Analysisis also part of the collaboration, so theUK cells might also ultimately be used inUS trials.ES cells come with some ethicalbaggage, so there is also interest in usingadult stem cells, such as mesenchymalstem cells. Although easier to obtainand available as a treatment in somecountries, they have shown few effectsin animal studies and Professor Barkeris sceptical of their value: “While they’reoffered around the globe for treatmentof Parkinson’s disease, the evidence thatthey will do anything substantial to yourdisease is pretty minimal.”iPS cells: a new routeto therapy?Another option might be ‘inducedpluripotent stem (iPS) cells’ – adultcells reprogrammed into a pluripotentprecursor state, which can then be used togenerate replacement neural cells. “Thatmay become a possibility,” acknowledgesProfessor Barker, but he highlights anobvious drawback. “The idea that you usethe patient’s own cells, while intuitivelyattractive, has problems, as the patienthas the disease. So if you make dopaminecells from the patient’s skin, what’s tostop them going the same way as thepatient’s own nigral dopamine cells?”Perhaps more significantly, iPS cellsare offering exciting new opportunitiesto study mechanisms of disease. Backin Edinburgh, Dr Kunath’s group hasmade an important step forward bygenerating iPS cells from a family in Iowawith a rare inherited form of Parkinson’sdisease, caused by triplication of theα-synuclein gene. As a result, affectedfamily members develop a severe earlyonsetform of Parkinson’s disease: “Allthe pathology is very similar to sporadicParkinson’s,” says Dr Kunath, “it’s justsped up.”The severity of the condition increasedthe likelihood that a phenotype wouldbe apparent in cultured cells, while theinvolvement of α-synuclein maintained thelink to the common form of the disease:“Everyone with sporadic Parkinson’s has aproblem with this protein.”Work on these cells has shown thatthey do indeed contain much moreα-synuclein in striatal cells. Since thefamily’s mutation actually spans multiplegenes, Dr Kunath has also developedES cells with an engineered α-synucleintriplication for use as an additionalexperimental system.Labelling in fibroblasts for DNA (left panel) and two fibroblast proteins (centre panels), merged in final panel.As well as providing a valuable toolfor investigating pathological changesin manageable timescales, the systemcan also be used to screen for drugs thatmight interfere with disease processes.Reactive oxygen species have beenimplicated in Parkinson’s pathology, andalthough trials with antioxidants suchas coenzyme Q have been disappointing,Dr Kunath believes that new agentsmay show more success: “We havea very interesting, potent compoundthat targets the mitochondria. Whenwe compare it with every commercialantioxidant that we can find, this novelone is much much better.” He is nowcollaborating with Manfred Auer inEdinburgh’s Chemistry Department todevelop a high-throughput screeningplatform to test a library of compoundscustom-designed by Professor Auer.Beyond Parkinson’sParkinson’s disease has been in thevanguard of cell-based therapies, butwhat about other neurodegenerativeconditions? Huntington’s disease hasfollowed a similar path to Parkinson’s butis, suggests Professor Barker, “severalsteps behind”. Similarly positive animalstudies led to open label clinical trials inFrance, the USA and the UK (carried outby Professor Anne Rosser and ProfessorSteve Dunnett, both of whom movedto Cardiff in 2000, Professor Barker anda team in London). Although one of hispatients has done “fabulously well”,overall the clinical results have beendecidedly mixed.French researchers were sufficientlyencouraged to begin a 60-patient trial, butgenerally prospects may be less bright:“The emerging picture is that the striatalpathology of Huntington’s disease is partof a much greater distributed network ofpathology. Simply trying to repair one partof it isn’t really going to work.”A similar picture may hold true ofthe most common neurodegenerativecondition, Alzheimer’s disease. “Thetrouble with AD is it’s hard to know whatyou want to target,” points outProfessor Barker.One option might be cholinergicneurons, the target of existing drugtherapies, but such cells are innervatingcortical areas that are themselvesatrophying. “That’s finger in the dyke stuff,”says Rick Livesey at the Gurdon Institutein Cambridge. “You’re losing so much realestate over so much of your brain.”Again, however, iPS cells aregenerating valuable information aboutdisease processes. Dr Livesey hasdeveloped highly efficient methodsto generate cortical neurons from iPScells. Notably, the recipe generates celltypes from all cortical layers, as well asastrocytes, and they organise themselvesinto rudimentary networks. “We replaycortical development in a dish,” says DrLivesey. “That gives us another level ofinsight into how networks form, how theyfunction, and how they go wrong.”His lab generates iPS cells frompatients with various forms of dementia,including Alzheimer’s disease butalso less common conditions such asfrontotemporal dementia. Inheritedforms of disease are again important.Notably, Professor Livesey’s group hasgenerated iPS cells from Down syndromepatients. Their cells carry an additionalcopy of chromosome 21, which carriesthe gene for amyloid precursor protein,the source of β-amyloid. Cortical neuronsgenerated from these cells show markedAlzheimer’s-like features, includingsubstantial β-amyloid accumulation: “It’snot subtle, it’s not like 10 per cent – it’sfivefold more, tenfold more.”Selina Wray20 BNA Bulletin Spring 2013www.bna.org.uk
