>tinuing problem. Annals ofEmergency Medicine, 1991, 20:652–654.158. Chen X et al. Frequency of caregiver supervisi<strong>on</strong> of young<strong>child</strong>ren during play. Internati<strong>on</strong>al Journal of InjuryC<strong>on</strong>trol and Safety Promoti<strong>on</strong>, 2007, 14:122–124.WORLD REPORT ON CHILD INJURY PREVENTION 119
159. Munro SA, van Niekerk A, Seedat M. Childhoodunintenti<strong>on</strong>al injuries: the perceived impact of theenvir<strong>on</strong>ment, lack of supervisi<strong>on</strong> and <strong>child</strong> characteristics.Child: Care, Health and Development, 2006, 32:269–279.160. Mull DS et al. Injury in <strong>child</strong>ren of low-income Mexican,Mexican American, and n<strong>on</strong>-Hispanic white mothersin the USA: a focused ethnography. Social Science andMedicine, 2001, 52:1081–1091.161. Thompst<strong>on</strong>e G, Chen J, Emm<strong>on</strong>s K. The participati<strong>on</strong>of <strong>child</strong>ren and young people in emergencies: a guide forrelief agencies based largely <strong>on</strong> experiences in the Asiantsunami resp<strong>on</strong>se. Bangkok, UNICEF East Asia and PacificRegi<strong>on</strong>al Office, 2007 (http://www.unicef.org/eapro/the_participati<strong>on</strong>_of_<strong>child</strong>ren_and_young_people_in_emergencies.pdf, accessed 21 March 2008).162. Jans<strong>on</strong> S et al. Accident risks for suburban preschoolJordanian <strong>child</strong>ren. Journal of Tropical Pediatrics, 1994,40:88–93.163. Drachler M et al. Effect of the home envir<strong>on</strong>ment <strong>on</strong>unintenti<strong>on</strong>al domestic injuries and related health careattendance in infants. Acta Paediatrica, 2007, 96:1169–1173.164. Howe LD, Huttly SRA, Abramsky T. Risk factors forinjuries in young <strong>child</strong>ren in four developing countries:the Young Lives Study. Tropical Medicine and Internati<strong>on</strong>alHealth, 2006, 11:1557–1566.165. Landman PF, Landman GB. Accidental injuries in<strong>child</strong>ren in day-care centers. American Journal of Diseasesof Children, 1987, 141:292–293.166. Wasserman RC et al. Injury hazards in home day care.Journal of Pediatrics, 1989, 114:591–593.167. Kopjar B, Wickizer T. How safe are day care centers? Daycare versus home injuries am<strong>on</strong>g <strong>child</strong>ren in Norway.Pediatrics, 1996, 97:43–47.168. Rivara FP et al. Risk of <strong>injury</strong> to <strong>child</strong>ren less than 5 yearsof age in day care versus home care settings. Pediatrics,1989, 84:1011–1016.169. Richter ED, Jacobs J. Work injuries and exposures in<strong>child</strong>ren and young adults: review and recommendati<strong>on</strong>sfor acti<strong>on</strong>. American Journal of Industrial Medicine, 1991,19:747–769.170. Tackling hazardous <strong>child</strong> labour in agriculture: guidance<strong>on</strong> policy and practice. User guide. Geneva, Internati<strong>on</strong>alLabour Organizati<strong>on</strong>, 2006 (http://tinyurl.com/24lfar,accessed 21 March 2008).171. Pickett W et al. Pediatric farm injuries involving n<strong>on</strong>working<strong>child</strong>ren injured by a farm work hazard: fivepriorities for primary preventi<strong>on</strong>. Injury Preventi<strong>on</strong>, 2005,11:6–11.172. Pickett W et al. Pediatric fall injuries in agriculturalsettings: a new look at a comm<strong>on</strong> <strong>injury</strong> c<strong>on</strong>trol problem.Journal of Occupati<strong>on</strong>al and Envir<strong>on</strong>mental Medicine,2007, 49:461–468.173. Noe R et al. Occupati<strong>on</strong>al injuries identified by anemergency department based <strong>injury</strong> surveillance systemin Nicaragua. Injury Preventi<strong>on</strong>, 2004, 10:227–232.174. Thepaksorn P et al. Occupati<strong>on</strong>al accidents and injuriesin Thailand. Internati<strong>on</strong>al Journal of Occupati<strong>on</strong>al andEnvir<strong>on</strong>mental Health, 2007, 13:290–294.175. Xia ZL et al. Fatal occupati<strong>on</strong>al injuries in a newdevelopment area in the People’s Republic of China.Journal of Occupati<strong>on</strong>al and Envir<strong>on</strong>mental Medicine,2000, 42:917–922.176. Mock CN, Denno D, Adzotor E. Paediatric trauma in therural developing world: low cost measures to improveoutcome. Injury, 1993, 24:291–296.177. Edet EE. Agent and nature of <strong>child</strong>hood <strong>injury</strong> and initialcare provided at the community level in Ibadan, Nigeria.Central African Journal of Medicine, 1996, 42:347–349.178. Mock CN et al. Trauma mortality patterns in three nati<strong>on</strong>sat different ec<strong>on</strong>omic levels: implicati<strong>on</strong>s for global traumasystem development. Journal of Trauma: Injury, Infecti<strong>on</strong>,and Critical Care, 1998, 44:804–814.179. West<strong>on</strong> PM. Care of the injured in the Third <str<strong>on</strong>g>World</str<strong>on</strong>g>: whatcan we learn? Injury, 1987, 18:297–303.180. MacKay M et al. Child safety good practice guide: goodinvestments in unintenti<strong>on</strong>al <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> andsafety promoti<strong>on</strong>. Amsterdam, European Child SafetyAlliance (EuroSafe), 2006.181. American Academy of Pediatrics, Committee <strong>on</strong> InjuryViolence and Pois<strong>on</strong> Preventi<strong>on</strong>. Shopping cart-relatedinjuries to <strong>child</strong>ren. Pediatrics, 2006, 118:825–827.182. Nursery products <str<strong>on</strong>g>report</str<strong>on</strong>g>. Washingt<strong>on</strong>, DC, United StatesC<strong>on</strong>sumer Product Safety Commissi<strong>on</strong>, 2000 (http://www.cpsc.gov/library/nursry00.pdf, accessed 21 March2008).183. Sherker S, Short A, Ozanne-Smith J. The in situperformance of playground surfacing: implicati<strong>on</strong>s formaintenance and <strong>injury</strong> preventi<strong>on</strong>. Internati<strong>on</strong>al Journalof Injury C<strong>on</strong>trol and Safety Promoti<strong>on</strong>, 2005, 12:63–66.184. Johns E, Farrant G, Civil I. Animal-related <strong>injury</strong> in anurban New Zealand populati<strong>on</strong>. Injury, 2004, 35:1234–1238.185. Holland AJ et al. Horse-related injuries in <strong>child</strong>ren.Medical Journal of Australia, 2001, 175:609–612.186. Ball CG et al. Equestrian injuries: incidence, <strong>injury</strong>patterns, and risk factors for 10 years of major traumaticinjuries. American Journal of Surgery, 2007, 193:636–640.187. Forjuoh SN, Li G. A review of successful transport andhome <strong>injury</strong> interventi<strong>on</strong>s to guide developing countries.Social Science and Medicine, 1996, 43:1551–1560.188. Ozanne-Smith J. Child <strong>injury</strong> by developmental stage.Australian Journal of Early Childhood, 1992, 17:39–48.189. Safety aspects: guidelines for <strong>child</strong> safety. Geneva,Internati<strong>on</strong>al Standardizati<strong>on</strong> Organizati<strong>on</strong>, 2002 (ISO/IEC Guide No. 50).120 WORLD REPORT ON CHILD INJURY PREVENTION
190. Standard c<strong>on</strong>sumer safety performance specificati<strong>on</strong>for infant walkers (ASTM F977-96). Philadelphia, PA,American Society for Testing and Materials, 1996.191. Sherker S, Ozanne-Smith J. Are current playground safetystandards adequate for preventing arm fractures? MedicalJournal of Australia, 2004, 180:562–565 [Erratum appearsin Medical Journal of Australia, 2004, 181:532].192. Al-Nouri L, Al-Isami SA. Baby walker injuries. Annals ofTropical Paediatrics, 2006, 26:67–71.193. Kendrick D et al. Promoting <strong>child</strong> safety in primary care: acluster randomised c<strong>on</strong>trolled trial to reduce baby walkeruse. British Journal of General Practice, 2005, 55:582–588.194. Kravitz H. Preventi<strong>on</strong> of accidental falls in infancyby counseling mothers. Illinois Medical Journal, 1973,144:570–573.195. C<strong>on</strong>ners GP et al. Still falling: a community-wide infantwalker <strong>injury</strong> preventi<strong>on</strong> initiative. Patient Educati<strong>on</strong> andCounselling, 2002, 46:169–173.196. Towner E, Erringt<strong>on</strong> G. How can injuries in <strong>child</strong>ren andolder people be prevented? Copenhagen, WHO Regi<strong>on</strong>alOffice for Europe, Health Evidence Network (HEN),2004 (http://www.euro.who.int/Document/E84938.pdf,accessed 21 March 2008).197. Kendrick D et al. Home safety educati<strong>on</strong> and provisi<strong>on</strong> ofsafety equipment for <strong>injury</strong> preventi<strong>on</strong>. Cochrane Databaseof Systematic Reviews, 2007, (1):CD005014.198. Kendrick D, Mulvaney C, Wats<strong>on</strong> M. Does targeting<strong>injury</strong> preventi<strong>on</strong> towards families in disadvantaged areasreduce inequalities in safety practice? Health Educati<strong>on</strong>Research, 2008 (http://her.oxfordjournals.org/cgi/c<strong>on</strong>tent/full/cym083, accessed 14 August 2008)..199. Gielen AC et al. Using a computer kiosk to promote <strong>child</strong>safety: results from a randomized c<strong>on</strong>trolled trial in anurban pediatric emergency department. Pediatrics, 2007,120:330–339.200. Hart JT. The Inverse Care Law. The Lancet, 1971, i:405–412.201. Gwatkin DR. Health inequalities and the health of thepoor: what do we know? What can we do? Bulletin of the<str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2000, 78:3–18.202. Roberts I, Kramer MS, Suissa S. Does home visiting prevent<strong>child</strong>hood <strong>injury</strong>? A systematic review of randomisedc<strong>on</strong>trolled trials. British Medical Journal, 1996, 312:29–33.203. King WJ et al. L<strong>on</strong>g term effects of a home visit to prevent<strong>child</strong>hood <strong>injury</strong>: three year follow up of a randomizedtrial. Injury Preventi<strong>on</strong>, 2005, 11:106–109.204. Posner JC et al. A randomized, clinical trial of a homesafety interventi<strong>on</strong> based in an emergency departmentsetting. Pediatrics, 2004, 113:1603–1608.205. Clamp M, Kendrick D. A randomised c<strong>on</strong>trolled trialof general practiti<strong>on</strong>er safety advice for families with<strong>child</strong>ren under 5 years. British Medical Journal, 1998,316:1576–1579.206. Wats<strong>on</strong> M et al. Providing <strong>child</strong> safety equipment toprevent injuries: randomised c<strong>on</strong>trolled trial. BritishMedical Journal, 2005, 330:178.207. Viscusi WK, Cavallo GO. The effect of product safetyregulati<strong>on</strong> <strong>on</strong> safety precauti<strong>on</strong>s. Risk Analysis, 1994,14:917–930.208. Oldenburg BF, Brodie AM. Trends and challenges ininterventi<strong>on</strong> research methods. In: Doll LS et al., eds.Handbook of <strong>injury</strong> and violence preventi<strong>on</strong>. New York,NY, Springer, 2007:359–380.209. McClure R et al. Community-based programmes toprevent falls in <strong>child</strong>ren: a systematic review. Journal ofPaediatrics and Child Health, 2005, 41:465–470.210. Nort<strong>on</strong> R et al. Unintenti<strong>on</strong>al injuries. In: Jamis<strong>on</strong> DT etal., eds. Disease c<strong>on</strong>trol priorities in developing countries,2nd ed. New York, NY, Oxford University Press and the<str<strong>on</strong>g>World</str<strong>on</strong>g> Bank, 2006.211. Butchart A, Kruger J, Lekoba R. Percepti<strong>on</strong>s of <strong>injury</strong>causes and soluti<strong>on</strong>s in a Johannesburg township:implicati<strong>on</strong>s for preventi<strong>on</strong>. Social Science and Medicine,2000, 50:331–344.212. Forjuoh SN, Gyebi-Ofosu E. Injury surveillance: shouldit be a c<strong>on</strong>cern to developing countries? Journal of PublicHealth Policy, 1993, 14:355–359.213. Archib<strong>on</strong>g AE, Onuba O. Fractures in <strong>child</strong>ren in southeastern Nigeria. Central African Journal of Medicine, 1996,42:340–343.214. Peltzer K. Accidents/injuries of <strong>child</strong>ren in surgicaladmissi<strong>on</strong>s at the University Teaching Hospital in Lusaka,Zambia: a psycho-social perspective. Central AfricanJournal of Medicine, 1989, 35:319–322.215. Mas<strong>on</strong> M, Christoffel KK, Sinacore J. Reliability andvalidity of the <strong>injury</strong> preventi<strong>on</strong> project home safetysurvey. Archives of Pediatrics and Adolescent Medicine,2007, 161:759–765.WORLD REPORT ON CHILD INJURY PREVENTION 121
© Royal Children’s Hospital Foudati<strong>on</strong>P O I SONINGHARRISON’S STORYHarris<strong>on</strong> is the youngest of five<strong>child</strong>ren in an Australian family.One day, Lisa, his mother, changedher usual morning routine. Insteadof going directly to the kitchen,checking that the cupboarddoors were locked and preparingbreakfast, she put <strong>on</strong> a videofor Harris<strong>on</strong>’s older sister. Inthat brief period, 18-m<strong>on</strong>th-oldHarris<strong>on</strong> opened a cupboard,removed the cap from a c<strong>on</strong>tainerof dishwasher detergent andswallowed the powder.Lisa heard his cry and ran to the kitchen to fi nd him vomiting blood. An ambulancerushed Harris<strong>on</strong> to hospital where doctors were unsure if he would survive.The c<strong>on</strong>tainer Harris<strong>on</strong> had managed to open had a cap that looked like a <strong>child</strong>resistantclosure. To secure this closure, the cap had to click twice. Instructi<strong>on</strong>s tothis effect, though, were not displayed <strong>on</strong> the packaging and Lisa mistakenly thoughtthe c<strong>on</strong>tainer was securely closed when she felt the fi rst click.Harris<strong>on</strong> survived, but his injuries changed his life and the lives of his family. Lisapublicized his case, which was then actively taken up by the media. Harris<strong>on</strong>’sstory, and the details of other small <strong>child</strong>ren who had sustained similar injuries,became fi rst local and then nati<strong>on</strong>al news. While Australian laws stipulated thatall dishwasher gels and liquids with a pH value greater than 11.5 be supplied inc<strong>on</strong>tainers with <strong>child</strong>-resistant closures, with specifi c warnings as to the causticnature of the c<strong>on</strong>tents, powders were exempt from this regulati<strong>on</strong>. The powderswallowed by Harris<strong>on</strong> was extremely alkaline – with a pH of 13.4.The manufacturer of the dishwasher detergent was c<strong>on</strong>tacted. Faced with the evidence,the company placed warning labels <strong>on</strong> all its c<strong>on</strong>tainers informing c<strong>on</strong>sumers of the“double-click mechanism” to engage the <strong>child</strong>-resistant closure. The company thenredesigned the c<strong>on</strong>tainer itself, incorporating a device to limit the fl ow of powder andchanging the closure to a “single-click” mechanism. Unfortunately, this was <strong>on</strong>ly <strong>on</strong>eproduct of many <strong>on</strong> the supermarket shelves, leaving other manufacturers’ productsunchanged.Government agencies and n<strong>on</strong>governmental organizati<strong>on</strong>s lobbied for a change tothe law, which was eventually amended. Dishwasher powder must now be distributedin <strong>child</strong>-resistant c<strong>on</strong>tainers with specifi c warning labels if the pH exceeds 11.5.Furthermore, detergents with a pH greater than 12.5 have been removed fromthe domestic market. In additi<strong>on</strong>, the performance standard for the <strong>child</strong>-resistantclosure is also under review. The aim is to ensure that if a closure appears to be<strong>child</strong>-resistant, then it must functi<strong>on</strong> as such. There cannot be different stagesof functi<strong>on</strong>ality, such as the “single-click” and “double-click” stages that Lisa’sc<strong>on</strong>tainer incorporated.
CHAPTER 6 – POISONINGChapter 6Pois<strong>on</strong>ingIntroducti<strong>on</strong>“All things are pois<strong>on</strong> and nothing is without pois<strong>on</strong>, <strong>on</strong>ly thedose permits something not to be pois<strong>on</strong>ous” – Paracelsus(1).The home and its surroundings can be dangerousplaces for <strong>child</strong>ren, particularly for the possibility ofunintenti<strong>on</strong>al pois<strong>on</strong>ing. Children are naturally curious,exploring in and around the home. As a result, each yearmilli<strong>on</strong>s of calls are made to pois<strong>on</strong> c<strong>on</strong>trol centres (alsocalled pois<strong>on</strong> informati<strong>on</strong> centres). Thousands of <strong>child</strong>renare admitted to emergency departments because theyhave inadvertently c<strong>on</strong>sumed some type of householdproduct, medicine or pesticide. Most of these “accidental”pois<strong>on</strong>ings could have been prevented.This chapter focuses <strong>on</strong> cases of acute pois<strong>on</strong>ing am<strong>on</strong>g<strong>child</strong>ren – predominantly unintenti<strong>on</strong>al <strong>on</strong>es. It covers theextent and nature of pois<strong>on</strong>ings, the risk factors and theinterventi<strong>on</strong> measures that can be employed to preventpois<strong>on</strong>ings or to mitigate the c<strong>on</strong>sequences. The chapterdoes not deal with chr<strong>on</strong>ic pois<strong>on</strong>ing issues related to lead,with indoor air polluti<strong>on</strong> or with other effects of repeatedor prol<strong>on</strong>ged exposure to toxic agents. Also excluded areallergic reacti<strong>on</strong>s to food or pois<strong>on</strong>ing stemming frominfectious agents. The issue of snake bites, a major problemin some parts of the world, is addressed in the form of abox.“Pois<strong>on</strong>ing” refers to an <strong>injury</strong> that results frombeing exposed to an exogenous substance that causescellular <strong>injury</strong> or death. Pois<strong>on</strong>s can be inhaled, ingested,injected or absorbed. Pois<strong>on</strong>ing may also be acquiredin utero. The exposure may be acute or chr<strong>on</strong>ic and theclinical presentati<strong>on</strong> will vary accordingly. The factorsdetermining the severity of pois<strong>on</strong>ing and its outcome ina <strong>child</strong> are interrelated. They include:– the type of pois<strong>on</strong>;– the dose;– the formulati<strong>on</strong>;– the route of exposure;– the age of the <strong>child</strong>;– the presence of other pois<strong>on</strong>s;– the state of nutriti<strong>on</strong> of the <strong>child</strong>;– the presence of other diseases or injuries.The time interval between the exposure to pois<strong>on</strong> andthe appearance of clinical symptoms is an importantwindow of opportunity. During this period, it is importantto minimize absorpti<strong>on</strong> by removing or neutralizing thepois<strong>on</strong> (in the case of ingesti<strong>on</strong>), or to administer agents thatprevent damage to the organs – such as the use of N-acetylcysteine in cases of paracetamol pois<strong>on</strong>ing. The l<strong>on</strong>gerthe time interval, the greater is the chance of survival. Ingeneral, if pois<strong>on</strong>s are ingested in solid doses, which havea slower <strong>on</strong>set of absorpti<strong>on</strong>, more time is available forinterventi<strong>on</strong>s targeting the absorpti<strong>on</strong> process. For liquidpois<strong>on</strong>s, <strong>on</strong> the other hand, absorpti<strong>on</strong> is usually too rapidto be easily prevented.Pois<strong>on</strong>ing with specific agents produces clinicalsyndromes that are frequently recognizable. All thesame, the syndromes may be easily misdiagnosed or gounrecognized in a <strong>child</strong>. For this reas<strong>on</strong>, treatment may bedelayed, with serious c<strong>on</strong>sequences. Pois<strong>on</strong>ing is thereforebest prevented. Understanding the pattern of pois<strong>on</strong>ing ishelpful for reducing the risk of unintenti<strong>on</strong>al pois<strong>on</strong>ing, aswell as for preventing intenti<strong>on</strong>al pois<strong>on</strong>ing (2).Epidemiology of pois<strong>on</strong>ingAccording to the WHO Global Burden of Disease project,an estimated 345 814 people of all ages died worldwideas a result of “accidental” pois<strong>on</strong>ing in 2004. Althoughthe majority of these accidental pois<strong>on</strong>ings were am<strong>on</strong>gadults, 13% occurred am<strong>on</strong>g <strong>child</strong>ren and youngpeople under the age of 20 years (see Statistical Annex,Table A.1). Am<strong>on</strong>g 15–19-year-olds, pois<strong>on</strong>ing ranks asthe 13th leading cause of death (see Table 1.1). A survey of16 middle-income and high-income countries revealedthat, of the different external causes of unintenti<strong>on</strong>al<strong>injury</strong> death am<strong>on</strong>g <strong>child</strong>ren aged between 1 and 14 years,pois<strong>on</strong>ings ranked fourth in 2000–01, after road trafficcrashes, fires and drowning (3).MortalityAcute pois<strong>on</strong>ing accounted for an estimated 45 000 deathsannually in <strong>child</strong>ren and young people under the age of20 years (see Statistical Annex, Table A.1). The global deathrate from pois<strong>on</strong>ings for <strong>child</strong>ren younger than 20 years is1.8 per 100 000 populati<strong>on</strong>. For high-income countries therate is 0.5 per 100 000 while for low-income and middleincomecountries it is four times higher, at 2.0 per 100 000.The map in Figure 6.1 shows the geographic distributi<strong>on</strong> offatal unintenti<strong>on</strong>al pois<strong>on</strong>ing, by WHO regi<strong>on</strong>. Althoughmortality rates are generally low and do not exceed 4 per100 000 populati<strong>on</strong>, Africa, the low-income and middleincomecountries of Europe, and the Western Pacificregi<strong>on</strong> have the highest rates.In general, low-income and middle-income countrieshave higher pois<strong>on</strong>ing death rates than high-incomeWORLD REPORT ON CHILD INJURY PREVENTION 123
countries. The <strong>on</strong>e excepti<strong>on</strong> is in the high-incomecountries of the Americas, where death rates are higherthan in the middle-income and low-income countries,particularly in the 15–19-year age range (see StatisticalAnnex, Table A.1).Reported mortality data from countries show higherrates than the estimated regi<strong>on</strong>al averages, but the trendsare similar. For instance, in Sri Lanka, the case fatalityrate from pois<strong>on</strong>ing was found to be as high as 3.2% (4).In India, the <str<strong>on</strong>g>report</str<strong>on</strong>g>ed figures for fatal pois<strong>on</strong>ings rangedbetween 0.6% and 11.6%, while in Viet Nam the <str<strong>on</strong>g>report</str<strong>on</strong>g>edcase fatality rate was 3.3% (5, 6).AgeChildren under the age of <strong>on</strong>e year have the highest ratesof fatal pois<strong>on</strong>ing (see Figure 6.2), particularly those inlow-income and middle-income countries. Generally,mortality rates are highest in infants and decrease withage until 14 years. After that, there is an increase again,almost everywhere, in <strong>child</strong>ren 15 years of age and older.In many settings, this increase may be due to substanceuse, or to unintenti<strong>on</strong>al or undetermined drug overdoses(7). In some places, the increase may be as a result ofentry into the workplace, with its increased exposure torisks.FIGURE 6.2Fatal pois<strong>on</strong>ing rates per 100 000 <strong>child</strong>ren by age and sex, <str<strong>on</strong>g>World</str<strong>on</strong>g>,2004Rate per 100 000 populati<strong>on</strong>6420Source: WHO (2008), Global Burden of Disease: 2004 update.BoysGirlsUnder 1 1–4 5–9 10–14 15–19 Under 20Age (years)GenderBoys have higher rates than girls in all regi<strong>on</strong>s of the worldexcept the low-income and middle-income countries ofthe Western Pacific regi<strong>on</strong> (see Table 6.1). The pois<strong>on</strong>ingrate for boys in the WHO African regi<strong>on</strong> is 5 per 100 000populati<strong>on</strong>, while for girls in the high-income countriesFIGURE 6.1Mortality rates due to pois<strong>on</strong>ing per 100 000 <strong>child</strong>ren a by WHO regi<strong>on</strong> and country income level, 20043+1.0–2.90.5–1.0
of the Eastern Mediterranean and Western Pacific regi<strong>on</strong>sthe rate is as low as 0.1 per 100 000 populati<strong>on</strong>.MorbidityIn c<strong>on</strong>trast to data <strong>on</strong> mortality, global data <strong>on</strong> n<strong>on</strong>-fataloutcomes of pois<strong>on</strong>ing are not readily available. Data atcountry level, though, usually obtained through pois<strong>on</strong>c<strong>on</strong>trol centres, specialized surveillance systems (suchas the Nati<strong>on</strong>al Pois<strong>on</strong> Data System in the United States)or the general <strong>injury</strong> surveillance systems that exist inmany countries, are available. Unfortunately, much ofthe country informati<strong>on</strong> is from high-income countries.Some low-income and middle-income countries, though,including South Africa and Sri Lanka, have establishedpois<strong>on</strong> c<strong>on</strong>trol centres and begun to c<strong>on</strong>duct research <strong>on</strong>pois<strong>on</strong>ings.One difficulty when comparing pois<strong>on</strong>ing incidencerates between countries is the variety of classificati<strong>on</strong>systems used.In Sweden, the annual rate of enquiries to the pois<strong>on</strong>c<strong>on</strong>trol centre c<strong>on</strong>cerning n<strong>on</strong>-pharmaceuticalchemicals – a category that could include natural toxins,or recreati<strong>on</strong>al drugs – was about 1400 per 100 000<strong>child</strong>ren aged between 0 and 9 years (8).In Japan, the pois<strong>on</strong> centre received 31 510 enquiriesin 1995 about pois<strong>on</strong>ing in <strong>child</strong>ren under 6 years ofage. The product most frequently involved was tobacco(20%). Enquiries relating to <strong>child</strong>ren less than 1 year oldmade up 35.7% of these cases (9).Data from 2006 from the American Associati<strong>on</strong> ofPois<strong>on</strong> C<strong>on</strong>trol Centers showed that the most comm<strong>on</strong>pois<strong>on</strong>ings am<strong>on</strong>g <strong>child</strong>ren were due to pharmaceuticalproducts. Enquiries relating to <strong>child</strong>ren less than6 years old made up 50.9% of cases and 2.4% of the total<str<strong>on</strong>g>report</str<strong>on</strong>g>ed fatalities (10).In the United States in 2004, there were over 1.25 milli<strong>on</strong>pois<strong>on</strong> exposures involving <strong>child</strong>ren less than 6 years ofage – 425 per 100 000 <strong>child</strong>ren – <str<strong>on</strong>g>report</str<strong>on</strong>g>ed to the ToxicExposure Surveillance System (11). The substancesmost frequently involved were cosmetics and pers<strong>on</strong>alcare products, cleaning substances and analgesics.Data from published hospital admissi<strong>on</strong>s are availablefor pois<strong>on</strong>ings in a number of high-income countries.Comparability is a problem here again, since admissi<strong>on</strong>criteria differ between countries and between urbanand rural settings. Child pois<strong>on</strong>ing admissi<strong>on</strong> rates inAustralia have been c<strong>on</strong>sistently higher in rural areas thanurban areas over a number of years. This is probably due tothe fact that <strong>child</strong>ren are more readily admitted to hospitalin rural areas, as doctors in these areas may err <strong>on</strong> the sideof cauti<strong>on</strong> and refer <strong>child</strong>ren to hospital even when thisis unnecessary. The actual agents involved, though, varylittle between urban and rural cases (12).Hospital discharge data are a better indicator ofmorbidity, since they include a c<strong>on</strong>firmed diagnosis. Atwo-year study based <strong>on</strong> hospital discharges and deathcertificates in California, United States, showed that<strong>child</strong>ren aged 15–17 m<strong>on</strong>ths had the highest overall <strong>injury</strong>rate and that pois<strong>on</strong>ing was the sec<strong>on</strong>d leading cause of<strong>injury</strong> in this group. More than two thirds of the casesinvolved the ingesti<strong>on</strong> of medicines (13).Although pois<strong>on</strong>ing death rates are highest in infantsunder 12 m<strong>on</strong>ths of age, the incidence of pois<strong>on</strong>ingcases – as reflected in calls to pois<strong>on</strong> c<strong>on</strong>trol centres andemergency department visits – is generally higher in otherage groups (14, 15). N<strong>on</strong>-fatal pois<strong>on</strong>ing, in fact, appearsto be more comm<strong>on</strong> am<strong>on</strong>g <strong>child</strong>ren aged 1 to 4 years (9).In a recent hospital-based study in four low-income andmiddle-income countries, <strong>on</strong>ly 2% of pois<strong>on</strong>ings occurredin <strong>child</strong>ren under 1 year of age, compared with 54% in the1–4-year age group (16).The fatality rate am<strong>on</strong>g older <strong>child</strong>ren admitted tohospital following an accidental pois<strong>on</strong>ing is generally lessthan 1% (4, 17). The higher mortality rate in very younginfants may be explained by the greater susceptibility ofthe infant body to damage by toxins.Types of pois<strong>on</strong>The prevalence and types of pois<strong>on</strong>ing vary c<strong>on</strong>siderablyacross the world and depend <strong>on</strong> socioec<strong>on</strong>omic statusand cultural practices, as well as <strong>on</strong> local industrial andagricultural activities.TABLE 6.1Mortality rates due to pois<strong>on</strong>ing per 100 000 <strong>child</strong>ren a by sex, country income level and WHO regi<strong>on</strong>, 2004Africa Americas South- East Asia Europe Eastern Mediterranean Western PacificLMIC HIC LMIC LMIC HIC LMIC HIC LMIC HIC LMICBoys 4.9 1.2 0.4 1.7 0.3 2.4 1.3 1.7 0.1 1.5Girls 3.0 0.4 0.3 1.6 0.2 1.7 0.0 1.5 0.1 2.1aThese data refer to those under 20 years of age.HIC = High-income countries; LMIC = low-income and middle-income countries.Source: WHO (2008), Global Burden of Disease: 2004 update.WORLD REPORT ON CHILD INJURY PREVENTION 125
Data from pois<strong>on</strong> c<strong>on</strong>trol centres and hospitals (4, 5,18 –24) indicate that the most comm<strong>on</strong> agents involvedin developed countries – as well as in some developingcountries – are:– medicines sold over the counter, such as paracetamol,cough and cold remedies, ir<strong>on</strong> tablets, antihistaminesand anti-inflammatory drugs;– prescripti<strong>on</strong> medicines, such as antidepressants,narcotics and analgesics;– recreati<strong>on</strong>al drugs, such as cannabis and cocaine;– household products – such as bleach, disinfectants,detergents, cleaning agents, cosmetics and vinegar;– pesticides – including insecticides, rodenticides andherbicides;– pois<strong>on</strong>ous plants;– animal or insect bites.The most comm<strong>on</strong> agents involved in <strong>child</strong>hoodpois<strong>on</strong>ings in low-income and middle-income countriesare hydrocarb<strong>on</strong>s used for fuel and lighting, such asparaffin oil (also known in some countries as kerosene)(5, 25–31).A study c<strong>on</strong>ducted in Bangladesh, Colombia, Egyptand Pakistan showed that medicati<strong>on</strong>s were resp<strong>on</strong>siblefor 31% of pois<strong>on</strong>ings in <strong>child</strong>ren under 12 years of age,followed by cleaning agents, which accounted for 20%(16).Older <strong>child</strong>ren may be employed in the informallabour sector, in extractive metal industries that involveprocessing with toxic chemicals, or in agriculture,where pesticides are used. Children living in povertymay scavenge in dump sites c<strong>on</strong>taining toxic waste. Inall these cases, there is a str<strong>on</strong>g likelihood of exposureto toxic substances, including lead, mercury andorganophosphates (32). Other <strong>child</strong>ren in the family,not directly involved in these activities, may come intoc<strong>on</strong>tact with toxins brought into the home <strong>on</strong> the clothesor shoes of their siblings. Children may also be exposedto toxins leached into water or sprayed in the air.MedicinesMedicinal drugs are the leading cause of n<strong>on</strong>-fatalpois<strong>on</strong>ing in <strong>child</strong>ren in middle-income and high-incomecountries.A hospital-based study from United Arab Emiratesfound that 55% of <strong>child</strong>hood pois<strong>on</strong>ings were due tomedicines. Analgesics, n<strong>on</strong>-steroidal anti-inflammatorydrugs and antihistamines were the most comm<strong>on</strong>lyingested drugs in <strong>child</strong>ren in the 1–5-year age group(21).A study from Turkey <str<strong>on</strong>g>report</str<strong>on</strong>g>ed that accidental ingesti<strong>on</strong>of drugs was most comm<strong>on</strong> (57.7%) in <strong>child</strong>ren agedbetween 1 and 5 years and that the most frequentoffending agent was analgesics (33).In the United States, in 2003, some 570 000pharmaceutical exposures were <str<strong>on</strong>g>report</str<strong>on</strong>g>ed in <strong>child</strong>renless than 6 years old (34). This figure represented 23.8%of all pois<strong>on</strong>ing <str<strong>on</strong>g>report</str<strong>on</strong>g>s, with analgesics accountingfor almost 100 000 cases. Additi<strong>on</strong>ally, more than50 000 <strong>child</strong>ren under the age of 5 years were treatedin emergency rooms for an unintenti<strong>on</strong>al exposure tomedicinal drugs. Prescripti<strong>on</strong> medicines were morecomm<strong>on</strong>ly implicated than over-the-counter drugs(34).In England and Wales, during the period 1968–2000,medicati<strong>on</strong>s accounted for 12.8% of unintenti<strong>on</strong>alpois<strong>on</strong>ing deaths in <strong>child</strong>ren aged less than 10 years(23).Organic fuels and solventsIngesti<strong>on</strong> of hydrocarb<strong>on</strong> fuel used for cooking, heatingor lighting is a comm<strong>on</strong> cause of <strong>child</strong>hood pois<strong>on</strong>ing inlow-income countries (25–29). Paraffin oil is the leadingcause of <strong>child</strong>hood pois<strong>on</strong>ings in many countries, whereit may account for up to 16% of all paediatric pois<strong>on</strong>ings,mainly in <strong>child</strong>ren aged between 1 and 3 years (2, 16, 30,31, 35–38).Organic solvents (such as paint remover, glue andacet<strong>on</strong>e), as wel l as d iet hylene g lycol (a comp<strong>on</strong>ent of a nt i-freeze), have also been implicated in mass unintenti<strong>on</strong>alpois<strong>on</strong>ings of <strong>child</strong>ren through c<strong>on</strong>taminated medicinesor toiletries. In 1998, 109 <strong>child</strong>ren in Haiti fell ill afterc<strong>on</strong>suming paracetamol (known as acetaminophenin the United States) c<strong>on</strong>taminated with diethyleneglycol, and 85 of them died (39). In similar incidents inBangladesh, India, Nigeria and Panama, <strong>child</strong>ren werepois<strong>on</strong>ed as a result of poorly regulated manufacturingprocesses (39).In additi<strong>on</strong> to the unintenti<strong>on</strong>al ingesti<strong>on</strong> of organicfuels and solvents, intenti<strong>on</strong>al inhalati<strong>on</strong> of volatilesubstances (such as “glue sniffing”) by adolescents canresult in sudden cardiac death, since inhaled hydrocarb<strong>on</strong>sare about 140 times more toxic than when ingested (40).PesticidesChildren living in agricultural communities are at riskof acute pesticide pois<strong>on</strong>ing. In the Central Americanregi<strong>on</strong>, in 2000, about 12% of all acute pesticide pois<strong>on</strong>ingoccurred in <strong>child</strong>ren less than 15 years of age, with anincidence rate of 5.7 per 100 000 populati<strong>on</strong> (41). In poorcommunities, where there is often little separati<strong>on</strong> betweenwork and the home, <strong>child</strong>ren may be exposed to pesticideresidues present in work clothes, in the air from sprayingand in household dust (42). In Nicaragua, <strong>child</strong>ren livingnear cott<strong>on</strong> farms have been found to suffer pois<strong>on</strong>ingfrom organophosphates (43).Some of the factors c<strong>on</strong>tributing to fatal foodpois<strong>on</strong>ings are the inappropriate use and storage ofpesticides; the handling of food, while or after working,without proper washing of hands; and the unsafe disposalor reuse of pesticide c<strong>on</strong>tainers. An example was the food126 WORLD REPORT ON CHILD INJURY PREVENTION
