358 Y. H. Chen et al./JCOS 25(2009) 357-364INTRODUCTIONNumerous studies have found an increased rate ofcentral nervous system (CNS) metastases in patientsreceiving trastuzumab-based regimens <strong>for</strong> HER2-positivestage IV breast cancer as compared with patientswith negative finding (25-34 vs. 6-16%) [1-9]. Leptomeningealcarcinomatosis is a rare complication(3.5%) of terminal breast cancer, but often has poorprognosis [9-11]. Blood–brain barrier (BBB) restrictsCNS penetration to molecules with molecular weightsexceeding 200 Da, so trastuzumab may not reachsufficient levels in the cerebrospinal fluid (CSF)[12,13]. <strong>Trastuzumab</strong> level in CSF was found consistentlyto be 300-fold to 400-fold lower as comparedwith the corresponding serum level [12,13]. There<strong>for</strong>e,it is unlikely that intravenous (iv) trastuzumab wouldbe useful to treat meningeal carcinomatosis. But apatient with meningeal carcinomatosis of breast cancerresponded to intravenous trastuzumab, althoughtthe response was transient and limited to radiologicalfindings [14]. Permeability of the BBB <strong>for</strong> larger moleculesincluding trastuzumab increases after wholebrainradiotherapy (WBRT) or in patients with animpairment of the BBB owing to leptomeningeal carcinomatosis[13,15]. To our knowledge, just six casereports of treatment of meningeal carcinomatosis byintrathecal trastuzumab with total dose 20~40 mg perweek have been reported till now [16-21]. But data onthe activity and safety of higher dose intrathecal trastuzumabare limited. Only Mir et al. reported on abreast cancer patient suffering from meningeal carcinomatosiswho received trastuzumab 100 mg weekly<strong>for</strong> four cycles [20]. In this case report, fifteen cyclesof high- dose trastuzumab (80~100 mg weekly) were*Corresponding author: Wei-Shiou Hwang M.D.* 通 訊 作 者 : 黃 偉 修 醫 師Tel: +886-6-2812811 ext.57111Fax: +886-6-2828928E-mail: cmh7300@mail.chimei.org.twgiven <strong>for</strong> meningeal carcinomatosis without obviousside effect.CASE REPORTThis 57-year-old woman was treated in 2006 <strong>for</strong>left breast cancer, invasive ductal carcinoma, ER(-)PR(-) Her-2(3+) T4NxM1 with liver and lung metastasis.She received chemotherapy with vinorelbine and5-fluorouracil (June 2006 to July 2006), weekly paclitaxeland trastuzumab (July 2006 to April 2007), andweekly epirubicin and cyclophosphamide (May 2007to November 2007). Capecitabine 1500 mg bid andlapatinib 1250 mg were given daily since December2007 <strong>for</strong> a new lesion over the left upper lung andmultiple brain metastases. However, brain magneticresonance imaging (MRI) in December 2008 revealedincreased in size and numbers of brain lesions andWBRT, 3300 cGy/ 11Fractions was given in January2009. Lapatinib was discontinued and oral vinorelbine80 mg bi-weekly were beginning in February 2009.The patient suffered from general soreness in April2009, and poor appetite, headache, progressive fourlimbweakness, dysphagia and lethargy were noted.The leptominges of the spinal cord and fila were seenon spinal MRI, so leptomeningeal seeding was diagnosed(Figure 1). CSF examination showed an increasedcell count with an elevated level of protein(932 mg/dl), and positive tumor cytology on 13 April2009. After placement of an Ommaya reservoir, thepatient was started on intrathecal methotrexate (MTX)12 mg on 17, 21, and 24 April 2009. However, neutropeniaoccurred and neurological symptoms improvedonly mildly, with persistence of malignantcells of CSF. <strong>Intrathecal</strong> trastuzumab 20 mg biw to tiwwas given (first dose on 08 May 2009), and neurologicalsymptoms improved gradually, especiallydysphagia, lethargy and increased intracranial pressure(IICP)-related headache. But paraplegia did not significantlyimprove. As demonstrated in Table 1, thecytology of CSF became negative, and the frequencyof trastuzumab was tapered to 20 mg weekly due to
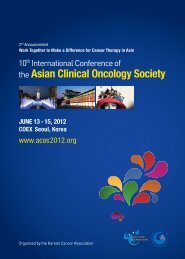
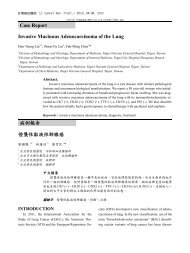
Y. H. Chen et al./JCOS 25(2009) 357-364 359A. B.Figure 1. T1W with contrast enhancement of lumbar spine MRI. (A) sagital view and (B) axial view revealedincreased meningeal contrast enhancement of the spinal cord and meningeal nodularthickening (arrows) led to the diagnosis of meningeal carcinomatosisclinical improvement on 25 May. However, neurologicalsymptoms worsened in July, even under regularCSF aspiration and intrathecal trastuzumab 20 mgweekly. <strong>Intrathecal</strong> trastuzumab 80~100 mg weeklyfrom 27 July was given, and neurological symptomsimproved without obvious headache or allergy. Oralcyclophosphamide 50 mg daily and palliative radiotherapywere given <strong>for</strong> new right chest wall lesions.Persistence of negative results of CSF cytology wasnoted, and a final lumbar puncture confirmed remissionof meningeal carcinomatosis with the absence oftumor cells in CSF on 07 November 2009. Un<strong>for</strong>tunately,general condition of the patient deterioratedwith pneumonia, Ommaya wound infection and multipleorgan failure, and she passed away on 09 November2009.DISCUSSIONNumerous previous studies have reported an unexpectedlyhigh incidence of clinically overt CNSmetastasis, ranging from 25 to 34% of patients havingreceived trastuzumab-based regimens <strong>for</strong> HER2-overexpressingstage IV breast cancer [1-9]. In contrast tothe relatively frequent parenchymal CNS metastases,leptomeningeal carcinomatosis represents a rare [9-11]but often disastrous manifestation of stage IV breastcancer [22,23]. Intact BBB is crossed only by smalllipid-soluble molecules, so chemotherapy reagentssuch as anthracyclines, vinca alkaloids, or the taxanesare poorly taken up into the brain [24]. Chemotherapyreagents, including methotrexate, thiotepa, and standardor liposome-bound cytosine arabinoside are administeredintrathecally [10,25]. <strong>Trastuzumab</strong> may notreach sufficient level in the cerebrospinal fluid (CSF)due to its molecular weight exceeding 200 Da [12,13],and the post-treatment concentration was 300-fold to400-fold lower in CSF than in serum [12,13,17]. Permeabilityof the BBB <strong>for</strong> trastuzumab increases afterWBRT or impairment of the BBB owing to leptomeningealcarcinomatosis [13,15]. Intravenous trastuzumabtherapy was active in meningeal carcinomatosisof breast cancer, althought the response was