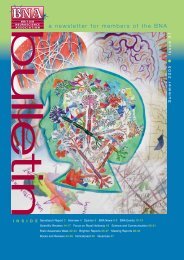
AnalysisThis contrasts markedly with animalmodels of Alzheimer’s disease. Mice areoddly refractory to Alzheimer’s – theclosest models rely on expression ofmutant forms of three proteins implicatedin the condition. “You have to push themreally hard,” says Dr Livesey. “Someonedescribed the mouse model as having anamyloid hand grenade going off in thebrain.” Even then the animals do not showthe full range of pathological featurestypical of the human disease.As well as looking at diseasemechanisms, Dr Livesey’s lab is alsogathering information about drugaction. As part of the EU InnovativeMedicines Initiative, a large public–privatepartnership, his lab is testing models ofAlzheimer’s disease with industry partners.With MRC funding, his lab is alsoexamining the impact of drugs withknown mechanisms of action. “Theidea being, can we identify new ways tochange the biology of disease using drugsthat hit known targets.” And as well assmall-chemical agents, he also hopes tolook at biological interventions, such asmonoclonal antibodies. An emerging ideais that one of the proteins implicatedin Alzheimer’s, tau, may play a rolein transferring disease between cells.Potentially, antibodies against tau mightprevent this intercellular transmissionof disease.Coping with Alzheimer’s disease.Selina Wray, who works on iPS cellsin John Hardy’s lab at UCL, agrees thatstem cell therapy for Alzheimer’s diseaseis a long shot. Some speculative animalmodel studies have obtained positiveresults, but probably because transplantedcells developed into astrocytes, whichprovided support for the degeneratingcortical neurons. “Those studies are stillpromising as it suggests that you couldlook for whatever factors the astrocyteswww.bna.org.ukUrsula Markus/SPLwere producing that are beneficial anduse those as therapy, but a neuronalreplacement therapy would be really toughfor Alzheimer’s.”Dr Wray has begun to work with DrKunath and Professor Livesey to studyan enigmatic gene, C9ORF72, mutationsin which have been implicated in bothfrontotemporal dementia and amyotrophiclateral sclerosis (a form of motor neurondisease). By generating iPS cells and thenturning them into either cortical cells ormotor neurons, she hopes to gain betterunderstanding of disease processes in thetwo situations.With Professor Hardy, she is also leadingan international initiative to accelerateresearch on iPS cells from patients withinherited forms of disease. Access tosuitable material is often an issue, soProfessor Hardy and other labs havedeveloped fibroblast patient cell lines whichare made available through the NationalInstitute for Neurological Disorders andStroke cell line repository held by the CoriellInstitute for Medical Research.ProspectsMuch as everyone might hope for amiracle cure, cell-based therapies forneurodegenerative conditions may yet besome way off. And even in the promisingcase, Parkinson’s disease, demonstrationsof efficacy may not be the final word,says Professor Barker: “If I’m honest thebig challenge for the field is not whetherit works, because I think it probably willwork, based on the fetal tissue. Thequestion is whether it works better andis competitive against conventionaldopamine therapies.”Potentially, cell therapy could formpart of a suite of treatment options, forselected patients early in disease. In thelonger term, though, it may be as tools tounderstand disease processes and screendrugs that stem cells have their biggestimpact on neurodegenerative disease.Devine MJ et al. Parkinson’s disease induced pluripotentstem cells with triplication of the α-synuclein locus. NatureCommun. 2011;2:440.Shi Y et al. A human stem cell model of early Alzheimer’sdisease pathology in Down syndrome. Sci Transl Med.2012;4(124):124ra29.Wray S et al. Creation of an open-access, mutation-definedfibroblast resource for neurological disease research. PLoSOne. 2012;7(8):e43099.Festival of <strong>Neuroscience</strong>Plenary lecture: Stem cell therapy forParkinson’s disease: Problems and prospects(Anders Björklund)Monday 8 April 2013 p.m. Human inducedpluripotent stem cells for nervous system diseasemodelling and development of new therapeutics(with Rick Livesey and Tilo Kunath)Tuesday 9 April 2013 p.m. Stem cells astherapies for the neurosciences and tools forpharmacology and toxicologyHuman ES cells differentiated into neural precursors(green) and neurons (red).Tilo KunathSpring 2013 BNA Bulletin 21