c<strong>on</strong>taminated with thallium, a rodent pois<strong>on</strong>, that waseaten by <strong>child</strong>ren in the Peruvian Andes in 1999, causing24 deaths (44).In additi<strong>on</strong> to these types of indirect exposureto pesticides, there are direct exposures. A study inChina found that <strong>child</strong>ren had been exposed directlyto rodenticides used in and around the home (45). TheInternati<strong>on</strong>al Labour Organizati<strong>on</strong> estimates that thereare approximately 250 milli<strong>on</strong> working <strong>child</strong>ren betweenthe ages of 5 and 14 years and that some 40% of these areexposed to toxic substances in the rural areas of developingcountries (42).Household chemicalsChemicals around the house to which <strong>child</strong>ren mayhave access c<strong>on</strong>tribute significantly to unintenti<strong>on</strong>alpois<strong>on</strong>ings in <strong>child</strong>hood. In the United States in 2004,am<strong>on</strong>g <strong>child</strong>ren less than 6 years of age, there were over120 000 exposures to household cleaning agents, such asamm<strong>on</strong>ia, bleach and laundry detergents (11). While mostexposures to cleaning agents result in mild pois<strong>on</strong>ing,bleach, dishwasher detergents and amm<strong>on</strong>ia can leadto severe tissue damage. These agents are found in mosthouseholds in developed countries. Several other studieshave c<strong>on</strong>firmed the existence of similar household agentsin <strong>child</strong>hood exposures to toxic substances (3, 21, 22, 46).Carb<strong>on</strong> m<strong>on</strong>oxideIn the United States, some 1600 <strong>child</strong>ren under 5 years of ageare treated in emergency departments each year and 10 die asa result of unintenti<strong>on</strong>al n<strong>on</strong>-fire-related exposure to carb<strong>on</strong>m<strong>on</strong>oxide. This type of pois<strong>on</strong>ing am<strong>on</strong>g <strong>child</strong>ren mostcomm<strong>on</strong>ly occurs from furnaces, motor vehicles, stoves, gaspipes and generators (47). In low-income countries, indoorcooking fires in homes with poor ventilati<strong>on</strong> can lead tocarb<strong>on</strong> m<strong>on</strong>oxide being produced as a result of incompletecombusti<strong>on</strong>. This in turn can result in respiratory diseasein <strong>child</strong>ren – from l<strong>on</strong>g-term exposure, rather than acutetoxicity (32, 33, 48).Other substancesInorganic substances – including arsenic and the heavymetals lead, copper and mercury – are also resp<strong>on</strong>sible forsome <strong>child</strong>hood pois<strong>on</strong>ings. The majority of pois<strong>on</strong>ingsdue to heavy metals and other inorganic substances are theresult of chr<strong>on</strong>ic exposure and are therefore excluded fromthis discussi<strong>on</strong>. In rare instances, though, acute exposureto these agents can result in pois<strong>on</strong>ings. As an example,acute lead encephalopathy with an 11% rate of mortalitywas <str<strong>on</strong>g>report</str<strong>on</strong>g>ed in Oman, after a lead-c<strong>on</strong>taining localmedicati<strong>on</strong> was given by parents to young infants (49).Plant toxin pois<strong>on</strong>ing – involving plants such as ackee,oleander, datura and cassava – is less frequently <str<strong>on</strong>g>report</str<strong>on</strong>g>ed.Such pois<strong>on</strong>ing can cause morbidity. Death from ingestingplant toxins, though, is rare. Two excepti<strong>on</strong>s are thetragedy in Haiti in 2001, in which 65 <strong>child</strong>ren died aftereating unripe ackee fruit (50); and the c<strong>on</strong>sumpti<strong>on</strong> ofC. occidentalis beans, the cause of recurrent outbreaks ofencephalopathy am<strong>on</strong>g young <strong>child</strong>ren in western UttarPradesh, India (51).Animal envenomati<strong>on</strong>s (pois<strong>on</strong>ing from bites or stings)from snakes (see Box 6.1), scorpi<strong>on</strong>s and spiders are arelatively comm<strong>on</strong> form of <strong>child</strong> pois<strong>on</strong>ing in certain areasof the world. These include parts of Asia, the Pacific andSouth America, and the desert areas of North Africa, WestAsia and North America. Envenomati<strong>on</strong>s, for instance, inSaudi Arabia account for as much as 30% of all pois<strong>on</strong>ingsam<strong>on</strong>g <strong>child</strong>ren aged 6–12 years (22, 52, 53).Cost of pois<strong>on</strong>ing-related <strong>injury</strong>Few studies have been d<strong>on</strong>e <strong>on</strong> the cost of pois<strong>on</strong>ings,especially those affecting <strong>child</strong>ren or those occurringin low-income or middle-income countries. One studyc<strong>on</strong>ducted in South Africa estimated that the direct costsal<strong>on</strong>e of hospitalizati<strong>on</strong> due to paraffin pois<strong>on</strong>ing wereat least US$ 1.4 milli<strong>on</strong> per year (54). The average cost oftreatment per patient amounted to US$ 106.50 in urbanPretoria (36) and approximately US$ 75.58 in the CapePeninsula (55).Data from the United States c<strong>on</strong>firm the South Africanfindings that pois<strong>on</strong>ings and their management are costly(56). Figures from 2000 show that, in <strong>child</strong>ren under15 years of age, there were a total of 219 000 pois<strong>on</strong>ings,of which 141 were fatal and 14 000 resulted in hospitalstays. The lifetime cost of pois<strong>on</strong>ings in <strong>child</strong>ren in thisage group was almost US$ 400 milli<strong>on</strong>, with medicaltreatment accounting for nearly 9% of the costs. Thisproduces a c<strong>on</strong>servative estimate of US$ 1780, <strong>on</strong> average,for each case of pois<strong>on</strong>ing – including medical costs, lostearnings and lost quality of life (57).Limitati<strong>on</strong>s of dataThe epidemiology of pois<strong>on</strong>ing can be studied fromhospital admissi<strong>on</strong>s and discharge records, mortality data,emergency department records and surveillance systems,as well as from enquiries to pois<strong>on</strong> c<strong>on</strong>trol centres. Globally,though, data <strong>on</strong> the type of toxic agents that result in<strong>child</strong> pois<strong>on</strong>ing and death are limited. There is substantialunder-recording and under-<str<strong>on</strong>g>report</str<strong>on</strong>g>ing of <strong>child</strong>hoodpois<strong>on</strong>ing incidents. In additi<strong>on</strong>, pois<strong>on</strong>ing is not generallya notifiable c<strong>on</strong>diti<strong>on</strong>, so few countries maintain recordsof pois<strong>on</strong>ings. Even where surveillance systems exist, <strong>child</strong>pois<strong>on</strong>ing cases are not necessarily <str<strong>on</strong>g>report</str<strong>on</strong>g>ed or counted.Cases may escape detecti<strong>on</strong>, especially if those affected d<strong>on</strong>ot seek treatment in a health-care facility. Furthermore,pois<strong>on</strong>ing in <strong>child</strong>ren may be attributed to the wr<strong>on</strong>gcause if the effects are similar to those of other c<strong>on</strong>diti<strong>on</strong>s.Even where pois<strong>on</strong>ing is correctly diagnosed, the healthcareworker or caregiver may not recognize the toxic agentthat is resp<strong>on</strong>sible.WORLD REPORT ON CHILD INJURY PREVENTION 127
BOX 6.1SnakebitesSnakebite is an eminently treatable, but neglected, <strong>injury</strong> affecting predominantly tropical developing countries. As is also the case with dog bites,recent improvements in <strong>injury</strong> coding and surveillance, including community surveys in low-income and middle-income countries, have led to anincreased understanding of the issue.How great is the problem of snakebite?The annual number of cases of snakebite worldwide is about 5 milli<strong>on</strong>, am<strong>on</strong>g which there are some 100 000 to 200 000 deaths (53, 59). Inadditi<strong>on</strong> to the deaths, there are an estimated 400 000 snakebite-related amputati<strong>on</strong>s each year around the world (60). Children have both higherincidence rates and suffer more severe effects than do adults, as a result of their smaller body mass (61, 62). Snakebites are c<strong>on</strong>centrated in mainlyrural areas and vary c<strong>on</strong>siderably by seas<strong>on</strong>, with the peak incidence seen in the rainy and harvesting seas<strong>on</strong>s (63).Analysis of 2002 WHO mortality data suggests that snakebite c<strong>on</strong>tributes to 35% of all <strong>child</strong> deaths, globally, from venomous bites and stings,with boys about twice as likely to suffer as girls (64). Boys appear to have a higher risk, from a very early age, of more severe, upper limb bites (65).This type of <strong>injury</strong> is c<strong>on</strong>siderably more comm<strong>on</strong> in low-income and middle-income countries, largely in Asia (53, 59).Unfortunately, although the specific antidotes for snakebites – antivenoms – are organic products, there is a worldwide shortage of this pharmaceutical(59). This has a severe impact <strong>on</strong> poor rural communities, who cannot afford the refined antivenoms used in high-income countries. As ac<strong>on</strong>sequence, many developing countries are driven to making crude sera that are both less safe and less effective. At the same time, those most atrisk of snakebite, such as rice farmers and plantati<strong>on</strong> workers and their families, are frequently far from medical care.There are a number of snakebite studies in the published literature, but few <str<strong>on</strong>g>report</str<strong>on</strong>g> specifically <strong>on</strong> the impact <strong>on</strong> <strong>child</strong>ren – although fatality ratesam<strong>on</strong>g <strong>child</strong>ren are generally higher (63). Furthermore, less than 10% of countries in WHO’s South-East Asia Regi<strong>on</strong>, an area of high snakebite incidence,<str<strong>on</strong>g>report</str<strong>on</strong>g> paediatric snakebite mortality data. N<strong>on</strong>etheless, the recent community health and <strong>injury</strong> surveys in Asia show that snakebite-related<strong>injury</strong> ranks as a leading cause of <strong>child</strong>hood morbidity and mortality in this regi<strong>on</strong> (66).Papua New Guinea has some of the highestsnakebite rates in the world, with the country’s ruralcentral province recording an annual incidenceof 561.9 cases per 100 000 populati<strong>on</strong> (63). Am<strong>on</strong>gpaediatric snakebites treated at Port MoresbyHospital Intensive Care Unit, the fatality rate for2003–2004 was 25.9%, compared to 14.5% foradults. Children also represent 36% of all snakebiterelatedventilator bed-days in an intensive care unit,in which snakebite-related paralysis accounts for60% of the ventilator bed-days (63).Data from developed countries, <strong>on</strong> the otherhand, reveal much lower snakebite-related <strong>injury</strong>and very low mortality rates. In Australia, 1512 snakebite hospitalizati<strong>on</strong>s wererecorded between 2000 and 2002, resulting in acrude annual rate of 3.9 per 100 000 populati<strong>on</strong>. Thehighest rates – of 7.5 per 100 000 – were am<strong>on</strong>g boysaged 10–14 years (61). In the United States during the period 2001–2004,the estimated crude rate of snakebite presentati<strong>on</strong>s toemergency departments was 3.4 per 100 000 populati<strong>on</strong>,with an overall admissi<strong>on</strong> rate of 31%. The crudepresentati<strong>on</strong> rate was highest am<strong>on</strong>g <strong>child</strong>ren aged10–14 years, at 5.5 per 100 000 populati<strong>on</strong> (62).© DA Warrell, Oxford UniversityWhat can be d<strong>on</strong>e about snakebites?Few studies have comprehensively examined thisquesti<strong>on</strong> for adults, and even fewer have looked atpaediatric snakebite. The evidence is therefore somewhatanecdotal. Nevertheless, several generalpoints can be made about why <strong>child</strong>ren are at particularlyhigh risk of snakebite (67). Natural curiosity leads <strong>child</strong>ren to interact withanimals in general, and in particular leads boys tointeract with snakes.128 WORLD REPORT ON CHILD INJURY PREVENTION
In rural areas in developing countries, <strong>child</strong>ren are often employed <strong>on</strong> the farm, thus incurring an increased risk of making c<strong>on</strong>tact withsnakes. Children’s small body weight meansthat a snakebite is likely to have arelatively great impact.Hence <strong>child</strong>ren, especially boys, shouldbe specifically targeted for snakebitepreventi<strong>on</strong> educati<strong>on</strong>al initiatives.The primary avoidance of snakebiterelies <strong>on</strong> minimizing <strong>child</strong>ren’s interacti<strong>on</strong>with snakes. Approaches hereinclude:– wearing appropriate protective clothing– such as shoes or boots – particularlyat night and in rural areas;– avoiding dem<strong>on</strong>izing snakes, asdeliberate aggressiveness towardsthem is more likely to result in a snakebite;– keeping sheds and fodder storageareas clear of mice and rats, as theseattract snakes;– keeping grassy areas well cut.Regarding sec<strong>on</strong>dary preventi<strong>on</strong>,two recommendati<strong>on</strong>s should be made. Compartment syndrome – where excessive pressure impairs blood supply, leading to possible nerve damage and muscle death – is often associatedwith tourniquet use following a snakebite, and is the most comm<strong>on</strong> reas<strong>on</strong> for amputati<strong>on</strong> in <strong>child</strong>ren in many areas of Africa. The useof tourniquets as first aid following snakebite should therefore be discouraged, and vigilance maintained against pressure-induced cell death(68). Traditi<strong>on</strong>al healers, who often initially treat snakebite, should be specifically targeted so that modern principles of medical care can be incorporatedinto their traditi<strong>on</strong>al methods. This can help avoid delays before treatment can be given in a health-care facility, and thus minimize thefrequent serious harm that results from late treatment of snakebite.Snakebite is a widespread and previously poorly-documented global <strong>injury</strong> problem, in which <strong>child</strong>ren and young people are disproporti<strong>on</strong>atelyrepresented. Low-income and middle-income countries, particularly the rural areas, are the most affected. Most deaths and serious c<strong>on</strong>sequencesfrom snakebites are entirely preventable by existing means, including making antivenom much more widely available. Better surveillance and<str<strong>on</strong>g>report</str<strong>on</strong>g>ing are necessary to assess the extent of this forgotten <strong>injury</strong> and to improve preventi<strong>on</strong> strategies.© D Williams, Australian Venom Research UnitData <strong>on</strong> <strong>child</strong> pois<strong>on</strong>ings are further affected by problemswith coding. The use of the Internati<strong>on</strong>al Classificati<strong>on</strong> ofDisease coding of external causes of death, for example,does not capture sufficient detail <strong>on</strong> the agent involved (58).In additi<strong>on</strong>, there is frequently insufficient informati<strong>on</strong> <strong>on</strong>which to make a determinati<strong>on</strong> of intent, with the result thatmany pois<strong>on</strong>ing cases are classified as being of undeterminedintent. Accurate informati<strong>on</strong> regarding intent is vital forpreventi<strong>on</strong> strategies. Studies show that pois<strong>on</strong>ings of<strong>child</strong>ren up to the age of 10 years tend to be unintenti<strong>on</strong>al,while those of adolescents tend to be intenti<strong>on</strong>al in termsof deliberate c<strong>on</strong>sumpti<strong>on</strong> of the agent, but not necessarilywith the intent to cause <strong>injury</strong> (7).Risk factorsAs with other injuries, the risk of a <strong>child</strong> being pois<strong>on</strong>edis affected by factors related to the <strong>child</strong>, the agent and theenvir<strong>on</strong>ment. These factors are interrelated and are highlydependent <strong>on</strong> the c<strong>on</strong>text (see Table 6.2). An understandingof these factors is important for the development ofinterventi<strong>on</strong>s to prevent and, where necessary, treat casesof <strong>child</strong> pois<strong>on</strong>ing.Child-related factorsAgeAge has a str<strong>on</strong>g associati<strong>on</strong> with pois<strong>on</strong>ing as itdetermines the behaviour, size and physiology of the<strong>child</strong>, thus influencing types of exposure and outcome(69). Infants and small <strong>child</strong>ren are closer to the groundthan older <strong>child</strong>ren and tend to put their hands and smallobjects into their mouths. As a result they are at increasedrisk of exposure to toxins found at low levels or in thesoil or dust – such as rodenticides. Many studies havec<strong>on</strong>firmed that pois<strong>on</strong>ing rates increase dramatically ataround 2 years of age, as young <strong>child</strong>ren become moremobile and have increased access to toxins (16). Young<strong>child</strong>ren are particularly susceptible to the unintenti<strong>on</strong>alWORLD REPORT ON CHILD INJURY PREVENTION 129
TABLE 6.2Hadd<strong>on</strong> Matrix applied to the risk factors for <strong>child</strong>hood pois<strong>on</strong>ingPre-eventEventPost-eventChild Agent Physical envir<strong>on</strong>ment Socioec<strong>on</strong>omic envir<strong>on</strong>mentAge and developmental factors(such as curiosity, judgement);gender; parental supervisi<strong>on</strong>.Child’s secrecy about ingesti<strong>on</strong>;parent not noticing unusualbehaviour.Child’s inability to communicateincident; lack of access to pois<strong>on</strong>c<strong>on</strong>trol centre.Ease of opening package;attractiveness of substance;inadequate labelling; poorstorage.Toxicity of chemical; dosec<strong>on</strong>sumed; ease with whichsubstance can be c<strong>on</strong>sumed(for instance, as liquidrather than solid).Chemical agent without anantidote.Cupboards within easyreach of <strong>child</strong>ren; absence oflocking devices <strong>on</strong> cabinets;exposure to agents.Places where <strong>child</strong> caningest substances withoutbeing seen.Lack of adequate prehospitalcare, acute care andrehabilitati<strong>on</strong>.Lack of regulati<strong>on</strong>s and standardsfor toxic products and packaging;poverty; lack of awareness oftoxicity and pois<strong>on</strong>ing risks am<strong>on</strong>gcaregivers.Lack of awareness by caregivers ofhow to react; lack of appropriate andtimely dec<strong>on</strong>taminati<strong>on</strong> by healthcareworkers.No pois<strong>on</strong> c<strong>on</strong>trol centre or lackof informati<strong>on</strong> <strong>on</strong> how to c<strong>on</strong>tactcentre; lack of access to emergencymedical care.ingesti<strong>on</strong> of pois<strong>on</strong>s, especially liquid <strong>on</strong>es (70). The risk ofpois<strong>on</strong>ing am<strong>on</strong>g young <strong>child</strong>ren is exacerbated by theirsize and physiological development. Most substancesincrease in toxicity as the dose increases relative to bodymass. Some toxins are eliminated by enzyme systems inthe body that develop as the <strong>child</strong> grows older.In adolescents, where pois<strong>on</strong>ing can be caused byalcohol misuse or the use of other recreati<strong>on</strong>al drugs,fatality rates are higher than in younger <strong>child</strong>ren (71).GenderBoys appear to be at c<strong>on</strong>sistently higher risk of pois<strong>on</strong>ingthan girls (4, 36, 72). With specific regard to pois<strong>on</strong>ingfrom the ingesti<strong>on</strong> of paraffin, though, some studieshave shown no difference between boys and girls, whileothers have shown a prep<strong>on</strong>derance am<strong>on</strong>g boys (25, 28,37). The discrepancy in these findings may be explainedby gender differences in socializati<strong>on</strong> between differentcountries. In some cultures, girls are expected not toengage in outdoor activities or to adopt risk-takingbehaviours (27).PovertySocioec<strong>on</strong>omic status is str<strong>on</strong>gly associated with <strong>injury</strong>and deaths from pois<strong>on</strong>ing, not <strong>on</strong>ly between countriesbut also within countries (73). Studies from the UnitedKingdom show that the risk of dying from pois<strong>on</strong>ingam<strong>on</strong>g <strong>child</strong>ren from poor backgrounds is more thanthree times higher than the risk for <strong>child</strong>ren in affluentareas (74). One study in Greece, however, showed noassociati<strong>on</strong> between social and demographic factorsand <strong>child</strong> pois<strong>on</strong>ings (75). N<strong>on</strong>etheless, socioec<strong>on</strong>omicstatus may well be the str<strong>on</strong>gest risk factor for pois<strong>on</strong>ingsin <strong>child</strong>ren as it affects exposure, is itself associatedwith several other risk factors (such as physicalunderdevelopment in <strong>child</strong>ren) and is linked to pooroutcomes of <strong>injury</strong>.In developing countries, socioec<strong>on</strong>omic status is astr<strong>on</strong>g predictor for household fuel c<strong>on</strong>sumpti<strong>on</strong>, itselflinked to an increased exposure to paraffin. At the sametime, poverty drives <strong>child</strong>ren into work that is usuallypoorly paid but with high risks of <strong>injury</strong>. Poor people tendto live with inadequate sanitary facilities – for washing,and sewerage and waste disposal – and limited storagespace to keep harmful substances away from <strong>child</strong>ren.Poor dwellings are more likely to be close to areas sprayedwith pesticides or to toxic dumps, or to draw their waterfrom c<strong>on</strong>taminated sources. Poverty and malnutriti<strong>on</strong> canalso place <strong>child</strong>ren at risk of pois<strong>on</strong>ing by forcing themto c<strong>on</strong>sume unsafe but cheaply obtained foods – such asundercooked cassava or unripe ackee fruit, both of whichare toxic.The ability to withstand toxic effects depends, am<strong>on</strong>gother factors, <strong>on</strong> the nutriti<strong>on</strong>al and health status of the<strong>child</strong>. Children living in poverty are generally inadequatelynourished and therefore more vulnerable to pois<strong>on</strong>s thantheir healthier counterparts. In additi<strong>on</strong>, c<strong>on</strong>diti<strong>on</strong>s ofpoverty frequently prevent people from accessing healthcare.Agent factorsCharacteristics of the agentThe more c<strong>on</strong>centrated or more potent the toxic agent,the greater the risk of severe morbidity and mortality.Chemical analyses of seven samples of paraffin from SouthAfrican refineries found significant differences in theirlevels of toxicity (76).The nature of the substance is also important. Thereis a higher incidence of <strong>injury</strong> associated with liquidagents than with solid compounds (69). Households130 WORLD REPORT ON CHILD INJURY PREVENTION
with <strong>child</strong>ren are more likely to have liquid medicati<strong>on</strong>s.Liquid preparati<strong>on</strong>s are easier to swallow than powderedpreparati<strong>on</strong>s, such as dishwasher detergents or tablets,because they do not stick to the mucosa of the mouth.Nor do they usually produce a burning sensati<strong>on</strong> (whichpowdered preparati<strong>on</strong>s do) which would limit the amountc<strong>on</strong>sumed. Unfortunately, powdered chemicals are nowbeing produced with an anti-caking agent, which increasesthe ease of flow of the powdered chemical, but which alsomakes ingesti<strong>on</strong> easier.The physical appearance of a toxic substance playsa large part in its attractiveness to <strong>child</strong>ren, while itschemical compositi<strong>on</strong> determines its effect. Features suchas size, colour and texture may attract or deter a <strong>child</strong> fromhandling and ingesting a substance. Studies show thatliquids rather than solids, clear liquids rather than darkcoloured <strong>on</strong>es, and small solids rather than large solidshave more appeal to young <strong>child</strong>ren and are thereforemore likely to be ingested by them (77). Bright colours insolid medicati<strong>on</strong>s may also make them more attractive to<strong>child</strong>ren.Storage and accessThe most obvious risk factor for ingesti<strong>on</strong> of a substanceis its presence in the domestic envir<strong>on</strong>ment, within reachof the <strong>child</strong>. Dispensing substances – such as paraffinand medicati<strong>on</strong>s – in unlabelled or incorrectly labelledc<strong>on</strong>tainers without <strong>child</strong>-resistant closures also increasesthe risk of pois<strong>on</strong>ing (14, 26). Paraffin oil is frequentlystored in bottles or other c<strong>on</strong>tainers meant for cold drinks,milk or fruit juice, which <strong>child</strong>ren associate with beverages(36, 66, 78). In some places, tablets are poured intounsealed envelopes or ziplock bags, and liquids into n<strong>on</strong>distinctive,poorly labelled c<strong>on</strong>tainers. Children may alsodrink from c<strong>on</strong>tainers, such as cups, which have previouslybeen used for refilling heating or lighting appliances (79).White pesticide powders improperly stored close to foodsubstances can be mistaken for flour, starch or milk, andhave led to pois<strong>on</strong>ings of entire families (80).Even when dangerous products are stored in distinctivec<strong>on</strong>tainers with visual warning labels – such as images of“skull and crossb<strong>on</strong>es” – young <strong>child</strong>ren are unlikely torecognize the significance of these signs (81). Some studieshave found carelessness, overcrowding or limited spaceto be the cause of incorrect storage (14, 36). Research inAustralia has shown that many products leading to <strong>child</strong>pois<strong>on</strong>ing incidents were recently purchased or else notkept in their usual place of storage (80, 82). Medicine andbathroom cabinets, and kitchen cupboards and drawersappeared to be the safest storage places, while handbags,refrigerators, shelves and bathroom ledges were the leastsafe (83). Even safe packaging cannot compensate forunsafe storage.In developed countries, many products are requiredby law to be distributed in <strong>child</strong>-resistant packaging (84).This usually involves either a bottle with a <strong>child</strong>-resistantclosure or a blister pack. Child-resistant closures make itmore difficult for a <strong>child</strong> to open a c<strong>on</strong>tainer because theyrequire a series of complex acti<strong>on</strong>s – such as squeezing andturning, or pushing downwards and turning. The standardfor the testing of <strong>child</strong>-resistant closures adopted inmost countries requires that at least 85% of <strong>child</strong>ren agedfrom 42 to 51 m<strong>on</strong>ths must be unable to open the c<strong>on</strong>tainerwithin five minutes, and at least 80% must fail to open thec<strong>on</strong>tainer following a n<strong>on</strong>-verbal dem<strong>on</strong>strati<strong>on</strong> (85).No closure, though, is perfect. In the <strong>child</strong> testing, upto 20% of <strong>child</strong>ren aged between 42 and 51 m<strong>on</strong>ths may beable to overcome the <strong>child</strong>-resistant closure. Many parentsare unaware that young <strong>child</strong>ren may indeed be able toaccess the c<strong>on</strong>tents of <strong>child</strong>-resistant packaging. Childresistantclosures should therefore never take the place ofgood supervisi<strong>on</strong> (24).Envir<strong>on</strong>mental factorsSeas<strong>on</strong> and climateThere are significant seas<strong>on</strong>al variati<strong>on</strong>s in the incidenceof pois<strong>on</strong>ing cases for different pois<strong>on</strong>ing agents. Summeris the time of greatest risk for the ingesti<strong>on</strong> of paraffin,medicati<strong>on</strong>s and organophosphates and for bites fromscorpi<strong>on</strong>s and snakes (25, 36). Several explanati<strong>on</strong>s havebeen put forward. Children <strong>on</strong> their summer holidays aremore likely to be outdoors or to be left at home unattendedor in the care of an older <strong>child</strong> or elderly relative (65, 86,87). Children may also c<strong>on</strong>sume more fluids because of thewarmer weather. Around nati<strong>on</strong>al or religious holidays,parents or siblings may be less alert to hazards or <strong>child</strong>renmay exhibit more attenti<strong>on</strong>-seeking behaviour (88).Although the incidence of pois<strong>on</strong>ing is higher duringthe summer m<strong>on</strong>ths, a few types of pois<strong>on</strong>ing are morecomm<strong>on</strong> in winter or during cold weather. These includecarb<strong>on</strong> m<strong>on</strong>oxide pois<strong>on</strong>ing – from heating appliances –and pois<strong>on</strong>ing through ingesting cough or cold medicines,as these are often c<strong>on</strong>sidered harmless and left unattended(89).Socioec<strong>on</strong>omic envir<strong>on</strong>mentSeveral case–c<strong>on</strong>trol studies in low-income and middleincomecountries have highlighted social and demographicrisk factors in the pois<strong>on</strong>ing of <strong>child</strong>ren. These factorsinclude the presence of young parents, residential mobilityand limited adult supervisi<strong>on</strong> (65, 90, 91). Although parentsand caregivers may have been present at the time of thepois<strong>on</strong>ing incident, studies c<strong>on</strong>firm they were usuallyengaged in household duties or attending to pers<strong>on</strong>alneeds. In a significant proporti<strong>on</strong> of cases, pois<strong>on</strong>ingoccurred when a <strong>child</strong> was left in the care of another <strong>child</strong>or with a grandparent (65, 87, 91, 92).Poor living c<strong>on</strong>diti<strong>on</strong>s, local beliefs and customs andignorance of the dangers of chemicals are other risk factorsassociated with acute pois<strong>on</strong>ing (14). Previous pois<strong>on</strong>ingmay also be a risk factor (72).WORLD REPORT ON CHILD INJURY PREVENTION 131
The socioec<strong>on</strong>omic envir<strong>on</strong>ment has an effect <strong>on</strong> theexposure to the risks of pois<strong>on</strong>ing as well as <strong>on</strong> outcomes.The absence in many countries of policies, standards orlaws governing the manufacture, labelling, distributi<strong>on</strong>,storage and disposal of toxic substances place <strong>child</strong>ren atrisk of pois<strong>on</strong>ing. Poor quality c<strong>on</strong>trol in the manufactureof medicines exposes <strong>child</strong>ren to toxic c<strong>on</strong>taminantsin these products. The unregulated packaging anddistributi<strong>on</strong> of medicines and other potentially toxicsubstances in sachets and c<strong>on</strong>tainers that are not <strong>child</strong>resistantincreases the ease with which <strong>child</strong>ren can gainaccess to them. The unc<strong>on</strong>trolled storage and dumpingof pesticides near homes and in water supplies expose<strong>child</strong>ren, especially those from poorer households, totoxins.The toxicity of agents is also influenced by the politicalenvir<strong>on</strong>ment. In the United Kingdom during the 1970s,a significant proporti<strong>on</strong> of <strong>child</strong> pois<strong>on</strong>ings wereattributed to medicines, such as aspirin, barbituratesand safapryn, a drug that was a dangerous combinati<strong>on</strong>of paracetamol and aspirin (23). Aspirin is no l<strong>on</strong>gerprescribed for <strong>child</strong>ren and barbiturates have beenreplaced by less toxic agents such as benzodiazepines. Inadditi<strong>on</strong>, the chemical industry now produces less toxicpesticides. Ec<strong>on</strong>omic forces, though, are resp<strong>on</strong>sible forthe c<strong>on</strong>tinuing use in developing countries of outdatedagents, both pharmaceutical and n<strong>on</strong>-pharmaceutical,that often carry high risks.Lack of prompt treatmentIn the event of a pois<strong>on</strong>ing, quick and appropriate triage,diagnosis and treatment are vital. Pois<strong>on</strong> c<strong>on</strong>trol centresdo an excellent job of advising the public when a pois<strong>on</strong>ingis suspected, as they rely <strong>on</strong> regularly updated databasesand standard management protocols. However, manycountries do not have such a system in place. Even if theydo, people may not have access to the centres.The availability of health-care facilities and the abilityto access such facilities rapidly affects the outcome ofpois<strong>on</strong>ing injuries. Although there are no data comparingfatality rates of pois<strong>on</strong>ings in rural or remote areas – wherehealth facilities are more likely to be scarce and of lowerquality – <strong>on</strong>e would expect pois<strong>on</strong>ings in more remoteareas to have more serious outcomes. Certainly, fatalityrates in countries with limited health-care facilities arehigher than rates in more developed areas. Once a <strong>child</strong>has been transported to a hospital, the prompt recogniti<strong>on</strong>of the signs and symptoms and treatment for the correcttype of pois<strong>on</strong> involve knowledge of the latest clinicaldevelopments and skill in toxicology analysis.Interventi<strong>on</strong>sInterventi<strong>on</strong>s are usually based <strong>on</strong> risk factors that areamenable to change and that are targeted at high-riskpopulati<strong>on</strong>s.Engineering measuresReducti<strong>on</strong> of toxicityRemoving a pois<strong>on</strong>ous substance effectively may notalways be possible. An alternative approach is to lower thelevel of the toxicity of the offending agent or to neutralizeit in some way. One way of doing this is to reduce thec<strong>on</strong>centrati<strong>on</strong> of the active ingredient. In Saint Lucia, apolicy of selling acetic acid <strong>on</strong>ly in diluted form led toa fall in the rate of <strong>child</strong>hood pois<strong>on</strong>ings. Previously,c<strong>on</strong>centrated vinegar had been easily available, andhad been resp<strong>on</strong>sible for several pois<strong>on</strong>ing deaths (93).Another example of lowering toxicity is the reformulati<strong>on</strong>of methylated spirits as principally ethyl alcohol, ratherthan the more toxic methanol.In a similar way, less toxic pesticides may be used toprevent cases of acute pesticide pois<strong>on</strong>ing (32). However,safer pesticides are generally more expensive, so thatfinancial incentives or subsidies are probably neededif they are to be used in poorer countries. Introducingorganic pesticide management or an integrated vectormanagement system (94) will also lead to a fall in thenumber of cases of acute pesticide pois<strong>on</strong>ing. To operatesuch systems, though, requires scientific expertise (41).Reducing the toxic effects of ingestible pois<strong>on</strong>s byadding an antidote to the substance has also beenattempted, but has not been proved to be effective. In theUnited Kingdom, paracetamol was manufactured withadded methi<strong>on</strong>ine, an antidote to paracetamol overdose(95). This product, though, was withdrawn because it wasmore expensive than the paracetamol-<strong>on</strong>ly formulati<strong>on</strong>sthat remained <strong>on</strong> the market. In additi<strong>on</strong>, the use oforal methi<strong>on</strong>ine was questi<strong>on</strong>ed, as the substance wasassociated with allergic reacti<strong>on</strong>s.Safer packaging and storageThe success in reducing unintenti<strong>on</strong>al <strong>child</strong> pois<strong>on</strong>ingthrough safer packaging and storage over the past threedecades has relied <strong>on</strong>:– educati<strong>on</strong> of parents and caregivers – about the risksand how to protect against them;– legislati<strong>on</strong> – to prevent unsuitable c<strong>on</strong>tainers (such asare normally used to store food or drinks) being usedto store harmful substances; and to make packagingaround harmful substances resistant to tampering by<strong>child</strong>ren.In South Africa, paraffin oil is used for heat for cookingand is frequently stored in bottles previously used forstoring beverages. A successful programme to tacklethis dangerous practice involved the free distributi<strong>on</strong>of c<strong>on</strong>tainers with <strong>child</strong>-resistant closures (see Box 6.2).As a result, the annual incidence of pois<strong>on</strong>ing fell, overa period of 14 m<strong>on</strong>ths, from 104 per 100 000 to 54 per100 000 (80).132 WORLD REPORT ON CHILD INJURY PREVENTION
In affluent countries, medicines stored in the home aremore likely to be implicated in <strong>child</strong>hood pois<strong>on</strong>ing thanthey are in poorer countries. In many places, tablets orcapsules are emptied into cheap c<strong>on</strong>tainers such as paperor plastic envelopes. In developed countries, commerciallypackaged medicines are sold in a variety of preparati<strong>on</strong>sand strengths – in standard screw-capped or clip-cappedbottles, in bottles with <strong>child</strong>-resistant closures and inblister packs. To avoid errors of dosage, particularly am<strong>on</strong>gelderly people, some medicati<strong>on</strong>s are dispensed in specialboxes where multiple morning, lunchtime and eveningdoses are stored together.Child-resistant packaging is <strong>on</strong>e of the best-documentedsuccesses in preventing the unintenti<strong>on</strong>al pois<strong>on</strong>ingof <strong>child</strong>ren (96). In England and Wales, unintenti<strong>on</strong>alpois<strong>on</strong>ing deaths of <strong>child</strong>ren aged under the age of 10years fell steadily from 151 per 100 000 in 1968 to 23 per100 000 in 2000 (23). Similarly, in the United States, theannual rate of unintenti<strong>on</strong>al ingesti<strong>on</strong> of 15 regulatedsubstances in <strong>child</strong>ren younger than 5 years fell from 5.7per 1000 in 1973 to 3.4 per 1000 <strong>child</strong>ren in 1978 – withnearly 200 000 unintenti<strong>on</strong>al ingesti<strong>on</strong>s prevented duringthat period (97). Both these reducti<strong>on</strong>s were largely as aresult of the introducti<strong>on</strong> of <strong>child</strong>-resistant packaging.Safe storage of pois<strong>on</strong>s in the home requires a securelocati<strong>on</strong> where a <strong>child</strong> cannot overcome barriers oflocks or height. Although <strong>child</strong>ren will devise complexstrategies to get hold of medicines, doing so takes time.The main reas<strong>on</strong>, therefore, for storing pois<strong>on</strong>s out of reachof <strong>child</strong>ren is that this is a delaying strategy – as indeed is<strong>child</strong>-resistant packaging.Child-resistant packaging has been proved effectivefor medicati<strong>on</strong>s, fuels, household chemicals andpesticides. The cost to manufacturers and distributorsmay be an obstacle, but this is likely to be outweighedby the large savings from treating <strong>child</strong>ren who havebeen unintenti<strong>on</strong>ally pois<strong>on</strong>ed. The costs to householdsmay be offset by government subsidies, such as the freedistributi<strong>on</strong> of such c<strong>on</strong>tainers (91). Child-resistantpackaging should be used <strong>on</strong> all drugs sold over thecounter, to help prevent <strong>child</strong>ren c<strong>on</strong>suming thesepotentially lethal products (98).Reducing an agent’s attractivenessOne study has shown that the appropriate design ofpackaging can be an effective means of reducing theattractiveness for <strong>child</strong>ren of harmful substances (99).Other studies, <strong>on</strong> the ingesti<strong>on</strong> by <strong>child</strong>ren of paraffin,have recommended that c<strong>on</strong>tainers be made of darkenedmaterial in which the c<strong>on</strong>tents are invisible (25). Thereas<strong>on</strong> for this is that, since paraffin may be easilymistaken for water, a n<strong>on</strong>-transparent, dark c<strong>on</strong>taineris less likely to be associated with a drinkable liquidthan a transparent, light-coloured c<strong>on</strong>tainer. Anothersuggesti<strong>on</strong> is to modify the taste and colour of paraffinas well as modifying the c<strong>on</strong>tainers in which it is storedBOX 6.2Change the packaging, save a lifeSome 40 000 to 60 000 <strong>child</strong>ren in South Africa ingest paraffin oileach year, and suffer c<strong>on</strong>sequent pois<strong>on</strong>ing. Between 170 and 500of those admitted to hospital with paraffin pois<strong>on</strong>ing do not survive.This figure, though, may be much higher because many serious casesdo not reach hospital in time and are therefore not included in thestatistics (100). The majority of <strong>child</strong>ren affected are under the ageof 5 years. In additi<strong>on</strong> to their suffering, and that of their families,there are substantial costs, borne by the state, for hospital care andtreatment.C<strong>on</strong>cerned groups are being called up<strong>on</strong> to step up efforts toprotect <strong>child</strong>ren in poor and marginalized communities, where themajority of paraffin pois<strong>on</strong>ing incidents and deaths occur. Local researchhas highlighted the effectiveness of <strong>child</strong>-resistant closuresin avoiding the ingesti<strong>on</strong> of pois<strong>on</strong>s am<strong>on</strong>g <strong>child</strong>ren (65). Childresistantclosures – packaging that is difficult for <strong>child</strong>ren underthe age of 5 years to open, but which an adult can easily open –are the <strong>on</strong>ly proven interventi<strong>on</strong> that will reduce the incidence ofparaffin ingesti<strong>on</strong> am<strong>on</strong>g <strong>child</strong>ren. In 1994, a study in a rural communityin South Africa showed that the free distributi<strong>on</strong> of <strong>child</strong>resistantclosures reduced the incidence of paraffin ingesti<strong>on</strong> by47.4% over a period of 14 m<strong>on</strong>ths, compared to a c<strong>on</strong>trol communitywhere there were no <strong>child</strong>-resistant c<strong>on</strong>tainers (65).Every <strong>child</strong> has a right, enshrined in South Africa’s c<strong>on</strong>stituti<strong>on</strong>,to grow up in an envir<strong>on</strong>ment that is not harmful to his or herhealth or well-being. The mandatory use of <strong>child</strong>-resistant closurescould save the lives of more than 80 <strong>child</strong>ren in the country eachyear and reduce incidence rates of paraffin ingesti<strong>on</strong> by half.© L. Matzopoulos, Khusela AbantwanaWORLD REPORT ON CHILD INJURY PREVENTION 133
