Assessing and Managing Delirium in Older Adults with Dementia
Assessing and Managing Delirium in Older Adults with Dementia
Assessing and Managing Delirium in Older Adults with Dementia
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
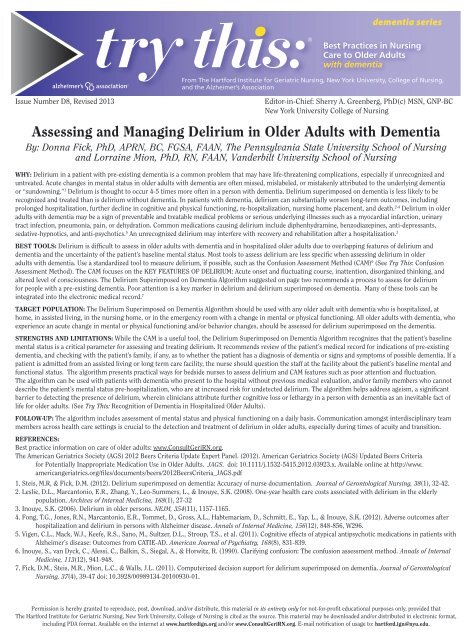
dementia seriesIssue Number D8, Revised 2013Best Practices <strong>in</strong> Nurs<strong>in</strong>gCare to <strong>Older</strong> <strong>Adults</strong><strong>with</strong> dementiaFrom The Hartford Institute for Geriatric Nurs<strong>in</strong>g, New York University, College of Nurs<strong>in</strong>g,<strong>and</strong> the Alzheimer’s AssociationEditor-<strong>in</strong>-Chief: Sherry A. Greenberg, PhD(c) MSN, GNP-BCNew York University College of Nurs<strong>in</strong>g<strong>Assess<strong>in</strong>g</strong> <strong>and</strong> <strong>Manag<strong>in</strong>g</strong> <strong>Delirium</strong> <strong>in</strong> <strong>Older</strong> <strong>Adults</strong> <strong>with</strong> <strong>Dementia</strong>By: Donna Fick, PhD, APRN, BC, FGSA, FAAN, The Pennsylvania State University School of Nurs<strong>in</strong>g<strong>and</strong> Lorra<strong>in</strong>e Mion, PhD, RN, FAAN, V<strong>and</strong>erbilt University School of Nurs<strong>in</strong>gWHY: <strong>Delirium</strong> <strong>in</strong> a patient <strong>with</strong> pre-exist<strong>in</strong>g dementia is a common problem that may have life-threaten<strong>in</strong>g complications, especially if unrecognized <strong>and</strong>untreated. Acute changes <strong>in</strong> mental status <strong>in</strong> older adults <strong>with</strong> dementia are often missed, mislabeled, or mistakenly attributed to the underly<strong>in</strong>g dementiaor “sundown<strong>in</strong>g.” 1 <strong>Delirium</strong> is thought to occur 4-5 times more often <strong>in</strong> a person <strong>with</strong> dementia. <strong>Delirium</strong> superimposed on dementia is less likely to berecognized <strong>and</strong> treated than is delirium <strong>with</strong>out dementia. In patients <strong>with</strong> dementia, delirium can substantially worsen long-term outcomes, <strong>in</strong>clud<strong>in</strong>gprolonged hospitalization, further decl<strong>in</strong>e <strong>in</strong> cognitive <strong>and</strong> physical function<strong>in</strong>g, re-hospitalization, nurs<strong>in</strong>g home placement, <strong>and</strong> death. 2-4 <strong>Delirium</strong> <strong>in</strong> olderadults <strong>with</strong> dementia may be a sign of preventable <strong>and</strong> treatable medical problems or serious underly<strong>in</strong>g illnesses such as a myocardial <strong>in</strong>farction, ur<strong>in</strong>arytract <strong>in</strong>fection, pneumonia, pa<strong>in</strong>, or dehydration. Common medications caus<strong>in</strong>g delirium <strong>in</strong>clude diphenhydram<strong>in</strong>e, benzodiazep<strong>in</strong>es, anti-depressants,sedative-hypnotics, <strong>and</strong> anti-psychotics. 5 An unrecognized delirium may <strong>in</strong>terfere <strong>with</strong> recovery <strong>and</strong> rehabilitation after a hospitalization. 