(27). In Australia, changing the colour of paraffin to blueled to a decrease in the incidence of paraffin ingesti<strong>on</strong>(101).The additi<strong>on</strong> of bitter agents is another method ofstopping <strong>child</strong>ren from c<strong>on</strong>suming significant quantitiesof harmful substances. Studies have shown that thisapproach may be useful, though it is possibly moreappropriate for household products of mild to moderatetoxicity rather than for pharmaceutical products (102,103).Labelling c<strong>on</strong>tainers with warning stickers showed nodeterrent effect <strong>on</strong> <strong>child</strong>ren at risk aged under 6 years(81, 104). The possible effectiveness of warning labelsdepends very heavily <strong>on</strong> their being understood by all,and assumes some degree of literacy. It has even beensuggested that in some cases, warning labels may attract<strong>child</strong>ren (81).Envir<strong>on</strong>mental measuresStudies show that 56% of unintenti<strong>on</strong>al pois<strong>on</strong>ings inyoung <strong>child</strong>ren occur within the <strong>child</strong>’s home, andanother 17% occur in or around some<strong>on</strong>e else’s home(16). Reducing <strong>child</strong>ren’s access to pois<strong>on</strong>s in the homecan be achieved in a number of ways.Removing toxic agentsThe most effective way to prevent <strong>child</strong>ren coming intoc<strong>on</strong>tact with a pois<strong>on</strong> is to remove the pois<strong>on</strong> itself. Anexample of this is the Manchineel tree. The fruit of thistree looks like an edible green apple but the fruit, barkand sap are all toxic. Pois<strong>on</strong>ings from the Manchineeltree, especially am<strong>on</strong>g <strong>child</strong>ren, used to be comm<strong>on</strong> inthe Caribbean, despite warning signs and educati<strong>on</strong>alcampaigns. Eventually, the trees were removed by theauthorities from the beach areas where they were prevalentand replaced by coco plum trees, with a c<strong>on</strong>sequent fall inthe number of pois<strong>on</strong>ing cases.Alternatively, toxic agents may be replaced by othersubstances with a lower toxicity. As examples, the followinghighly toxic substances have been largely replaced in manyplaces by less toxic substances having a similar intendedeffect (23):– barbiturates (a class of sedative-hypnotic drugs) bybenzodiazepines;– cresol (a preservative) by chlorocresol;– aspirin by paracetamol;– toxic anti-inflammatory drugs with less toxic n<strong>on</strong>steroidalanti-inflammatory drugs.Sometimes the change from toxic to less toxic substancesoccurs as a side effect of ec<strong>on</strong>omic development. Theincidence of paraffin ingesti<strong>on</strong>, for instance, has beenfound to fall when countries move from using individualfuel sources, such as bottled paraffin, to safer alternativessuch as electricity and natural gas supplied by publicutilities (32).Laws and regulati<strong>on</strong>sA comprehensive strategy to prevent <strong>child</strong>hood pois<strong>on</strong>ingmust include laws supported by enforcement. This has beenshown in the case of <strong>child</strong>-resistant closures. The laws <strong>on</strong><strong>child</strong>-resistant closures and a high degree of compliance bymanufacturers have seen falls in mortality rates in severaldeveloped countries.Child-resistant packagingStandards and policies for <strong>child</strong>-resistant packagingcurrently <strong>on</strong>ly exist in a handful of high-income countries,such as Australia, Canada, New Zealand, the UnitedStates and the European Uni<strong>on</strong>. The absence of laws (ortheir lack of enforcement) and policies <strong>on</strong> manufacturing,storing, distributing and disposing of hazardous productshas led to deaths of <strong>child</strong>ren as a result of c<strong>on</strong>taminatedmedicines and toothpaste. In the Bhopal catastrophe,methyl isocyanate – a pois<strong>on</strong>ous gas, heavier than air, thatis used in the producti<strong>on</strong> of pesticides – was released intothe atmosphere. In the absence of a str<strong>on</strong>g local legislativeframework, internati<strong>on</strong>al standards and laws need to playa role in regulating global companies, currently often ableto operate with lower levels of care than in their countryof origin.In 1970, the United States introduced <strong>child</strong>-resistantpackaging in its Pois<strong>on</strong>s Preventi<strong>on</strong> Packaging Act. Withrates of compliance am<strong>on</strong>g manufacturers of between60% and 75%, the incidence of unintenti<strong>on</strong>al ingesti<strong>on</strong>of baby aspirin was reduced by 45%–55% and of regularaspirin by 40%–45% in <strong>child</strong>ren less than 5 years old(105). Pois<strong>on</strong>ing deaths am<strong>on</strong>g <strong>child</strong>ren under 5 years ofage, resulting from the ingesti<strong>on</strong> of substances regulatedby the 1970 law, declined from 450 in 1962 to 216 in 1972and 33 in 2005 (106).The European Uni<strong>on</strong> has laws (107) mandating thestorage of toxic substances in <strong>child</strong>-resistant c<strong>on</strong>tainersthat are:– clearly and appropriately labelled;– in places that are not within reach of <strong>child</strong>ren or near tofoodstuff;– labelled in such a way that the substances in questi<strong>on</strong>cannot be mistaken for food.This clearly places the <strong>on</strong>us for protecting <strong>child</strong>ren fromtoxic substances <strong>on</strong> households as well as <strong>on</strong> manufacturersand distributors. These laws may account for the low ratesof <strong>child</strong> pois<strong>on</strong>ing seen in much of Europe.Blister packsBlister packs (n<strong>on</strong>-reclosable packaging) for medicinesin tablet or capsule form are increasingly being used fordispensing. So<strong>on</strong> after they were introduced such packswere c<strong>on</strong>sidered to be <strong>child</strong>-resistant, because of the timeit takes to remove each individual tablet or capsule andled to some reducti<strong>on</strong>s in <strong>child</strong> pois<strong>on</strong>ing (108). However,134 WORLD REPORT ON CHILD INJURY PREVENTION
as the use of blister packs has increased, it has becomeclear from pois<strong>on</strong> centre data that young <strong>child</strong>ren canaccess medicati<strong>on</strong>s from such packs. While removingand swallowing the tablets from a single strip of a blisterpack may be less likely to be harmful than having accessto a full bottle of the comparable liquid form, for manymedicines even a few tablets can be a toxic or even a lethaldose for a young <strong>child</strong>. One advantage of blister packagingis that parents may better recall how many tablets hadbeen used before the <strong>child</strong> swallowed some – thus beingable to calculate the maximum number that may havebeen ingested. The disadvantage of blister packs is theirtransportability. Studies have shown that <strong>child</strong>ren oftenremove medicati<strong>on</strong>s from handbags, particularly thosebel<strong>on</strong>ging to the grandmother (109). This has promptedthe development of a European standard for <strong>child</strong>-resistantblister packs, using a <strong>child</strong> test panel similar to the <strong>on</strong>e forthe reclosable <strong>child</strong>-resistant packaging standard.Educati<strong>on</strong>al approachesAlthough not an effective interventi<strong>on</strong> strategy by itself,educati<strong>on</strong> <strong>on</strong> how to prevent pois<strong>on</strong>ing has been shown tobe a useful comp<strong>on</strong>ent of preventi<strong>on</strong> programmes (110–114). Educati<strong>on</strong> <strong>on</strong> pois<strong>on</strong>ing should aim to:– raise awareness;– increase knowledge and skills <strong>on</strong> pois<strong>on</strong> preventi<strong>on</strong>;– change attitudes and behaviours;– influence policy and legislati<strong>on</strong>;– create good practices within organizati<strong>on</strong>s.Educati<strong>on</strong>al interventi<strong>on</strong>s should be used incombinati<strong>on</strong> with other interventi<strong>on</strong>s seeking to preventpois<strong>on</strong>ing.Most pois<strong>on</strong>ings in young <strong>child</strong>ren occur at home, withparents or caregivers nearby and engaged in householdtasks. While c<strong>on</strong>tinuous direct supervisi<strong>on</strong> (always withineyesight) would reduce the access of <strong>child</strong>ren to pois<strong>on</strong>s,it is not practical to promote such a strategy. C<strong>on</strong>tinuoussupervisi<strong>on</strong> is difficult to achieve even for caregiversin affluent households with few <strong>child</strong>ren. In poorerhouseholds, there are likely to be more <strong>child</strong>ren to be caredfor and other competing household tasks to be performed.In such circumstances, passive measures are likely to bemore effective.The effectiveness of public awareness and generaleducati<strong>on</strong> campaigns in reducing the incidence of<strong>child</strong> pois<strong>on</strong>ing cases is open to questi<strong>on</strong>. Educati<strong>on</strong>alcampaigns in isolati<strong>on</strong> have not had a significant impact<strong>on</strong> the ingesti<strong>on</strong> of harmful substances (110, 115). Onestudy in the state of Massachusetts in the United Statesshowed no significant increase in compliance followinga campaign of advice <strong>on</strong> how to prevent pois<strong>on</strong>ing (111).Research has also shown that mothers and caregiverstake fewer precauti<strong>on</strong>s against <strong>child</strong> pois<strong>on</strong>ings if theseprecauti<strong>on</strong>s involve more effort, and especially if theyinvolve changes in behaviour. Passive interventi<strong>on</strong>s, asalready stated, are likely to be more successful and shouldbe promoted (112).It has been suggested that messages used in educati<strong>on</strong>alprogrammes directed at caregivers (including parents)may be more effective if they address the factorsinfluencing the behaviour of the caregivers. Further, homevisits by health-care workers to reinforce the messagesof the educati<strong>on</strong>al programmes have been shown to beeffective (113).Educati<strong>on</strong>al programmes with a narrower, morespecific aim may be more successful. Such programmesmay include:– point-of-sale warnings from pharmacists <strong>on</strong> thepossible dangers of the medicati<strong>on</strong> being dispensed;– public awareness campaigns that “<strong>child</strong>-resistant doesnot mean <strong>child</strong>-proof”;– messages to parents and caregivers reminding themto test <strong>child</strong>-resistant closures and to ensure that theseclosures have been properly re-engaged;– messages to parents and caregivers that comm<strong>on</strong>household products may be dangerous for young<strong>child</strong>ren – even such “healthy” or “natural” products asir<strong>on</strong> tablets or essential oils.A recent systematic review <strong>on</strong> the effect of home safetyeducati<strong>on</strong> and the provisi<strong>on</strong> of safety equipment <strong>on</strong>pois<strong>on</strong>ing preventi<strong>on</strong> practices revealed that althoughthese interventi<strong>on</strong>s improve pois<strong>on</strong> preventi<strong>on</strong> strategies,their impact <strong>on</strong> pois<strong>on</strong>ing preventi<strong>on</strong> rates remainsunclear (116).Managing pois<strong>on</strong>ingManagement of a pois<strong>on</strong>ing requires immediate adviceand first aid, followed by directed treatment wherenecessary.Acute management of pois<strong>on</strong>ingBox 6.3 outlines the general principles governing themanagement of all cases of acute pois<strong>on</strong>ing (48, 117).Early and accurate diagnosis and management ofpois<strong>on</strong>ing decrease the risk of morbidity and mortality.It is therefore vital that caregivers seek help from a pois<strong>on</strong>centre or a professi<strong>on</strong>al health-care worker. An assessment,including the previous history, should be made if possible,though this may be difficult with <strong>child</strong>ren. It is importantto keep the airway clear, the breathing regular and thecirculati<strong>on</strong> flowing.The agent is likely to be known, but the dosage may haveto be estimated. Treatment should be based <strong>on</strong> the greatestexposure that could have occurred. There are manysophisticated tests and procedures, but their effectivenesshas in some cases been questi<strong>on</strong>ed. Some of these tests mayin any case not be possible to perform in most developingcountries.WORLD REPORT ON CHILD INJURY PREVENTION 135
BOX 6.3Managing acute pois<strong>on</strong>ing: the general principles1. Remove the <strong>child</strong> from the source of exposure and dec<strong>on</strong>taminate the <strong>child</strong>, as described below, if the pois<strong>on</strong> has been inhaled or absorbedthrough the skin or mucous membranes. C<strong>on</strong>taminated clothing, including shoes and socks, and jewellery should be removed. Where toxins havebeen inhaled, the <strong>child</strong> should be removed to an envir<strong>on</strong>ment of fresh air.2. Assess what agent, or agents, and doses are involved, the time since ingesti<strong>on</strong> and the current clinical status – as well as other factors related tothe <strong>child</strong>, such as age, gender and the presence of other illnesses. Toxic screening has limited value as it delays management and is seldom availablein developing countries.3. Stabilize the <strong>child</strong>. The general approach to acute pois<strong>on</strong>ing involves giving priority to the airway, breathing and circulati<strong>on</strong> – as for any emergency.4. Dec<strong>on</strong>taminate the <strong>child</strong>, if appropriate. It is important to limit the absorpti<strong>on</strong> of an ingested agent. Gastrointestinal dec<strong>on</strong>taminati<strong>on</strong> is reservedfor severe or life-threatening cases, where the pois<strong>on</strong> is still in the gastrointestinal tract and can be removed. The airways must be secured andgut motility assured before embarking <strong>on</strong> gastrointestinal dec<strong>on</strong>taminati<strong>on</strong>.Specific dec<strong>on</strong>taminati<strong>on</strong> measures include the following. Topical dec<strong>on</strong>taminati<strong>on</strong>. Whatever the means of exposure, any body surface – including the eyes – that is exposed to a toxin should be flushedwell with large amounts of water, saline or other fluids specific to the pois<strong>on</strong>. Activated charcoal may be used to absorb many organic pois<strong>on</strong>s. It is ineffective, though, for hydrocarb<strong>on</strong>s, caustics, alcohols and some heavymetals. Though not proved to achieve a better clinical outcome, activated charcoal does result in a decrease in absorpti<strong>on</strong> of the pois<strong>on</strong> if it isused within <strong>on</strong>e hour of ingesti<strong>on</strong>. Complicati<strong>on</strong>s associated with activated charcoal include aspirati<strong>on</strong> and c<strong>on</strong>stipati<strong>on</strong>. Gastric emptying can be achieved in two ways.– One means of gastric emptying is through vomiting, but it is no l<strong>on</strong>ger a routinely used method as its effectiveness is in doubt. There mayalso be complicati<strong>on</strong>s with vomiting and it is c<strong>on</strong>traindicated in <strong>child</strong>ren less than six m<strong>on</strong>ths of age, in <strong>child</strong>ren with unprotected airwaysor when the ingested substance is an organic solvent, such as petrol or paraffin oil, or a corrosive agent.– The sec<strong>on</strong>d means is through gastric lavage. In this method, the stomach is washed out with small aliquots of normal saline until its c<strong>on</strong>tentsare cleared. This procedure should <strong>on</strong>ly be performed if indicated and is not recommended for <strong>child</strong>ren less than six m<strong>on</strong>ths of age. Catharsis to increase gastrointestinal motility and hence hasten the expulsi<strong>on</strong> of unabsorbed pois<strong>on</strong>. There is little evidence, though, tosupport the use of catharsis as a means of reducing gastrointestinal absorpti<strong>on</strong> following an overdose, and the complicati<strong>on</strong>s offl u i dl o s sa n delectrolyte imbalance outweigh any benefits. Whole bowel irrigati<strong>on</strong> can be used to physically eliminate highly toxic substances not absorbed by charcoal. Its use is neither supported norrefuted if substances such as ir<strong>on</strong>, lead and paraquat have been ingested. A n<strong>on</strong>-absorbable liquid such as polyethylene glycol soluti<strong>on</strong> is usedto induce a liquid stool until the rectal effluent clears. Complicati<strong>on</strong>s include fluid and electrolyte imbalance, bloating and vomiting. Alkaline diuresis enhances eliminati<strong>on</strong> of some acidic substances. An example is bicarb<strong>on</strong>ate administered to enhance the eliminati<strong>on</strong> ofaspirin. Dialysis – including haemodialysis, perit<strong>on</strong>eal dialysis, haemofiltrati<strong>on</strong> and haemoperfusi<strong>on</strong> – may be used in specific circumstances to clearcertain water-soluble pois<strong>on</strong>s from the circulati<strong>on</strong>. Antidotes. Envenomati<strong>on</strong>s should be treated with antivenom, most comm<strong>on</strong>ly for snakebite and scorpi<strong>on</strong> stings, and also for some spiders’bites. Atropine is used for carbamates; atropine and pralidoxime for organophosphorus pesticide pois<strong>on</strong>ing; nalox<strong>on</strong>e for opioids; acetylcysteinefor paracetamol overdoses; and chelating agents for some heavy metals.5. Provide supportive therapy, including the treatment of complicati<strong>on</strong>s. The main management in acute pois<strong>on</strong>ing includes: airway stabilizati<strong>on</strong>;seizure c<strong>on</strong>trol; correcti<strong>on</strong> of hypoglycaemia; correcti<strong>on</strong> of hyperthermia; treatment of shock and pain; and the use of antidotes.Pois<strong>on</strong> c<strong>on</strong>trol centresPois<strong>on</strong> c<strong>on</strong>trol centres provide advice to individualsand health-care instituti<strong>on</strong>s. They direct first aid whereappropriate, and refer more severe pois<strong>on</strong>ings to a healthcarefacility. Pois<strong>on</strong> c<strong>on</strong>trol centres are resp<strong>on</strong>sible forless severe outcomes in cases of pois<strong>on</strong>ing. They alsoeliminate much unnecessary c<strong>on</strong>tact with more expensivehealth-care services (118). They were initially set up inhigh-income countries and have since been establishedin many low-income and middle-income countries (seeBox 6.4).There are problems, though, in establishing pois<strong>on</strong>c<strong>on</strong>trol centres in less developed countries. Often, theneed for such centres is not properly appreciated. Thereis likely to be a shortage of adequately trained staff,and poor clinical and laboratory toxicology servicesfor further management of cases (119). In additi<strong>on</strong>, theeffectiveness of pois<strong>on</strong> c<strong>on</strong>trol centres depends <strong>on</strong> goodteleph<strong>on</strong>e communicati<strong>on</strong>s, which may in some places belimited, though this obstacle is likely to be overcome bythe increasing use of mobile teleph<strong>on</strong>es (120).It is estimated that for every dollar spent <strong>on</strong> a pois<strong>on</strong>c<strong>on</strong>trol centre c<strong>on</strong>tact there is a saving of nearly eightdollars, as more than 70% of cases are resolved over theteleph<strong>on</strong>e (118). If these centres did not exist, an estimated600 000 additi<strong>on</strong>al possible pois<strong>on</strong>ing cases would receive136 WORLD REPORT ON CHILD INJURY PREVENTION
treatment at a health-care facility each year, at an addedcost of US$ 545 milli<strong>on</strong>.Involving a range of sectorsThere is a wide range of groups and sectors that need tobe involved for the successful preventi<strong>on</strong> of accidentalpois<strong>on</strong>ing of <strong>child</strong>ren. In additi<strong>on</strong> to the health-caresector, parents and caregivers, there are: the educati<strong>on</strong>sector; the justice ministry; the departments of tradeand industry; c<strong>on</strong>sumer groups; n<strong>on</strong>governmentalorganizati<strong>on</strong>s c<strong>on</strong>cerned with <strong>child</strong> safety; producersBOX 6.4The Nati<strong>on</strong>al Pois<strong>on</strong>s Informati<strong>on</strong>Centre in Sri LankaIn Sri Lanka in 2005, pois<strong>on</strong>ing accounted for almost 90 000 hospitaladmissi<strong>on</strong>s and 1785 deaths. Around a third of these cases were in<strong>child</strong>ren under the age of 18 years.The first pois<strong>on</strong> c<strong>on</strong>trol centre in the world was established in1953 in the state of Illinois, United States, largely in resp<strong>on</strong>se to thenumber of pois<strong>on</strong>ing cases involving <strong>child</strong>ren. One of its aims wasto instruct doctors <strong>on</strong> how to deal promptly with accidental overdoses,cases of chemical pois<strong>on</strong>ing and animal bites or stings. Moregenerally, the centre provided informati<strong>on</strong> <strong>on</strong> the toxic ingredientsof substances and their chemical effects.In Sri Lanka, the Nati<strong>on</strong>al Pois<strong>on</strong>s Informati<strong>on</strong> Centre was set upin 1988 – the first such centre in South Asia (121). Deaths from insecticidepois<strong>on</strong>ing were of special c<strong>on</strong>cern, and three pesticides in particular– m<strong>on</strong>ocrotofos, methamidofos and endosulfan – were foundto be killing agricultural workers and their <strong>child</strong>ren. As a result, theimportati<strong>on</strong> of these pesticides was banned in Sri Lanka.In the first 10 years of its existence the Nati<strong>on</strong>al Pois<strong>on</strong>s Informati<strong>on</strong>Centre dealt with 4070 enquiries (121). Of these, 3671 wereby teleph<strong>on</strong>e (about a third of them relating to <strong>child</strong>ren and youngpeople under 20 years of age), 368 were pers<strong>on</strong>al visits to the centre,and 31 written enquiries. Over 90% of the teleph<strong>on</strong>e calls were fromhealth-care pers<strong>on</strong>nel, most of the rest coming from members of thepublic. Around half the enquiries were in c<strong>on</strong>necti<strong>on</strong> with suicideattempts, and a further third c<strong>on</strong>cerned unintenti<strong>on</strong>al pois<strong>on</strong>ingincidents (4).The centre is staffed by three informati<strong>on</strong> officers covering thehours from 8:00 to 17:00 every day. Calls outside working hoursare referred to the intensive care unit at the Nati<strong>on</strong>al Hospital ofSri Lanka (4).In 1993, again in resp<strong>on</strong>se to a c<strong>on</strong>tinuing problem with pesticides,several new measures were put in place to strengthen the Nati<strong>on</strong>alPois<strong>on</strong> Informati<strong>on</strong> Centre. These included:– a 24-hour service for health-care professi<strong>on</strong>als and doctors;– a laboratory facility for analysing blood, urine and stomach c<strong>on</strong>tents;– the ability to supply antidotes to hospitals.As a result of these and other services provided by the centre,the incidence of morbidity and mortality from pois<strong>on</strong>ing in Sri Lankahas fallen.and retailers of pharmaceuticals, agrochemicals andother toxic substances; and industries that handle toxicsubstances and in which <strong>child</strong>ren are employed.In the Netherlands, a programme to preventunintenti<strong>on</strong>al pois<strong>on</strong>ing am<strong>on</strong>g <strong>child</strong>ren aged 0–4 yearsresulted in a 15% reducti<strong>on</strong> in the number of pois<strong>on</strong>ingcases and a 50% fall in the number of admissi<strong>on</strong>s to healthcarefacilities. The programme involved health-careworkers, parents, kindergarten teachers, the mass media,n<strong>on</strong>governmental organizati<strong>on</strong>s, and the pharmaceuticaland chemical industries (including retailers anddistributors) (122). Another example of a multisectoralcollaborati<strong>on</strong> to prevent pois<strong>on</strong>ings is the establishmentof pois<strong>on</strong> c<strong>on</strong>trol centres in developing countries (120).Industry has an important role to play in reducing thenumber of toxic substances produced, both directly and asby-products. In developed countries, as demand for moreenvir<strong>on</strong>mentally-friendly products has increased, industryhas resp<strong>on</strong>ded by modifying products, with the increasedcost met by c<strong>on</strong>cerned c<strong>on</strong>sumers. Products have in thisway been modified to produce safer versi<strong>on</strong>s, not throughplanned interventi<strong>on</strong>s but as a result of independentlyoccurring social changes. Financial incentives to industry,that have led to a reducti<strong>on</strong> in carb<strong>on</strong> emissi<strong>on</strong>s, may alsobe effective in reducing the range of household pois<strong>on</strong>s towhich young <strong>child</strong>ren are exposed. Both legislati<strong>on</strong> and astr<strong>on</strong>g voluntary engagement of the corporate sector arelikely to be required to ensure the safe storage and disposalof toxic products and by-products.Evaluating interventi<strong>on</strong>sEvaluati<strong>on</strong> is vital in determining whether policies andprogrammes for pois<strong>on</strong>ing preventi<strong>on</strong> are effective.An essential element of evaluati<strong>on</strong> is having an <strong>injury</strong>surveillance system or else the ability to collect data fromhealth-care settings. In the Netherlands, surveillance datathat had been gathered were used successfully to evaluatea range of interventi<strong>on</strong>s – from <strong>child</strong>-resistant closures toeducati<strong>on</strong>al campaigns for safer storage (123).C<strong>on</strong>clusi<strong>on</strong>s and recommendati<strong>on</strong>sDespite reducti<strong>on</strong>s in the incidence of <strong>child</strong> pois<strong>on</strong>ingfollowing specific interventi<strong>on</strong>s, cases of pois<strong>on</strong>ing stillc<strong>on</strong>tribute towards a significant proporti<strong>on</strong> of <strong>child</strong>injuries.One of the greatest obstacles in the way of effectivepreventi<strong>on</strong> and c<strong>on</strong>trol of pois<strong>on</strong>ing is the lack of reliabledata. Few data collecti<strong>on</strong> systems exist and those that doare mainly in developed countries. As a result, it is difficultto estimate the scale of the problem precisely in thoseplaces where the incidence may be the greatest.Several interventi<strong>on</strong>s have been tried, with varyinglevels of success (see Table 6.3) (124–126). Measuresthat have been found effective to some degree includepois<strong>on</strong> c<strong>on</strong>trol centres, <strong>child</strong>-resistant packaging, andWORLD REPORT ON CHILD INJURY PREVENTION 137
educati<strong>on</strong> (including training of parents and caregivers)combined with home visitati<strong>on</strong>s (113, 116). Many of thesuccessful preventi<strong>on</strong> interventi<strong>on</strong>s have been tested <strong>on</strong>lyin developed countries.Recommendati<strong>on</strong>sData collecti<strong>on</strong> systems need to be improved in waysappropriate to the setting. The data obtained willhelp to identify populati<strong>on</strong>s at risk and their specificrisk factors, as well as facilitating the design andimplementati<strong>on</strong> of interventi<strong>on</strong>s.More research is needed <strong>on</strong> the ability to reproduceand transfer across cultural boundaries successfulpreventi<strong>on</strong> interventi<strong>on</strong>s <strong>on</strong> <strong>child</strong>hood pois<strong>on</strong>ing.Pois<strong>on</strong> c<strong>on</strong>trol centres, with well-trained pers<strong>on</strong>nel,should be set up as widely as possible. In places wherethey have operated, they have saved many lives andlarge amounts in health-care costs (127).Countries should set laws and standards relating tothe manufacture, storage, distributi<strong>on</strong> and disposal ofpotentially toxic substances.Countries should introduce laws mandating <strong>child</strong>resistantpackaging for medicati<strong>on</strong>s, and for pesticides,rodenticides and other potentially toxic householditems. The effectiveness of such packaging shouldbe evaluated, particularly where blister packs arec<strong>on</strong>cerned.Industry needs to play a greater role in reducing thepresence of toxins and in safely packaging itemsthat are sold to households. Greater care needs tobe taken in the producti<strong>on</strong> process itself, to ensurethat by-products and waste do not c<strong>on</strong>taminate theenvir<strong>on</strong>ment.Treatment protocols should be developed to assist withthe initial assessment and management of potential<strong>child</strong> pois<strong>on</strong>ing cases. These protocols should target themost frequently involved and most toxic pharmaceuticals(128).References1. Paracelsus. Encyclopaedia Britannica <strong>on</strong>line (http://www.britannica.com/eb/article-9058368, accessed 7 April2008).2. Bateman DN. The epidemiology of pois<strong>on</strong>ing. Medicine,2007, 35:537–539.3. Taft C et al. Childhood unintenti<strong>on</strong>al <strong>injury</strong> worldwide:meeting the challenge. Washingt<strong>on</strong>, DC, Safekids<str<strong>on</strong>g>World</str<strong>on</strong>g>wide, 2002 (http://www.safekids.org/pdf/WW-Study-Ltr.pdf, accessed 6 April 2008).4. Fernando R, Fernando DN. Childhood pois<strong>on</strong>ing in SriLanka. Indian Journal of Pediatrics, 1997, 64:457–560.5. Dutta AK et al. Pois<strong>on</strong>ing in <strong>child</strong>ren: Indian scenario.Indian Journal of Pediatrics, 1998, 65:365–370.6. Du NT, Due B, Due P. Epidemiology of acute pois<strong>on</strong>ingsin Vietnam. Clinical Toxicology, 2001, 39:527–528.7. Agran PF et al. Rates of pediatric and adolescent injuriesby year of age. Pediatrics, 2001, 108:E45.8. Forum IV: Chemical safety in a vulnerable world: facts andfigures. Inter-governmental Forum <strong>on</strong> Chemical Safety,2003 (http://www.who.int/ifcs/documents/forums/forum4/en/facts_en.pdf, accessed 6 April 2008).9. Goto K et al. Pois<strong>on</strong>ing in <strong>child</strong>ren in Japan. Indian Journalof Pediatrics, 1997, 64:461–468.TABLE 6.3Key strategies to prevent pois<strong>on</strong>ing am<strong>on</strong>g <strong>child</strong>renStrategyEffectivePromisingInsufficientevidenceIneffectivePotentiallyharmfulRemoving the toxic agentLegislating for (and enforcing) <strong>child</strong>-resistant packaging of medicines and pois<strong>on</strong>sPackaging drugs in n<strong>on</strong>-lethal quantitiesEstablishing pois<strong>on</strong> c<strong>on</strong>trol centresLocking away medicines and other toxic substancesRemoving or regulating availability of toxic substances that are easily mistaken foredible itemsTeaching <strong>child</strong>ren to avoid pois<strong>on</strong>ous substancesReducing the attractiveness of medicati<strong>on</strong>s and pois<strong>on</strong>ous productsProviding home safety educati<strong>on</strong> and safety equipmentClearly labelling toxic productsIntroducing n<strong>on</strong>-standardized, n<strong>on</strong>-reclosable packaging for tablets138 WORLD REPORT ON CHILD INJURY PREVENTION
10. Br<strong>on</strong>stein AC et al. 2006 annual <str<strong>on</strong>g>report</str<strong>on</strong>g> of the AmericanAssociati<strong>on</strong> of Pois<strong>on</strong> C<strong>on</strong>trol Centres’ Nati<strong>on</strong>al Pois<strong>on</strong>Data System (NPDS). Clinical Toxicology, 2007, 45:815–917.11. Wats<strong>on</strong> W et al. 2004 Annual <str<strong>on</strong>g>report</str<strong>on</strong>g> of the AmericanAssociati<strong>on</strong> of Pois<strong>on</strong> C<strong>on</strong>trol Centers Toxic ExposureSurveillance System. American Journal of EmergencyMedicine, 2005, 23:589–666.12. O’C<strong>on</strong>nor PJ. Differentials in pois<strong>on</strong>ing rates of youngAustralian <strong>child</strong>ren according to residential locati<strong>on</strong>and geographical remoteness. Injury Preventi<strong>on</strong>, 2005,11:204–206.13. Agran PF et al. Rates of pediatric injuries by 3-m<strong>on</strong>thintervals for <strong>child</strong>ren 0–3 years of age. Pediatrics, 2003,111:E683–E692.14. Nhachi CF, Kasilo OM. The pattern of pois<strong>on</strong>ing in urbanZimbabwe. Journal of Applied Toxicology, 1992, 12:435–438.15. Khare M et al. Pois<strong>on</strong>ing in <strong>child</strong>ren: analysis of 250 cases.Journal of Postgraduate Medicine, 1990, 36:203–206.16. Hyder AA et al. Childhood unintenti<strong>on</strong>al <strong>injury</strong>surveillance: a multi-site pilot study. Baltimore, MD, JohnsHopkins University and <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong> (inpress).17. Ballesteros MF et al. Differential ranking of causes offatal versus n<strong>on</strong>-fatal injuries am<strong>on</strong>g US <strong>child</strong>ren. InjuryPreventi<strong>on</strong>, 2003, 9:173–176.18. Rajka T et al. Acute <strong>child</strong> pois<strong>on</strong>ings in Oslo: a 2-yearprospective study. Acta Paediatrica, 2007, 96:1355–1359.19. Nati<strong>on</strong>al Pois<strong>on</strong> Preventi<strong>on</strong> Week warns: most <strong>child</strong>pois<strong>on</strong>ings from comm<strong>on</strong> household products. Washingt<strong>on</strong>,DC, US C<strong>on</strong>sumers Product Safety Commissi<strong>on</strong>, 2005(Release #05–136) (http://www.cpsc.gov/cpscpub/prerel/prhtml05/05136.html, accessed 7 April 2008).20. Hanssens Y, Deleu D, Taqi A. Etiologic and demographiccharacteristics of pois<strong>on</strong>ing: A prospective hospital-basedstudy in Oman. Clinical Toxicology, 2001, 39:371–380.21. Daws<strong>on</strong> KP et al. Accidental pois<strong>on</strong>ing of <strong>child</strong>ren in theUnited Arab Emirates. Eastern Mediterranean HealthJournal, 1997, 3:38–42.22. Gupta SK et al. A study of <strong>child</strong>hood pois<strong>on</strong>ing at Nati<strong>on</strong>alPois<strong>on</strong>s Informati<strong>on</strong> Centre, All India Institute of MedicalSciences, New Delhi. Journal of Occupati<strong>on</strong>al Health,2003, 45:191–196.23. Flanagan R, Ro<strong>on</strong>ey C, Griffiths C. Fatal pois<strong>on</strong>ing in<strong>child</strong>hood, England and Wales, 1968–2000. ForensicScience Internati<strong>on</strong>al, 2005, 148:121–129.24. Chien C et al. Unintenti<strong>on</strong>al ingesti<strong>on</strong> of over the countermedicati<strong>on</strong>s in <strong>child</strong>ren less than 5 years old. Journal ofPaediatrics and Child Health, 2003, 39:264–269.25. Abu-Ekteish F. Kerosene pois<strong>on</strong>ing in <strong>child</strong>ren: a <str<strong>on</strong>g>report</str<strong>on</strong>g>from Northern Jordan. Tropical Doctor, 2002, 32:27–29.26. Chibwana C, Mhango T, Molyneux E. Childhoodpois<strong>on</strong>ing at the Queen Elizabeth Central Hospital,Blantyre, Malawi. East African Medical Journal, 2001,78:292–295.27. Barss P et al. Injury preventi<strong>on</strong>: an internati<strong>on</strong>al perspective.New York, NY, Oxford University Press, 1998.28. Singh H et al. Management of accidental keroseneingesti<strong>on</strong>. Annals of Tropical Paediatrics, 1992, 12:105–109.29. Chitsike I. Acute pois<strong>on</strong>ing in a paediatric intensive careunit in Harare. Central African Journal of Medicine, 1994,40:315–319.30. Gupta S et al. Trends in pois<strong>on</strong>ing in <strong>child</strong>ren: experienceat a large referral teaching hospital. Nati<strong>on</strong>al MedicalJournal of India, 1998, 11:166–168.31. Akhtar S, Gulali RR, Al-Anezi F. Risk factors in acutepois<strong>on</strong>ing in <strong>child</strong>ren: a retrospective study. KuwaitMedical Journal, 2006, 38:33–36.32. Goldman L, Tran N. Toxics and poverty: the impact oftoxic substances <strong>on</strong> the poor in developing countries.Washingt<strong>on</strong>, DC, <str<strong>on</strong>g>World</str<strong>on</strong>g> Bank, 2002.33. Andiran N, Sarikayalar F. Pattern of acute pois<strong>on</strong>ings in<strong>child</strong>hood in Ankara: what has changed in twenty years?Turkish Journal of Pediatrics, 2004, 46:147–152.34. Burt A et al. N<strong>on</strong>fatal, unintenti<strong>on</strong>al medicati<strong>on</strong> exposuresam<strong>on</strong>g young <strong>child</strong>ren: United States, 2001–2003.Morbidity and Mortality Weekly Report, 2006, 55:1–5.35. Orisakwe O, Egenti L, Orish C. Childhood n<strong>on</strong>-drugpois<strong>on</strong>ing in Nnewi, Nigeria. Tropical Doctor, 2000,30:209–211.36. Ellis JB et al. Paraffin ingesti<strong>on</strong>: the problem. South AfricanMedical Journal, 1994, 84:727–730.37. de Wet B et al. Paraffin (kerosene) pois<strong>on</strong>ing in <strong>child</strong>hood:is preventi<strong>on</strong> affordable in South Africa? South AfricanMedical Journal, 1994, 84:735–738.38. Joubert PH. Pois<strong>on</strong>ing admissi<strong>on</strong>s of Black South Africans.Clinical Toxicology, 1990, 28:85–94.39. O’Brien KL et al. Epidemic of pediatric deaths fromacute renal failure caused by diethylene glycol pois<strong>on</strong>ing.Journal of the American Medical Associati<strong>on</strong>, 1998,279:1175–1180.40. Hydrocarb<strong>on</strong> pois<strong>on</strong>ing. Merck Manuals <strong>on</strong>line(http://www.merck.com/mmpe/sec21/ch326/ch326h.html?qt=glue%20sniffing&alt=sh, accessed 8 April 2008).41. Henao S, Arbelaez M. Epidemiologic situati<strong>on</strong> of acutepesticide pois<strong>on</strong>ing in Central America, 1992–2000.Epidemiology Bulletin, 2002, 23:5–9.42. Childhood pesticide pois<strong>on</strong>ing: informati<strong>on</strong> for advocacyand acti<strong>on</strong>. Geneva, Chemicals Programme of the UnitedNati<strong>on</strong>s Envir<strong>on</strong>ment Programme, Food and AgricultureOrganizati<strong>on</strong>, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2004 (http://www.who.int/entity/ceh/publicati<strong>on</strong>s/pestpois<strong>on</strong>ing.pdf,accessed 6 April 2008).43. McC<strong>on</strong>nell R, Hruska A. An epidemic of pesticidepois<strong>on</strong>ing in Nicaragua: Implicati<strong>on</strong>s for preventi<strong>on</strong> inWORLD REPORT ON CHILD INJURY PREVENTION 139
developing countries. American Journal of Public Health,1993, 83:1559–1562.44. Rosenthal E. The tragedy of Tauccamarca: a humanrights perspective <strong>on</strong> the pesticide pois<strong>on</strong>ing deaths of 24<strong>child</strong>ren in the Peruvian Andes. Internati<strong>on</strong>al Journal ofOccupati<strong>on</strong>al and Envir<strong>on</strong>mental Health, 2003, 9:53–58.45. Zhang P et al. A prospective study of accidental deathsam<strong>on</strong>g 0–14 year old <strong>child</strong>ren in Jiangsu 1994–1995(article in Chinese). Chinese Journal of Epidemiology,1998, 19:290–293.46. Scott D et al. N<strong>on</strong>-medicinal ingesti<strong>on</strong>s in Queensland<strong>child</strong>ren. Brisbane, Queensland Injury Surveillance Unit,2005 (Injury Bulletin No. 87).47. Unintenti<strong>on</strong>al n<strong>on</strong>-fire-related carb<strong>on</strong> m<strong>on</strong>oxideexposures: United States, 2001–2003. Morbidity andMortality Weekly Report, 2005, 54:36–39, 131–132.48. Riordan M, Rylance G, Berry K. Pois<strong>on</strong>ing in <strong>child</strong>ren 1:general management. Archives of Disease in Childhood,2002, 87:392–396.49. Woolf DA. Aetiology of acute lead encephalopathy inOmani infants. Journal of Tropical Pediatrics, 1990,36:328–330.50. Moya J. Ackee (Blighia sapida) pois<strong>on</strong>ing in the NorthernProvince, Haiti. PAHO Epidemiological Bulletin, 2001,22:8–9 (http://www.paho.org/english/sha/be_v22n2-ackee.htm, accessed 6 April 2008).51. Vashishtha VM et al. Cassia occidentalis pois<strong>on</strong>ing as theprobable cause of hepatomyoencephalopathy in <strong>child</strong>renin western Uttar Pradesh. Indian Journal of MedicalResearch, 2007, 125:756–762.52. Saddique A. Pois<strong>on</strong>ing in Saudi Arabia: a ten-yearexperience in King Khaled University Hospital. Annals ofSaudi Medicine, 2001, 21:88–91.53. Chippaux JP. Snake-bites: appraisal of the global situati<strong>on</strong>.Bulletin of the <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 1998, 76:515–524.54. Danseco ER, Miller TR, Spicer RS. Incidence and costs of1987–1994 <strong>child</strong>hood injuries: demographic breakdowns.Pediatrics, 2000, 105:E27.55. Krug A et al. The impact of <strong>child</strong>-resistant c<strong>on</strong>tainers <strong>on</strong>the incidence of paraffin (kerosene) ingesti<strong>on</strong> in <strong>child</strong>ren.South African Medical Journal, 1994, 84:730–734.56. Finkelstein EA, Corso PS, Miller TR. The incidence andec<strong>on</strong>omic burden of injuries in the United States. New York,NY, Oxford University Press, 2006.57. Durkin MS et al. Low-income neighborhoods and therisk of severe pediatric <strong>injury</strong>: a small-area analysis innorthern Manhattan. American Journal of Public Health,1994, 84:587–592.58. Griffiths C, Ro<strong>on</strong>ey C. The effect of the introducti<strong>on</strong> ofICD-10 <strong>on</strong> trends in mortality from <strong>injury</strong> and pois<strong>on</strong>ingin England and Wales. Health Statistics Quarterly, 2003,19:10–21.59. Cheng AC, Winkel KD. Snakebite and antivenoms in theAsia-Pacific: wokabaut wantaim, raka hebou (“walkingtogether”). Medical Journal of Australia, 2001, 175:648–651.60. Tchoua R et al. Analyse des envenimati<strong>on</strong>s par morsuresde serpent au Gab<strong>on</strong> [Analysis of snake bite envenomati<strong>on</strong>sin Gab<strong>on</strong>]. Bulletin of the Exotic Pathology Society,2002, 95:188–190.61. Kreisfeld R, Winkel KD, Harris<strong>on</strong> J. Hospitalisati<strong>on</strong>s dueto animal and plant <strong>injury</strong> in Australia 2000/01–2001/2.Canberra, Research Centre for Injury Studies, AustralianInstitute of Health and Welfare, 2007 (in press).62. O’Neill ME et al. Snakebite injuries treated in UnitedStates emergency departments, 2001–2004. Wildernessand Envir<strong>on</strong>mental Medicine, 2007, 18:281–287.63. McGain F et al. Snakebite mortality at Port MoresbyGeneral Hospital, Papua New Guinea, 1992–2001. MedicalJournal of Australia, 2004, 181:687–691.64. WHO mortality database: tables. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g>Health Organizati<strong>on</strong> (http://www.who.int/healthinfo/morttables/en/index.html, accessed 21 April 2008).65. Matteucci MJ et al. Pediatric sex group differences inlocati<strong>on</strong> of snakebite injuries requiring antivenom therapy.Journal of Medical Toxicology, 2007, 3:103–106.66. Linnan M et al. Child mortality and <strong>injury</strong> in Asia:survey results and evidence. Florence, UNICEF InnocentiResearch Centre, 2007 (http://www.unicef-irc.org/publicati<strong>on</strong>s/pdf/iwp_2007_06.pdf, accessed 21 January2008). (Innocenti Working Paper 2007-06, Special series<strong>on</strong> <strong>child</strong> <strong>injury</strong> No. 3).67. Lopoo JB et al. Treating the snake bitten <strong>child</strong> in NorthAmerica: a study of pit viper bite. Journal of PediatricSurgery, 1998, 33:1593–1595.68. Mars M, Hadley GP. Raised compartmental pressure in<strong>child</strong>ren: a basis for management. Injury, 1998, 29:183–185.69. Epidemiological notes and <str<strong>on</strong>g>report</str<strong>on</strong>g>s of unintenti<strong>on</strong>alingesti<strong>on</strong>s of prescripti<strong>on</strong> drugs in <strong>child</strong>ren under fiveyears old. Morbidity and Mortality Weekly Report, 1987,36:124–126, 131–132 (http://iier.isciii.es/mmwr/preview/mmwrhtml/00000884.htm, accessed 6 April 2008).70. Korb FA, Young MH. The epidemiology of accidentalpois<strong>on</strong>ing in <strong>child</strong>ren. South African Medical Journal,1985, 68:225–228.71. Cheng TL et al. The spectrum of intoxicati<strong>on</strong> and pois<strong>on</strong>ingam<strong>on</strong>g adolescents: surveillance in an urban populati<strong>on</strong>.Injury Preventi<strong>on</strong>, 2006, 12:129–132.72. Soori H. Developmental risk factors for unintenti<strong>on</strong>al<strong>child</strong>hood pois<strong>on</strong>ing. Saudi Medical Journal, 2001,22:227–230.73. Turrel G, Mathers C. Socioec<strong>on</strong>omic inequalities in allcauseand specific-cause mortality in Australia: 1985–1987and 1995–1997. Internati<strong>on</strong>al Journal of Epidemiology,2001, 30:231–239.140 WORLD REPORT ON CHILD INJURY PREVENTION
74. Roberts I. Cause specific mortality differentials for <strong>child</strong><strong>injury</strong> and pois<strong>on</strong>ing in England and Wales. Journal ofEpidemiology and Community Health, 1996, 51:334–335.75. Petridou E et al. Risk factors for <strong>child</strong>hood pois<strong>on</strong>ing:a case-c<strong>on</strong>trol study in Greece. Injury Preventi<strong>on</strong>, 1996,2:208–211.76. Dlamini N, Gqaleni N. The chemical compositi<strong>on</strong> andtoxicity of South African paraffin samples. Southern AfricanJournal of Epidemiology and Infecti<strong>on</strong>, 2006, 21:75–76.77. Gee P, Ardagh M. Paediatric exploratory ingesti<strong>on</strong>sof paracetamol. New Zealand Medical Journal, 1998,111:186–188.78. Abrahams N. Safe closures for paraffin. Trauma Review,1994, 2:5–6.79. Caelers D. City innocents drinking from the cup of death.Cape Argus, 13 August 2001:5.80. Ferrer A, Cabral R. Recent epidemics of pois<strong>on</strong>ing bypesticides. Toxicology Letters, 1995, 82–83:55–63.81. Ferguss<strong>on</strong> DM. A c<strong>on</strong>trolled field trial of a pois<strong>on</strong>ing preventi<strong>on</strong>method. Pediatrics, 1982, 69:515–620.82. Ozanne-Smith J et al. Childhood pois<strong>on</strong>ing: access andpreventi<strong>on</strong>. Journal of Paediatric Child Health, 2001,37:262–265.83. Wiseman HM et al. Accidental pois<strong>on</strong>ing in <strong>child</strong>hood: amulticentre survey and the role of packaging in accidentsinvolving medicati<strong>on</strong>s. Human Toxicology, 1987, 6:303–314.84. Child-resistant packaging saves lives. US C<strong>on</strong>sumerProduct Safety Commissi<strong>on</strong> [CPSC Document No. 5019](http://www.cpsc.gov/cpscpub/pubs/5019.html, accessed6 April 2008).85. Durham G. Code of practice for <strong>child</strong>-resistant packagingof toxic substances. Wellingt<strong>on</strong>, Ministry of Health, 1998.86. Preventing pois<strong>on</strong>ing in <strong>child</strong>ren. Indian Academy ofPaediatrics, Kerala State Branch (http://www.pediatricskerala.com/html/pois<strong>on</strong>ing.htm,accessed 6 April2008).87. Wezorek C, Dean B, Krenzelok E. Accidental <strong>child</strong>hoodpois<strong>on</strong>ing: influence of the type of caretaker <strong>on</strong> aetiologyand risk. Veterinary and Human Toxicology, 1998, 30:574–576.88. Amitai Y. Pois<strong>on</strong> exposure in <strong>child</strong>ren before Passover.Israeli Medical Associati<strong>on</strong> Journal, 2000, 2:142–144.89. Wils<strong>on</strong> RC, Saunders PJ, Smith G. An epidemiologicalstudy of acute carb<strong>on</strong> m<strong>on</strong>oxide pois<strong>on</strong>ing in the WestMidlands. Occupati<strong>on</strong>al and Envir<strong>on</strong>mental Medicine,1998, 55:723–728.90. Jolly DL, Moller JN, Volkmer RE. The socio-ec<strong>on</strong>omicc<strong>on</strong>text of <strong>child</strong> <strong>injury</strong> in Australia. Journal of Paediatricsand Child Health, 1993, 29:438–444.91. Azizi BH, Zulkifli HI, Kasim MS. Risk factors for accidentalpois<strong>on</strong>ing in urban Malaysian <strong>child</strong>ren. Annals ofTropical Paediatrics, 1993, 13:183–188.92. Reed RP, C<strong>on</strong>radie FM. The epidemiology and clinicalfeatures of paraffin (kerosene) pois<strong>on</strong>ing in rural African<strong>child</strong>ren. Annals of Tropical Paediatrics, 1997, 17:49–55.93. Caribbean Epidemiology Centre (CAREC). Epidemiologyof pois<strong>on</strong>ing in CAREC-member countries. CARECSurveillance Report, 1986, 12:2–3.94. Global strategic framework for integrated vectormanagement. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2004(http://whqlibdoc.who.int/hq/2004/WHO_CDS_CPE_PVC_2004_10.pdf, accessed 7 April 2008).95. J<strong>on</strong>es AL et al. Should methi<strong>on</strong>ine be added to everyparacetamol tablet? British Medical Journal, 1997, 315:301–304.96. CPSC requires <strong>child</strong>-resistant packaging for comm<strong>on</strong>household products c<strong>on</strong>taining hydrocarb<strong>on</strong>s, includingsome baby oils. US C<strong>on</strong>sumer Product Safety Commissi<strong>on</strong>(http://www.cpsc.gov/cpscpub/prerel/prhtml02/02015.html, accessed 6 April 2008).97. Walt<strong>on</strong> WW. An evaluati<strong>on</strong> of the Pois<strong>on</strong> Preventi<strong>on</strong>Packaging Act. Paediatrics, 1982, 69:363–370.98. O’D<strong>on</strong>nell J, Brown FD, Beattie TF. Accidental <strong>child</strong>pois<strong>on</strong>ing: <strong>child</strong> resistant packaging should be used <strong>on</strong>all over the counter drugs. British Medical Journal, 1998,316:1460–1461.99. Schneider KC. Preventi<strong>on</strong> of accidental pois<strong>on</strong>ing throughpackage and label design. Journal of C<strong>on</strong>sumer Research,1977, 4:67–74.100. Matzopoulos R, Carolissen G. Estimating the incidence ofparaffin ingesti<strong>on</strong>. African Safety Promoti<strong>on</strong>: a Journal ofInjury and Violence Preventi<strong>on</strong>, 2006, 3:4–14.101. Pearn J et al. Accidental pois<strong>on</strong>ing in <strong>child</strong>hood: five yearurban populati<strong>on</strong> study with 15 year analysis of fatalities.British Medical Journal (Clinical Research Editi<strong>on</strong>), 1984,288:44–46.102. Sibert JR, Frude N. Bittering agents in the preventi<strong>on</strong> ofaccidental pois<strong>on</strong>ing: <strong>child</strong>ren’s reacti<strong>on</strong>s to denat<strong>on</strong>iumbenzoate (Bitrex). Archives of Emergency Medicine, 1991,8:1–7.103. Klein-Schwartz W. Denat<strong>on</strong>ium benzoate: review ofefficacy and safety. Veterinary and Human Toxicology,1991, 33:545–547.104. Vernberg K, Culver-Dickins<strong>on</strong> P, Spyker DA. The deterrenteffect of pois<strong>on</strong>-warning stickers. American Journal ofDiseases of Children, 1984, 138:1018–1020.105. Best practices: pois<strong>on</strong>ing interventi<strong>on</strong>s. Harborview InjuryPreventi<strong>on</strong> Research Centre (http://depts.washingt<strong>on</strong>.edu/hiprc/practices/topic/pois<strong>on</strong>ing/packaging.html,accessed 6 April 2008).106. O’Brien C. Pediatric pois<strong>on</strong>ing fatalities from 1972 to 2005.Bethesda, MD, US C<strong>on</strong>sumer Product Safety Commissi<strong>on</strong>,2008 (http://www.cpsc.gov/library/pppa2005.pdf,accessed 8 April 2008).107. SI No. 462/2998 – European Communities (Dangeroussubstances and preparati<strong>on</strong>s) (Marketing and use)WORLD REPORT ON CHILD INJURY PREVENTION 141
Regulati<strong>on</strong>s. European Commissi<strong>on</strong>, 1998 (http://www.irishstatutebook.ie/1998/en/si/0462.html, accessed 6 April2008).108. Turvill JL, Burroughs AK, Moore KP. Change in occurrenceof paracetamol overdose in UK after introducti<strong>on</strong> of blisterpacks. The Lancet, 2000, 355:2048–2049.109. McFee RB, Caraccio TR. Hang up your pocketbook: aneasy interventi<strong>on</strong> for the granny syndrome. Grandparentsas a risk factor in unintenti<strong>on</strong>al pediatric exposures topharmaceuticals. Journal of the American OsteopathicAssociati<strong>on</strong>, 2006, 106:405–411.110. D<strong>on</strong>ald PR, Bezuidenhout CJ, Camer<strong>on</strong> NA. Aneducati<strong>on</strong>al campaign in the Cape Town area to preventparaffin pois<strong>on</strong>ing [Corresp<strong>on</strong>dence]. South AfricanMedical Journal, 1991, 79:281–282.111. Woolf AD, Saperstein A, Forjuoh S. Pois<strong>on</strong>ing preventi<strong>on</strong>knowledge and practices of parents after a <strong>child</strong>hoodpois<strong>on</strong>ing incident. Pediatrics, 1992, 90:867–870.112. Gielen AC et al. In-home <strong>injury</strong> preventi<strong>on</strong> practices.Health Educati<strong>on</strong> Quarterly, 1995, 22:85–95.113. Nix<strong>on</strong> J et al. Community based programs to preventpois<strong>on</strong>ing in <strong>child</strong>ren 0–15 years. Injury Preventi<strong>on</strong>, 2004,10:43–46.114. Roberts I, Kramer MS, Suissa S. Does home visiting prevent<strong>child</strong>hood <strong>injury</strong>? A systematic review of randomisedc<strong>on</strong>trol trials. British Medical Journal, 1996, 312:29–33.115. O’C<strong>on</strong>nor PJ. Pois<strong>on</strong>ing preventi<strong>on</strong>: results of a publicmedia campaign. Australian Paediatric Journal, 1982,18:250–252.116. Kendrick D et al. Effect of educati<strong>on</strong> and safety equipment<strong>on</strong> pois<strong>on</strong>ing-preventi<strong>on</strong> practices and pois<strong>on</strong>ing: asystematic review, meta-analysis and meta-regressi<strong>on</strong>.Archives of Disease in Childhood, 2008, 93:599–608.117. Pois<strong>on</strong>ing: general principles. Merck Manuals <strong>on</strong>line(http://www.merck.com/mmpe/sec21/ch326/ch326b.html, accessed 6 April 2008).118. Miller T, Lestina D. Costs of pois<strong>on</strong>ing in the UnitedStates and savings from pois<strong>on</strong> c<strong>on</strong>trol centers: a costbenefit analysis. Annals of Emergency Medicine, 1997,29:239–245.119. Clarke EEK. The experience of starting a pois<strong>on</strong> c<strong>on</strong>trolcentre in Africa: the Ghana experience. Toxicology, 2004,108:267–272.120. Makalinao I, Awang R. Pois<strong>on</strong> c<strong>on</strong>trol centers indeveloping countries and Asia’s need for toxicologyeducati<strong>on</strong>. Toxicology, 2005, 207(2 Suppl):S716–S721.121. Ravindra F. The Nati<strong>on</strong>al Pois<strong>on</strong>s Informati<strong>on</strong> Centre inSri Lanka: the first ten years. Clinical Toxicology, 2002,40:551–555.122. Pois<strong>on</strong>ous persuaders: safe packaging to reduce <strong>child</strong> pois<strong>on</strong>ingat home (the Netherlands). Copenhagen, <str<strong>on</strong>g>World</str<strong>on</strong>g> HealthOrganizati<strong>on</strong> Regi<strong>on</strong>al Office for Europe, 2006 (http://www.euro.who.int/<strong>child</strong>healthenv/studies/20060130_1,accessed 7 April 2008).123. Sethi D et al. Injuries and violence in Europe: why theymatter and what can be d<strong>on</strong>e. Copenhagen, <str<strong>on</strong>g>World</str<strong>on</strong>g> HealthOrganizati<strong>on</strong> Regi<strong>on</strong>al Office for Europe, 2006.124. Nort<strong>on</strong> R et al. Unintenti<strong>on</strong>al injuries. In: Jamis<strong>on</strong> DT etal., eds. Disease c<strong>on</strong>trol priorities in developing countries,2nd ed. New York, Oxford University Press, 2006:737–753(http://files.dcp2.org/pdf/DCP/DCP39.pdf, accessed 7 April2008).125. Runyan CW, Freire KE. Developing interventi<strong>on</strong>s whenthere is little science. In: Doll LS et al., eds. Handbookof <strong>injury</strong> and violence preventi<strong>on</strong>. Atlanta, GA, Springer,2007.126. MacKay M et al. Child safety good practice guide: goodinvestments in unintenti<strong>on</strong>al <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> andsafety promoti<strong>on</strong>. Amsterdam, European Child SafetyAlliance, Eurosafe, 2006.127. Litovitz T, White N, Wats<strong>on</strong> W. Epidemiology of pediatricpois<strong>on</strong> exposures: an analysis of 2003 pois<strong>on</strong> c<strong>on</strong>trolcenter data. Clinical Pediatric Emergency Medicine, 2005,6:68–75.128. Ozanne-Smith J et al. Pharmaceutical pois<strong>on</strong>ing to0 –19 year olds. Melbourne, M<strong>on</strong>ash University AccidentResearch Centre, 2002 (Report No. 193) (http://www.m<strong>on</strong>ash.edu.au/muarc/<str<strong>on</strong>g>report</str<strong>on</strong>g>s/muarc193.pdf, accessed5 July 2008).142 WORLD REPORT ON CHILD INJURY PREVENTION
WORLD REPORT ON CHILD INJURY PREVENTION 143
CONCLUSIONANAPUMA’S STORY© M Kokic, WHOChildren are powerful agents of change and should be includedduring the development and implementati<strong>on</strong> of <strong>child</strong> <strong>injury</strong>preventi<strong>on</strong> projects at local, nati<strong>on</strong>al and internati<strong>on</strong>al levels.The following is an essay written by sixteen-year-old Anupama Kumar of Kerala,India. She w<strong>on</strong> the UNICEF Voices of the Youth road safety essay competiti<strong>on</strong>and received her award during the <str<strong>on</strong>g>World</str<strong>on</strong>g> Youth Assembly, held at the Palais desNati<strong>on</strong>s of the United Nati<strong>on</strong>s in Geneva, Switzerland in April 2007.“1.2 milli<strong>on</strong> die in road accidents each year. A <strong>child</strong> is killed in an accident everythree minutes. Road safety is increasingly becoming a major killer and a worldwidec<strong>on</strong>cern, particularly for young people. What can we do to address the issue?The media has been a largely overlooked factor in creating road safety awareness.Celebrity endorsements, coupled with televisi<strong>on</strong> messages <strong>on</strong> prime-time slotsand peer educati<strong>on</strong> programmes would provide an accessible and engaging meansof promoting awareness, particularly am<strong>on</strong>g young people. They would c<strong>on</strong>veythe message that safe driving is “cool” driving, and c<strong>on</strong>stantly reinforce thatdrunken driving, using a cell ph<strong>on</strong>e <strong>on</strong> the road and driving without a seat-belt (orhelmet) are not <strong>on</strong>ly dangerous, but “seriously unfashi<strong>on</strong>able”. Celebrities couldalso actively encourage walking or cycling whenever and wherever possible.Role-plays, “make-believe” situati<strong>on</strong>s, movies and field trips could be used aseffective learning tools for <strong>child</strong>ren at school. Safe Road User awards at theschool level would provide an incentive for many <strong>child</strong>ren to follow road safetyrules. Road safety educati<strong>on</strong> programmes can also be extended to adults at theworkplace, particularly those from disadvantaged backgrounds. This would holdparticular importance for parents, and efforts must be made to involve them asmuch as possible.There is a need for stricter licensing laws, particularly with regard to publictransport operators. Laws could require prominent display of the driver’s licence<strong>on</strong> his or her vehicle while driving, in additi<strong>on</strong> to safety regulati<strong>on</strong>s (such asadequate maintenance and the use of the seat-belt) and random breath testingpolicies. Policies could provide for the creati<strong>on</strong> of better roads and pavements,supervised playing areas for <strong>child</strong>ren and m<strong>on</strong>itored crossings near schools.Citizens must campaign for safer,wider roads and better sidewalks tolimit accidents. Speed governors ineach vehicle would provide a low-costsoluti<strong>on</strong> to speeding. There is also aneed to provide well-maintained, safeand efficient public transport systems,particularly in developing nati<strong>on</strong>s.Fingerprint identificati<strong>on</strong> systems,similar to those in laptop computers,could be used in each vehicle, witheach vehicle resp<strong>on</strong>ding <strong>on</strong>ly to aprogrammed set of fingerprints.For any effective change in thesafety of our roads, however, weneed to c<strong>on</strong>sciously change ourattitudes towards providing saferroads – not just for ourselvesor for young people, but forevery<strong>on</strong>e.”
CHAPTER 7 – CONCLUSION AND RECOMMENDATIONSChapter 7C<strong>on</strong>clusi<strong>on</strong> and recommendati<strong>on</strong>sIntroducti<strong>on</strong>Earlier chapters have discussed in detail the nature andobjectives of <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>. In additi<strong>on</strong>, foreach of the five leading causes of unintenti<strong>on</strong>al injuriesincurred during <strong>child</strong>hood, the magnitude of the problem,the risk factors and the specific interventi<strong>on</strong>s have beendescribed. This chapter brings together the main points ofthe <str<strong>on</strong>g>report</str<strong>on</strong>g> and presents a set of generic recommendati<strong>on</strong>sthat governments and others involved in the field of <strong>child</strong><strong>injury</strong> should c<strong>on</strong>sider using to develop their nati<strong>on</strong>alor local strategies to prevent <strong>child</strong> <strong>injury</strong>. The chapterc<strong>on</strong>cludes with suggesti<strong>on</strong>s as to how those c<strong>on</strong>cernedwith the issue, including the <strong>child</strong>ren themselves, couldbecome more involved in <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>.Main messages from the <str<strong>on</strong>g>report</str<strong>on</strong>g>This <str<strong>on</strong>g>report</str<strong>on</strong>g>, the first world <str<strong>on</strong>g>report</str<strong>on</strong>g> <strong>on</strong> the topic of <strong>child</strong>injuries, presents the current knowledge about the fivemost important causes of unintenti<strong>on</strong>al <strong>injury</strong> to <strong>child</strong>renunder the age of 18 years as well as some of the acti<strong>on</strong>sthat need to be taken in order to tackle the problem. Thefollowing are the <str<strong>on</strong>g>report</str<strong>on</strong>g>’s main messages.Child injuries are a major public health issueInjuries mar the lives of milli<strong>on</strong>s of young people andtheir families each year. The <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>estimates that, in 2004, around 830 000 <strong>child</strong>ren under theage of 18 years died as a result of an unintenti<strong>on</strong>al <strong>injury</strong>.Recent community-based studies c<strong>on</strong>ducted by UNICEF,however, have suggested that the number could be muchhigher. Tens of milli<strong>on</strong>s more <strong>child</strong>ren are n<strong>on</strong>-fatallyinjured and many of these require hospital treatment. Forsurvivors, the impairment that injuries can cause and theresulting need for care and rehabilitati<strong>on</strong> have far-reachingimpacts <strong>on</strong> a <strong>child</strong>’s prospects for health, educati<strong>on</strong> andsocial inclusi<strong>on</strong> and <strong>on</strong> their parents’ livelihood.The unequal burden of <strong>injury</strong> is an additi<strong>on</strong>al reas<strong>on</strong>to address the problem. Children in poorer countriesand those from poorer families in better-off countriesare the most vulnerable. More than 95% of <strong>injury</strong> deathsam<strong>on</strong>g <strong>child</strong>ren occur in low-income and middle-incomecountries. Approximately 40% of the deaths am<strong>on</strong>g thoseunder 18 years of age in high-income countries are the resultof an <strong>injury</strong> – an indicati<strong>on</strong> of the fact that these countries,although doing better, still have a serious problem.If countries do not address their <strong>child</strong> <strong>injury</strong> problem itis likely to escalate and as a result, unnecessary lives willbe lost to causes that are largely preventable.Injuries directly affect <strong>child</strong> survivalSpecific c<strong>on</strong>cern for the lives, health and well-being of<strong>child</strong>ren is voiced in a series of internati<strong>on</strong>al agreementsand initiatives. Most notable of these is the C<strong>on</strong>venti<strong>on</strong><strong>on</strong> the Rights of the Child, adopted in November1989 during a sessi<strong>on</strong> of the United Nati<strong>on</strong>s GeneralAssembly, which affirms that each <strong>child</strong> has the rightto the highest attainable level of health and the rightto a safe envir<strong>on</strong>ment. The C<strong>on</strong>venti<strong>on</strong> requires that“all appropriate legislative, administrative, social andeducati<strong>on</strong>al measures to protect the <strong>child</strong> from all formsof physical or mental violence, <strong>injury</strong> or abuse, neglector negligent treatment, maltreatment or exploitati<strong>on</strong>,including sexual abuse” are taken by countries (1). Mostcountries in the world have ratified this c<strong>on</strong>venti<strong>on</strong>, andit represents a powerful statement of their collectiveviews <strong>on</strong> the resp<strong>on</strong>sibilities towards <strong>child</strong>ren.In additi<strong>on</strong>, the fourth objective of the MillenniumDevelopment Goals is to reduce by two thirds themortality of <strong>child</strong>ren under five years of age by theyear 2015 (2). Most countries are focusing <strong>on</strong> reducinginfectious diseases. However, in many places the relativeproporti<strong>on</strong> of deaths as a result of injuries in this agegroup is significant enough to hamper the attainment ofthe goal if it is not addressed at the same time.Child survival has been described as “the most pressingmoral dilemma of the new millennium” (3). As injuriesare a leading cause of death and disability am<strong>on</strong>g <strong>child</strong>renworldwide, to prevent those injuries is particularlyimportant for the wider issue of <strong>child</strong> survival and theimprovement globally of <strong>child</strong> health. Injury programmesneed to be integrated into other <strong>child</strong> health strategies,with ministries of health playing a pivotal role. In additi<strong>on</strong>,injuries need to be included as <strong>on</strong>e of the indicators inoverall <strong>child</strong> survival programmes.Children are susceptible to injuriesThere is a str<strong>on</strong>g associati<strong>on</strong> between the stage of lifeand the type of injuries sustained by a <strong>child</strong>. The ageof a <strong>child</strong>, the stage of his or her development, how the<strong>child</strong> interacts with the world, and the type of activitiesthe <strong>child</strong> undertakes are all relevant to this associati<strong>on</strong>.Am<strong>on</strong>g infants, for instance, fires, drowning and falls arethe leading causes of <strong>injury</strong> death. Am<strong>on</strong>g 1–4-year-olds,as <strong>child</strong>ren start to move more independently, drowningbecomes the leading cause of <strong>injury</strong>-related death inmany places, followed by road traffic crashes and fires –the three of which combined accounting for almost twoWORLD REPORT ON CHILD INJURY PREVENTION 145
thirds of <strong>injury</strong> deaths in that age group. Over the age offive years, road traffic injuries, drowning and fires are thepredominant causes.In additi<strong>on</strong> to these biological factors, there areother risk factors for <strong>child</strong> injuries. These includesocioec<strong>on</strong>omic factors such as poverty, the absence ofprotective factors, and the envir<strong>on</strong>ment in which <strong>child</strong>renlive. The quality, availability and access to medical careare important factors that can influence not <strong>on</strong>ly thelikelihood of surviving an <strong>injury</strong> but also the l<strong>on</strong>g-termc<strong>on</strong>sequences.“We have a duty to protect <strong>child</strong>ren from <strong>injury</strong> and violence. Childrenlive in a world designed for adults, but they have special needs and aremore vulnerable than adults to certain factors in their envir<strong>on</strong>mentwhich may place them at additi<strong>on</strong>al risk of <strong>injury</strong>” Ann M. Veneman,Executive Director, UNICEF.Child injuries can be preventedSimply reproducing safe strategies that are relevant toadults will not protect <strong>child</strong>ren sufficiently. Variousdevelopmental issues, risk taking behaviours, levelsof activity and the <strong>child</strong>’s degree of dependence makethe matter more complicated. Preventi<strong>on</strong> programmesthat take into account these vulnerabilities and use amultidisciplinary approach have been shown to be themost effective for reducing <strong>child</strong> mortality as a result of<strong>injury</strong>. A number of countries have achieved remarkablereducti<strong>on</strong>s in their <strong>child</strong> <strong>injury</strong> death rates, in some casesby more than 50% (see Box 7.1).There is no single blueprint for success but six basicprinciples underlie most of the successful <strong>child</strong> <strong>injury</strong>preventi<strong>on</strong> programmes around the world. These are:– legislati<strong>on</strong> and regulati<strong>on</strong>s, and their enforcement;– product modificati<strong>on</strong>;BOX 7.1How did Sweden achieve its reducti<strong>on</strong>s in <strong>child</strong> injuries?Since the early 1950s, Sweden has seen a reducti<strong>on</strong> in <strong>child</strong> injuries, champi<strong>on</strong>ed largely by the paediatrician Dr Ragnar Berfenstam (4). In 1969 the<strong>injury</strong> death rate in Sweden for boys and girls under the age of 18 years was 24 per 100 000 and 11 per 100 000 <strong>child</strong>ren, respectively. Over the lastthree decades, Sweden has been able to bring the rates down to 5 per 100 000 for boys and 3 per 100 000 for girls. These dramatic reducti<strong>on</strong>s havebeen achieved using a range of approaches cutting across several sectors, and involving <strong>child</strong>ren and the community.The health sector played an important and leading role in the initiati<strong>on</strong> and follow-up <strong>on</strong> a wide range of acti<strong>on</strong>s which included:– envir<strong>on</strong>mental planning: traffic was diverted away from residential areas and towns so that <strong>child</strong>ren could walk to school, play and return homewithout encountering busy streets; Sweden had originated the idea of Safe Communities l<strong>on</strong>g before it was taken up by others;– measures against drowning: much of the early reducti<strong>on</strong> in <strong>child</strong> <strong>injury</strong> was attributed to water safety interventi<strong>on</strong>s; rates am<strong>on</strong>g <strong>child</strong>ren aged0–14 years fell from 8 per 100 000 in 1951 to 1 per 100 000 <strong>child</strong>ren in 1985 (4);– safety measures in the home;– home visits by health professi<strong>on</strong>als;– traffic safety measures – such as helmets and <strong>child</strong>-restraints – taking into account the limited capacity of small <strong>child</strong>ren to adopt safe practicesin traffic;– improved product safety and standards;– improved health care services for <strong>child</strong>ren;– safety measures at school.TRENDS IN CHILD INJURIES, SWEDEN, 1969–1999Rate per 100 000 <strong>child</strong>ren30252015105BoysGirls01969 1974 1979 1984 1989 1994 1999Source: Laflamme, Karolinska Institute, Sweden.146 WORLD REPORT ON CHILD INJURY PREVENTION
– envir<strong>on</strong>mental modificati<strong>on</strong>;– supportive home visits;– the promoti<strong>on</strong> of safety devices;– educati<strong>on</strong> and the teaching of skills.In countries where the greatest reducti<strong>on</strong>s havebeen recorded, a combinati<strong>on</strong> of these approaches hasbeen employed. In additi<strong>on</strong>, countries that encouragea culture of safety and display str<strong>on</strong>g political commitmenthave made great progress in reducing their <strong>child</strong><strong>injury</strong> burden.As important as the idea of “what works” is the noti<strong>on</strong>of “what to avoid”. Certain preventi<strong>on</strong> strategies have beentested in high-income countries and found to have nobeneficial effects. There are some that even have negativec<strong>on</strong>sequences. Countries planning <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>programmes should be aware of these dangers.Furthermore, a reliance <strong>on</strong> the single, stand-al<strong>on</strong>e <strong>injury</strong>preventi<strong>on</strong> strategy of educating <strong>child</strong>ren (or their parents)in order to change <strong>child</strong>ren’s behaviour – while comm<strong>on</strong>– is sadly misplaced. This is not to say that educati<strong>on</strong> isunnecessary. It is indeed a valuable comp<strong>on</strong>ent that shouldbe incorporated into most <strong>injury</strong> preventi<strong>on</strong> strategies, anda useful tool to encourage the use of passive measures –acti<strong>on</strong>s that people have to do themselves, such as putting<strong>on</strong> a helmet. However, there is no evidence to show thateducati<strong>on</strong> <strong>on</strong> its own can reduce injuries.Child <strong>injury</strong> preventi<strong>on</strong> strategies should be based <strong>on</strong>available evidence (see Table 7.1). Interventi<strong>on</strong>s shouldbe prioritized after c<strong>on</strong>sidering the scale of the problem,and the known effectiveness, cost-effectiveness and cost ofeach interventi<strong>on</strong>.“Evidence is the foundati<strong>on</strong> for setting priorities, crafting policies, andmeasuring results. Evidence can have great persuasive power at thepolicy level.” Dr Margaret Chan, WHO Director-General.The cost of doing nothing is unacceptableFor many parents, the grief of losing a <strong>child</strong> unexpectedlycan take decades to heal and for many it never does. Forsome families the emoti<strong>on</strong>al pain is even greater if simplemeasures could have been taken to prevent the incident.Even if the outcome is not fatal, the medical costs and thespecial care that is often needed for a severely injured ordisabled <strong>child</strong> can put a huge financial demand <strong>on</strong> parentsand cause great difficulties for families or caretakers.In additi<strong>on</strong> to what parents, siblings, families andcommunities have to endure, <strong>child</strong> injuries also placea significant strain <strong>on</strong> often overstretched health caresystems. The cost of primary preventi<strong>on</strong> programmesis much cheaper than treating a <strong>child</strong>, sometimes form<strong>on</strong>ths, because of a preventable <strong>injury</strong>. Many wealthiercountries have already implemented cost-effective primarypreventi<strong>on</strong> programmes that have led to a reducti<strong>on</strong> inhealth-care costs. In the United States, for instance, ithas been estimated that for every <strong>on</strong>e US dollar spent <strong>on</strong>a <strong>child</strong> car seat, there is a saving of 29 dollars in directand indirect health care costs and other costs to society.If similarly effective interventi<strong>on</strong>s to prevent <strong>child</strong> <strong>injury</strong>TABLE 7.1Key approaches to addressing <strong>child</strong> injuriesKey approaches Trafc Drowning Burns Falls Pois<strong>on</strong>ingLegislati<strong>on</strong>, Speed limits; Four-sided pool Hot water tap Playground Manufacture, storageregulati<strong>on</strong>s and comprehensive fencing temperature equipment and distributi<strong>on</strong> ofenforcement drink-driving laws; legislati<strong>on</strong>; standards harmful substances<strong>child</strong> restraints smoke alarms requiring safepackagingProduct Vehicle-fr<strong>on</strong>t Pers<strong>on</strong>al flotati<strong>on</strong> N<strong>on</strong>-tip lanterns Baby walker Medicati<strong>on</strong> packaging;modicati<strong>on</strong> modificati<strong>on</strong>; devices and candle modificati<strong>on</strong>; <strong>child</strong> resistant closures<strong>child</strong> restraint holders safety glasssystemsEnvir<strong>on</strong>mental Child friendly Barriers – such as Separati<strong>on</strong> of Window guards Safe storage ofmodicati<strong>on</strong> infrastructure; well coverings and cooking area <strong>on</strong> tall buildings; potentially harmfulsafer routes to fencing from living area roof railings; substancesschool; safer playn<strong>on</strong>-climbablespacesbanistersEducati<strong>on</strong> Helmet wearing; Swimming training First aid – “cool Supportive home Immediate first aidand skills using <strong>child</strong> and supervisi<strong>on</strong> the burn” visitati<strong>on</strong> todevelopment restraints identify fallhazardsEmergency Child-sized Immediate Burns centres Appropriate Pois<strong>on</strong> c<strong>on</strong>trol centresmedical care equipment; <strong>child</strong>- resuscitati<strong>on</strong> paediatric acutefriendly envir<strong>on</strong>mentcareWORLD REPORT ON CHILD INJURY PREVENTION 147