3BEST TOOLS: <strong>Delirium</strong> is difficult to assess <strong>in</strong> older adults <strong>with</strong> dementia <strong>and</strong> <strong>in</strong> hospitalized older adults due to overlapp<strong>in</strong>g features of delirium <strong>and</strong>dementia <strong>and</strong> the uncerta<strong>in</strong>ty of the patient’s basel<strong>in</strong>e mental status. Most tools to assess delirium are less specific when assess<strong>in</strong>g delirium <strong>in</strong> olderadults <strong>with</strong> dementia. Use a st<strong>and</strong>ardized tool to measure delirium, if possible, such as the Confusion Assessment Method (CAM) 6 (See Try This: ConfusionAssessment Method). The CAM focuses on the KEY FEATURES OF DELIRIUM: Acute onset <strong>and</strong> fluctuat<strong>in</strong>g course, <strong>in</strong>attention, disorganized th<strong>in</strong>k<strong>in</strong>g, <strong>and</strong>altered level of consciousness. The <strong>Delirium</strong> Superimposed on <strong>Dementia</strong> Algorithm suggested on page two recommends a process to assess for deliriumfor people <strong>with</strong> a pre-exist<strong>in</strong>g dementia. Poor attention is a key marker <strong>in</strong> delirium <strong>and</strong> delirium superimposed on dementia. Many of these tools can be<strong>in</strong>tegrated <strong>in</strong>to the electronic medical record. 7TARGET POPULATION: The <strong>Delirium</strong> Superimposed on <strong>Dementia</strong> Algorithm should be used <strong>with</strong> any older adult <strong>with</strong> dementia who is hospitalized, athome, <strong>in</strong> assisted liv<strong>in</strong>g, <strong>in</strong> the nurs<strong>in</strong>g home, or <strong>in</strong> the emergency room <strong>with</strong> a change <strong>in</strong> mental or physical function<strong>in</strong>g. All older adults <strong>with</strong> dementia, whoexperience an acute change <strong>in</strong> mental or physical function<strong>in</strong>g <strong>and</strong>/or behavior changes, should be assessed for delirium superimposed on the dementia.STRENGTHS AND LIMITATIONS: While the CAM is a useful tool, the <strong>Delirium</strong> Superimposed on <strong>Dementia</strong> Algorithm recognizes that the patient’s basel<strong>in</strong>emental status is a critical parameter for assess<strong>in</strong>g <strong>and</strong> treat<strong>in</strong>g delirium. It recommends review of the patient’s medical record for <strong>in</strong>dications of pre-exist<strong>in</strong>gdementia, <strong>and</strong> check<strong>in</strong>g <strong>with</strong> the patient’s family, if any, as to whether the patient has a diagnosis of dementia or signs <strong>and</strong> symptoms of possible dementia. If apatient is admitted from an assisted liv<strong>in</strong>g or long term care facility, the nurse should question the staff at the facility about the patient’s basel<strong>in</strong>e mental <strong>and</strong>functional status. The algorithm presents practical ways for bedside nurses to assess delirium <strong>and</strong> CAM features such as poor attention <strong>and</strong> fluctuation.The algorithm can be used <strong>with</strong> patients <strong>with</strong> dementia who present to the hospital <strong>with</strong>out previous medical evaluation, <strong>and</strong>/or family members who cannotdescribe the patient’s mental status pre-hospitalization, who are at <strong>in</strong>creased risk for undetected delirium. The algorithm helps address ageism, a significantbarrier to detect<strong>in</strong>g the presence of delirium, where<strong>in</strong> cl<strong>in</strong>icians attribute further cognitive loss or lethargy <strong>in</strong> a person <strong>with</strong> dementia as an <strong>in</strong>evitable fact oflife for older adults. (See Try This: Recognition of <strong>Dementia</strong> <strong>in</strong> Hospitalized <strong>Older</strong> <strong>Adults</strong>).FOLLOW-UP: The algorithm <strong>in</strong>cludes assessment of mental status <strong>and</strong> physical function<strong>in</strong>g on a daily basis. Communication amongst <strong>in</strong>terdiscipl<strong>in</strong>ary teammembers across health care sett<strong>in</strong>gs is crucial to the detection <strong>and</strong> treatment of delirium <strong>in</strong> older adults, especially dur<strong>in</strong>g times of acuity <strong>and</strong> transition.REFERENCES:Best practice <strong>in</strong>formation on care of older adults: www.ConsultGeriRN.org.The American Geriatrics Society (AGS) 2012 Beers Criteria Update Expert Panel. (2012). American Geriatrics Society (AGS) Updated Beers Criteriafor Potentially Inappropriate Medication Use <strong>in</strong> <strong>Older</strong> <strong>Adults</strong>. JAGS. doi: 10.1111/j.1532-5415.2012.03923.x. Available onl<strong>in</strong>e at http://www.americangeriatrics.org/files/documents/beers/2012BeersCriteria_JAGS.pdf1. Steis, M.R, & Fick, D.M. (2012). <strong>Delirium</strong> superimposed on dementia: Accuracy of nurse documentation. Journal of Gerontological Nurs<strong>in</strong>g, 38(1), 32-42.2. Leslie, D.L., Marcantonio, E.R., Zhang, Y., Leo-Summers, L., & Inouye, S.K. (2008). One-year health care costs associated <strong>with</strong> delirium <strong>in</strong> the elderlypopulation. Archives of Internal Medic<strong>in</strong>e, 168(1), 27-323. Inouye, S.K. (2006). <strong>Delirium</strong> <strong>in</strong> older persons. NEJM, 354(11), 1157-1165.4. Fong, T.G., Jones, R.N., Marcantonio, E.R., Tommet, D., Gross, A.L., Habtemariam, D., Schmitt, E., Yap, L., & Inouye, S.K. (2012). Adverse outcomes afterhospitalization <strong>and</strong> delirium <strong>in</strong> persons <strong>with</strong> Alzheimer disease. Annals of Internal Medic<strong>in</strong>e, 156(12), 848-856, W296.5. Vigen, C.L., Mack, W.J., Keefe, R.S., Sano, M., Sultzer, D.L., Stroup, T.S., et al. (2011). Cognitive effects of atypical antipsychotic medications <strong>in</strong> patients <strong>with</strong>Alzheimer’s disease: Outcomes from CATIE-AD. American Journal of Psychiatry, 168(8), 831-839.6. Inouye, S., van Dyck, C., Alessi, C., Balk<strong>in</strong>, S., Siegal, A., & Horwitz, R. (1990). Clarify<strong>in</strong>g confusion: The confusion assessment method. Annals of InternalMedic<strong>in</strong>e, 113(12), 941-948.7. Fick, D.M., Steis, M.R., Mion, L.C., & Walls, J.L. (2011). Computerized decision support for delirium superimposed on dementia. Journal of GerontologicalNurs<strong>in</strong>g, 37(4), 39-47 doi: 10.3928/00989134-20100930-01.Permission is hereby granted to reproduce, post, download, <strong>and</strong>/or distribute, this material <strong>in</strong> its entirety only for not-for-profit educational purposes only, provided thatThe Hartford Institute for Geriatric Nurs<strong>in</strong>g, New York University, College of Nurs<strong>in</strong>g is cited as the source. This material may be downloaded <strong>and</strong>/or distributed <strong>in</strong> electronic format,<strong>in</strong>clud<strong>in</strong>g PDA format. Available on the <strong>in</strong>ternet at www.hartfordign.org <strong>and</strong>/or www.ConsultGeriRN.org. E-mail notification of usage to: hartford.ign@nyu.edu.