were implemented around the world, many thousands oflives would be saved (see Box 7.2). Injury preventi<strong>on</strong> canthus be a very cost-effective public health strategy, with thecosts of interventi<strong>on</strong>s often much lower than the costs ofthe c<strong>on</strong>sequences of <strong>injury</strong>.“…We cannot accept these injuries as just accidents that will happen. Ifa disease were killing our <strong>child</strong>ren at the rate that unintenti<strong>on</strong>al injuriesare, the public would be unbelievably outraged and demand that thiskiller be stopped.” Former United States Surge<strong>on</strong> General, C. EverettKoop, 2001.Few countries have good data <strong>on</strong> <strong>child</strong> <strong>injury</strong>Data <strong>on</strong> <strong>injury</strong> and its determinants are essential foridentifying priority issues and high-risk groups, and alsofor understanding the underlying causes of <strong>injury</strong>. Inadditi<strong>on</strong>, agreement <strong>on</strong> the definiti<strong>on</strong>s of specific injuriesis essential for accurate measurement and comparability.The availability of good quality data and of trained peopleto analyse such data are therefore important in the searchfor effective preventi<strong>on</strong> interventi<strong>on</strong>s (see Box 7.3). By thesame token, a lack of data can hold back acti<strong>on</strong> for want ofevidence, prevent priorities from being correctly set, andhamper research and the evaluati<strong>on</strong> of interventi<strong>on</strong>s.In developed countries, detailed analysis of sound datahas undoubtedly been instrumental in achieving high ratesof success in <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>. Elsewhere, data <strong>on</strong><strong>child</strong> death and <strong>injury</strong> are generally either of a poor qualityor missing. Furthermore, discrepancies in data collectedare sometimes used as excuses not to do anything, wherethey could instead serve as a foundati<strong>on</strong> to strengtheninformati<strong>on</strong> systems.A major difficulty in <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>, as withall <strong>injury</strong> preventi<strong>on</strong>, is obtaining reliable estimates ofthe scale and pattern of <strong>child</strong> <strong>injury</strong> and death. To thisend, the volume, quality and availability of nati<strong>on</strong>al andregi<strong>on</strong>al data needs to be increased through a combinati<strong>on</strong>of:– better data collecti<strong>on</strong> systems;– improved surveillance;– use of hospital discharge systems (including ICDexternal cause codes);– more community-based surveys <strong>on</strong> <strong>child</strong> <strong>injury</strong> (usingstandard protocols).Research <strong>on</strong> <strong>child</strong> injuries is too limitedReducti<strong>on</strong>s in <strong>child</strong> <strong>injury</strong> mortality have beenachieved in some developed countries as a result of theapplicati<strong>on</strong> of evidence-based programmes based <strong>on</strong>rigorous research and priority-setting. Unfortunately,such research is not widespread even in all high-incomecountries and is particularly limited in low-income andmiddle-income countries, resulting in a significant gapin knowledge.BOX 7.2Saving 1000 <strong>child</strong>ren a dayIn 2002 more than 875 000 <strong>child</strong>ren died from preventable injurieswhile milli<strong>on</strong>s more were injured or permanently disabled. Manyof these injuries, such as pois<strong>on</strong>ings, falls, and burns, occurred in ornear the home. Others, including those caused by road traffic crashes,occurred as <strong>child</strong>ren were <strong>on</strong> their way to school or during other activities.Household and envir<strong>on</strong>mental factors also c<strong>on</strong>tribute to theoverall risk of <strong>child</strong>hood <strong>injury</strong>.In the past several decades, significant progress has been madein understanding better the epidemiology of injuries in <strong>child</strong>ren. Developingeffective interventi<strong>on</strong>s to prevent these injuries, however,has not progressed as far. A number of interventi<strong>on</strong> strategies – includingthe use of helmets, seat-belts, and pool fences – have beenshown to be effective at preventing <strong>injury</strong>-related deaths in <strong>child</strong>ren.Sadly though, the benefits of these interventi<strong>on</strong>s have not been fullyrealized in many places. As a c<strong>on</strong>sequence, hundreds of thousands of<strong>child</strong>ren die every year.To highlight what can be achieved through effective interventi<strong>on</strong>s,a comprehensive review of preventi<strong>on</strong> strategies for <strong>child</strong>hoodinjuries was carried out, quantifying their unrealized benefitsin terms of the number of <strong>child</strong>ren’s lives saved (5). More than 80studies and 46 interventi<strong>on</strong>s were reviewed, from which quantifiableeffectiveness data <strong>on</strong> 12 interventi<strong>on</strong> strategies for <strong>injury</strong> preventi<strong>on</strong>am<strong>on</strong>g <strong>child</strong>ren were identified. These strategies related to unintenti<strong>on</strong>al<strong>child</strong>hood injuries from road traffic, pois<strong>on</strong>ing, drowning, andburns. Data <strong>on</strong> the effectiveness of these particular interventi<strong>on</strong>swere then applied to the global burden of fatal <strong>child</strong> injuries.Am<strong>on</strong>g these interventi<strong>on</strong>s, the use of fences or other barrierspreventing access to water bodies al<strong>on</strong>e could save more than 50 000lives of young <strong>child</strong>ren each year. Similarly over 50 000 deaths fromfire-related burns are potentially preventable using smoke detectors.On a lower scale, the use of <strong>child</strong>-proof c<strong>on</strong>tainers could preventnearly 5000 deaths from kerosene pois<strong>on</strong>ing.For road traffic injuries, better data allow the modelling of moreinterventi<strong>on</strong>s. A very promising interventi<strong>on</strong> is the strengthening oftraffic codes and fines, including the suspensi<strong>on</strong> of licences for trafficviolati<strong>on</strong>s, which could save 80 000 <strong>child</strong>ren’s lives annually. The useof motorcycle or bicycle helmets for <strong>child</strong>ren, daytime running lightsfor motorcycles, speed reducti<strong>on</strong> measures, and <strong>child</strong> restraints canpotentially save between 30 000 and 40 000 lives each if implementedal<strong>on</strong>e, however, the combined effect of these interventi<strong>on</strong>s is notyet quantifiable.Current data do not allow refined estimati<strong>on</strong>s of the potentialbenefits of a package of interventi<strong>on</strong>s for <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>– a research agenda for the future. However, crude estimates indicatethat if a set of 12 interventi<strong>on</strong> strategies (which have beentested in a wide range of settings) covering road traffic, drowning,pois<strong>on</strong>ing and burns were implemented around the world, morethan 1000 <strong>child</strong>ren’s lives could be saved each day.While the urgent need to research new interventi<strong>on</strong> strategies forpreventing <strong>injury</strong> deaths in <strong>child</strong>ren remains, this study has shownthe huge benefits that can be realized by implementing interventi<strong>on</strong>sthat have already been tried and tested. While the estimate obtainedof the potential benefits of interventi<strong>on</strong>s to prevent <strong>child</strong> injuries is asomewhat crude <strong>on</strong>e – due to limitati<strong>on</strong>s in the data available – theover-all message is clear: <strong>child</strong>ren all over the world are needlesslydying as a result of unintenti<strong>on</strong>al injuries for which there are knowninterventi<strong>on</strong>s.Source: reference 5.148 WORLD REPORT ON CHILD INJURY PREVENTION
BOX 7.3The Canadian Hospitals Injury Reporting and Preventi<strong>on</strong> Program (CHIRPP)CHIRPP is an emergency department-based <strong>injury</strong> surveillance programme operated by the Public Health Agency of Canada (PHAC) in collaborati<strong>on</strong>with 14 hospitals (6). The programme began in 1990 within Canada’s ten <strong>child</strong>ren’s hospitals. Although several general hospitals now participate, asof October 2007, 84% of the 1.8 milli<strong>on</strong> records in its database relate to <strong>child</strong>ren and young people less than 20 years old.CHIRPP was set up to complement existing sources of informati<strong>on</strong> <strong>on</strong> <strong>injury</strong> mortality and hospitalizati<strong>on</strong>. Its main strength is the informati<strong>on</strong>it holds <strong>on</strong> the circumstances in which injuries occur. Informati<strong>on</strong> about such injuries is gathered in emergency departments directly from injuredpatients, or accompanying adults, who are asked to complete a <strong>on</strong>e-page form c<strong>on</strong>taining open-ended questi<strong>on</strong>s about where and how the <strong>injury</strong>occurred. Clinical staff provide informati<strong>on</strong> <strong>on</strong> the type of injuries and their severity, the parts of the body affected, and whether the patients wereadmitted or discharged. Informati<strong>on</strong> from the forms is then coded and entered into a central electr<strong>on</strong>ic database at the PHAC.Am<strong>on</strong>g the 40 variables used to describe the circumstances in which injuries occur is a narrative of up to 100 characters that describes the event.The narrative is particularly valuable as a source of informati<strong>on</strong> for which specific codes are not available. Events associated with particular places,activities (such as specific sports) or products that do not have Internati<strong>on</strong>al Classificati<strong>on</strong> of Disease codes are easy to identify in CHIRPP data.Between its detailed codes and its narratives, the database provides a wealth of informati<strong>on</strong> about how injuries happen.Analysts at CHIRPP receive, <strong>on</strong> average, four to five requests each week for informati<strong>on</strong> <strong>on</strong> injuries. Resp<strong>on</strong>ding to these requests may takeanything from a few minutes to several m<strong>on</strong>ths of work. About two thirds of requests come from the media. Most of the remainder are from HealthCanada’s Product Safety Bureau and from n<strong>on</strong>governmental organizati<strong>on</strong>s such as Safe Kids Canada.CHIRPP produces <str<strong>on</strong>g>report</str<strong>on</strong>g>s <strong>on</strong> a wide range of <strong>injury</strong> issues. Many of its short <str<strong>on</strong>g>report</str<strong>on</strong>g>s, fact sheets and m<strong>on</strong>ographs are posted <strong>on</strong> the PHAC website (7). The areas it has examined include:– the impact of legislati<strong>on</strong> <strong>on</strong> bicycle helmet use;– the effect of new regulati<strong>on</strong>s allowing bodycheckingin younger ice-hockey players;– the impact of new Canadian standards for playgroundequipment.CHIRPP’s <str<strong>on</strong>g>report</str<strong>on</strong>g>s c<strong>on</strong>taining detailed data <strong>on</strong> allaspects of injuries associated with baby walkers led toHealth Canada’s Product Safety Bureau deciding thatbaby walkers posed significant and unnecessary risks toyoung <strong>child</strong>ren. This led in turn, in June 2007, to Canada’sMinister of Health upholding an earlier prohibiti<strong>on</strong><strong>on</strong> baby walkers, including their advertising, sale andimporting. Canada remains the <strong>on</strong>ly country to date toban all types of baby walkers.Other investigati<strong>on</strong>s being carried out by various organizati<strong>on</strong>s,using CHIRPP’s data, c<strong>on</strong>cern:– the use of trampolines in homes and playgrounds;– all-terrain vehicles;– baby bath seats;– the ingesti<strong>on</strong> of magnets;– falls from windows and balc<strong>on</strong>ies;– injuries associated with diving structures;– scalds from tap water;– nursery products.© P. Lanvers/WHOResearch <strong>on</strong> <strong>child</strong> <strong>injury</strong> should not <strong>on</strong>ly c<strong>on</strong>cern theevaluati<strong>on</strong> of interventi<strong>on</strong> studies but also include:– ec<strong>on</strong>omic analyses;– programme effectiveness studies;– behavioural and developmental science research;– health utilizati<strong>on</strong> analyses.Research into the whole spectrum of <strong>child</strong> injuries indeveloping countries – from primary preventi<strong>on</strong> throughto rehabilitati<strong>on</strong> – needs much higher levels of funding.Such research will not <strong>on</strong>ly benefit developing countriesenormously, but has the potential to uncover soluti<strong>on</strong>s notyet found in high-income countries.There are too few practiti<strong>on</strong>ers in <strong>child</strong> <strong>injury</strong>preventi<strong>on</strong>Most countries around the world have limited humancapacity to prevent the epidemic of <strong>child</strong> injuries,deliver emergency and <strong>on</strong>going care following an<strong>injury</strong>, and provide appropriate rehabilitati<strong>on</strong> services.This problem is particularly acute in poorer countrieswhere the bur-den of <strong>child</strong> <strong>injury</strong> is greatest. In manyWORLD REPORT ON CHILD INJURY PREVENTION 149
settings around the world public health training doesnot address issues related to <strong>child</strong> <strong>injury</strong>. Medicalcourses teach students how to treat trauma but usuallyoverlook preventi<strong>on</strong>. Furthermore, government staff insectors relevant to <strong>child</strong> <strong>injury</strong> do not as a rule receivetraining <strong>on</strong> injuries and do not work in a structure thatenables informati<strong>on</strong> <strong>on</strong> <strong>injury</strong> preventi<strong>on</strong> to be sharedeffectively (see Box 7.4).BOX 7.4Developing knowledge and skills for<strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>While capacity building in the field of <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> is notlimited to human resources, knowledge and skills are n<strong>on</strong>etheless aclear priority. One tool to develop the knowledge base around <strong>injury</strong>is TEACH-VIP. 1 This is a comprehensive <strong>injury</strong> preventi<strong>on</strong> and c<strong>on</strong>trolcurriculum, developed over three years through the efforts of WHOand a network of over 60 experts <strong>on</strong> <strong>injury</strong> preventi<strong>on</strong> in 19 countries.The course material is designed for classroom instructi<strong>on</strong>, andc<strong>on</strong>tains PowerPoint slide presentati<strong>on</strong>s, supporting lecture notesand learning exercises addressing a range of topics relevant to <strong>injury</strong>preventi<strong>on</strong> and c<strong>on</strong>trol.TEACH-VIP is a modular curriculum, whose c<strong>on</strong>tent allows forthe flexible arrangement of less<strong>on</strong>s. Training courses may thereforebe structured differently depending <strong>on</strong> the particular audience orphysical setting.Within a year of being launched in October 2005, TEACH-VIP wasbeing used for training in over 60 countries. Experience has shownthat it is suitable for a wide variety of audiences – including studentsin public health and medical and nursing sciences, <strong>injury</strong> preventi<strong>on</strong>practiti<strong>on</strong>ers, <strong>injury</strong> resp<strong>on</strong>se service providers and governmentpers<strong>on</strong>nel. This is important, as the preventi<strong>on</strong> and c<strong>on</strong>trol of <strong>injury</strong>requires collaborati<strong>on</strong> across a range of sectors and disciplines, withparticipants working with a comm<strong>on</strong> understanding of the issues.TEACH-VIP provides training that is of both general and specificrelevance to <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>. Less<strong>on</strong>s of general relevance includethose relating to research methodologies, <strong>injury</strong> surveillanceand coding, trauma care, the communicati<strong>on</strong> of <strong>injury</strong> informati<strong>on</strong>,and general <strong>injury</strong> preventi<strong>on</strong>. Less<strong>on</strong>s that are specifically relevantcover road traffic injuries, falls, burns, drowning, animal bites andpois<strong>on</strong>ing. In additi<strong>on</strong>, TEACH-VIP c<strong>on</strong>tains a range of less<strong>on</strong>s <strong>on</strong>intenti<strong>on</strong>al injuries involving <strong>child</strong>ren and young people, including<strong>on</strong>es <strong>on</strong> youth violence and <strong>child</strong> abuse and neglect.Aside from knowledge transfer, there is also a need for a more targeteddevelopment of skills. WHO has created a distance mentor-ingprogramme known as MENTOR-VIP, 2 designed to assist junior <strong>injury</strong>practiti<strong>on</strong>ers in developing specific skills through a structured collaborati<strong>on</strong>with a more experienced pers<strong>on</strong> who has volunteered to actas a mentor. MENTOR-VIP thus provides a means to match demandfor technical guidance with offers to provide technical support.1Available at the web site: http://www.who.int/violence_<strong>injury</strong>_preventi<strong>on</strong>/capacitybuilding/teach_vip/en/index.html2Available at the web site: http://www.who.int/violence_<strong>injury</strong>_preventi<strong>on</strong>/capacitybuilding/mentor_vip/en/index.htmlChild <strong>injury</strong> preventi<strong>on</strong> is the resp<strong>on</strong>sibility of manysectorsChild <strong>injury</strong> preventi<strong>on</strong>, by the very nature of the type ofinjuries involved, should be a resp<strong>on</strong>sibility shared betweengovernments, n<strong>on</strong>governmental organizati<strong>on</strong>s, academicinstituti<strong>on</strong>s, internati<strong>on</strong>al agencies and the business sector.The health sector has a leading role to play (8),particularly with regard to:– collecting and analysing data;– carrying out research <strong>on</strong> risk factors;– implementing, m<strong>on</strong>itoring and evaluating interventi<strong>on</strong>s;– delivering appropriate primary, sec<strong>on</strong>dary and tertiarycare;– campaigning for greater attenti<strong>on</strong> to the issue of <strong>child</strong>injuries.All the same, a multisectoral approach is indeednecessary. The sectors of transport, police, educati<strong>on</strong>, lawand envir<strong>on</strong>ment all play a major role in the preventi<strong>on</strong>and c<strong>on</strong>trol of <strong>child</strong>hood injuries. Preventing injuriesfrom falls in schools comes under the remit of theeducati<strong>on</strong> ministry, for instance, while the legal sectorwill be resp<strong>on</strong>sible for legislating for mandatory <strong>child</strong>resistantc<strong>on</strong>tainers. The collaborati<strong>on</strong> between sectorshas to cross organizati<strong>on</strong>al boundaries, so that the publicsector, private organizati<strong>on</strong>s and n<strong>on</strong>-profit groups cancombine their expertise.Child <strong>injury</strong> preventi<strong>on</strong> is underfundedWell-targeted investment of financial resources is neededto tackle the problem of <strong>child</strong> injuries. Over the lastdecade, as countries have focused <strong>on</strong> the MillenniumDevelopment Goals, much funding has been provided toaddress infectious diseases – the major killer of <strong>child</strong>renunder five years of age. It would be a tragic mistake ifthis good investment were to be lost after <strong>child</strong>ren hadsurvived their infancy, because <strong>injury</strong> preventi<strong>on</strong> hadearlier been ignored. The cost-effectiveness of some <strong>child</strong><strong>injury</strong> preventi<strong>on</strong> strategies has been found to be at leastequal to that of other well-accepted strategies to prevent<strong>child</strong>hood illnesses.It is essential to engage the d<strong>on</strong>or communityif interventi<strong>on</strong>s are to be tested and implemented,especially in poorer countries. Child <strong>injury</strong> preventi<strong>on</strong>needs to be a stated priority of public and privatefunding agencies.Awareness needs to be created and maintainedThe magnitude, risk factors and preventability of <strong>child</strong>injuries are not widely appreciated at all levels, from policymakersand d<strong>on</strong>ors to the local community. This lack ofunderstanding means that the resources required are notbeing allocated to preventi<strong>on</strong> efforts and the political andorganizati<strong>on</strong>al structures that are needed are not being putin place.150 WORLD REPORT ON CHILD INJURY PREVENTION
It is of prime importance to show that resources can beefficiently and effectively used in this area for the benefitof public health. Sustained campaigning is thereforerequired to raise awareness about the public health,social and ec<strong>on</strong>omic impacts of <strong>child</strong> injuries, and howthese injuries can be prevented. Awareness, of course,also needs to be created about how some risk factors arec<strong>on</strong>nected to other issues – such as obesity, mobility anddisaster management – and how tackling these issueswould reduce <strong>child</strong> injuries and improve <strong>child</strong>ren’shealth overall.Recommended acti<strong>on</strong>sGovernments and others involved are encouraged toc<strong>on</strong>sider the following seven recommendati<strong>on</strong>s whendeveloping <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> programmes.poor and homeless <strong>child</strong>ren, <strong>child</strong>ren with disabilities andfemale <strong>child</strong>ren, and should be linked to other <strong>child</strong> healthstrategies.A country’s <strong>child</strong> <strong>injury</strong> policy should promote thedevelopment of nati<strong>on</strong>al standards and codes <strong>on</strong> issuesthat have a direct bearing <strong>on</strong> <strong>child</strong> <strong>injury</strong>, includingsuch items as products and appliances, playground andschool safety, and residential building regulati<strong>on</strong>s andlaws.A nati<strong>on</strong>al strategy needs to set ambitious but realistictargets for at least five or ten years. It should havemeasurable outcomes and sufficient funding to develop,implement, manage, m<strong>on</strong>itor and evaluate acti<strong>on</strong>s. Oncethe <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> strategy is established, nati<strong>on</strong>aland local acti<strong>on</strong> plans should be prepared laying downspecific acti<strong>on</strong>s to be taken and allocating resources forthese acti<strong>on</strong>s.Recommendati<strong>on</strong> 1: Integrate <strong>child</strong> <strong>injury</strong> intoa comprehensive approach to <strong>child</strong> health anddevelopmentRecommendati<strong>on</strong> 3: Implement specific acti<strong>on</strong>s toprevent and c<strong>on</strong>trol <strong>child</strong> injuriesA comprehensive strategy for <strong>child</strong> health and developmentshould include all leading causes of ill health and disabilityam<strong>on</strong>g <strong>child</strong>ren, and therefore include injuries. Existing<strong>child</strong> survival programmes need to introduce <strong>child</strong> <strong>injury</strong>preventi<strong>on</strong> strategies as part of the basic package of <strong>child</strong>health services. The current renewed emphasis <strong>on</strong> primaryhealth care provides an opportunity for governments,ministries of health and civil society organizati<strong>on</strong>s torestructure their <strong>child</strong> health programmes to include <strong>child</strong>injuries.The success of <strong>child</strong> health programmes should bemeasured not <strong>on</strong>ly by traditi<strong>on</strong>al measures of infectiousdisease mortality but also by other indicators of fatal andn<strong>on</strong>-fatal <strong>injury</strong>.Recommendati<strong>on</strong> 2: Develop and implement a <strong>child</strong><strong>injury</strong> preventi<strong>on</strong> policy and a plan of acti<strong>on</strong>Each country should prepare a <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> andc<strong>on</strong>trol policy bringing in a wide range of sectors. Agenciesinvolved should include those c<strong>on</strong>cerned with transport,health, planning, c<strong>on</strong>sumer product safety, agriculture,educati<strong>on</strong>, and law. There should also be representati<strong>on</strong>across the disciplines, with <strong>child</strong> development experts,<strong>injury</strong> epidemiologists, engineers, urban planners,clinicians, social scientists and others all participating.C<strong>on</strong>cerned groups should be brought in from government,the private sector, n<strong>on</strong>governmental organizati<strong>on</strong>s, themedia and the general public.The policy should take the needs of all <strong>child</strong>ren intoaccount, particularly those who are vulnerable, such asSpecific acti<strong>on</strong>s are needed to prevent and c<strong>on</strong>trol <strong>child</strong>injuries and to minimize their c<strong>on</strong>sequences. These acti<strong>on</strong>s– forming a part of the nati<strong>on</strong>al <strong>child</strong> health strategy– should be based <strong>on</strong> sound evidence, be appropriate interms of culture and other local c<strong>on</strong>text, and have beentested locally. The evaluati<strong>on</strong> of interventi<strong>on</strong>s should bean integral part of the programme.Chapters 1 to 6 discussed in detail specific interventi<strong>on</strong>sfor each type of <strong>injury</strong>, their impact <strong>on</strong> the frequency andseverity of injuries, and their cost-effectiveness where thiswas known. No standard package of interventi<strong>on</strong>s will besuitable for all countries. Table 7.1, though, summarized themain approaches, with some examples, that can be used.If specific interventi<strong>on</strong>s are not introduced, it isunlikely that simple awareness <strong>on</strong> its own will bring aboutsignificant reducti<strong>on</strong>s in <strong>child</strong> injuries and deaths.Recommendati<strong>on</strong> 4: Strengthen health systems toaddress <strong>child</strong> injuriesThe health system as a whole should be strengthened toprovide high quality care to injured <strong>child</strong>ren, as well asrehabilitati<strong>on</strong> and support services. These improvementsshould include:– the development and maintenance of an efficient systemof pre-hospital care;– good quality acute management of injured <strong>child</strong>ren inhospitals and clinics, with appropriate <strong>child</strong>-specificequipment and drugs;– suitable rehabilitati<strong>on</strong> programmes, addressing boththe physical and psychological l<strong>on</strong>g-term c<strong>on</strong>sequencesof injuries;WORLD REPORT ON CHILD INJURY PREVENTION 151
– coordinati<strong>on</strong> with allied sectors to ensure holistic careand management of the injured <strong>child</strong>.The health system should also be strengthened toprovide financial protecti<strong>on</strong> and social support to thefamilies and households of injured <strong>child</strong>ren. If this is notd<strong>on</strong>e, households may be pushed into poverty as a result of<strong>child</strong> injuries, especially in poorer countries.Appropriate training programmes should be a priority.Many countries do not have sufficient pers<strong>on</strong>nel with theskills and experience needed to develop and implement aneffective <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> programme.Governments should start this process by designatinga focal pers<strong>on</strong> or coordinator for <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>within the health ministry. The particular organizati<strong>on</strong>almodel to be used may depend <strong>on</strong> the nati<strong>on</strong>al situati<strong>on</strong>,but it is important that accountability for <strong>child</strong> <strong>injury</strong>preventi<strong>on</strong> and c<strong>on</strong>trol is explicitly set out.Recommendati<strong>on</strong> 5: Enhance the quality andquantity of data for <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>An important element in dealing with <strong>child</strong> injuries isascertaining the magnitude and characteristics of theproblem, as well as assessing nati<strong>on</strong>al policies <strong>on</strong> <strong>child</strong><strong>injury</strong> and the capacity to handle such injuries. A thoroughunderstanding is needed, not <strong>on</strong>ly of the volume of <strong>child</strong><strong>injury</strong> deaths, n<strong>on</strong>-fatal injuries and disabilities, but alsoof:– the <strong>child</strong>ren who are most affected;– the types of <strong>injury</strong> that are most prevalent;– the geographic areas where the greatest problems arefound;– the particular risk factors;– the <strong>child</strong> health policies, programmes and specific<strong>injury</strong> interventi<strong>on</strong>s that are in place.In additi<strong>on</strong> to these things, standardized definiti<strong>on</strong>s areneeded that are used across countries, not <strong>on</strong>ly for injuriesbut for disability as well.Sources of data can differ depending <strong>on</strong> the type of<strong>injury</strong>. Road traffic <strong>injury</strong> data, for instance, may beobtained from police, health ministry and health caresettings, and transport ministries. Data <strong>on</strong> falls, <strong>on</strong> theother hand, may be obtained from <strong>injury</strong> surveillancesystems, community-based surveys and paediatricadmissi<strong>on</strong> records. In any case, the limitati<strong>on</strong>s of thesesources of data and their potential to influence what needsto be observed, should be c<strong>on</strong>sidered before making useof them.Informati<strong>on</strong> systems <strong>on</strong> <strong>child</strong> injuries should be:– simple and cost-effective to implement;– appropriate to the levels of skill of the staff using them;– c<strong>on</strong>sistent with nati<strong>on</strong>al and internati<strong>on</strong>al standards(including external cause coding).Where possible, these systems should be integratedinto other <strong>child</strong> health informati<strong>on</strong> systems, such asdemographic and health surveys, integrated managementof <strong>child</strong>hood disease surveys and verbal autopsy studies.Data should be widely shared am<strong>on</strong>g the relevantauthorities and c<strong>on</strong>cerned groups, particularly thoseresp<strong>on</strong>sible for <strong>child</strong> health, educati<strong>on</strong> and social services,such as <strong>child</strong> development agencies.There are scant data <strong>on</strong> the ec<strong>on</strong>omic impact of <strong>child</strong>injuries in most countries, though it is known that theimpact is substantial. There are also no studies <strong>on</strong> thecost-effectiveness of preventi<strong>on</strong> interventi<strong>on</strong>s. Assessingthe direct and indirect ec<strong>on</strong>omic costs, where this ispossible, as well as the proporti<strong>on</strong> of gross nati<strong>on</strong>al productattributable to <strong>child</strong> injuries, can help increase awarenessof the scale of the problem.Recommendati<strong>on</strong> 6: Define priorities for research,and support research <strong>on</strong> the causes, c<strong>on</strong>sequences,costs and preventi<strong>on</strong> of <strong>child</strong> injuriesA research agenda for <strong>child</strong> injuries should be developed atregi<strong>on</strong>al and nati<strong>on</strong>al levels. The agenda should be based <strong>on</strong>evidence from a broad range of sectors. Research in all themain areas related to <strong>child</strong> <strong>injury</strong> should be strengthened,including <strong>on</strong>:– ec<strong>on</strong>omic analysis – including the cost of <strong>child</strong> injuriesand the cost of interventi<strong>on</strong>s;– large-scale interventi<strong>on</strong> trials, especially in poorercountries;– n<strong>on</strong>-fatal outcomes of <strong>injury</strong> and disability;– how best to integrate <strong>injury</strong> interventi<strong>on</strong>s into <strong>child</strong>health programmes.Research, if it is to be successful, requires focusedinvestments in human and technical capacity, particularlyin low-income and middle-income countries. A criticalmass of trained researchers <strong>on</strong> injuries and their preventi<strong>on</strong>needs to be built up.Research skills should be strengthened in a range ofdisciplines, including those of:– epidemiology;– clinical trials;– ec<strong>on</strong>omics;– engineering;– sociology;– behavioural and developmental psychology;– product evaluati<strong>on</strong>;– policy analysis.Recommendati<strong>on</strong> 7: Raise awareness of and targetinvestments towards <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>That <strong>child</strong> injuries are predictable and preventable isoften not understood, by the lay public and also by152 WORLD REPORT ON CHILD INJURY PREVENTION
policy-makers, medical pers<strong>on</strong>nel and d<strong>on</strong>ors. It isvital, therefore, that awareness is created about thefact that these injuries can generally be prevented. Itis an enormous advantage if well-known pers<strong>on</strong>alitiesor political leaders can actively champi<strong>on</strong> the causeof <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>. In additi<strong>on</strong>, an active civilsociety movement for <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>, grassrootslocal organizati<strong>on</strong>s for <strong>child</strong> safety, and sensitiveand resp<strong>on</strong>sible media <str<strong>on</strong>g>report</str<strong>on</strong>g>s can all bring about thenecessary cultural changes in society.Internati<strong>on</strong>al c<strong>on</strong>ferences, furthermore, provideopportunities to exchange knowledge and establishnetworks and partnerships. Complementary strategies,such as introducing <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> into schooland university curricula, can also help sensitize youngpeople to the risk of <strong>child</strong> injuries.Well-targeted financial investments can reduce <strong>child</strong>injuries and deaths c<strong>on</strong>siderably. Assessing the costsagainst the benefits of specific interventi<strong>on</strong>s and settingpriorities accordingly is important for all countries.Internati<strong>on</strong>al n<strong>on</strong>governmental organizati<strong>on</strong>s and largecorporati<strong>on</strong>s can help raise awareness at the global andnati<strong>on</strong>al level, as can – at the local level – socially awareemployers and ordinary committed citizens.Translating recommendati<strong>on</strong>s into realityThe previous secti<strong>on</strong> presented seven recommendati<strong>on</strong>swhich should be c<strong>on</strong>sidered when implementing a <strong>child</strong><strong>injury</strong> preventi<strong>on</strong> strategy. Child <strong>injury</strong> preventi<strong>on</strong>, though,is the resp<strong>on</strong>sibility of many. Reducing the risk of <strong>injury</strong> for<strong>child</strong>ren requires the involvement and commitment of abroad range of groups – from internati<strong>on</strong>al agencies throughto <strong>child</strong>ren themselves. The following are some of the acti<strong>on</strong>swhich can be taken by the various groups involved.Internati<strong>on</strong>al, development and d<strong>on</strong>or organizati<strong>on</strong>s– make – in a highly visible way – <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>a priority at an internati<strong>on</strong>al level;– fund and promote research, interventi<strong>on</strong>s andevaluati<strong>on</strong>s <strong>on</strong> <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>;– encourage governments to take sustainable acti<strong>on</strong> <strong>on</strong><strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>;– support capacity-building efforts.Governments– make <strong>child</strong> injuries a priority;– identify an agency or unit to lead <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>– either within the broader <strong>child</strong> health strategy or themore specific <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> plan;– appoint at least <strong>on</strong>e full-time pers<strong>on</strong> with resp<strong>on</strong>sibilityfor <strong>injury</strong> preventi<strong>on</strong>, including <strong>child</strong> injuries, in anappropriate ministry;– establish a sustainable data collecti<strong>on</strong> system based <strong>on</strong>the country’s needs and particular local issues relatedto <strong>child</strong>ren;– develop a multisectoral plan of acti<strong>on</strong> for <strong>child</strong> <strong>injury</strong>preventi<strong>on</strong>, including the setting of targets (see Box 7.5);– coordinate activities and collaborate across sectorsfor the implementati<strong>on</strong> and evaluati<strong>on</strong> of <strong>child</strong> <strong>injury</strong>preventi<strong>on</strong> programmes;– enact, implement and enforce laws and standards thathave been proven to reduce injuries;– ensure sufficient funds and human resources for <strong>child</strong><strong>injury</strong> preventi<strong>on</strong> efforts;– provide affordable access to all levels of health care andservices for all <strong>child</strong>ren;– promote the integrati<strong>on</strong> of health and safety c<strong>on</strong>cernsand an <strong>injury</strong> impact evaluati<strong>on</strong> into all new projects;– include <strong>child</strong>ren and young people in the developmentand implementati<strong>on</strong> of projects at the nati<strong>on</strong>al andlocal levels.N<strong>on</strong>governmental organizati<strong>on</strong>s– encourage governments to undertake proven <strong>child</strong><strong>injury</strong> preventi<strong>on</strong> activities and help in implementingsuch interventi<strong>on</strong>s;– identify local safety problems;– campaign for a safer envir<strong>on</strong>ment, standards andbehaviours;– campaign for the rights of those affected by <strong>injury</strong>;– undertake pilot preventi<strong>on</strong> programmes <strong>on</strong> <strong>child</strong> <strong>injury</strong>in the community;– support capacity-building;– build and extend networks and partnerships withothers involved in <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>.The private sector– recognize the importance of <strong>child</strong> injuries and theirpreventi<strong>on</strong>;– apply “design for safety” from c<strong>on</strong>cept, throughproducti<strong>on</strong>, to quality c<strong>on</strong>trol – including riskassessment and product approval;– ensure that products comply with safety standards,regulati<strong>on</strong>s and codes;– work with regulators to achieve harm<strong>on</strong>ized standardsand regulati<strong>on</strong>s worldwide;– advertise merchandise resp<strong>on</strong>sibly and emphasize thesafety aspects;– fund <strong>on</strong>going research and development in the area of<strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>;– fund the development and evaluati<strong>on</strong> of safetypromotingeducati<strong>on</strong>al material – such as games, toys,DVDs and videos.The media– <str<strong>on</strong>g>report</str<strong>on</strong>g> resp<strong>on</strong>sibly, accurately and sensitively thetraumatic c<strong>on</strong>sequences of injuries – with informati<strong>on</strong><strong>on</strong> preventi<strong>on</strong> always included in <str<strong>on</strong>g>report</str<strong>on</strong>g>s;– promote <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> by featuring stories ofyoung survivors and their families, highlighting goodpractices in <strong>injury</strong> preventi<strong>on</strong>;WORLD REPORT ON CHILD INJURY PREVENTION 153
BOX 7.5Developing a Nati<strong>on</strong>al Acti<strong>on</strong> Plan for <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>: the experienceof the Czech RepublicIn 2004, the Child Safety Acti<strong>on</strong> Plan was launched in 18 European countries under the umbrella of the European Child Safety Alliance (9). Its aim was tocoordinate acti<strong>on</strong>s <strong>on</strong> <strong>child</strong> <strong>injury</strong> in the participating countries. A set of standard indicators was agreed <strong>on</strong> to assess the burden of <strong>injury</strong>, to facilitatecomparis<strong>on</strong>s between different countries and to provide compelling arguments for str<strong>on</strong>ger nati<strong>on</strong>al commitments to <strong>injury</strong> preventi<strong>on</strong>. The Alliancegathered examples of best practice from partner countries, and shared them am<strong>on</strong>g the members (10). With the help of the secretariat and particulargroups of experts, each country was encouraged to develop a Nati<strong>on</strong>al Child Safety Plan setting out goals and priorities for acti<strong>on</strong> <strong>on</strong> <strong>child</strong> safety.In the Czech Republic, the initiative was taken up by the Ministry of Health, which, in 2005, established a multidisciplinary working group toaddress the problem. This group worked <strong>on</strong> a basic strategy and examined how all the relevant sectors – including those of traffic, public health,welfare, educati<strong>on</strong>, sports and c<strong>on</strong>sumer protecti<strong>on</strong> – could c<strong>on</strong>tribute to reducing the <strong>injury</strong> burden am<strong>on</strong>g <strong>child</strong>ren. From the beginning, a practicalapproach was stressed. Various models of good practices were endorsed, including those for “Safe Communities”, “Healthy Cities” and “HealthySchools”. University departments served as the research centres.With support provided by the European Child Safety Alliance and the involvement of WHO’s country office in Prague, the working group completeda draft Nati<strong>on</strong>al Acti<strong>on</strong> Plan for Child Injury Preventi<strong>on</strong>. This plan is currently awaiting endorsement from the government. Its principal aim is to engagegovernment departments and a wide range of other c<strong>on</strong>cerned organizati<strong>on</strong>s and individuals, including health care practiti<strong>on</strong>ers, to work together for asafer and healthier <strong>child</strong> populati<strong>on</strong>. The formati<strong>on</strong> of a Nati<strong>on</strong>al Child Injury Register provides informati<strong>on</strong> <strong>on</strong> preventi<strong>on</strong> activities and health care.The plan stresses the safety of <strong>child</strong>ren <strong>on</strong> the road – including through modificati<strong>on</strong>s to the traffic envir<strong>on</strong>ment – injuries in the home, schoolsafety and <strong>child</strong> c<strong>on</strong>sumer protecti<strong>on</strong>.Road safety educati<strong>on</strong> in the Czech Republic has a l<strong>on</strong>g history. However, a fresh approach is now necessary to improve the road traffic competencesof <strong>child</strong>ren. With proper training, a <strong>child</strong> can acquire knowledge, skills and the ability to analyse and solve safety problems.In the home envir<strong>on</strong>ment, where the majority of injuries treated in health-care units occur, the situati<strong>on</strong> still lags behind. Injuries in the homeare generally less serious, but far more numerous, than those <strong>on</strong> the roads. One problem is that the role of health care practiti<strong>on</strong>ers in publicsafety educati<strong>on</strong> is still not properly accepted as part of <strong>injury</strong> preventi<strong>on</strong> and care. It is usually the police who are the most active in educati<strong>on</strong><strong>on</strong> pers<strong>on</strong>al safety, particularly as regards the preventi<strong>on</strong> of violence.In the school envir<strong>on</strong>ment – where injuries most often occur through sport – topics such as <strong>injury</strong> preventi<strong>on</strong> and the preventi<strong>on</strong> of obesityshould be addressed at the same time as improving the general fitness of <strong>child</strong>ren.Czech laws and regulati<strong>on</strong>s should adopt the European standards and enforce them strictly. The country has had a good experience with Europeanstandards, which it adopted in 2002, relating to playground surfaces and equipment. In the following years, playground safety dramaticallyincreased. The regulati<strong>on</strong> for mandatory helmet use am<strong>on</strong>g <strong>child</strong> cyclists has lowered the number of head injuries, even though it <strong>on</strong>ly applies topublic roads and not to cycling in other places.WHO’s “Safe Community” programme has been introduced in the Czech Republic. One city has already been designated a “Safe Community” and there areother applicants in line. Nati<strong>on</strong>al <strong>injury</strong>-free days are celebrated each year in 17 “Healthy Cities”. Gradually, with str<strong>on</strong>g commitment from the Working Groupmembers and the Ministry of Health, the preventi<strong>on</strong> of <strong>child</strong> <strong>injury</strong> is being firmly placed <strong>on</strong> the agenda of policy-makers and decisi<strong>on</strong>-makers.– feature safe practices in radio and televisi<strong>on</strong> dramas,and other broadcast programmes;– initiate or support <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> campaigns.Teachers and community leaders– teach <strong>injury</strong> preventi<strong>on</strong> at school from a young age;– ensure that schools, playgrounds, and the access toschools are all safe;– set up and maintain safe public places and safe sportsand recreati<strong>on</strong>al facilities;– promote <strong>injury</strong> preventi<strong>on</strong> at universities and integratethe topic into existing professi<strong>on</strong>al programmes;– foster research into <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> ineducati<strong>on</strong>al settings;– include <strong>child</strong>ren and youth when implementinginterventi<strong>on</strong>s for <strong>child</strong> <strong>injury</strong> at a community level.Parents– create a safe envir<strong>on</strong>ment for <strong>child</strong>ren to live in;– properly store materials which are harmful to <strong>child</strong>ren– such as fireworks and pois<strong>on</strong>ing agents;– supervise potentially hazardous activities;– inform and educate <strong>child</strong>ren about the risk factors forinjuries as well as how injuries can be prevented;– encourage <strong>child</strong>ren to wear safety devices;– act as role models for <strong>child</strong>ren by adopting safe behaviourand using safety devices;– lobby for change in the community.Children and young people– act as role models by adopting safe methods to reduce<strong>injury</strong> risks – such as using safety devices, and playingin safe locati<strong>on</strong>s;– promote <strong>injury</strong> preventi<strong>on</strong> am<strong>on</strong>g peers and family;– refrain from engaging in high-risk behaviours;– c<strong>on</strong>tribute to determining priorities for acti<strong>on</strong>;– become involved in <strong>injury</strong> preventi<strong>on</strong> campaigns andprogrammes (see Box 7.6).C<strong>on</strong>clusi<strong>on</strong>The commitment to reduce the burden of <strong>child</strong>hooddiseases has often been proclaimed by internati<strong>on</strong>al154 WORLD REPORT ON CHILD INJURY PREVENTION
and nati<strong>on</strong>al declarati<strong>on</strong>s. All the same, high levels of<strong>child</strong>hood mortality, morbidity and disability still persist.In many countries <strong>on</strong>e of the reas<strong>on</strong>s for this is the impactof <strong>child</strong>hood injuries, affecting <strong>child</strong>ren of all ages.BOX 7.6Youth Declarati<strong>on</strong> for Road SafetyThe first ever <str<strong>on</strong>g>World</str<strong>on</strong>g> Youth Assembly for Road Safety was held at theUnited Nati<strong>on</strong>s in Geneva, Switzerland in April 2007. Nearly 400 delegatesfrom over 100 countries met to share experiences and ideasand identify ways to strengthen road safety efforts in their homecountries. In particular, they discussed how young people could bemore involved in such efforts.The two-day event was organized and led by young people. Itculminated in the adopti<strong>on</strong> of a Youth Declarati<strong>on</strong> for Road Safetywhich was handed to the United Nati<strong>on</strong>s (11). In accepting the Declarati<strong>on</strong>,Sheikha Haya Rashed Al Khalifa, President of the UnitedNati<strong>on</strong>s General Assembly, called it an important statement that the<str<strong>on</strong>g>World</str<strong>on</strong>g> Youth Ambassadors for Road Safety should use to campaignfor much greater attenti<strong>on</strong> to road safety in their countries.In an additi<strong>on</strong>al, moving tribute to victims of road traffic crashes,the delegates gathered <strong>on</strong> the steps of the Palais des Nati<strong>on</strong>s andreleased 1049 white ballo<strong>on</strong>s. As she released her ballo<strong>on</strong>, YomnaSafwat from Egypt dedicated hers to her young brother killed in aroad crash, saying “These ballo<strong>on</strong>s as many as they are, are withoutquesti<strong>on</strong> outnumbered by the tears shed over loved <strong>on</strong>es needlesslylost <strong>on</strong> the road. In tribute to these young souls, each ballo<strong>on</strong> isa cry out to the world to take acti<strong>on</strong>, to save the youth and to preventroad deaths and injuries. I send my ballo<strong>on</strong> to my dear brother,Mohammed Karim, with a message that your life has not been lostin vain, but will fuel the efforts of the youth all around the world tomake roads safer.”© WHOThe global community has the knowledge, an armouryof interventi<strong>on</strong>s and the resources to prevent this loss ofhealthy life in the youngest members of our community.This <str<strong>on</strong>g>report</str<strong>on</strong>g> is a plea for evidence-based interventi<strong>on</strong>s andsustained investments by all sectors – public, private andcivil – in <strong>injury</strong> preventi<strong>on</strong> and c<strong>on</strong>trol for <strong>child</strong>ren. It istime to unleash the promise of governments and createa world where <strong>child</strong>ren can learn, play, grow up and livewithout being killed or injured.References1. C<strong>on</strong>venti<strong>on</strong> <strong>on</strong> the Rights of the Child. New York, NY, UnitedNati<strong>on</strong>s, 1989 (A/RES/44/25) (http://www.unhchr.ch/html/menu3/b/k2crc.htm, accessed 21 January 2008).2. United Nati<strong>on</strong>s Millennium Declarati<strong>on</strong>. New York, NY,United Nati<strong>on</strong>s, 2000 (A/RES/55/2) (http://www.un.org/millennium/declarati<strong>on</strong>/ares552e.htm, accessed 22 January2008).3. The Bellagio Group <strong>on</strong> Child Survival. The Lancet series.Child survival [WHO press release]. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> HealthOrganizati<strong>on</strong> (http://www.who.int/<strong>child</strong>-adolescent-health/NEWS/news_27.htm, accessed 22 January 2008).4. Berfenstam R. Sweden’s pi<strong>on</strong>eering <strong>child</strong> accidentprogramme: 40 years later. Injury Preventi<strong>on</strong>, 1995:68–69.5. Hyder AA et al. Saving 1000 <strong>child</strong>ren a day: the potentialof <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> [unpublished manuscript].Baltimore, MD, Johns Hopkins University, 2008.6. Mackenzie SG, Pless IB. CHIRPP: Canada’s principal <strong>injury</strong>surveillance program. Injury Preventi<strong>on</strong>, 1999, 5:208 –213.7. CHIRPP Injury Reports (http://www.phac-aspc.gc.ca/<strong>injury</strong>-bles/chirpp/injrep-rapbles/index. html, accessed 19November 2007).8. Preventing injuries and violence: a guide for ministries ofhealth. Geneva, Switzerland, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>,2007 (http://whqlibdoc.who.int/publicati<strong>on</strong>s/2007/9789241595254_eng.pdf, accessed 7 March 2008).9. Vincenten J. Priorities for <strong>child</strong> safety in the European Uni<strong>on</strong>:agenda for acti<strong>on</strong>, 2nd ed. Amsterdam, ECOSA, 2004.10. MacKay M et al. Child safety good practice guide: goodinvestments in unintenti<strong>on</strong>al <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> andsafety promoti<strong>on</strong>. Amsterdam, European Child SafetyAlliance, 2006.11. Youth Declarati<strong>on</strong> for Road Safety. Geneva, United Nati<strong>on</strong>sRoad Safety Collaborati<strong>on</strong>, 23–24 April 2007 (http://www.who.int/entity/roadsafety/week/activities/global/youth/declarati<strong>on</strong>/en/index.html, accessed 4 May 2008).WORLD REPORT ON CHILD INJURY PREVENTION 155
156 WORLD REPORT ON CHILD INJURY PREVENTION
STATISTICAL ANNEX – EXPLANATORY NOTESStatistical AnnexExplanatory notesBackgroundEach year, Member States with vital registrati<strong>on</strong>systems send detailed informati<strong>on</strong> to the <str<strong>on</strong>g>World</str<strong>on</strong>g> HealthOrganizati<strong>on</strong> using the Internati<strong>on</strong>al Classificati<strong>on</strong> ofDisease (ICD) codes (1). Death registrati<strong>on</strong> data c<strong>on</strong>tainingusable informati<strong>on</strong> <strong>on</strong> the causes of death are availablefrom 111 countries. The majority of these are in highincomecountries, although Latin America, the Caribbeanand Central Asia are also well represented (2).The <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong> uses these data,supplemented by additi<strong>on</strong>al informati<strong>on</strong> from surveys,censuses, epidemiological studies and health facilities, todevelop regi<strong>on</strong>al and global estimates of mortality andmorbidity for various causes of illness and injuries. Firstpublished in 1996, the Global Burden of Disease (GBD)represents the most comprehensive examinati<strong>on</strong> of globalmortality and morbidity available (2).In 2000, a new assessment of the global burden of diseasewas undertaken, the original <strong>on</strong>e having been carriedout in 1990. The GBD project for 2000 used all availableand relevant informati<strong>on</strong> to create the best possiblepopulati<strong>on</strong>-based data. Even for regi<strong>on</strong>s and causes wheredata were sparse, the GBD used evidence at hand and thebest available methods to make inferences. Since thensubsequent versi<strong>on</strong>s of the GBD estimates have appearedin the 2002 and 2004 WHO <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Reports (3, 4).Updated estimates of the global burden of <strong>injury</strong> for theyear 2004 are presented in this <str<strong>on</strong>g>report</str<strong>on</strong>g> (5).In additi<strong>on</strong> to the GBD data, this <str<strong>on</strong>g>report</str<strong>on</strong>g> also uses datafrom the Global School Health Survey, UNICEF communitysurveys and a pilot surveillance study <strong>on</strong> unintenti<strong>on</strong>al<strong>injury</strong> am<strong>on</strong>g <strong>child</strong>ren c<strong>on</strong>ducted in four developingcountries. A brief outline of the methodology of each ofthese data sources is presented in the following pages.<str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong> dataDeaths and n<strong>on</strong>-fatal injuries are categoricallyattributed to a single underlying cause using the rulesand c<strong>on</strong>venti<strong>on</strong>s of the ICD (1). The cause list used forthe GBD 2004 project has four levels of disaggregati<strong>on</strong>and includes 135 specific diseases and injuries. Overallmortality is divided into three broad groups of causes,as follows:– Group I: communicable diseases, maternal causes,c<strong>on</strong>diti<strong>on</strong>s arising in the perinatal period and nutriti<strong>on</strong>aldeficiencies;– Group II: n<strong>on</strong>communicable diseases;– Group III: intenti<strong>on</strong>al and unintenti<strong>on</strong>al injuries.Injury categories within Group III are further definedin terms of external cause codes.For the purpose of this <str<strong>on</strong>g>report</str<strong>on</strong>g> the following ICD versi<strong>on</strong>10 codes (or the associated versi<strong>on</strong> 9 codes) have beenused.Road traffic injuries: V01–V04, V06, V09–V80, V87,V89, V99:– excludes injuries sustained while repairing a vehicle(W00–W59) or shutting a car door (W00–W59);– excludes assault by crashing a vehicle (Y03),intenti<strong>on</strong>al self-harm (X81–X83).Drowning: W65–W74:– excludes drowning or submersi<strong>on</strong> due to cataclysms(X34–X39);– excludes transport incidents (V01–V99) or watertransport incidents (V90, V92).Burns: X00–X59:– excludes fire from ars<strong>on</strong> (X97), sec<strong>on</strong>dary to anexplosi<strong>on</strong> (W35–W40) or a transport incident(V01–V99);– excludes exposure to electric current, radiati<strong>on</strong> andextreme temperature (W85–W99);– excludes c<strong>on</strong>tact with heat and hot substances(X10–X19).Falls: W00–W19:– excludes assaults (Y01–Y02) or intenti<strong>on</strong>al self-harm(X80–X81);– excludes falls from animals (V80), burning buildings(X00) or a vehicle (V01–V99);– excludes falls into fire (X00–X04, X08–X09), water(W65–W74) or machinery (W28–W31).Pois<strong>on</strong>ing: X40–X49:– excludes pois<strong>on</strong>ing with suicidal or homicidal intent(W60–W69, X85–X90, Y10–Y19);– excludes the adverse effects of therapeutic drugsadministered in the correct dosage (Y40–Y59).Absolute numbers and rates per 100 000 populati<strong>on</strong> arepresented by sex and WHO regi<strong>on</strong> for the following agegroups: under 1 year, 1–4 years, 5–9 years, 10–14 years,15–19 years and under 20 years.WHO Member States are grouped into six regi<strong>on</strong>s: theAfrican Regi<strong>on</strong>, the Regi<strong>on</strong> of the Americas, the South-East Asia Regi<strong>on</strong>, the European Regi<strong>on</strong>, the EasternMediterranean Regi<strong>on</strong> and the Western Pacific Regi<strong>on</strong>.Countries within these six regi<strong>on</strong>s are further dividedby income level, based <strong>on</strong> <str<strong>on</strong>g>World</str<strong>on</strong>g> Bank estimates of grossnati<strong>on</strong>al income (GNI) per capita for the year 2004 (6,7). On the basis of their GNI per capita, ec<strong>on</strong>omies areWORLD REPORT ON CHILD INJURY PREVENTION 157
classified as low-income and middle-income (less thanUS$ 10 066), or high-income (US$ 10 066 or more). Thecountries included in each of the WHO regi<strong>on</strong>s, dividedinto low-income and middle-income and high-incomecategories, are shown in Table D.1.Global estimates of mortality due to <strong>injury</strong>The GBD 2004 update uses the latest populati<strong>on</strong> estimatesfor WHO Member States prepared by the United Nati<strong>on</strong>sPopulati<strong>on</strong> Divisi<strong>on</strong> (8), as well as life tables publishedin the 2006 <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Report (9). The methodologyemployed to generate the GBD 2004 revisi<strong>on</strong> was similarto that used in previous revisi<strong>on</strong>s (5). The estimates werederived from an extensive analysis of mortality datafor all regi<strong>on</strong>s of the world, together with systematicreviews of epidemiological studies and other healthservice data. They were based <strong>on</strong> complete or incompletevital registrati<strong>on</strong> data, together with informati<strong>on</strong> fromsample registrati<strong>on</strong> systems covering around 70% of theglobal mortality. Survey data and indirect demographictechniques provided informati<strong>on</strong> <strong>on</strong> the levels of <strong>child</strong> andadult mortality for the remaining 30% of estimated globalmortality. Data <strong>on</strong> causes of death from death registrati<strong>on</strong>systems with incomplete coverage were adjusted to takeinto account the likely differences in patterns in the causeof death that would be expected in the uncovered andoften poorer subpopulati<strong>on</strong>s (5).For countries lacking vital registrati<strong>on</strong> data, mainlyin Africa, cause-of-death models were used for an initialestimate of the most likely distributi<strong>on</strong> of deaths across thebroad categories of communicable and n<strong>on</strong>communicablediseases and injuries, based <strong>on</strong> estimated total mortalityrates and income. A regi<strong>on</strong>al model of the pattern ofspecific causes of death was then c<strong>on</strong>structed based <strong>on</strong>local vital registrati<strong>on</strong> and data from verbal autopsies(a method of medically determining the cause of deathbased <strong>on</strong> interviews with the next of kin or caregivers).This proporti<strong>on</strong>ate distributi<strong>on</strong> was then applied withineach broad group of causes. Finally, the resulting estimateswere adjusted according to other epidemiological evidencefrom studies <strong>on</strong> specific diseases and injuries. For the2004 data presented here, the choice of death registrati<strong>on</strong>data to estimate within-group cause distributi<strong>on</strong>s for thevarious WHO regi<strong>on</strong>s was c<strong>on</strong>sistent with that used inprevious GBD estimates – the <strong>on</strong>ly excepti<strong>on</strong> being Africa.The regi<strong>on</strong>al pattern <strong>on</strong> cause of death distributi<strong>on</strong>s forAfrica in this 2004 update is based <strong>on</strong> death registrati<strong>on</strong>data from four countries, and verbal autopsy data fromseven countries, unlike the earlier estimates which useddata from rural South Africa <strong>on</strong>ly.Special attenti<strong>on</strong> has also been paid to injuries, wherethere are often problems of misattributi<strong>on</strong> or miscoding.For example, the category “<strong>injury</strong> undetermined whetheraccidentally or purposely inflicted” (Y10–Y34 in ICD 10)can often include a significant share of deaths due to <strong>injury</strong>.Except where more detailed local informati<strong>on</strong> is available,these deaths have been proporti<strong>on</strong>ately allocated to theother <strong>injury</strong> causes of death. Deaths coded as “unspecifiedaccidents” (E928.9 in ICD 10), have also been redistributedproporti<strong>on</strong>ally across other causes of unintenti<strong>on</strong>al <strong>injury</strong>death.Table A.1 presents estimates for fatal <strong>child</strong>unintenti<strong>on</strong>al injuries (and the subtypes of this group)by age groupings, sex and WHO regi<strong>on</strong>s and countryincome levels.Global and regi<strong>on</strong>al ranking of deaths andDALYsThe DALY (disability-adjusted life years lost) measure isused to quantify the burden of disease (2). It is a healthgapmeasure that combines informati<strong>on</strong> <strong>on</strong> the numberof years of life lost from premature death with the loss ofhealth from disability.As in the analysis for the deaths, the burden of <strong>injury</strong> inthe 2004 update is similar to the method used for the 1990,2000 and 2002 estimates. It utilizes the 1990 disabilityweights relating to <strong>injury</strong> (2, 10). The GBD 1990 projectmethods defined a case of <strong>injury</strong> as <strong>on</strong>e severe enough towarrant medical attenti<strong>on</strong> or <strong>on</strong>e that leads to death. Aswas d<strong>on</strong>e in previous revisi<strong>on</strong>s, the GBD 2004 update usedmany sources of informati<strong>on</strong> to estimate the years livedwith disability as a result of an <strong>injury</strong> or disease. Theseincluded nati<strong>on</strong>al and internati<strong>on</strong>al surveillance data anddisease registries, health survey statistics, data <strong>on</strong> useof hospital and medical services, and internati<strong>on</strong>al andcountry-specific epidemiological studies (2). The results<str<strong>on</strong>g>report</str<strong>on</strong>g>ed here are based <strong>on</strong> analyses for the GBD 2000 ofhealth-facility data obtained after an extensive period ofc<strong>on</strong>sultati<strong>on</strong>s with Member States.The proporti<strong>on</strong> of incident cases resulting in l<strong>on</strong>g-termdisabling sequelae was estimated for each <strong>injury</strong> categoryfrom a review of l<strong>on</strong>g-term epidemiological studies of<strong>injury</strong> outcomes.To produce the rankings in Table A.2, deaths anddisabilities were first divided into the three broad groupsof causes menti<strong>on</strong>ed earlier. Next, deaths and disabilitieswithin each of these groups were divided into categories.For example, injuries were divided between unintenti<strong>on</strong>aland intenti<strong>on</strong>al injuries. Following this level ofdisaggregating, deaths and disabilities were furtherdivided into subcategories. Unintenti<strong>on</strong>al injuries, forexample, were subdivided into road traffic injuries,pois<strong>on</strong>ings, falls, fire-related burns and drowning. Thesame procedure was followed for the other two broadgroups of deaths and disabilities. The rankings wereproduced by ordering the subcategories.The 15 leading causes of death and DALYs for <strong>child</strong>renunder the age of 15 years are <str<strong>on</strong>g>report</str<strong>on</strong>g>ed in Table A.2 forall WHO Member States and for each of the six WHOregi<strong>on</strong>s.158 WORLD REPORT ON CHILD INJURY PREVENTION
Global School-based Student Health SurveyThe Global School-based Student Health Survey (GSHS)is a collaborative surveillance project designed to helpcountries measure and assess behavioural risk andprotective factors am<strong>on</strong>g <strong>child</strong>ren aged 13 to 15 years inthe following 10 key areas (11):– alcohol and other drug use;– dietary behaviours;– hygiene;– mental health;– physical activity;– protective factors;– resp<strong>on</strong>dent demographics;– sexual behaviours;– tobacco use;– violence and unintenti<strong>on</strong>al <strong>injury</strong>.The GSHS is a relatively inexpensive school-basedsurvey which uses a self-administered questi<strong>on</strong>naireto obtain informati<strong>on</strong> about young people’s healthbehaviours. It is c<strong>on</strong>ducted primarily am<strong>on</strong>g studentsaged 13–15 years and uses a two-stage cluster samplingdesign; a comm<strong>on</strong> school-based methodology; andthree questi<strong>on</strong>naire comp<strong>on</strong>ents: a core module, coreexpandedquesti<strong>on</strong>s, and country-specific questi<strong>on</strong>s. Thequesti<strong>on</strong>naire is administered during school during asingle standard school period.At the time of analysis for this <str<strong>on</strong>g>report</str<strong>on</strong>g>, 28 countries hadvoluntarily c<strong>on</strong>ducted the survey and submitted their finalresults to WHO. Data from 26 of these countries whichhad complete informati<strong>on</strong> <strong>on</strong> unintenti<strong>on</strong>al injuries arepresented in Table A.3.UNICEF dataSeveral tables and figures appearing in the <str<strong>on</strong>g>report</str<strong>on</strong>g> have beentaken from the UNICEF/The Alliance for Safe Children(TASC) data sources. This has been d<strong>on</strong>e in an attempt toovercome some of the limitati<strong>on</strong>s of the Global Burden ofDisease studies. However, the UNICEF data are from <strong>on</strong>ly<strong>on</strong>e c<strong>on</strong>tinent, Asia, and thus cannot be generalized tothe rest of the world. Nevertheless, these data have str<strong>on</strong>gpolicy and programme implicati<strong>on</strong>s (12).Since 2002, as part of their collaborative project <strong>on</strong><strong>child</strong> <strong>injury</strong> preventi<strong>on</strong>, UNICEF and TASC have jointlyc<strong>on</strong>ducted six nati<strong>on</strong>al or subnati<strong>on</strong>al surveys <strong>on</strong> <strong>child</strong>injuries in South and East Asia. The specific survey siteswere Bangladesh, China (Beijing and Jiangxi provinces),the Philippines, Thailand and Viet Nam.These community-based surveys examined all causes ofmortality from injuries and other illnesses, though for thepurpose of this <str<strong>on</strong>g>report</str<strong>on</strong>g> and the Statistical Annex, <strong>on</strong>ly the<strong>injury</strong> data will be included. Their objectives were to gain abetter understanding of the <strong>injury</strong> incidence, risk factors,associated ec<strong>on</strong>omic and social costs, health-seekingbehaviours of injured people, and overall knowledge,attitudes and practices of communities regarding <strong>injury</strong>preventi<strong>on</strong>.In brief, the following methodology was employed.A representative sample of households was drawn upin each nati<strong>on</strong>al or subnati<strong>on</strong>al survey using the censussampling scheme.Standardized methodology was used in all six sites,with similar questi<strong>on</strong>s, fieldwork, quality assuranceand procedures of analysis.The recall period for morbidity was <strong>on</strong>e year in allsurveys, and for mortality it was three years, except inthe first survey in Viet Nam, where it was <strong>on</strong>e year.The cause of death was ascertained through medicalcertificates where they existed, or through verbal autopsywhere medical certificates were unavailable, using thestandard WHO verbal autopsy guidelines (13).The survey questi<strong>on</strong>naire c<strong>on</strong>sisted of six modules. Thefirst four modules were designed to collect demographicinformati<strong>on</strong> <strong>on</strong> household members, causes of mortalityand morbidity, and circumstances and c<strong>on</strong>sequences of<strong>injury</strong> events, and to provide a descripti<strong>on</strong> of household<strong>injury</strong> hazards. The other two modules were used for anested case–c<strong>on</strong>trol study of drowning. Sociodemographicinformati<strong>on</strong> was gathered from the head of the householdand informati<strong>on</strong> <strong>on</strong> n<strong>on</strong>-fatal injuries from the injuredpers<strong>on</strong>, if an adult, or from the caregiver if a <strong>child</strong>, and froma relative if the <strong>injury</strong> was fatal. The detailed methodologymay be found in the recently published Innocenti Report(14).Table 1 summarizes the sample sizes, definiti<strong>on</strong>s andmethods employed in each of the sites. Altogether, inthe combined surveys 516 818 households were visited,involving 2 157 291 individuals of whom 788 194 were<strong>child</strong>ren.While all survey sites classified <strong>injury</strong> severity in thesame way, the case definiti<strong>on</strong>s for <strong>injury</strong> or illness variedslightly between the various settings. The following fivecategories were used.Fatal <strong>injury</strong> (death). An <strong>injury</strong> resulting in death,whether immediate or delayed, but as a direct resultof the <strong>injury</strong>. This classificati<strong>on</strong> was the same for allsurveys.Severe <strong>injury</strong> (permanent disability). Injury thatresulted in permanent disability – such as blindness,deafness, loss of an extremity or the inability to walk, orthe loss of mental abilities. Emoti<strong>on</strong>al and psychiatriccauses were not included because of the difficulty ofdiagnosis and classificati<strong>on</strong>. This classificati<strong>on</strong> was thesame for all surveys.Serious <strong>injury</strong>. Injury requiring hospitalizati<strong>on</strong> for10 days or more – that is, requiring a major surgicalprocedure. This classificati<strong>on</strong> was the same for allsurveys.Major <strong>injury</strong>. An <strong>injury</strong> requiring hospitalizati<strong>on</strong>for less than 10 days. This definiti<strong>on</strong> was designed toWORLD REPORT ON CHILD INJURY PREVENTION 159
TABLE 1Methodology utilized in surveysBangladesh China Philippines Thailand Viet NamBeijingJiangxiSurvey year 2003 2004 2005 2003 2003 2000Household 171 366 28 084 100 010 90 446 100 179 26 733Members 819 429 81 604 319 543 418 522 389 531 128 662Children 351 651 13 508 98 335 178 938 98 904 46 858Strata urban/rural 18 districts urban/rural nati<strong>on</strong>al 5 regi<strong>on</strong>surban/rural8 regi<strong>on</strong>surban/ruralAllocati<strong>on</strong> method PPS PPS PPS PPS PPS PPS(square rootallocati<strong>on</strong>)Primary Sampling UnitDistrictDistrictStreetRegi<strong>on</strong> Province Province(PSU)committee committeeMethod SRS PPS PPS SRS PPS SRSSec<strong>on</strong>dary Sampling UnitUpazilla (rural)Mohalla (urban)Street committeeNeighbourhoodcommitteevillagesCensus blocksCensus blocks(urban)Villages (rural)DistrictsMethod SRS PPS PPS PPS PPS SRSTertiary Sampling UnitUni<strong>on</strong> (rural)HouseholdsNeighbourhoodcommittees200 householdcensus blocksBarangay Households(urban)90 householdcensus blocks(urban)MethodSRS (rural)Systematic(urban)PPS PPS Systematic Systematic SRSSampling Unit Household Household Household Household Household HouseholdObservati<strong>on</strong> Unit All Members All Members All Members All Members All Members All MembersPPS = Probability-proporti<strong>on</strong>al-to-size; SRS = simple random sampling.Source: reference 15.capture injuries that required significant care but didnot necessarily require surgical interventi<strong>on</strong>. Thisclassificati<strong>on</strong> was the same for all surveys.Moderate <strong>injury</strong>. An <strong>injury</strong> requiring medical care orfor which school or work was missed for a period, orwhere the <strong>child</strong> was unable to carry out activities of dailyliving and for which hospitalizati<strong>on</strong> was not required.The definiti<strong>on</strong> used a period of <strong>on</strong>e day in Beijing,Jiangxi and Viet Nam, and three days in Bangladesh,the Philippines and Thailand.There are some differences between the UNICEF/TASCdataset for fatal <strong>child</strong> <strong>injury</strong> and the Global Burden ofDisease (2004 update) dataset for the two regi<strong>on</strong>s coveredby this survey. It is most likely that these differences resultfrom the following c<strong>on</strong>siderati<strong>on</strong>s.The different methods used for the two datasets. TheUNICEF/TASC data come from direct, householdsurveys using representative samples, as noted inTable 1, while GBD data come from vital registrati<strong>on</strong>and proporti<strong>on</strong>al mortality models, as described in theprevious secti<strong>on</strong>.Definiti<strong>on</strong>s of <strong>injury</strong>. The UNICEF/TASC surveysdo not c<strong>on</strong>form to ICD 9 or 10 as they are based <strong>on</strong>verbal autopsy and incident interviews. In additi<strong>on</strong>,they include drowning as a result of floods and othercataclysms, which the GBD data exclude.Definiti<strong>on</strong>s of age. The UNICEF/TASC data are for<strong>child</strong>ren under 18 years, whereas the GBD data shownin Table 2 pertain to <strong>child</strong>ren and young people under20 years.The major difference between the data from these two<strong>injury</strong> systems was the drowning rate am<strong>on</strong>g <strong>child</strong>ren.Drowning was the leading cause of <strong>child</strong> death in all fivecountries surveyed and was <strong>on</strong> average 3.4 times morefrequent than deaths from road traffic fatalities (15).Global <strong>child</strong>hood unintenti<strong>on</strong>al <strong>injury</strong>surveillanceIn 2007, because of the lack of standardized data for <strong>child</strong>injuries from low-income and middle-income countries,and the limited number of multicountry datasets, WHO160 WORLD REPORT ON CHILD INJURY PREVENTION
TABLE 2Differences between datasets in causes of deathCauses of death (rates per 100 000 populati<strong>on</strong>): Global Burden of Disease data compared with UNICEF/TASC survey dataGBD 2004 updateUNICEF/TASC surveysSouth-East Asia Regi<strong>on</strong> Western Pacific Regi<strong>on</strong> (lowincomeAll 5 countriescountries)Drowning 6.2 13.9 30.1Road traffic injuries 7.4 8.6 8.9Falls 2.7 2.2 2.6Pois<strong>on</strong>ing 1.7 1.8 0.8Burns 6.1 0.6 0.4commissi<strong>on</strong>ed a pilot study <strong>on</strong> global <strong>child</strong>hood unintenti<strong>on</strong>al<strong>injury</strong> surveillance (GCUIS). The goals of the studywere:– to pilot-test a standardized protocol for facility-based<strong>child</strong>hood injuries;– to determine the nature and magnitude of <strong>child</strong>hoodinjuries and their burden <strong>on</strong> the health-care system.While the pilot study focused <strong>on</strong> unintenti<strong>on</strong>al injuries,the ultimate aim of the project was to improve <strong>on</strong>going<strong>injury</strong> surveillance in the target countries.A standard proforma was administered to caregiversof injured <strong>child</strong>ren less than 12 years old presenting atan urban emergency department in the following fourcountries: Bangladesh, Colombia, Egypt and Pakistan.The surveillance form was based <strong>on</strong> the Internati<strong>on</strong>alClassificati<strong>on</strong> of External Causes of Injuries (short form)(15), as well as forms used previously in Pakistan, SouthAfrica and the United States.The operati<strong>on</strong>al definiti<strong>on</strong> of an <strong>injury</strong> was “any typeof unintenti<strong>on</strong>al <strong>injury</strong> <strong>on</strong> any body part of a <strong>child</strong> under12 years of age seen in <strong>on</strong>e of the designated GCUISemergency rooms”. The resp<strong>on</strong>dent for the surveillancesystem was the caregiver arriving with the <strong>child</strong> at theemergency department, while the unit of analysis was theinjured <strong>child</strong>.Using a standardized electr<strong>on</strong>ic form in Epi InfoVersi<strong>on</strong> 3.3.2, the study recorded:– demographic informati<strong>on</strong>;– injuries, measured in terms of mortality and disability;– risk factors – including age, gender, level of educati<strong>on</strong>,time, locati<strong>on</strong> and activity;– socioec<strong>on</strong>omic informati<strong>on</strong>;– outcome data during treatment in the emergency department;– <strong>injury</strong>-specific risk factors for road traffic injuries, falls,burns and pois<strong>on</strong>ing;– clinical criteria – including waiting time, <strong>injury</strong> severityscore and distance travelled;– preventi<strong>on</strong> measures.Each site, with a pilot surveillance system derived fromthe same protocol, was requested to submit up to 550 cases,based <strong>on</strong> n<strong>on</strong>-random, sequential sampling, to the coordinatingcentre at Johns Hopkins University. The data werecollected between January and December 2007, with eachcountry taking <strong>on</strong> average 25 weeks to collect 550 cases.Preliminary results from the pilot study are presentedin Table C.1 of this Statistical Annex.References1. Internati<strong>on</strong>al statistical classificati<strong>on</strong> of diseases and relatedhealth problems, tenth revisi<strong>on</strong>. Volume 1: Tabular list;Volume 2: Instructi<strong>on</strong> manual; Volume 3: Index. Geneva,<str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 1992–1994.2. Murray CJL, Lopez AD. The global burden of disease: acomprehensive assessment of mortality and disability fromdiseases, injuries, and risk factors in 1990 and projected to2020. Bost<strong>on</strong>, MA, Harvard School of Public Health, 1996(Global Burden of Disease and Injury Series, Vol. I).3. The <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Report 2002. Reducing risks, promotinghealthy lives. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2002(http://www.who.int/entity/whr/2002/en/whr02_en.pdf,accessed 21 May 2008).4. <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Report 2004. Changing history. Geneva,<str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2004 (http://www.who.int/entity/whr/2004/en/<str<strong>on</strong>g>report</str<strong>on</strong>g>04_en.pdf, accessed 21 May2008).5. Global burden of disease, 2004. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>,2008 (in press).6. <str<strong>on</strong>g>World</str<strong>on</strong>g> Development Report 2004: equity and development.Washingt<strong>on</strong>, DC, The <str<strong>on</strong>g>World</str<strong>on</strong>g> Bank, 2006.7. Country classificati<strong>on</strong>: classificati<strong>on</strong> of ec<strong>on</strong>omies. Washingt<strong>on</strong>,DC, The <str<strong>on</strong>g>World</str<strong>on</strong>g> Bank Group, 2002 (http://www.worldbank.org/data/countryclass/countryclass.html, accessed20 June 2008).8. <str<strong>on</strong>g>World</str<strong>on</strong>g> populati<strong>on</strong> prospects: the 2006 revisi<strong>on</strong>. New York,NY, Populati<strong>on</strong> Divisi<strong>on</strong>, Department of Ec<strong>on</strong>omic andSocial Affairs, United Nati<strong>on</strong>s Secretariat, 2007.WORLD REPORT ON CHILD INJURY PREVENTION 161
9. The <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Report 2006: working together for health.Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2006 (http://www.who.int/entity/whr/2006/whr06_en.pdf, accessed 21 May2008).10. Begg S, Tomijima N. Global burden of <strong>injury</strong> in the year2000: an overview of methods. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>,2003.11. Global school-based student health survey (GSHS). Geneva,<str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, Chr<strong>on</strong>ic Diseases and HealthPromoti<strong>on</strong> (http://www.who.int/chp/gshs/en/index.html,accessed 20 May 2008).12. Linnan M et al. Child mortality and <strong>injury</strong> in Asia: policyand programme implicati<strong>on</strong>s. Florence, UNICEFInnocenti Research Centre, 2007 (http://www.unicef-irc.org/publicati<strong>on</strong>s/pdf/iwp_2007_07.pdf, accessed 20 May2008).13. Verbal autopsy standards: ascertaining and attributingcause of death. Geneva, <str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong>, 2007(http://www.who.int/whosis/mort/verbal_autopsy_standards0.pdf,accessed 20 June 2008).14. Linnan M et al. Child mortality and <strong>injury</strong> in Asia: surveymethods. Florence, UNICEF Innocenti Research Centre,2007 (http://www.unicef-irc.org/publicati<strong>on</strong>s/pdf/iwp_2007_05.pdf, accessed 20 May 2007).15. Internati<strong>on</strong>al classificati<strong>on</strong> of external causes of injuries.Short versi<strong>on</strong> (Short ICECI) data collecti<strong>on</strong> form for a pilotstudy. Atlanta, GA, Centers for Disease C<strong>on</strong>trol and Preventi<strong>on</strong>,Nati<strong>on</strong>al Center for Injury Preventi<strong>on</strong> and C<strong>on</strong>trol,1999 (http://www.cdc.gov/ncipc/pub-res/dataform.pdf, accessed 20 June 2008).162 WORLD REPORT ON CHILD INJURY PREVENTION
WORLD REPORT ON CHILD INJURY PREVENTION 163
TABLE A.1All unintenti<strong>on</strong>al injuriesEstimated mortality by sex, age group, a WHO regi<strong>on</strong> and income level, b 2004Absolute numbers cBoysWHO regi<strong>on</strong>Income level
TABLE A.1 (CONTINUED)All unintenti<strong>on</strong>al injuriesEstimated mortality by sex, age group, a WHO regi<strong>on</strong> and income level, b 2004Rate e per 100 000 populati<strong>on</strong>BoysWHO regi<strong>on</strong>Income level
TABLE A.1 (CONTINUED)Road traffic injuriesEstimated mortality by sex, age group, a WHO regi<strong>on</strong> and income level, b 2004Absolute numbers cBoysWHO regi<strong>on</strong>Income level
TABLE A.1 (CONTINUED)Road traffic injuriesEstimated mortality by sex, age group, a WHO regi<strong>on</strong> and income level, b 2004Rate e per 100 000 populati<strong>on</strong>BoysWHO regi<strong>on</strong>Income level
TABLE A.1 (CONTINUED)DrowningEstimated mortality by sex, age group, a WHO regi<strong>on</strong> and income level, b 2004Absolute numbers cWHO regi<strong>on</strong> Income level Boys
TABLE A.1 (CONTINUED)DrowningEstimated mortality by sex, age group, a WHO regi<strong>on</strong> and income level, b 2004Rate e per 100 000 populati<strong>on</strong>BoysWHO regi<strong>on</strong>Income level
TABLE A.1 (CONTINUED)Fire-related burnsEstimated mortality by sex, age group, a WHO regi<strong>on</strong> and income level, b 2004Absolute numbers cBoysWHO regi<strong>on</strong>Income level
TABLE A.1 (CONTINUED)Fire-related burnsEstimated mortality by sex, age group, a WHO regi<strong>on</strong> and income level, b 2004Rate e per 100 000 populati<strong>on</strong>BoysWHO regi<strong>on</strong>Income level
TABLE A.1 (CONTINUED)FallsEstimated mortality by sex, age group, a WHO regi<strong>on</strong> and income level, b 2004Absolute numbers cBoysWHO regi<strong>on</strong>Income level
TABLE A.1 (CONTINUED)FallsEstimated mortality by sex, age group, a WHO regi<strong>on</strong> and income level, b 2004Rate e per 100 000 populati<strong>on</strong>BoysWHO regi<strong>on</strong>Income level
TABLE A.1 (CONTINUED)Pois<strong>on</strong>ingEstimated mortality by sex, age group, a WHO regi<strong>on</strong> and income level, b 2004Absolute numbers cBoysWHO regi<strong>on</strong>Income level
TABLE A.1 (CONTINUED)Pois<strong>on</strong>ingEstimated mortality by sex, age group, a WHO regi<strong>on</strong> and income level, b 2004Rate e per 100 000 populati<strong>on</strong>BoysWHO regi<strong>on</strong>Income level
TABLE A.1 (CONTINUED)Other unintenti<strong>on</strong>al injuriesEstimated mortality by sex, age group, a WHO regi<strong>on</strong> and income level, b 2004Absolute numbers cBoysWHO regi<strong>on</strong>Income level
TABLE A.1 (CONTINUED)Other unintenti<strong>on</strong>al injuriesEstimated mortality by sex, age group, a WHO regi<strong>on</strong> and income level, b 2004Rate e per 100 000 populati<strong>on</strong>BoysWHO regi<strong>on</strong>Income level
TABLE A.2The 15 leading causes of mortality and DALYs am<strong>on</strong>g <strong>child</strong>ren under 15 years by sex and income level, 2004All Member StatesBoth sexesRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 26.8 1 Perinatal causes 23.02 Lower respiratory infecti<strong>on</strong>s 16.7 2 Lower respiratory infecti<strong>on</strong>s 13.13 Diarrhoeal diseases 14.9 3 Diarrhoeal diseases 11.64 Malaria 7.8 4 Malaria 6.65 Measles 3.5 5 C<strong>on</strong>genital anomalies 4.46 C<strong>on</strong>genital anomalies 3.3 6 Protein–energy malnutriti<strong>on</strong> 3.07 HIV/AIDS 2.5 7 Measles 2.78 Pertussis 2.1 8 Pertussis 2.09 Meningitis 1.9 9 HIV/AIDS 1.910 Protein–energy malnutriti<strong>on</strong> 1.4 10 Road traffic injuries 1.711 Road traffic injuries 1.4 11 Meningitis 1.612 Tetanus 1.2 12 Asthma 1.213 Drowning 1.1 13 Falls 1.114 Tuberculosis 0.7 14 Ir<strong>on</strong>-deficiency anaemia 1.115 Fire-related burns 0.6 15 Unipolar depressive disorders 1.0BoysRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 26.9 1 Perinatal causes 22.82 Lower respiratory infecti<strong>on</strong>s 16.5 2 Lower respiratory infecti<strong>on</strong>s 13.13 Diarrhoeal diseases 14.9 3 Diarrhoeal diseases 11.74 Malaria 7.8 4 Malaria 6.55 Measles 3.5 5 C<strong>on</strong>genital anomalies 4.36 C<strong>on</strong>genital anomalies 3.2 6 Protein–energy malnutriti<strong>on</strong> 3.07 HIV/AIDS 2.5 7 Measles 2.78 Pertussis 2.1 8 HIV/AIDS 1.99 Meningitis 1.7 9 Road traffic injuries 1.910 Road traffic injuries 1.6 10 Pertussis 1.811 Tetanus 1.5 11 Meningitis 1.512 Protein–energy malnutriti<strong>on</strong> 1.4 12 Falls 1.213 Drowning 1.4 13 Tetanus 1.114 Tuberculosis 0.7 14 Asthma 1.115 Syphilis 0.5 15 Drowning 1.1GirlsRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 26.6 1 Perinatal causes 23.32 Lower respiratory infecti<strong>on</strong>s 16.9 2 Lower respiratory infecti<strong>on</strong>s 13.13 Diarrhoeal diseases 14.9 3 Diarrhoeal diseases 11.64 Malaria 7.9 4 Malaria 6.65 Measles 3.5 5 C<strong>on</strong>genital anomalies 4.56 C<strong>on</strong>genital anomalies 3.4 6 Protein–energy malnutriti<strong>on</strong> 3.07 HIV/AIDS 2.6 7 Measles 2.78 Pertussis 2.2 8 HIV/AIDS 2.09 Meningitis 2.0 9 Pertussis 1.810 Protein–energy malnutriti<strong>on</strong> 1.5 10 Meningitis 1.711 Road traffic injuries 1.1 11 Road traffic injuries 1.612 Tetanus 0.9 12 Asthma 1.213 Drowning 0.9 13 Falls 1.114 Fire-related burns 0.7 14 Unipolar depressive disorders 1.115 Tuberculosis 0.7 15 Ir<strong>on</strong>-deficiency anaemia 1.1178 WORLD REPORT ON CHILD INJURY PREVENTION
TABLE A.2 (CONTINUED)All Member StatesHigh-income countriesRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 36.3 1 Perinatal causes 17.82 C<strong>on</strong>genital anomalies 19.2 2 C<strong>on</strong>genital anomalies 14.33 Road traffic injuries 5.7 3 Asthma 8.14 Lower respiratory infecti<strong>on</strong>s 3.4 4 Unipolar depressive disorders 5.65 Endocrine disorders 2.9 5 Migraine 3.86 Diarrhoeal diseases 2.4 6 Endocrine disorders 3.37 Drowning 2.0 7 Road traffic injuries 3.08 Leukaemia 1.7 8 Refractive errors 3.09 Violence 1.6 9 Schizophrenia 2.510 Fire-related burns 0.8 10 Diarrhoeal diseases 2.111 Meningitis 0.8 11 Dental caries 2.012 Inflammatory heart diseases 0.8 12 Falls 2.013 Falls 0.6 13 Lower respiratory infecti<strong>on</strong>s 1.414 Self-inflicted injuries 0.6 14 Epilepsy 1.115 Epilepsy 0.5 15 Otitis media 1.0Low-income and middle-income countriesRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 26.7 1 Perinatal causes 23.12 Lower respiratory infecti<strong>on</strong>s 16.8 2 Lower respiratory infecti<strong>on</strong>s 13.33 Diarrhoeal diseases 15.0 3 Diarrhoeal diseases 11.94 Malaria 7.9 4 Malaria 6.65 Measles 3.6 5 C<strong>on</strong>genital anomalies 4.26 C<strong>on</strong>genital anomalies 3.1 6 Protein–energy malnutriti<strong>on</strong> 3.07 HIV/AIDS 2.6 7 Measles 2.78 Pertussis 2.2 8 HIV/AIDS 2.09 Meningitis 1.9 9 Pertussis 1.810 Protein–energy malnutriti<strong>on</strong> 1.5 10 Road traffic injuries 1.711 Road traffic injuries 1.4 11 Meningitis 1.612 Tetanus 1.2 12 Falls 1.113 Drowning 1.1 13 Ir<strong>on</strong>-deficiency anaemia 1.114 Tuberculosis 0.7 14 Asthma 1.015 Fire-related burns 0.6 15 Unipolar depressive disorders 0.9WORLD REPORT ON CHILD INJURY PREVENTION 179
TABLE A.2 (CONTINUED)African Regi<strong>on</strong> aBoth sexesRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Lower respiratory infecti<strong>on</strong>s 20.0 1 Perinatal causes 17.72 Perinatal causes 18.8 2 Lower respiratory infecti<strong>on</strong>s 17.23 Malaria 15.5 3 Malaria 14.34 Diarrhoeal diseases 15.4 4 Diarrhoeal diseases 13.35 HIV/AIDS 5.3 5 HIV/AIDS 4.46 Measles 3.5 6 Protein–energy malnutriti<strong>on</strong> 3.17 Meningitis 2.1 7 Measles 3.08 Pertussis 2.0 8 C<strong>on</strong>genital anomalies 2.69 C<strong>on</strong>genital anomalies 1.8 9 Pertussis 2.010 Protein–energy malnutriti<strong>on</strong> 1.7 10 Meningitis 1.911 Road traffic injuries 1.3 11 Road traffic injuries 1.512 Tetanus 1.3 12 Tetanus 1.113 Tuberculosis 0.9 13 Tuberculosis 0.914 Fire-related burns 0.7 14 Fire-related burns 0.815 Syphilis 0.6 15 Ir<strong>on</strong>-deficiency anaemia 0.7BoysRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Lower respiratory infecti<strong>on</strong>s 10.2 1 Perinatal causes 17.92 Perinatal causes 10.2 2 Lower respiratory infecti<strong>on</strong>s 17.03 Diarrhoeal diseases 8.1 3 Malaria 14.14 Malaria 8.0 4 Diarrhoeal diseases 13.35 HIV/AIDS 2.7 5 HIV/AIDS 4.36 Measles 1.8 6 Protein–energy malnutriti<strong>on</strong> 3.07 Pertussis 1.0 7 Measles 2.98 Meningitis 1.0 8 C<strong>on</strong>genital anomalies 2.69 C<strong>on</strong>genital anomalies 0.9 9 Pertussis 1.710 Protein–energy malnutriti<strong>on</strong> 0.9 10 Meningitis 1.711 Tetanus 0.8 11 Road traffic injuries 1.612 Road traffic injuries 0.8 12 Tetanus 1.313 Tuberculosis 0.5 13 Tuberculosis 0.914 Syphilis 0.3 14 Fire-related burns 0.815 Fire-related burns 0.3 15 Ir<strong>on</strong>-deficiency anaemia 0.7GirlsRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Lower respiratory infecti<strong>on</strong>s 9.7 1 Perinatal causes 17.62 Perinatal causes 8.6 2 Lower respiratory infecti<strong>on</strong>s 17.43 Malaria 7.5 3 Malaria 14.64 Diarrhoeal diseases 7.4 4 Diarrhoeal diseases 13.35 HIV/AIDS 2.6 5 HIV/AIDS 4.66 Measles 1.7 6 Protein–energy malnutriti<strong>on</strong> 3.27 Meningitis 1.1 7 Measles 3.08 Pertussis 1.0 8 C<strong>on</strong>genital anomalies 2.79 Protein–energy malnutriti<strong>on</strong> 0.9 9 Meningitis 2.210 C<strong>on</strong>genital anomalies 0.8 10 Pertussis 1.811 Road traffic injuries 0.5 11 Road traffic injuries 1.412 Tetanus 0.5 12 Tuberculosis 0.813 Tuberculosis 0.4 13 Tetanus 0.814 Fire-related burns 0.3 14 Ir<strong>on</strong>-deficiency anaemia 0.815 Syphilis 0.3 15 Fire-related burns 0.7180 WORLD REPORT ON CHILD INJURY PREVENTION
TABLE A.2 (CONTINUED)Regi<strong>on</strong> of the AmericasBoth sexesRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 33.0 1 Perinatal causes 21.52 Lower respiratory infecti<strong>on</strong>s 11.7 2 C<strong>on</strong>genital anomalies 9.13 Diarrhoeal diseases 11.2 3 Lower respiratory infecti<strong>on</strong>s 7.54 C<strong>on</strong>genital anomalies 9.2 4 Diarrhoeal diseases 7.25 Protein–energy malnutriti<strong>on</strong> 3.7 5 Asthma 4.56 Road traffic injuries 2.4 6 Protein–energy malnutriti<strong>on</strong> 3.37 Meningitis 1.6 7 Endocrine disorders 3.08 Endocrine disorders 1.5 8 Unipolar depressive disorders 2.49 Drowning 1.3 9 Dental caries 2.210 Leukaemia 1.0 10 Road traffic injuries 2.111 Pertussis 0.9 11 Migraine 2.012 Violence 0.9 12 Refractive errors 1.213 HIV/AIDS 0.8 13 Ir<strong>on</strong>-deficiency anaemia 1.214 Ir<strong>on</strong>-deficiency anaemia 0.6 14 Falls 1.115 Malaria 0.5 15 Epilepsy 1.0BoysRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 33.4 1 Perinatal causes 21.92 Lower respiratory infecti<strong>on</strong>s 11.5 2 C<strong>on</strong>genital anomalies 8.93 Diarrhoeal diseases 11.1 3 Lower respiratory infecti<strong>on</strong>s 7.54 C<strong>on</strong>genital anomalies 8.9 4 Diarrhoeal diseases 7.25 Protein–energy malnutriti<strong>on</strong> 3.6 5 Asthma 3.96 Road traffic injuries 2.7 6 Protein–energy malnutriti<strong>on</strong> 3.27 Meningitis 1.6 7 Endocrine disorders 3.08 Drowning 1.6 8 Road traffic injuries 2.39 Endocrine disorders 1.5 9 Dental caries 2.110 Violence 1.0 10 Unipolar depressive disorders 2.111 Leukaemia 1.0 11 Violence 1.312 Pertussis 0.9 12 Falls 1.213 HIV/AIDS 0.7 13 Refractive errors 1.214 Ir<strong>on</strong>-deficiency anaemia 0.6 14 Ir<strong>on</strong>-deficiency anaemia 1.215 Nephritis and nephrosis 0.5 15 Migraine 1.2GirlsRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 32.4 1 Perinatal causes 20.92 Lower respiratory infecti<strong>on</strong>s 12.0 2 C<strong>on</strong>genital anomalies 9.43 Diarrhoeal diseases 11.4 3 Lower respiratory infecti<strong>on</strong>s 7.54 C<strong>on</strong>genital anomalies 9.5 4 Diarrhoeal diseases 7.15 Protein–energy malnutriti<strong>on</strong> 3.8 5 Asthma 5.26 Road traffic injuries 2.1 6 Protein–energy malnutriti<strong>on</strong> 3.37 Meningitis 1.6 7 Migraine 3.18 Endocrine disorders 1.5 8 Endocrine disorders 3.09 Leukaemia 1.0 9 Unipolar depressive disorders 2.810 Pertussis 1.0 10 Dental caries 2.311 Drowning 0.9 11 Road traffic injuries 1.912 HIV/AIDS 0.8 12 Refractive errors 1.313 Violence 0.8 13 Ir<strong>on</strong>-deficiency anaemia 1.314 Ir<strong>on</strong>-deficiency anaemia 0.6 14 Epilepsy 1.115 Malaria 0.5 15 Meningitis 1.0WORLD REPORT ON CHILD INJURY PREVENTION 181
TABLE A.2 (CONTINUED)Regi<strong>on</strong> of the AmericasHigh-income countriesRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 41.7 1 Perinatal causes 20.72 C<strong>on</strong>genital anomalies 19.0 2 C<strong>on</strong>genital anomalies 15.43 Road traffic injuries 5.7 3 Asthma 9.64 Violence 2.6 4 Unipolar depressive disorders 5.55 Endocrine disorders 2.1 5 Migraine 4.96 Drowning 1.9 6 Road traffic injuries 3.17 Lower respiratory infecti<strong>on</strong>s 1.6 7 Refractive errors 2.98 Fire-related burns 1.3 8 Endocrine disorders 2.29 Leukaemia 1.3 9 Dental caries 1.910 Inflammatory heart diseases 0.8 10 Schizophrenia 1.711 Self-inflicted injuries 0.8 11 Falls 1.412 Cerebrovascular disease 0.6 12 Violence 1.313 Meningitis 0.5 13 Epilepsy 1.114 Nephritis and nephrosis 0.4 14 Diarrhoeal diseases 1.115 Asthma 0.4 15 Otitis media 0.9Low-income and middle-income countriesRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 32.1 1 Perinatal causes 21.42 Lower respiratory infecti<strong>on</strong>s 12.7 2 Lower respiratory infecti<strong>on</strong>s 8.43 Diarrhoeal diseases 12.3 3 C<strong>on</strong>genital anomalies 8.24 C<strong>on</strong>genital anomalies 8.2 4 Diarrhoeal diseases 8.05 Protein–energy malnutriti<strong>on</strong> 4.0 5 Asthma 3.76 Road traffic injuries 2.1 6 Protein–energy malnutriti<strong>on</strong> 3.67 Meningitis 1.7 7 Endocrine disorders 3.08 Endocrine disorders 1.4 8 Dental caries 2.29 Drowning 1.2 9 Unipolar depressive disorders 1.910 Pertussis 1.0 10 Road traffic injuries 1.911 Leukaemia 1.0 11 Migraine 1.612 HIV/AIDS 0.8 12 Meningitis 1.413 Violence 0.7 13 Ir<strong>on</strong>-deficiency anaemia 1.314 Ir<strong>on</strong>-deficiency anaemia 0.7 14 Pertussis 1.215 Malaria 0.6 15 Epilepsy 1.0182 WORLD REPORT ON CHILD INJURY PREVENTION
TABLE A.2 (CONTINUED)South-East Asia Regi<strong>on</strong> aBoth sexesRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 33.1 1 Perinatal causes 27.82 Diarrhoeal diseases 16.2 2 Diarrhoeal diseases 12.53 Lower respiratory infecti<strong>on</strong>s 13.4 3 Lower respiratory infecti<strong>on</strong>s 10.64 Measles 5.2 4 C<strong>on</strong>genital anomalies 4.45 Pertussis 3.2 5 Measles 3.96 C<strong>on</strong>genital anomalies 3.2 6 Protein–energy malnutriti<strong>on</strong> 3.17 Malaria 2.0 7 Pertussis 2.88 Meningitis 1.5 8 Malaria 1.89 Tetanus 1.3 9 Falls 1.710 Protein–energy malnutriti<strong>on</strong> 1.0 10 Road traffic injuries 1.511 Drowning 0.9 11 Meningitis 1.412 Road traffic injuries 0.9 12 Ir<strong>on</strong>-deficiency anaemia 1.413 Fire-related burns 0.7 13 Unipolar depressive disorders 1.214 Cirrhosis of the liver 0.6 14 Fire-related burns 1.215 Tuberculosis 0.5 15 Tetanus 1.0BoysRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 32.9 1 Perinatal causes 27.42 Diarrhoeal diseases 16.5 2 Diarrhoeal diseases 12.93 Lower respiratory infecti<strong>on</strong>s 13.7 3 Lower respiratory infecti<strong>on</strong>s 10.94 Measles 5.4 4 C<strong>on</strong>genital anomalies 4.35 Pertussis 3.2 5 Measles 4.16 C<strong>on</strong>genital anomalies 2.9 6 Protein–energy malnutriti<strong>on</strong> 3.27 Malaria 2.0 7 Pertussis 2.78 Tetanus 1.7 8 Malaria 1.89 Meningitis 1.5 9 Falls 1.710 Road traffic injuries 1.0 10 Road traffic injuries 1.611 Drowning 1.0 11 Meningitis 1.412 Protein–energy malnutriti<strong>on</strong> 0.9 12 Ir<strong>on</strong>-deficiency anaemia 1.413 Fire-related burns 0.5 13 Tetanus 1.214 Tuberculosis 0.4 14 Unipolar depressive disorders 1.215 Falls 0.4 15 Lymphatic filariasis 1.1GirlsRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 33.3 1 Perinatal causes 28.22 Diarrhoeal diseases 15.8 2 Diarrhoeal diseases 12.23 Lower respiratory infecti<strong>on</strong>s 13.2 3 Lower respiratory infecti<strong>on</strong>s 10.44 Measles 5.0 4 C<strong>on</strong>genital anomalies 4.55 C<strong>on</strong>genital anomalies 3.4 5 Measles 3.86 Pertussis 3.2 6 Protein–energy malnutriti<strong>on</strong> 3.17 Malaria 1.9 7 Pertussis 2.78 Meningitis 1.5 8 Falls 1.89 Protein–energy malnutriti<strong>on</strong> 1.0 9 Malaria 1.710 Fire-related burns 0.9 10 Fire-related burns 1.611 Tetanus 0.9 11 Road traffic injuries 1.512 Drowning 0.8 12 Meningitis 1.413 Road traffic injuries 0.7 13 Ir<strong>on</strong>-deficiency anaemia 1.314 Cirrhosis of the liver 0.7 14 Migraine 1.315 Epilepsy 0.5 15 Unipolar depressive disorders 1.2WORLD REPORT ON CHILD INJURY PREVENTION 183
TABLE A.2 (CONTINUED)European Regi<strong>on</strong>Both sexesRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 33.2 1 Perinatal causes 21.62 Lower respiratory infecti<strong>on</strong>s 13.8 2 C<strong>on</strong>genital anomalies 9.83 Diarrhoeal diseases 12.4 3 Lower respiratory infecti<strong>on</strong>s 7.54 C<strong>on</strong>genital anomalies 10.3 4 Diarrhoeal diseases 7.15 Road traffic injuries 2.2 5 Iodine deficiency 4.06 Meningitis 2.2 6 Unipolar depressive disorders 3.17 Drowning 1.9 7 Asthma 2.78 Upper respiratory infecti<strong>on</strong>s 1.3 8 Falls 2.29 Leukaemia 1.0 9 Road traffic injuries 1.910 Endocrine disorders 0.8 10 Refractive errors 1.711 HIV/AIDS 0.7 11 Migraine 1.712 Pois<strong>on</strong>ing 0.6 12 Endocrine disorders 1.513 Fire-related burns 0.6 13 Schizophrenia 1.414 Epilepsy 0.5 14 Meningitis 1.415 Violence 0.5 15 Ir<strong>on</strong>-deficiency anaemia 1.3BoysRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 33.5 1 Perinatal causes 21.82 Lower respiratory infecti<strong>on</strong>s 13.4 2 C<strong>on</strong>genital anomalies 9.73 Diarrhoeal diseases 11.9 3 Lower respiratory infecti<strong>on</strong>s 7.54 C<strong>on</strong>genital anomalies 10.1 4 Diarrhoeal diseases 7.05 Road traffic injuries 2.5 5 Iodine deficiency 3.56 Drowning 2.2 6 Falls 2.77 Meningitis 2.0 7 Unipolar depressive disorders 2.68 Upper respiratory infecti<strong>on</strong>s 1.2 8 Asthma 2.39 Leukaemia 1.0 9 Road traffic injuries 2.010 Endocrine disorders 0.8 10 Refractive errors 1.611 Pois<strong>on</strong>ing 0.6 11 Schizophrenia 1.512 HIV/AIDS 0.6 12 Endocrine disorders 1.413 Fire-related burns 0.6 13 Meningitis 1.314 Self-inflicted injuries 0.5 14 Drowning 1.315 Epilepsy 0.5 15 Ir<strong>on</strong>-deficiency anaemia 1.2GirlsRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 32.8 1 Perinatal causes 21.22 Lower respiratory infecti<strong>on</strong>s 14.3 2 C<strong>on</strong>genital anomalies 10.03 Diarrhoeal diseases 12.9 3 Lower respiratory infecti<strong>on</strong>s 7.54 C<strong>on</strong>genital anomalies 10.6 4 Diarrhoeal diseases 7.25 Meningitis 2.4 5 Iodine deficiency 4.66 Road traffic injuries 1.9 6 Unipolar depressive disorders 3.77 Upper respiratory infecti<strong>on</strong>s 1.4 7 Asthma 3.18 Drowning 1.3 8 Migraine 2.39 Leukaemia 1.0 9 Refractive errors 1.910 Endocrine disorders 0.9 10 Road traffic injuries 1.711 HIV/AIDS 0.8 11 Endocrine disorders 1.612 Pois<strong>on</strong>ing 0.7 12 Falls 1.413 Fire-related burns 0.6 13 Ir<strong>on</strong>-deficiency anaemia 1.414 Epilepsy 0.5 14 Meningitis 1.415 Violence 0.5 15 Schizophrenia 1.3184 WORLD REPORT ON CHILD INJURY PREVENTION
TABLE A.2 (CONTINUED)European Regi<strong>on</strong>High-income countriesRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 38.4 1 Perinatal causes 16.72 C<strong>on</strong>genital anomalies 23.0 2 C<strong>on</strong>genital anomalies 15.13 Road traffic injuries 4.1 3 Asthma 8.04 Endocrine disorders 3.6 4 Unipolar depressive disorders 7.35 Leukaemia 2.3 5 Endocrine disorders 4.36 Lower respiratory infecti<strong>on</strong>s 1.4 6 Schizophrenia 3.67 Meningitis 1.3 7 Refractive errors 3.68 Drowning 1.3 8 Migraine 3.39 Violence 1.0 9 Dental caries 2.410 Inflammatory heart diseases 0.9 10 Falls 2.111 Epilepsy 0.9 11 Road traffic injuries 2.012 Falls 0.6 12 Diarrhoeal diseases 1.413 Cerebrovascular disease 0.6 13 Otitis media 1.114 Fire-related burns 0.5 14 Ir<strong>on</strong>-deficiency anaemia 1.115 Self-inflicted injuries 0.4 15 Epilepsy 1.1Low-income and middle-income countriesRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 32.6 1 Perinatal causes 22.52 Lower respiratory infecti<strong>on</strong>s 15.2 2 Lower respiratory infecti<strong>on</strong>s 9.03 Diarrhoeal diseases 13.7 3 C<strong>on</strong>genital anomalies 8.64 C<strong>on</strong>genital anomalies 8.8 4 Diarrhoeal diseases 8.35 Meningitis 2.3 5 Iodine deficiency 4.96 Road traffic injuries 2.0 6 Falls 2.27 Drowning 1.9 7 Unipolar depressive disorders 2.18 Upper respiratory infecti<strong>on</strong>s 1.4 8 Road traffic injuries 1.89 Leukaemia 0.9 9 Asthma 1.510 HIV/AIDS 0.7 10 Meningitis 1.411 Pois<strong>on</strong>ing 0.7 11 Ir<strong>on</strong>-deficiency anaemia 1.412 Fire-related burns 0.6 12 Migraine 1.413 Endocrine disorders 0.5 13 Refractive errors 1.314 Self-inflicted injuries 0.5 14 Protein-energy malnutriti<strong>on</strong> 1.315 Epilepsy 0.5 15 Drowning 1.2WORLD REPORT ON CHILD INJURY PREVENTION 185
TABLE A.2 (CONTINUED)Eastern Mediterranean Regi<strong>on</strong>Both sexesRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 28.6 1 Perinatal causes 25.42 Lower respiratory infecti<strong>on</strong>s 19.4 2 Lower respiratory infecti<strong>on</strong>s 15.33 Diarrhoeal diseases 14.6 3 Diarrhoeal diseases 11.44 C<strong>on</strong>genital anomalies 4.5 4 C<strong>on</strong>genital anomalies 5.45 Measles 3.0 5 Protein–energy malnutriti<strong>on</strong> 2.96 Malaria 2.8 6 Road traffic injuries 2.57 Road traffic injuries 2.2 7 Measles 2.38 Pertussis 2.1 8 Malaria 2.29 Meningitis 1.7 9 Pertussis 1.710 Protein–energy malnutriti<strong>on</strong> 1.6 10 Meningitis 1.411 Tetanus 1.5 11 Falls 1.412 War and c<strong>on</strong>flict 0.9 12 Tetanus 1.113 Syphilis 0.9 13 Iodine deficiency 1.114 Drowning 0.9 14 Ir<strong>on</strong>-deficiency anaemia 0.915 Tuberculosis 0.7 15 Fire-related burns 0.8BoysRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 28.9 1 Perinatal causes 25.12 Lower respiratory infecti<strong>on</strong>s 18.8 2 Lower respiratory infecti<strong>on</strong>s 15.03 Diarrhoeal diseases 14.4 3 Diarrhoeal diseases 11.34 C<strong>on</strong>genital anomalies 4.5 4 C<strong>on</strong>genital anomalies 5.55 Measles 2.9 5 Protein–energy malnutriti<strong>on</strong> 2.86 Malaria 2.7 6 Road traffic injuries 2.87 Road traffic injuries 2.6 7 Measles 2.38 Pertussis 2.1 8 Malaria 2.19 Tetanus 1.8 9 Pertussis 1.710 Meningitis 1.7 10 Meningitis 1.411 Protein–energy malnutriti<strong>on</strong> 1.5 11 Falls 1.412 Drowning 1.1 12 Tetanus 1.313 War and c<strong>on</strong>flict 1.0 13 Iodine deficiency 1.014 Syphilis 0.9 14 War and c<strong>on</strong>flict 0.915 Tuberculosis 0.7 15 Ir<strong>on</strong>-deficiency anaemia 0.9GirlsRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 28.3 1 Perinatal causes 25.62 Lower respiratory infecti<strong>on</strong>s 20.1 2 Lower respiratory infecti<strong>on</strong>s 15.73 Diarrhoeal diseases 14.9 3 Diarrhoeal diseases 11.54 C<strong>on</strong>genital anomalies 4.5 4 C<strong>on</strong>genital anomalies 5.45 Measles 3.1 5 Protein–energy malnutriti<strong>on</strong> 2.96 Malaria 2.9 6 Measles 2.37 Pertussis 2.2 7 Malaria 2.38 Road traffic injuries 1.7 8 Road traffic injuries 2.19 Meningitis 1.7 9 Pertussis 1.810 Protein–energy malnutriti<strong>on</strong> 1.6 10 Meningitis 1.411 Tetanus 1.1 11 Falls 1.312 Syphilis 0.9 12 Iodine deficiency 1.113 War and c<strong>on</strong>flict 0.8 13 Ir<strong>on</strong>-deficiency anaemia 1.014 Tuberculosis 0.7 14 Fire-related burns 1.015 Drowning 0.6 15 Migraine 1.0186 WORLD REPORT ON CHILD INJURY PREVENTION
TABLE A.2 (CONTINUED)Eastern Mediterranean Regi<strong>on</strong>High-income countriesRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal c<strong>on</strong>diti<strong>on</strong>s 27.0 1 Perinatal c<strong>on</strong>diti<strong>on</strong>s 19.22 C<strong>on</strong>genital anomalies 13.0 2 C<strong>on</strong>genital anomalies 10.83 Diarrhoeal diseases 10.8 3 Diarrhoeal diseases 6.64 Lower respiratory infecti<strong>on</strong>s 9.4 4 Road traffic injuries 5.85 Road traffic injuries 8.4 5 Lower respiratory infecti<strong>on</strong>s 5.56 Endocrine disorders 4.0 6 Endocrine disorders 5.07 Drowning 2.4 7 Protein–energy malnutriti<strong>on</strong> 2.58 Tuberculosis 1.2 8 Falls 2.59 Leukaemia 1.1 9 Asthma 2.110 Meningitis 0.9 10 Migraine 1.811 Falls 0.9 11 Unipolar depressive disorders 1.812 Nephritis and nephrosis 0.8 12 Malaria 1.813 Dengue 0.7 13 Dental caries 1.314 Violence 0.5 14 Drowning 1.315 Epilepsy 0.5 15 Ir<strong>on</strong>-deficiency anaemia 1.1Low-income and middle-income countriesRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 28.7 1 Perinatal causes 25.42 Lower respiratory infecti<strong>on</strong>s 19.5 2 Lower respiratory infecti<strong>on</strong>s 15.43 Diarrhoeal diseases 14.6 3 Diarrhoeal diseases 11.44 C<strong>on</strong>genital anomalies 4.4 4 C<strong>on</strong>genital anomalies 5.35 Measles 3.0 5 Protein–energy malnutriti<strong>on</strong> 2.96 Malaria 2.8 6 Malaria 2.67 Pertussis 2.1 7 Road traffic injuries 2.48 Road traffic injuries 2.1 8 Measles 2.39 Meningitis 1.7 9 Pertussis 1.910 Protein–energy malnutriti<strong>on</strong> 1.6 10 Meningitis 1.411 Tetanus 1.5 11 Falls 1.412 War and c<strong>on</strong>flict 0.9 12 Tetanus 1.113 Syphilis 0.9 13 Iodine deficiency 1.114 Drowning 0.9 14 Ir<strong>on</strong>-deficiency anaemia 0.915 Tuberculosis 0.7 15 Fire-related burns 0.9WORLD REPORT ON CHILD INJURY PREVENTION 187
TABLE A.2 (CONTINUED)Western Pacific Regi<strong>on</strong>Both sexesRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 39.4 1 Perinatal causes 28.02 Diarrhoeal diseases 10.0 2 Diarrhoeal diseases 6.83 Lower respiratory infecti<strong>on</strong>s 9.4 3 Lower respiratory infecti<strong>on</strong>s 6.24 Drowning 6.3 4 C<strong>on</strong>genital anomalies 5.75 C<strong>on</strong>genital anomalies 5.6 5 Drowning 4.06 Meningitis 2.0 6 Refractive errors 3.87 Road traffic injuries 1.9 7 Protein–energy malnutriti<strong>on</strong> 2.68 Endocrine disorders 1.5 8 Asthma 2.59 Malaria 1.3 9 Falls 2.410 Leukaemia 1.1 10 Unipolar depressive disorders 2.311 Tetanus 1.0 11 Road traffic injuries 2.012 Upper respiratory infecti<strong>on</strong>s 0.9 12 Meningitis 1.413 Measles 0.8 13 Ir<strong>on</strong>-deficiency anaemia 1.314 Protein–energy malnutriti<strong>on</strong> 0.7 14 Intestinal nematode infecti<strong>on</strong>s 1.215 Falls 0.7 15 Endocrine disorders 1.2BoysRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 37.9 1 Perinatal causes 26.72 Diarrhoeal diseases 9.8 2 Diarrhoeal diseases 6.63 Lower respiratory infecti<strong>on</strong>s 9.3 3 Lower respiratory infecti<strong>on</strong>s 6.14 Drowning 8.0 4 C<strong>on</strong>genital anomalies 5.45 C<strong>on</strong>genital anomalies 5.2 5 Drowning 4.96 Road traffic injuries 2.4 6 Refractive errors 3.97 Meningitis 2.0 7 Protein–energy malnutriti<strong>on</strong> 2.78 Endocrine disorders 1.6 8 Falls 2.49 Malaria 1.4 9 Asthma 2.310 Tetanus 1.3 10 Road traffic injuries 2.311 Leukaemia 1.1 11 Unipolar depressive disorders 2.212 Upper respiratory infecti<strong>on</strong>s 0.8 12 Schizophrenia 1.613 Falls 0.8 13 Alcohol use disorders 1.514 Protein–energy malnutriti<strong>on</strong> 0.8 14 Meningitis 1.415 Measles 0.8 15 Ir<strong>on</strong>-deficiency anaemia 1.4GirlsRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 41.0 1 Perinatal causes 29.52 Diarrhoeal diseases 10.2 2 Diarrhoeal diseases 7.03 Lower respiratory infecti<strong>on</strong>s 9.5 3 Lower respiratory infecti<strong>on</strong>s 6.44 C<strong>on</strong>genital anomalies 6.0 4 C<strong>on</strong>genital anomalies 6.15 Drowning 4.7 5 Refractive errors 3.76 Meningitis 1.9 6 Drowning 3.07 Endocrine disorders 1.5 7 Asthma 2.78 Road traffic injuries 1.4 8 Protein–energy malnutriti<strong>on</strong> 2.59 Malaria 1.2 9 Unipolar depressive disorders 2.410 Leukaemia 1.1 10 Falls 2.411 Upper respiratory infecti<strong>on</strong>s 0.9 11 Road traffic injuries 1.712 Measles 0.8 12 Meningitis 1.413 Pois<strong>on</strong>ing 0.8 13 Ir<strong>on</strong>-deficiency anaemia 1.314 Tetanus 0.7 14 Endocrine disorders 1.315 Protein–energy malnutriti<strong>on</strong> 0.7 15 Intestinal nematode infecti<strong>on</strong>s 1.2188 WORLD REPORT ON CHILD INJURY PREVENTION
TABLE A.2 (CONTINUED)Western Pacific Regi<strong>on</strong>High-income countriesRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal c<strong>on</strong>diti<strong>on</strong>s 28.1 1 C<strong>on</strong>genital anomalies 13.22 C<strong>on</strong>genital anomalies 23.3 2 Perinatal c<strong>on</strong>diti<strong>on</strong>s 10.93 Road traffic injuries 6.0 3 Asthma 10.04 Drowning 3.3 4 Unipolar depressive disorders 6.25 Leukaemia 2.9 5 Schizophrenia 4.66 Lower respiratory infecti<strong>on</strong>s 2.9 6 Refractive errors 4.27 Endocrine disorders 2.3 7 Migraine 3.88 Violence 1.8 8 Falls 2.89 Inflammatory heart diseases 1.2 9 Road traffic injuries 2.510 Self-inflicted injuries 1.1 10 Endocrine disorders 2.311 Epilepsy 1.0 11 Dental caries 2.312 Falls 1.0 12 Diarrhoeal diseases 1.813 Fire-related burns 1.0 13 Ir<strong>on</strong>-deficiency anaemia 1.614 Cerebrovascular disease 0.8 14 Alcohol use disorders 1.415 Meningitis 0.5 15 Self-inflicted injuries 1.3Low-income and middle-income countriesRank Cause of death Proporti<strong>on</strong> oftotal (%)Rank Cause of DALYs Proporti<strong>on</strong> oftotal (%)1 Perinatal causes 39.6 1 Perinatal causes 28.42 Diarrhoeal diseases 10.2 2 Diarrhoeal diseases 6.93 Lower respiratory infecti<strong>on</strong>s 9.5 3 Lower respiratory infecti<strong>on</strong>s 6.44 Drowning 6.4 4 C<strong>on</strong>genital anomalies 5.55 C<strong>on</strong>genital anomalies 5.4 5 Drowning 4.06 Meningitis 2.0 6 Refractive errors 3.77 Road traffic injuries 1.9 7 Protein–energy malnutriti<strong>on</strong> 2.68 Endocrine disorders 1.5 8 Falls 2.39 Malaria 1.3 9 Asthma 2.210 Leukaemia 1.1 10 Unipolar depressive disorders 2.211 Tetanus 1.0 11 Road traffic injuries 2.012 Upper respiratory infecti<strong>on</strong>s 0.9 12 Meningitis 1.413 Measles 0.8 13 Ir<strong>on</strong>-deficiency anaemia 1.314 Protein–energy malnutriti<strong>on</strong> 0.7 14 Intestinal nematode infecti<strong>on</strong>s 1.215 Falls 0.7 15 Endocrine disorders 1.2aNo high-income countries in the regi<strong>on</strong>.DALYs = disability-adjusted life years lost.Source: WHO (2008), Global Burden of Disease: 2004 update.WORLD REPORT ON CHILD INJURY PREVENTION 189
TABLE A.3Unintenti<strong>on</strong>al injuries <str<strong>on</strong>g>report</str<strong>on</strong>g>ed by 13–15-year-olds included in the Global School Health SurveyCountry Botswana Cayman Islands a Chile(Metropolitan)Year200520072004Overall resp<strong>on</strong>se rate95.0%79.0%85.0%Number of schools25825All students219712992111China(Beijing)200399.0%252348Djibouti200783.0%111777Sample n % n % n % n % n %Students 13–15 yrs 1375 63.4 935 73.3 1766 81.1 1936 81.6 923 52.7Sex n % n % n % n % n %Male 581 46.4 474 53.9 812 50.9 922 49.8 535 60.1Female 788 53.6 457 46.1 951 49.1 1014 50.2 387 39.9Injuries % 95% CI % % 95% CI % 95% CI % 95% CIAny <strong>injury</strong> 65.8 62.4–69.1 50.2 – 36.4 33.9–39.0 16.4 14.5–18.4 60.6 56.1–65.0Unintenti<strong>on</strong>al <strong>injury</strong> 56.0 50.6–61.4 86.0 – 83.6 80.3–86.9 83.6 78.5–88.8 57.3 49.4–65.1Cause of <strong>injury</strong> n % n % n % n % n %Road traffic <strong>injury</strong> 41 12.3 16 5.8 13 3.5 7 3.1 9 6.9Fall 114 34.8 79 26.6 208 46.6 84 40.0 64 45.9Burn 27 7.7 11 3.3 4 1.0 7 3.2 1 0.7Struck by an object 51 15.2 24 9.1 25 5.9 35 16.4 16 11.3Other 99 30.0 154 55.1 200 43.1 80 37.2 48 35.2Total 332 100.0 284 100.0 450 100.0 213 100.0 138 100.0Activity n % n % n % n % n %Playing a sport 107 32.8 105 37.9 232 52.1 43 20.4 51 40.4Walking/running 47 14.4 27 8.7 55 12.9 42 19.7 8 6.1Riding a two-wheeler 70 21.5 75 26.2 41 9.2 29 14.3 18 14.7Driving motor vehicle 18 5.5 6 2.4 7 1.6 5 2.3 8 6.2Doing work 40 11.3 11 3.2 12 2.3 12 5.5 3 2.1Nothing 25 7.2 12 3.8 13 2.7 31 14.3 16 12.5Something else 22 7.3 52 17.7 90 19.2 51 23.6 22 18.1Total 329 100.0 288 100.0 450 100.0 213 100.0 126 100.0Nature of <strong>injury</strong> n % n % n % n % n %Fracture or dislocati<strong>on</strong> 78 23.7 71 27.8 214 48.3 60 28.4 17 13.5Penetrating <strong>injury</strong> 108 33.7 67 23.7 24 5.5 30 14.1 17 12.7Head <strong>injury</strong> 33 9.4 17 6.8 29 6.5 6 2.8 29 21.8Gunshot wound 11 3.4 10 3.7 1 0.3 0 0.0 25 18.7Burn 45 12.9 19 7.0 6 1.4 3 1.4 6 4.5Amputati<strong>on</strong> 11 3.3 1 0.3 4 0.8 2 0.9 5 3.7Other 46 13.6 84 30.7 173 37.2 111 52.4 32 25.1Total 332 100.0 269 100.0 451 100.0 212 100.0 131 100.0190 WORLD REPORT ON CHILD INJURY PREVENTION
TABLE A.3 (CONTINUED)Country Egypt Guatemala(Capital City)Year20062006Overall resp<strong>on</strong>se rate87.0%41.0%Number of schools5119All students5249898Guyana200480.0%251212200495.0%262457Jordan200799.8%252197Sample n % n % n % n % n %Students 13–15 yrs 3910 75.4 690 78.2 1052 86.6 1844 74.0 1631 73.9Sex n % n % n % n % n %Male 2082 54.1 275 44.8 415 47.0 820 48.4 916 47.5Female 1795 45.9 412 55.2 626 53.0 1004 51.6 711 52.5Injuries % 95% CI % 95% CI % 95% CI % 95% CI % 95% CIAny <strong>injury</strong> 38.5 33.4–43.6 33.0 28.3–37.8 33.3 29.1–37.6 36.1 33.0–39.3 43.5 36.5–50.5Unintenti<strong>on</strong>al <strong>injury</strong> 83.5 78.9–88.2 72.3 66.2–78.3 68.4 61.9–75.0 80.9 76.8–85.0 77.4 72.0–82.8Cause of <strong>injury</strong> n % n % n % n % n %Road traffic <strong>injury</strong> 126 28.3 9 8.7 14 8.8 17 4.8 17 4.6Fall 100 23.7 59 52.0 55 35.7 91 23.6 91 26.9Burn 8 1.6 0 0.0 3 1.5 7 1.8 7 2.2Struck by an object 59 14.9 11 7.7 17 12.0 63 16.8 72 22.0Other 121 31.5 32 31.6 68 42.0 206 52.9 140 40.9Total 414 100.0 111 100.0 157 100.0 384 100.0 327 100.0Activity n % n % n % n % n %Playing a sport 203 47.1 72 62.9 27 19.9 101 27.2 105 30.7Walking/running 108 24.4 11 10.1 27 17.4 59 15.0 42 13.8Riding a two-wheeler 33 7.9 4 2.3 18 11.7 20 5.3 18 5.2Driving motor vehicle 15 3.1 3 3.7 6 4.4 14 3.9 9 2.7Doing work 18 4.7 9 7.3 18 10.6 21 5.9 22 7.6Nothing 31 8.1 2 0.9 20 11.8 78 19.3 46 15.4Something else 22 4.7 14 12.9 39 24.2 91 23.4 74 24.5Total 430 100.0 115 100.0 155 100.0 384 100.0 316 100.0Nature of <strong>injury</strong> n % n % n % n % n %Fracture or dislocati<strong>on</strong> 170 36.3 54 46.6 34 22.3 103 27.0 91 28.2Penetrating <strong>injury</strong> 146 37.5 0 0.0 48 31.7 73 20.1 56 16.7Head <strong>injury</strong> 27 6.9 6 4.5 6 3.7 23 6.1 34 10.7Gunshot wound 9 2.3 1 1.0 1 0.6 1 0.4 4 1.2Burn 8 2.0 3 2.4 9 5.7 13 3.3 6 2.1Amputati<strong>on</strong> 5 1.2 0 0.0 2 1.1 1 0.2 2 0.5Other 51 13.8 45 45.5 57 35.0 168 43.0 120 40.6Total 416 100.0 109 100.0 157 100.0 382 100.0 313 100.0WORLD REPORT ON CHILD INJURY PREVENTION 191
TABLE A.3 (CONTINUED)Country Kenya Leban<strong>on</strong> Libyan ArabJamahiriyaYear200320052007Overall resp<strong>on</strong>se rate84.0%88.0%98.0%Number of schools509250All students369151152242Morocco b200684.0%252670Namibia c200482.0%956367Sample n % n % n % n % n %Students 13–15 yrs 2758 75.1 3754 73.4 1492 69.3 1866 72.8 4251 63.4Sex n % n % n % n % n %Male 1280 47.7 1743 48.3 646 51.1 888 53.3 1852 42.7Female 1462 52.3 2009 51.7 828 48.9 953 46.7 2370 57.3Injuries % 95% CI % 95% CI % 95% CI % 95% CI % 95% CIAny <strong>injury</strong> 71.0 66.4–75.6 31.1 29.1–33.1 40.3 36.7–43.9 44.7 40.6–48.8 60.2 55.8–64.6Unintenti<strong>on</strong>al <strong>injury</strong> 64.1 60.7–67.5 85.8 83.4–88.2 74.2 68.3–80.1 65.7 60.1–71.3 60.0 56.4–63.5Cause of <strong>injury</strong> n % n % n % n % n %Road traffic <strong>injury</strong> 107 15.5 50 7.0 20 12.3 41 13.8 105 14.0Fall 231 30.1 204 28.9 28 17.6 135 46.0 237 21.7Burn 58 7.7 23 3.1 7 3.8 9 2.6 65 8.7Struck by an object 165 21.7 159 22.8 22 12.4 29 10.4 128 15.0Other 203 24.9 273 38.2 89 53.9 80 27.1 351 40.5Total 764 100.0 709 100.0 166 100.0 294 100.0 886 100.0Activity n % n % n % n %Playing a sport 224 30.9 234 33.4 74 47.1 123 44.6Walking/running 215 27.8 89 12.5 31 16.4 25 9.1Riding a two-wheeler 162 20.3 88 12.4 11 6.3 33 11.3Driving motor vehicle 25 3.2 33 4.9 9 4.6 14 5.5Doing work 59 7.2 41 5.9 13 6.7 11 4.4Nothing 60 7.5 81 11.0 16 7.6 33 12.0Something else 23 3.2 144 20.0 22 11.3 38 13.1Total 768 100.0 710 100.0 176 100.0 277 100.0Nature of <strong>injury</strong> n % n % n % n %Fracture or dislocati<strong>on</strong> 234 30.4 262 37.5 42 24.7 209 21.3Penetrating <strong>injury</strong> 290 38.9 166 23.2 50 30.9 176 19.0Head <strong>injury</strong> 69 9.5 83 11.7 15 9.9 74 9.5Gunshot wound 23 3.3 9 1.4 3 1.7 24 2.6Burn 36 4.5 26 3.6 5 2.6 56 7.6Amputati<strong>on</strong> 21 3.3 6 0.9 1 0.5 54 6.6Other 87 10.1 157 21.7 56 29.8 296 33.3Total 760 100.0 709 100.0 172 100.0 889 100.0192 WORLD REPORT ON CHILD INJURY PREVENTION
TABLE A.3 (CONTINUED)Country Oman Philippines Saint Lucia Saint Vincent andthe GrenadinesYearOverall resp<strong>on</strong>se rateNumber of schoolsAll students200597.0%512979200384.0%1487338200781.0%735657200782.0%201276200784.0%261333Sample n % n % n % n % n %Students 13–15 yrs 2280 77.7 4160 69.9 3433 61.1 864 69.4 1029 74.7Sex n % n % n % n % n %Male 1109 52.6 1643 40.9 1383 49.4 371 45.3 473 47.5Female 1146 47.4 2495 59.1 2047 50.6 492 54.7 554 52.5Injuries % 95% CI % 95% CI % 95% CI % 95% CI % 95% CIAny <strong>injury</strong> 26.6 22.5–30.7 29.9 26.2–33.6 46.0 43.0–49.0 47.8 43.4–52.3 48.4 41.0–55.7Unintenti<strong>on</strong>al <strong>injury</strong> 83.2 79.3–87.1 77.9 74.0–81.8 81.9 78.7–85.0 77.9 72.3–83.6 67.7 60.1–75.3Cause of <strong>injury</strong> n % n % n % n % n %Road traffic <strong>injury</strong> 23 7.4 91 11.7 78 14.1 13 5.7 12 6.5Fall 109 33.3 128 24.6 136 23.9 100 41.8 79 40.7Burn 2 0.6 25 4.4 6 1.1 1 0.4 6 3.1Struck by an object 32 9.8 63 9.3 91 17.7 15 6.6 18 8.5Other 159 49.0 278 47.4 256 43.3 109 45.6 86 41.3Total 325 100.0 585 100.0 567 100.0 238 100.0 201 100.0Activity n % n % n % n % n %Playing a sport 115 36.7 158 28.8 163 30.0 64 28.5 43 21.6Walking/running 43 13.1 108 17.5 114 19.0 33 13.4 45 24.9Riding a two-wheeler 16 5.3 49 6.5 68 10.9 30 13.9 23 11.9Driving motor vehicle 10 3.1 18 2.8 14 2.2 5 1.9 6 2.8Doing work 14 4.3 90 15.7 81 12.1 19 8.1 26 12.0Nothing 75 22.9 78 14.5 85 14.2 12 4.7 16 7.9Something else 48 14.5 71 14.1 69 11.7 72 29.4 37 19.0Total 321 100.0 572 100.0 594 100.0 235 100.0 196 100.0Nature of <strong>injury</strong> n % n % n % n % n %Fracture or dislocati<strong>on</strong> 73 22.8 118 18.9 115 23.1 59 28.1 53 28.5Penetrating <strong>injury</strong> 93 29.1 116 20.9 88 19.1 65 26.3 67 33.3Head <strong>injury</strong> 14 4.4 66 13.1 65 12.9 11 5.0 5 2.9Gunshot wound 5 1.6 5 1.0 5 1.4 2 0.8 2 1.4Burn 14 4.4 13 1.5 2 0.5 9 3.4 11 5.7Amputati<strong>on</strong> 125 37.4 2 0.4 5 0.8 0 0.0 0 0.0Other 1 0.3 259 44.3 230 42.2 86 36.4 59 28.1Total 325 100.0 579 100.0 510 100.0 232 100.0 197 100.0WORLD REPORT ON CHILD INJURY PREVENTION 193
TABLE A.3 (CONTINUED)Country Swaziland Tajikistan Trinidad andTobagoYearOverall resp<strong>on</strong>se rateNumber of schoolsAll students200396.0%977341200680.0%999714200778.0%322969Uganda200369.0%453215United Republicof Tanzania(Dar es Salaam)200687.0%252176Sample n % n % n % n % n %Students 13–15 yrs 6784 95.4 7395 76.3 2095 69.1 1878 60.5 1217 49.6Sex n % n % n % n % n %Male 2341 35.6 3629 54.1 1018 50.1 880 47.6 649 51.4Female 4240 64.4 3694 45.9 1063 49.9 963 52.4 560 48.6Injuries % 95% CI % 95% CI % 95% CI % 95% CI % 95% CIAny <strong>injury</strong> 38.6 36.7–40.4 17.6 14.1–21.1 46.5 43.1–49.8 63.4 58.5–68.4 39.9 36.1–43.7Unintenti<strong>on</strong>al <strong>injury</strong> 58.4 56.0–60.9 82.0 75.4–88.6 75.4 71.5–79.2 71.6 67.7–75.7 89.6 86.3–92.8Cause of <strong>injury</strong> n % n % n % n % n %Road traffic <strong>injury</strong> 121 11.6 29 12.6 24 7.6 84 14.0 17 5.2Fall 366 35.5 117 57.0 173 38.3 227 38.8 133 50.7Burn 73 6.8 2 0.9 2 0.3 46 7.8 23 8.6Struck by an object 126 11.7 14 6.5 66 13.9 98 16.7 39 13.4Other 367 34.4 33 23.0 182 38.9 142 22.7 67 22.1Total 1053 100.0 195 100.0 447 100.0 597 100.0 279 100.0Activity n % n % n % n % n %Playing a sport 342 32.6 135 58.6 176 37.4 233 38.5 100 38.9Walking/running 157 14.7 33 13.4 38 8.3 117 19.4 41 17.9Riding a two-wheeler 119 11.7 28 19.0 55 12.4 97 17.1 38 13.8Driving motor vehicle 52 5.2 3 1.1 15 4.1 17 2.6 5 1.5Doing work 141 13.2 13 4.4 35 5.8 54 9.2 8 3.3Nothing 93 8.7 4 2.2 21 5.4 41 7.1 46 19.2Something else 146 13.9 4 1.3 112 26.6 39 6.1 14 5.5Total 1050 100.0 220 100.0 452 100.0 598 100.0 252 100.0Nature of <strong>injury</strong> n % n % n % n % n %Fracture or dislocati<strong>on</strong> 314 30.0 92 47.5 102 24.1 186 30.3 61 23.4Penetrating <strong>injury</strong> 310 30.1 39 20.0 124 24.8 238 40.2 60 20.8Head <strong>injury</strong> 62 6.0 27 14.4 21 5.0 45 7.7 42 15.5Gunshot wound 7 0.7 0 0.0 4 0.7 8 1.5 4 2.1Burn 89 8.8 12 4.9 20 5.7 35 5.7 33 13.9Amputati<strong>on</strong> 24 2.6 3 2.1 2 0.0 21 3.6 6 3.5Other 237 21.9 21 11.1 165 39.8 64 11.0 47 20.9Total 1043 100.0 194 100.0 438 100.0 597 100.0 253 100.0194 WORLD REPORT ON CHILD INJURY PREVENTION
TABLE A.3 (CONTINUED)Country Uruguay Zambia Zimbabwe (Harare)YearOverall resp<strong>on</strong>se rateNumber of schoolsAll students200671.0%953406200470.0%472257200384.0%251997Sample n % n % n %Students 13–15 yrs 2372 70.4 1241 58.9 1435 72.8Sex n % n % n %Male 1070 45.1 553 51.5 604 47.8Female 1296 54.9 651 48.5 823 52.2Injuries % 95% CI % 95% CI % 95% CIAny <strong>injury</strong> 25.5 23.7–27.3 71.5 65.5–77.4 57.1 49.7–64.5Unintenti<strong>on</strong>al <strong>injury</strong> 86.3 82.9–89.7 61.7 55.6–67.8 68.6 64.0–73.3Cause of <strong>injury</strong> n % n % n %Road traffic <strong>injury</strong> 38 10.5 54 26.5 49 12.5Fall 152 37.3 43 20.2 143 36.6Burn 3 0.6 18 9.4 33 8.1Struck by an object 47 11.1 43 21.5 62 14.9Other 164 40.5 51 22.5 107 27.9Total 404 100.0 209 100.0 394 100.0Activity n % n % n %Playing a sport 223 54.2 79 38.8 123 32.2Walking/running 26 6.6 40 18.8 68 17.3Riding a two-wheeler 53 13.7 20 8.7 65 16.4Driving motor vehicle 22 5.7 6 2.8 15 3.6Doing work 11 2.9 29 15.2 63 14.8Nothing 6 1.7 25 11.7 24 6.8Something else 62 15.2 9 3.9 38 8.9Total 403 100.0 208 100.0 396 100.0Nature of <strong>injury</strong> n % n % n %Fracture or dislocati<strong>on</strong> 145 36.2 52 23.4 146 38.3Penetrating <strong>injury</strong> 29 7.7 40 19.2 90 23.2Head <strong>injury</strong> 24 6.2 32 16.7 49 12.4Gunshot wound 0 0.0 8 4.0 6 1.5Burn 9 2.1 20 10.5 28 6.6Amputati<strong>on</strong> 0 0.0 16 6.6 13 3.7Other 187 47.8 41 19.5 58 14.2Total 394 100.0 209 100.0 390 100.0CI = C<strong>on</strong>fidence interval.aNo c<strong>on</strong>fidence intervals available.bDid not collect informati<strong>on</strong> about the nature of <strong>injury</strong>.cDid not collect informati<strong>on</strong> about activity.Source: WHO Global School Health Survey (http://www.who.int/chp/gshs/en/, accessed 18 July 2008).WORLD REPORT ON CHILD INJURY PREVENTION 195
TABLE B.1Child mortality and <strong>injury</strong> in AsiaAll countries surveyedBoth sexes (age in years)
TABLE B.1 (CONTINUED)BangladeshBoys (age in years)Girls (age in years)
TABLE B.1 (CONTINUED)Jiangxi, ChinaBoys (age in years)Girls (age in years)
TABLE B.1 (CONTINUED)PhilippinesBoth sexes (age in years) c
TABLE C.1Unintenti<strong>on</strong>al injuries am<strong>on</strong>g <strong>child</strong>ren a presenting to emergency departments in four low-income countries, b 2007Road traffic injuries(n=350)Drowning(n=20)Burns(n=210)n % n % n %Sex Boys 247 70.6 11 55.0 111 52.9Girls 103 29.4 9 45.0 99 47.1Age 0–12 m<strong>on</strong>ths 2 0.6 1 5.0 8 3.81–4 years 76 21.7 8 40.0 110 52.4≥5 years 272 77.7 11 55.0 92 43.8Time of <strong>injury</strong> Morning (06:01–12:00) 128 36.6 6 30.0 80 38.1Lunchtime (12:01–14:30) 71 20.3 4 20.0 40 19.0Afterno<strong>on</strong> (14:31–17:00) 39 11.1 0 0 39 18.6Evening (17:01–20:00) 53 15.1 4 20.0 26 12.4Night (20:01–06:00) 59 16.9 6 30.0 25 11.9Mode oftransport tohospitalWhobrought <strong>child</strong>to hospital?Activity at timeof <strong>injury</strong>Where did<strong>injury</strong> occur?Nature of mostsevere <strong>injury</strong>Outcome after<strong>injury</strong>Estimated l<strong>on</strong>gtermeffect of<strong>injury</strong>Private car 86 24.6 11 55.0 44 21.0Public ambulance 59 16.9 0 0 14 6.7Private ambulance 48 13.7 1 5.0 19 9.0Motorcycle 17 4.9 1 5.0 1 0.5Bicycle 3 0.9 0 0 1 0.5Walking 31 8.9 2 10.0 18 8.6Taxi 80 22.9 5 25.0 109 51.9Other 26 7.4 0 0 4 1.9Mother 111 31.7 6 30.0 78 37.1Father 159 45.4 9 45.0 108 51.4Other family member 51 14.6 5 25.0 22 10.5Friend 5 1.4 0 0 2 1.0Teacher 2 0.6 0 0 0 0Other 22 6.3 0 0 0 0Sports 11 3.1 0 0 1 0.5Leisure/play 104 29.7 17 85.0 145 69.0Travelling 156 44.6 0 0 1 0.5Work (paid and unpaid) 19 5.4 0 0 15 7.1Educati<strong>on</strong>al activity 19 5.4 0 0 2 1.0Daily living 26 7.4 1 5.0 22 10.5Other/unknown/refused to answer 15 4.3 2 10.0 24 11.4Home (inside) 5 1.4 4 20.0 142 67.6Home (outside) 57 16.3 7 35.0 19 9.0Road/street/highway 249 71.1 2 10.0 2 1.0Countryside/farm/marketplace 2 0.6 1 5.0 1 0.5Other public building 2 0.6 6 30.0 44 21.0School/sports/play area 3 0.9 0 0 2 1.0Other/unknown 5 1.4 4 20.0 142 67.6C<strong>on</strong>cussi<strong>on</strong> 80 26.0 3 15.0 1 0.5Cut/bite/open wound 78 25.3 7 35.0 0 0Fracture 65 21.1 1 5.0 0 0Sprain 33 10.7 1 5.0 0 0Bruise 42 13.6 3 15.0 2 1.0Burn 2 0.6 1 5.0 191 96.0Organ system 3 1.0 4 20.0 1 0.5Other/unknown 5 1.6 0 0 4 2.0Treated and discharged home 173 55.1 11 55.0 41 19.7Admitted to a ward/intensive care unit/burn unit 100 31.8 4 20.0 164 78.8Admitted for emergency surgery 20 6.4 0 0 0 0Died in emergency room 2 0.6 2 10.0 0 0Referred to another centre 9 2.9 3 15.0 2 1.0Left before treatment completed 3 1.0 0 0 1 0.5Other/unknown 7 2.2 0 0 0 0No significant disability 119 34.0 13 65.0 108 51.4Short-term temporary disability (
TABLE C.1 (CONTINUED)Falls(n=913)Pois<strong>on</strong>ing(n=66)Total(n=1559)n % n % n %Sex Boys 598 65.5 43 65.2 1010 64.8Girls 315 34.5 23 34.8 549 35.2Age 0–12 m<strong>on</strong>ths 20 2.2 1 1.5 32 2.11–4 years 355 38.9 37 56.1 586 37.6≥5 years 538 58.9 28 42.4 941 60.4Time of <strong>injury</strong> Morning (06:01–12:00) 294 32.2 27 40.9 535 34.3Lunchtime (12:01–14:30) 203 22.2 13 19.7 331 21.2Afterno<strong>on</strong> (14:31–17:00) 136 14.9 9 13.6 223 14.3Evening (17:01–20:00) 112 12.3 7 10.6 202 13.0Night (20:01–06:00) 168 18.4 10 15.2 268 17.2Mode oftransport tohospitalWhobrought <strong>child</strong>to hospital?Activity at timeof <strong>injury</strong>Where did<strong>injury</strong> occur?Nature of mostsevere <strong>injury</strong>Outcome after<strong>injury</strong>Estimated l<strong>on</strong>gtermeffect of<strong>injury</strong>Private car 263 28.8 27 40.9 431 27.6Public ambulance 77 8.4 6 9.1 156 10.0Private ambulance 33 3.6 3 4.5 104 6.7Motorcycle 26 2.8 4 6.1 49 3.1Bicycle 3 0.3 0 0 7 0.4Walking 123 13.5 7 10.6 181 11.6Taxi 303 33.2 10 15.2 507 32.5Other 85 9.3 9 13.6 124 8.0Mother 376 41.2 35 53.0 606 38.9Father 412 45.1 25 37.9 713 45.7Other family member 92 10.1 6 9.1 176 11.3Friend 9 1.0 0 0 16 1.0Teacher 12 1.3 0 0 14 0.9Other 12 1.3 0 0 34 2.2Sports 42 4.6 2 3.0 56 3.6Leisure/play 684 74.9 36 54.5 986 63.2Travelling 16 1.8 1 1.5 174 11.2Work (paid or unpaid) 37 4.1 1 1.5 72 4.6Educati<strong>on</strong>al activity 23 2.5 1 1.5 45 2.9Daily living 80 8.8 18 27.3 147 9.4Other/unknown/refused to answer 31 3.4 7 10.6 79 5.1Home (inside) 351 38.4 41 62.1 543 34.8Home (outside) 237 26.0 9 13.6 329 21.1Road/street/highway 44 4.8 1 1.5 328 21.0Countryside/farm/marketplace 9 1.0 0 0 12 0.8Other public building 157 17.2 13 19.7 222 14.2School/sports/play area 96 10.5 2 3.0 103 6.6Other/unknown 19 2.1 0 0 21 1.3C<strong>on</strong>cussi<strong>on</strong> 134 17.0 0 0 218 16.0Cut/bite/open wound 200 25.3 1 2.1 286 21.0Fracture 195 24.7 1 2.1 262 19.2Sprain 93 11.8 1 2.1 128 9.4Bruise 152 19.2 0 0 199 14.6Burn 4 0.5 6 12.8 204 15.0Organ system 1 0.1 27 57.4 36 2.6Other/unknown 11 1.4 11 23.4 31 2.3Treated and discharged home 717 79.0 52 78.8 994 65.6Admitted to a ward/intensive care unit/burn unit 136 15.0 10 15.2 414 27.3Admitted for emergency surgery 15 1.7 1 1.5 36 2.4Died in emergency room 2 0.2 0 0 6 0.4Referred to another centre 14 1.5 1 1.5 29 1.9Left before treatment completed 4 0.4 2 3.0 10 0.7Other/unknown 20 2.2 0 0 27 1.8No significant disability 483 53.0 53 80.3 776 51.0Short-term temporary disability (
TABLE D.1WHO regi<strong>on</strong>s and countries (in 2004)African Regi<strong>on</strong> Regi<strong>on</strong> of the Americas South-East Asia Regi<strong>on</strong> European Regi<strong>on</strong> Eastern Mediterranean Regi<strong>on</strong> Western Pacific Regi<strong>on</strong>46 Member States 35 Member States 11 Member States 51 Member States 22 Member States 27 Member StatesLow-income and middle-income High-income Low-income and middle-income High-income High-income High-incomeAlgeria Antigua and Barbuda Bangladesh Andorra Bahrain AustraliaAngola Bahamas Bhutan Austria Cyprus Brunei DarussalamBenin Barbados Democratic People’s Republic of Korea Belgium Kuwait JapanBotswana Canada India Denmark Qatar New ZealandBurkina Faso United States of America Ind<strong>on</strong>esia Finland United Arab Emirates Republic of KoreaBurundi Low-income and middle-income Maldives France Low-income and middle-income SingaporeCamero<strong>on</strong> Argentina Myanmar Germany Afghanistan Low-income and middle-incomeCape Verde Belize Nepal Greece Djibouti CambodiaCentral African Republic Bolivia Sri Lanka Iceland Egypt ChinaChad Brazil Thailand Ireland Iraq Cook IslandsComoros Chile Timor-Leste Israel Islamic Republic of Iran Federated States of Micr<strong>on</strong>esiaC<strong>on</strong>go Colombia Italy Jordan FijiCôte d’Ivoire Costa Rica Luxembourg Leban<strong>on</strong> KiribatiDemocratic Republic of the C<strong>on</strong>go Cuba Malta Libyan Arab Jamahiriya Lao People’s Democratic RepublicEquatorial Guinea Dominica M<strong>on</strong>aco Morocco MalaysiaEritrea Dominican Republic Netherlands Oman Marshall IslandsEthiopia Ecuador Norway Pakistan M<strong>on</strong>goliaGab<strong>on</strong> El Salvador Portugal Saudi Arabia NauruGambia Grenada San Marino Somalia NiueGhana Guatemala Slovenia Sudan PalauGuinea Guyana Spain Syrian Arab Republic Papua New GuineaGuinea-Bissau Haiti Sweden Tunisia PhilippinesKenya H<strong>on</strong>duras Switzerland Yemen SamoaLesotho Jamaica United Kingdom Solom<strong>on</strong> IslandsLiberia Mexico Low-income and middle-income T<strong>on</strong>gaMadagascar Nicaragua Albania TuvaluMalawi Panama Armenia VanuatuMali Paraguay Azerbaijan Viet NamMauritania Peru BelarusMauritius Saint Kitts and Nevis Bosnia and HerzegovinaMozambique Saint Lucia BulgariaNamibia Saint Vincent and the Grenadines CroatiaNiger Suriname Czech RepublicNigeria Trinidad and Tobago Est<strong>on</strong>iaRwanda Uruguay GeorgiaSao Tome and Principe Venezuela HungarySenegal KazakhstanSeychelles KyrgyzstanSierra Le<strong>on</strong>e LatviaSouth Africa LithuaniaSwaziland MoldovaTogo PolandUganda RomaniaUnited Republic of Tanzania Zambia Russian Federati<strong>on</strong>Serbia and M<strong>on</strong>tenegroZimbabwe SlovakiaTajikistanThe former Yugoslav Republicof Maced<strong>on</strong>iaTurkeyTurkmenistanUkraineUzbekistan202 WORLD REPORT ON CHILD INJURY PREVENTION
INDEXIndexAbdominal injuries 33, 105Access to care 10, 13burns 90drowning 66improving 19lack of 41, 110pois<strong>on</strong>ing 132recommendati<strong>on</strong>s 151–152Accommodati<strong>on</strong> 10Acetaminophen (paracetamol) 126, 132Ackee fruit 127Adolescents (see also Young drivers)drowning 63, 68, 71pois<strong>on</strong>ing 130road traffic injuries 37–38, 48Africa 202burns 80, 82, 85drowning 59, 60falls 101, 102, 103pois<strong>on</strong>ing 124, 125, 129road traffic injuries 5, 31, 32statistical tables 158, 164–177, 180Ageburns and 81–82, 85<strong>child</strong> injuries and 6drowning and 61, 63, 64falls and 102–103, 106–107pois<strong>on</strong>ing and 124, 125, 129–130road traffic injuries and 32susceptibility to <strong>injury</strong> and 8–9, 145–146Agriculture 109, 114, 126–127Airbags 49Alcoholdriving and 40, 46, 47drowning risks 65–66, 68, 71interlock systems 43misuse 130The Alliance for Safe Children (TASC) surveys, seeUNICEF/The Alliance for Safe Children (TASC) Asiancommunity surveysAmbulance services 13, 48Americas 201burns 80, 85drowning 60falls 101, 102, 103pois<strong>on</strong>ing 124, 125road traffic injuries 32, 33statistical tables 164–177, 181–182Angola 82Animalsbite injuries 14–15falls from 108–109venomous 127, 128–129Antidotes 136Antivenoms 128Aspirin 132, 134Australia 11, 12, 17burns 86, 88, 89dog-bite injuries 14drowning 59, 60, 62, 63, 66, 71falls 103, 105, 106, 108, 110, 111pois<strong>on</strong>ing 125, 128, 131, 134road safety 39, 43, 44, 46road traffic injuries 35water safety 67, 69, 70Autism 65Awareness, creating and maintaining 150–151, 152–153Baby bouncers 108Baby equipment, see Nursery equipmentBaby walkers/exercisers 110, 111, 112Bangladesh 11, 12, 159–160burns 82, 83, 89drowning 60, 61, 62, 65, 66, 69falls 103pois<strong>on</strong>ing 126road traffic injuries 32, 34, 36UNICEF/TASC surveys 3, 159–160, 197Baths 66, 67, 70–71baby seats 72Beds, falls from 108Behaviour change 18Belgium 8Bhopal catastrophe 134Bicycle helmets 16, 18, 39, 44, 50Bicycles, design 41Bicyclistsinjuries 35risks of <strong>injury</strong> 38–39safety measures 42, 43, 44, 45–46, 48, 50Bitesdog 14–15venomous 127, 128–129Blister packs 134–135Boatssafety equipment 65, 68unsafe 65Booster seats 16, 39, 43–44WORLD REPORT ON CHILD INJURY PREVENTION 203
Botswana 190Brain <strong>injury</strong>, traumatic 33–34, 105Brazilburns 82drowning 61falls 107, 109n<strong>on</strong>-fatal <strong>child</strong> injuries 7road traffic injuries 45Buckets 4, 67Built envir<strong>on</strong>ment 42, 109, 110, 114Bunk beds 108Burden of <strong>child</strong> injuries 1–2, 3, 145Burns 79–94case story 78chemical 79, 83classificati<strong>on</strong> 79c<strong>on</strong>tact 79, 83, 85definiti<strong>on</strong> 79disability after 8, 83electrical 79, 83epidemiology 9, 80–84flame-related 79, 83ICD coding 157inhalati<strong>on</strong>al 79, 83interventi<strong>on</strong>s 17, 87–93limitati<strong>on</strong>s of data 84management 90–92nature and severity 83protective factors 86–87recommendati<strong>on</strong>s 93–94risk factors 84–86statistical tables 170–171timing 86Buses 35, 42, 43Cambodia 13Camel racing 109Canada 14, 17, 18burns 81, 84, 88falls 105, 108, 109, 110, 111pois<strong>on</strong>ing 134road traffic injuries 35, 40Canadian Hospitals Injury Reporting and Preventi<strong>on</strong>Program (CHIRPP) 149Carb<strong>on</strong> m<strong>on</strong>oxide pois<strong>on</strong>ing 127, 131Cardiac arrhythmias 65Caregivers, see ParentsCarsdesign 41, 43occupants 35, 38Cassia occidentalis beans 127Catering industry 82Causes of death<strong>child</strong> injuries 5, 6<strong>child</strong>hood 2, 178–189differences between datasets 161Cayman Islands 190Chemical burns 79, 83Chemicals, household 127, 131, 137Chest injuries 33, 105Child(ren)causes of death 2, 178–189definiti<strong>on</strong> 1<strong>injury</strong> preventi<strong>on</strong> role 154, 155survival 3, 145susceptibility to <strong>injury</strong> 8–9, 145–146working see Labour, <strong>child</strong>worlds 9Child abuse 105Child health programmes 2–3, 151Child injurieschanging world 3–5characteristics 5–12fatal 5–6, 159importance 1–2n<strong>on</strong>-fatal 7–8other unintenti<strong>on</strong>al 176–177preventi<strong>on</strong> see Preventi<strong>on</strong>, <strong>injury</strong>public health approach 12, 145pyramid 5Childhood, nature of 1, 8Children Can’t Fly programme 110, 112, 113Chile 107, 190China 190animal-bite injuries 15burns 82drowning 60, 61, 62, 65, 69falls 103, 104, 105, 110pois<strong>on</strong>ing 127road traffic injuries 31, 39, 41UNICEF/TASC surveys 3, 159–160, 197–198Climate change 5Closures, <strong>child</strong>-resistant 131, 133, 134–135Cognitive development 36–37Colombia 126, 161Communitiesimpact of disability 62, 83–84interventi<strong>on</strong>s 19, 113Community-based studies 18Community leaders 154C<strong>on</strong>spicuity 45–46, 48C<strong>on</strong>structi<strong>on</strong> industry 17, 110C<strong>on</strong>sumer products, see Products, c<strong>on</strong>sumerC<strong>on</strong>tainers<strong>child</strong>-resistant 17, 131labelling 134C<strong>on</strong>venti<strong>on</strong> <strong>on</strong> the Rights of the Child 1, 3, 145Cooking areas 86Cooking equipment/stoves 86, 87–88Cooking fires 17, 85, 86, 127Cost-effectiveness, interventi<strong>on</strong>s 20, 147–148204 WORLD REPORT ON CHILD INJURY PREVENTION
Costs, ec<strong>on</strong>omic 20burns 84, 91drowning 62–63fall-related <strong>injury</strong> 105–106injuries 20, 147–148pois<strong>on</strong>ing-related <strong>injury</strong> 127road traffic injuries 36safety 20trauma care 13Côte d’Ivoire 82Cuba 107Cultural change, encouraging 19Cycle helmets, see Bicycle helmets; Motorcycle helmetsCzech Republic 35, 154DALYs, see Disability-adjusted life yearsDatalimitati<strong>on</strong>s 21, 36, 63, 84, 106, 127–129need for better 148, 149, 152Day-care facilities 109, 111Daytime running lights 46, 50Deaths, see MortalityDenmark 35, 43Developed countries, see High-income countriesDeveloping countries, see Low-and middle-incomecountriesDevelopment organizati<strong>on</strong>s 153Developmental stageburns and 85drowning and 63falls and 106–107road traffic injuries and 36–37susceptibility to <strong>injury</strong> and 8–9, 145–146Diethylene glycol 126Disability 7–8, 159burns 8, 83falls 103, 104, 105n<strong>on</strong>-fatal drowning 59, 62road traffic injuries 8, 33–34services 13vulnerability to <strong>injury</strong> 85, 107Disability-adjusted life years (DALYs) 1, 158causes 178–189falls 104n<strong>on</strong>-fatal drowning 62Distracti<strong>on</strong>s, young drivers 40Djibouti 190Dog bites 14–15Dominican Republic 42D<strong>on</strong>or organizati<strong>on</strong>s 153Drink-driving 40, 43, 46, 50Drivers, young, see Young driversDrowning 3, 59–73case story 58definiti<strong>on</strong> 59ec<strong>on</strong>omic impact 62–63epidemiology 59–63globalizati<strong>on</strong> and 4ICD coding 63, 157interventi<strong>on</strong>s 19, 66–72locati<strong>on</strong> 61–62managing 71–72mortality 59–62, 167–168recommendati<strong>on</strong>s 72–73risk factors 63–66statistical tables 168–169Drug misuse 124, 130Eastern Mediterranean 202burns 80, 81, 85drowning 59, 60falls 102, 103pois<strong>on</strong>ing 124, 125road traffic injuries 31, 32, 33statistical tables 164–177, 186–187Ec<strong>on</strong>omic costs, see Costs, ec<strong>on</strong>omicEducati<strong>on</strong> (and skills) 18, 150burns preventi<strong>on</strong> 89, 93falls preventi<strong>on</strong> 111–112road safety 47–48, 50–51safety of pois<strong>on</strong>s 132, 135water safety 69–71Egypt 126, 161, 191Electrical appliances, unsafe 86Electrical burns 79, 83Emergency care 13burns 90–91drowning 66lack of 41road traffic injuries 48–49Engineering measuresburns preventi<strong>on</strong> 87–88falls preventi<strong>on</strong> 110pois<strong>on</strong>ing preventi<strong>on</strong> 132–134road safety 42–43water safety 67England, see United KingdomEnvir<strong>on</strong>mental change 5Envir<strong>on</strong>mental modificati<strong>on</strong> 17–18, 88, 108, 114–115, 134Envir<strong>on</strong>mental risk factors 9, 10burns 86drowning 66falls 109–110pois<strong>on</strong>ing 131–132road traffic injuries 41Epilepsy 65, 71, 85Ethnic minorities, drowning risk 65Europe 202burns 80, 85, 89drowning 60falls 102, 103pois<strong>on</strong>ing 124, 125, 134WORLD REPORT ON CHILD INJURY PREVENTION 205
oad traffic injuries 31, 32, 33, 43statistical tables 164–177, 184–185Falls 101–115case story 100definiti<strong>on</strong>s 101epidemiology 8–9, 101–106ICD coding 157interventi<strong>on</strong>s 110–114limitati<strong>on</strong>s of data 106recommendati<strong>on</strong>s 114–115risk factors 106–110severity 104–105statistical tables 172–173types 103Family (see also Parents)impact of injuries 62, 83–84structure 10Farming, see AgricultureFatal <strong>child</strong> injuries (see also Mortality) 5–6, 159Fate, attributi<strong>on</strong> to 21Fathers, deaths from injuries 34Fatigue, young drivers 40Fencing, water bodies 67–68Finland 35, 81Fire-retardant household materials 88Fire sprinkler systems 88Firesopen 17, 85, 86, 127safety measures 17, 18Fireworks 86, 89First aidburns 90, 93training 48, 71–72Flammable substances 86, 87Flooding 5, 60, 66Flotati<strong>on</strong> devices, pers<strong>on</strong>al 65, 68Food pois<strong>on</strong>ing 126–127Fractures 7, 33, 105, 108France 21, 35, 105Fuels (see also Paraffin)burns and 86, 87–88ingesti<strong>on</strong> 126Funding, preventi<strong>on</strong> strategies 22, 150Gambia 106Gender differencesburns 81, 82, 85<strong>child</strong> injuries 6, 9drowning 61, 63–64falls 103, 107pois<strong>on</strong>ing 124–125, 130road traffic injuries 32–33, 38Germany 35, 60Ghana 12, 42Global Burden of Disease (GBD) 157, 158Global Childhood Unintenti<strong>on</strong>al Injury Surveillance 8,160–161, 200–201Global School Health Survey (GSHS) 7, 157, 159, 190–195Globalizati<strong>on</strong> 4Glue sniffing 126Governments, acti<strong>on</strong>s needed 153Greece 44, 86, 107, 108, 130Guatemala 17, 87, 191Guyana 191Hadd<strong>on</strong> Matrix 12burns 84drowning 64falls 106pois<strong>on</strong>ing 130road traffic injuries 37Hadd<strong>on</strong>’s 10 <strong>injury</strong> preventi<strong>on</strong> strategies 12, 13Haiti 126, 127Head injuries 7, 18, 33–34, 105Health educati<strong>on</strong>, see Educati<strong>on</strong>Health systems, strengthening 151–152Heating equipment 86, 87–88Heavy metal pois<strong>on</strong>ing 127Heavy vehicles 35Heelys 108Heights, falls from 103, 104, 105High-income countries (HIC)burden of <strong>child</strong> injuries 1, 5, 6, 10burns 80, 85classificati<strong>on</strong> 157–158, 202dog-bite injuries 14drowning 60, 61, 65, 66falls 102, 103, 104, 105–106, 107<strong>injury</strong> preventi<strong>on</strong> 2, 16–17pois<strong>on</strong>ing 123, 126road traffic injuries 32socioec<strong>on</strong>omic factors 11Holiday activities 66Home envir<strong>on</strong>ment 16, 17burns and 86, 88drowning and 66, 70–71falls and 107, 109, 110pois<strong>on</strong>ing and 131, 132–133, 134Home visits, supportive 18, 112–113Horiz<strong>on</strong>tal standards 111Horse riding 108–109, 110Hospital care (see also Trauma care) 13Hot-water taps, temperature 88, 89Household chemicals 127, 131, 137Housing, poor quality 107Human resources 149–150Iceland 35India 4, 11animal-bite injuries 15burns 82, 83, 90206 WORLD REPORT ON CHILD INJURY PREVENTION
pois<strong>on</strong>ing 124, 126, 127, 134road safety 43road traffic injuries 31, 33–34, 36, 40Indigenous populati<strong>on</strong>s 12Individuals, strengthening 19Infanticide 63Informati<strong>on</strong> systems 152Injuries, defined 1The Injury Preventi<strong>on</strong> Project Safety Survey (TIPP-SS)113–114Injury Severity Score 7, 8Intenti<strong>on</strong>al injuries 1Internati<strong>on</strong>al Classificati<strong>on</strong> of Disease (ICD) 63, 129, 157Internati<strong>on</strong>al Federati<strong>on</strong> of Red Cross and Red CrescentSocieties 48Internati<strong>on</strong>al organizati<strong>on</strong>s 153Interventi<strong>on</strong>scost-effectiveness 20effective 16–18, 147, 148implementati<strong>on</strong> 22universal and targeted 18–20Intoxicati<strong>on</strong>, see Pois<strong>on</strong>ingIran, Islamic Republic of 9, 15, 82, 110Iraq 13Japan 46–47, 125Jordan 113, 190Keloids 83Kenya 41, 81, 82, 191Kerosene, see ParaffinKitchens 82, 83, 86Knowledge transfer 19–20, 150Korea, Republic of 35Kuwait 10, 81Labour, <strong>child</strong> 4, 82, 109–110, 126, 127Lamps, safer 87Latvia 46Lead pois<strong>on</strong>ing 127Leban<strong>on</strong> 192Legislati<strong>on</strong> 8, 16–17burns preventi<strong>on</strong> 88–89drowning preventi<strong>on</strong> 68falls preventi<strong>on</strong> 111road safety 46–47safety of pois<strong>on</strong>s 132, 134–135Leisure activities 16, 71, 108Libyan Arab Jamahiriya 192Licensing, driver 46, 47, 50Life jackets 65, 68Lifeguards (lifesavers) 70Lighters, <strong>child</strong>-resistant 88–89Lighting 86, 87Lights, daytime running 46, 50Low-and middle-income countries (LMIC)burden of <strong>child</strong> injuries 1, 3, 5, 6, 9, 10burns 80, 81–82, 85classificati<strong>on</strong> 157–158, 202cost-effectiveness of interventi<strong>on</strong>s 20dog-bite injuries 14–15drowning 59, 60, 61, 65, 66falls 101, 102, 103, 104, 106, 107<strong>injury</strong> preventi<strong>on</strong> 2, 18–20obstacles to <strong>injury</strong> preventi<strong>on</strong> 21–22pois<strong>on</strong>ing 123–124road traffic injuries 31, 32socioec<strong>on</strong>omic factors 11Macroec<strong>on</strong>omic change, encouraging 19Malawi 106Malaysia 40, 43, 46, 47Manchineel tree 134Media 153–154Medical services, access to, see Access to careMedicinesingesti<strong>on</strong> 126, 131, 132safety measures 133, 134–135Mental disability 107Mental health problems 34MENTOR-VIP 150Methanol 132Methyl isocyanate 134Mexico 41, 64–65, 66, 67, 82, 107Middle-income countries, see Low-and middle-incomecountriesMillennium Development Goals 3, 5, 9–10, 145Mobile ph<strong>on</strong>es 40, 47Morbidityburns 81–84drowning 62falls 103–105pois<strong>on</strong>ing 125road traffic injuries 33–34Morocco 5, 15, 192Mortalityburns 80–81, 170–171<strong>child</strong> injuries 3, 5–6, 164–165drowning 59–62, 168–169falls 101, 102–103, 172–173pois<strong>on</strong>ing 123–125, 174–175road traffic injuries 31–33, 166–167sources of data 158Mothers, deaths from injuries 34Motor vehiclesdesign 41, 43, 50licensing 46reversing aids 43Motorcycle helmets 18, 39–40, 45, 47, 50Motorcycles 35licensing 46WORLD REPORT ON CHILD INJURY PREVENTION 207
isks of <strong>injury</strong> 39–40safety measures 43, 45, 46, 50Motorizati<strong>on</strong> 4–5Motorized two-wheelers 46, 47Mozambique 87, 104Multisectoral approach 150Namibia 192Nati<strong>on</strong>al acti<strong>on</strong> plan, developing 151, 154Netherlandsdrowning 65falls 109pois<strong>on</strong>ing 137road safety 42, 43, 44, 48road traffic injuries 35New Zealand 8, 12, 19burns 88drowning 71falls 105, 108, 110pois<strong>on</strong>ing 134road traffic injuries 35, 40, 46Nicaragua 105, 126Nigeria 10, 82, 104, 105, 110, 126N<strong>on</strong>-fatal <strong>child</strong> injuries 7–8N<strong>on</strong>governmental organizati<strong>on</strong>s 83, 153Norway 35, 48, 65, 88Nursery equipment 17, 107–108, 110, 111Occupants, car 35, 38Oman 127, 193Organisati<strong>on</strong> for Ec<strong>on</strong>omic Co-operati<strong>on</strong> and Development(OECD), road safety study 16Orphans 34Packaging, <strong>child</strong>-resistant 131, 132–133, 134–135, 138Pakistan 17, 90, 91, 104, 126, 161Panama 126Papau New Guinea 128Paracetamol 126, 132Paraffin (kerosene)flammability 86, 87pois<strong>on</strong>ing 126, 130, 131, 132, 133–134Parents (and caregivers)acti<strong>on</strong>s needed 154<strong>child</strong> supervisi<strong>on</strong> see Supervisi<strong>on</strong>, <strong>child</strong>death/incapacity from injuries 5, 12, 34educati<strong>on</strong> see Educati<strong>on</strong>smoking 85Partnerships, drowning preventi<strong>on</strong> 72Pedestriansinjuries 35risk factors 36, 37, 38safety 42, 43, 45–46, 48Peer influences 38Peru 127Pesticides 126–127, 131, 132Philippines 3, 61, 159–160, 193, 199Plant toxin pois<strong>on</strong>ing 127Play areas, safe 42, 110, 113Playground equipment, falls from 105, 108Pois<strong>on</strong> c<strong>on</strong>trol centres 125, 132, 136–137, 138Pois<strong>on</strong>ing 123–138case story 122epidemiology 8, 9, 123–129ICD coding 129, 157interventi<strong>on</strong>s 17, 132–137limitati<strong>on</strong>s of data 127–129management 135–137recommendati<strong>on</strong>s 138risk factors 129–132statistical tables 174–175Pois<strong>on</strong>sreducing attractiveness 133–134removal 134safety measures 132–135storage and access 131, 132–133types 125–127, 130–131Poland 35Policy, <strong>child</strong> <strong>injury</strong> preventi<strong>on</strong> 151Political commitment 21Poor populati<strong>on</strong>sburden of <strong>child</strong> injuries 1, 145impact of road traffic injuries 36vulnerability to injuries 11–12Post-traumatic stress disorder 34, 83Poverty 9–12burns risk 85–86definiti<strong>on</strong>s 10drowning risk 64–65falls risk 107, 109injuries as cause 11–12as <strong>injury</strong> risk factor 10–11pois<strong>on</strong>ing and 126, 130road traffic <strong>injury</strong> risk 41targeting 19Pre-hospital care 13, 41, 48, 110PRECEDE-PROCEED model 18Preventi<strong>on</strong>, <strong>injury</strong> 2, 12–22, 146–147effective approaches 16–18, 147, 148funding 22, 150Hadd<strong>on</strong>’s 10 strategies 12, 13learning from others 16obstacles to 20–22principles 12public health approaches 12recommendati<strong>on</strong>s 151–153sectors resp<strong>on</strong>sible 150shortage of practiti<strong>on</strong>ers 149–150universal and targeted interventi<strong>on</strong>s 18–20Primary preventi<strong>on</strong> 12Private sector 153208 WORLD REPORT ON CHILD INJURY PREVENTION
Products, c<strong>on</strong>sumerfalls risk 107–108safety/modificati<strong>on</strong> 17, 110, 111, 137Psychosocial impactburns 83, 92drowning 72road traffic injuries 34Public health approach 12, 145Public transport vehicles 35Puerto Rico 48Pushchairs 107–108Pyramid, <strong>child</strong> <strong>injury</strong> 5Rabies 15Recommendati<strong>on</strong>s, <str<strong>on</strong>g>report</str<strong>on</strong>g> 151–153implementing 153–155Rehabilitati<strong>on</strong> services 13, 41, 49, 66, 92Research priorities 148–149, 152Restaurants 82Restraints, <strong>child</strong> car 16, 43–44, 50effectiveness 39, 43legislati<strong>on</strong> 46–47rates of use 38Resuscitati<strong>on</strong>, drowning victims 71–72, 73Risk-taking behaviour 37–38, 40, 65, 107Road envir<strong>on</strong>mentlegislati<strong>on</strong> 16modificati<strong>on</strong> 17–18, 42–43risk factors for injuries 41Road infrastructure 4–5Road safety 42–48case story 144educati<strong>on</strong> and skills 47–49effectiveness 148engineering measures 42–43equipment 43–46evaluating 49legislati<strong>on</strong> and standards 46–47potentially harmful measures 49recommendati<strong>on</strong>s 49–51vehicle design 43Youth Declarati<strong>on</strong> 155Road trafficincreased motorizati<strong>on</strong> 4–5reducing speed 17, 42, 47, 50Road traffic crash, definiti<strong>on</strong> 31Road traffic injuries 31–51case story 30definiti<strong>on</strong> 31ec<strong>on</strong>omic impact 36epidemiology 1, 2, 8, 31–36fatal, definiti<strong>on</strong> 31ICD coding 157interventi<strong>on</strong>s 42–49limitati<strong>on</strong>s of data 36nature and severity 33risk factors 9, 36–41by road user type 34–35statistical tables 166–167Road user typesdeaths 31injuries 34–35risk factors 38–40Safe Communities model, WHO 18, 19, 113, 154Safety, learning from others 16Safety devices 18, 20Saint Lucia 132, 193Saint Vincent and the Grenadines 193Saudi Arabia 127Scalds 79, 81, 82, 83preventi<strong>on</strong> 88, 89risk factors 85Scarring, hypertrophic 83School, safe routes to 42–43Scorpi<strong>on</strong> stings 127Scotland, see United KingdomSeas<strong>on</strong>al variati<strong>on</strong>s 86, 131Seat-belts 44, 50effectiveness 39mandatory use 47n<strong>on</strong>-use 38, 40Sec<strong>on</strong>dary preventi<strong>on</strong> 12Sensati<strong>on</strong>-seeking 37–38Severity of <strong>injury</strong> 7, 8, 159–160Sex differences, see Gender differencesSingapore 46Slums, urban 4Smoke alarms 18, 88Smoke inhalati<strong>on</strong> 80, 83Smoking, tobacco 85Snakebites 127, 128–129Socioec<strong>on</strong>omic factors (see also Poverty) 9–12burns 86falls 109pois<strong>on</strong>ing 130, 131–132Socioec<strong>on</strong>omic inequalities, tackling 19Solvents, organic 126South Africa 11, 15, 17, 19burns 86, 92drowning 61–62falls preventi<strong>on</strong> 113pois<strong>on</strong>ing 125, 127, 132, 133road traffic injuries 39, 48South-East Asia 202burns 80, 81, 85drowning 59, 60falls 102, 103pois<strong>on</strong>ing 124, 125road traffic injuries 31, 32statistical tables 164–177, 183Spain 35WORLD REPORT ON CHILD INJURY PREVENTION 209
Speed reducti<strong>on</strong> measures 17, 42, 47, 50Speeding 40Spider bites 127Spinal-cord injuries 105Sports injuries 108Sprinkler systems, fire 88Squatter camps 4, 5Sri Lanka 15, 87, 124, 125, 137St John’s Ambulance 48Stair gates 112Stature 36Street <strong>child</strong>ren 85Substance misuse 124, 130Supervisi<strong>on</strong>, <strong>child</strong> 10, 11burns preventi<strong>on</strong> 89drowning and 63, 65, 70–71falls and 109, 115pois<strong>on</strong>ing and 131road traffic <strong>injury</strong> risk and 40Swaziland 194Sweden 8, 16, 146burns 85–86drowning 60, 65pois<strong>on</strong>ing 125road safety 42, 43–44road traffic injuries 35, 41Swimming 67safety equipment 65, 68supervisi<strong>on</strong> 70–71teaching 69–70Swimming pools 66, 67fencing 67, 68flexible solar covers 72Switzerland 35Systems approach, road safety 42, 49Tajikistan 194Tanzania, United Republic of 15, 194TASC surveys, see UNICEF/The Alliance for Safe Children(TASC) Asian community surveysTEACH-VIP 150Teachers 154Tertiary preventi<strong>on</strong> 12, 13Thailand 3burns 84dog bites 15drowning 60, 61, 62falls 105road traffic injuries 32, 41, 43UNICEF/TASC surveys 159–160, 198Toxins, see Pois<strong>on</strong>sToys 17Traditi<strong>on</strong>al healers 129Training 21, 150, 152Transport systems, improved 4–5Trauma care 10, 13, 41, 49burns 91–92Traumatic brain <strong>injury</strong> 33–34, 105Treatment, lack of prompt 41Trees, falls from 104Trinidad and Tobago 194Tunisia 15Turkey 35, 106, 126Two-wheelers, separati<strong>on</strong> 43, 50Uganda 15, 64, 65, 104, 194UNICEF/The Alliance for Safe Children (TASC) Asiancommunity surveys 5, 145, 159–160, 196–199dog-bite injuries 14–15drowning 60, 61falls 103, 105fatal <strong>child</strong> injuries 3, 6n<strong>on</strong>-fatal <strong>child</strong> injuries 7Unintenti<strong>on</strong>al injuries 1all unintenti<strong>on</strong>al 164–165other unintenti<strong>on</strong>al 176–177United Arab Emirates 101United Kingdom 11, 19burns 84, 85, 89drowning 60, 62, 66falls 105pois<strong>on</strong>ing 126, 130, 132, 133road safety 43, 44, 48road traffic injuries 35, 41United Nati<strong>on</strong>s<strong>child</strong> health initiatives 3C<strong>on</strong>venti<strong>on</strong> <strong>on</strong> the Rights of the Child 1, 3, 145United States of America 5, 12burns 81, 86, 88–89, 90cost-effectiveness of interventi<strong>on</strong>s 20, 147–148costs of <strong>child</strong> injuries 20dog-bite injuries 14drowning 59, 61, 62, 63, 65, 67, 69falls 103, 105, 109, 110, 111–112<strong>injury</strong> preventi<strong>on</strong> 17, 19, 22pois<strong>on</strong>ing 125, 126, 127, 128, 133, 134, 135road safety measures 39, 43, 44, 46, 47road traffic injuries 35, 36, 40Urbanizati<strong>on</strong> 4Uruguay 195Vehicle design 41, 43, 50Venezuela 107Vertical standards 17, 111Viet Nam 11–12animal-bite injuries 15burns 90drowning 61, 62falls 103, 105road traffic injuries 39, 45UNICEF/TASC surveys 3, 159–160, 199210 WORLD REPORT ON CHILD INJURY PREVENTION
Vinegar 132Visibility, improving 45–46, 48Walking buses 42Water (see also Drowning; Scalds)to douse fires 86piped systems 67temperature of hot 88, 89Water bodiesbarriers around 67–68types 61–62, 66Water safety 66–71, 72equipment 65, 68legislati<strong>on</strong> and standards 67recommendati<strong>on</strong>s 72–73Weather c<strong>on</strong>diti<strong>on</strong>s, extreme 5, 66Wells, covering 67–68Western Pacific 202burns 80, 85drowning 59, 60, 62falls 102, 103pois<strong>on</strong>ing 124, 125road traffic injuries 31, 32statistical tables 164–177, 188–189Wheelchair users 107Window guards 110, 111, 112Windows, falls from 105, 112Work-related injuries 4, 82, 109–110, 126, 127<str<strong>on</strong>g>World</str<strong>on</strong>g> Fit for Children, A 3<str<strong>on</strong>g>World</str<strong>on</strong>g> Health Assembly 3<str<strong>on</strong>g>World</str<strong>on</strong>g> Health Organizati<strong>on</strong> (WHO)data 157–158regi<strong>on</strong>s and countries 157–158, 202Wrist fractures 108Wrist guards 108, 110Young driverscrashes and injuries 35, 36educati<strong>on</strong> 48licensing 46, 47, 50risk factors for crashes 37, 38, 40Youth Declarati<strong>on</strong> for Road Safety 155Zambia 195Zimbabwe 195WORLD REPORT ON CHILD INJURY PREVENTION 211
Keeping <strong>child</strong>ren safe is a universal priority. Yet each year milli<strong>on</strong>s of <strong>child</strong>ren areaffected by unintenti<strong>on</strong>al injuries, which can result in disability, hospitalizati<strong>on</strong>, andeven death. CDC's Injury Center is committed to raising awareness about what researchshows – that there are steps governments, organizati<strong>on</strong>s, communities, and individualscan take to reduce the enormous burden of <strong>child</strong>hood <strong>injury</strong>. By keeping our <strong>child</strong>rensafe and secure, we can help them live to their fullest potential.— Ileana Arias, Director, Nati<strong>on</strong>al Center for Injury Preventi<strong>on</strong> and C<strong>on</strong>trol, US Centers forDisease C<strong>on</strong>trol and Preventi<strong>on</strong>We have l<strong>on</strong>g known that <strong>injury</strong> is not well counted outside high-income countrieswith their well-developed death registrati<strong>on</strong> and certificati<strong>on</strong> systems. This <str<strong>on</strong>g>report</str<strong>on</strong>g>makes it clear that we need to count these events better, as they are the leading causeof <strong>child</strong> death after infancy and equally important, we need to work to prevent themwith the same intensity and commitment as other causes of <strong>child</strong> death and disability.— “Pete” Petersen, Co-Founder, The Alliance for Safe ChildrenThe <str<strong>on</strong>g>World</str<strong>on</strong>g> Report <strong>on</strong> Child Injury Preventi<strong>on</strong> highlights the urgent need to addressgaps in our knowledge base to understand, c<strong>on</strong>trol, and prevent <strong>child</strong> and adolescentinjuries. Research that examines ways to decrease exposure, mitigate risks, andpromote safer interventi<strong>on</strong>s is needed worldwide, and especially in low- and middleincomecountries. Paediatric <strong>injury</strong> research is a global imperative and we hope thatthis <str<strong>on</strong>g>report</str<strong>on</strong>g> will inspire a new era of support, capacity development and utilizati<strong>on</strong> ofresearch findings.— Adnan Hyder, President, Internati<strong>on</strong>al Society for Child and Adolescent Injury Preventi<strong>on</strong>The European Child Safety Alliance fully supports the recommendati<strong>on</strong>s of the <str<strong>on</strong>g>World</str<strong>on</strong>g>Report <strong>on</strong> Child Injury Preventi<strong>on</strong>, as Europe is a regi<strong>on</strong> that has some of the world'shighest and lowest <strong>child</strong> <strong>injury</strong> rates. This <str<strong>on</strong>g>report</str<strong>on</strong>g> reflects the goals that the Alliance, as agrowing network of 32 countries, is striving to achieve through joint work to advocatefor the adopti<strong>on</strong>, implementati<strong>on</strong> and evaluati<strong>on</strong> of proven good practices in <strong>child</strong><strong>injury</strong> preventi<strong>on</strong> in the European setting. It is hoped that the work in Europe will alsosupport efforts in other parts of the world.— Joanne Vincenten, Director, European Child Safety AllianceChildhood <strong>injury</strong> is <strong>on</strong>e of the greatest challenges in present and future global healthcare, particularly in Africa; this timely publicati<strong>on</strong> of the <str<strong>on</strong>g>World</str<strong>on</strong>g> Report <strong>on</strong> Child InjuryPreventi<strong>on</strong> makes a significant c<strong>on</strong>tributi<strong>on</strong> to promoting <strong>child</strong> safety and mitigating<strong>child</strong> trauma.— Sebastian van As, President, Childsafe South AfricaThe WHO <str<strong>on</strong>g>World</str<strong>on</strong>g> Report <strong>on</strong> Child Injury Preventi<strong>on</strong> provides a call to acti<strong>on</strong> to prevent<strong>injury</strong> to <strong>child</strong>ren worldwide. The soluti<strong>on</strong>s are low cost and require simple technology.We must act now to eliminate death to <strong>child</strong>ren from preventable <strong>injury</strong> in all nati<strong>on</strong>s.Safe Kids <str<strong>on</strong>g>World</str<strong>on</strong>g>wide is committed to this global initiative to save the lives of <strong>child</strong>ren.— Martin Eichelberger, Founder and Director, Safe Kids <str<strong>on</strong>g>World</str<strong>on</strong>g>wide
I MPLEMENTING PROVEN CHILD INJURYpreventi<strong>on</strong> interventi<strong>on</strong>s could save morethan a thousand <strong>child</strong>ren’s lives a day.— Dr Margaret Chan,Director-General, WHOand Mrs Ann Veneman,Executive Director, UNICEFISBN 978 92 4 156357 4