<strong>Delirium</strong> Superimposed on <strong>Dementia</strong> AlgorithmAssess for pre-hospital cognitive function:Review the patient’s medical record for <strong>in</strong>dications of pre-exist<strong>in</strong>g dementia <strong>and</strong>/or functional difficulties.Ask the patient’s family, if any, whether the patient has a diagnosis of dementia or signs <strong>and</strong> symptoms ofpossible dementia. Ask about mental status <strong>in</strong> past 6 months to one year.If a patient is admitted from an assisted liv<strong>in</strong>g or long term care facility, question the staff about the patient’sbasel<strong>in</strong>e mental <strong>and</strong> functional status.Complete a tool, such as the Family Questionnaire, to help assess pre-hospital cognitive <strong>and</strong> functionalabilities (See Try This: Recognition of <strong>Dementia</strong> <strong>in</strong> Hospitalized <strong>Older</strong> <strong>Adults</strong>).Assess for <strong>and</strong> identify delirium promptly:Use an <strong>in</strong>strument, such as the Confusion Assessment Method (CAM), to identify delirium quickly <strong>and</strong> at thebedside (Inouye, 1990).Acute onset (acute mean<strong>in</strong>g m<strong>in</strong>utes, hours, shifts, days--up to 2 weeks) or any change <strong>in</strong> cognition (<strong>in</strong>attention,memory loss, disorientation, halluc<strong>in</strong>ations, delusions) or any change <strong>in</strong> function.Acute change <strong>in</strong> behaviors such as verbal <strong>and</strong>/or physical aggression, resistance to care, <strong>and</strong> w<strong>and</strong>er<strong>in</strong>g (See TryThis: W<strong>and</strong>er<strong>in</strong>g <strong>in</strong> the Hospitalized <strong>Older</strong> Adult).Fluctuation of mental status (unusual or chang<strong>in</strong>g function).Inattention: Assess by ask<strong>in</strong>g to say Days of the Week backwards or spell WORLD backwards <strong>and</strong> by observ<strong>in</strong>gfor problems focus<strong>in</strong>g, star<strong>in</strong>g off <strong>in</strong>to space, or los<strong>in</strong>g track of questions.Disorganized th<strong>in</strong>k<strong>in</strong>g: Assess by ask<strong>in</strong>g, “What would you do if your home or room were on fire?”Altered level of consciousness. Hyperactive or hypoalert. Remember lethargy, fall<strong>in</strong>g asleep, star<strong>in</strong>g off <strong>in</strong>tospace, <strong>and</strong> decreased motor activity is NOT NORMAL <strong>in</strong> older adults <strong>with</strong> dementia.(See Try This: Confusion Assessment Method)Assess for physiologic causes <strong>and</strong> riskfactors for delirium:Medication(s) (See AGS 2012 BeersCriteria; Try This: Beers Criteria)Fecal impactionUr<strong>in</strong>ary retentionInfection (ur<strong>in</strong>e, lungs, sk<strong>in</strong>)HypoxiaDehydrationHypo/hyperglycemiaPa<strong>in</strong> (See Try This: <strong>Assess<strong>in</strong>g</strong> Pa<strong>in</strong>)ImmobilitySensory impairmentPrevent <strong>in</strong>jury:Room near nurse’s station(monitor for excessive noise<strong>and</strong> stimulation due tolocation)Motion sensor alarmAsses fall risk (See TryThis: Fall Risk Assessment)Remove/camouflage tubeswhen possibleUse of <strong>in</strong>creasedsurveillance & round<strong>in</strong>gAdditional preventativestrategies:Environmental stimuli asappropriateMobilizeNon-drug alternatives <strong>and</strong>sleep protocolProvide sensory aidesCognitive stimulationHydration & nutritionPersonalizeactivities/room (all aboutme poster)Follow-up assessment Educate the family about the nature of delirium, <strong>in</strong>dicat<strong>in</strong>g this is not a “worsen<strong>in</strong>g ofdementia” but an acute or emergent health issue. Do admission <strong>and</strong> discharge teach<strong>in</strong>g. Cont<strong>in</strong>ue to assess cognition us<strong>in</strong>g the CAM <strong>and</strong> observ<strong>in</strong>g behaviors. Cont<strong>in</strong>ue <strong>with</strong> preventative strategies. Educate <strong>and</strong> counsel family regard<strong>in</strong>g signs of re-occurrence <strong>and</strong> duration (2 weeks to 6months) of delirium.dementia seriesBest Practices <strong>in</strong> Nurs<strong>in</strong>gCare to <strong>Older</strong> <strong>Adults</strong><strong>with</strong> dementiaA series provided by The Hartford Institute for Geriatric Nurs<strong>in</strong>g,New York University, College of Nurs<strong>in</strong>gEMAIL hartford.ign@nyu.edu HARTFORD INSTITUTE WEBSITE www.hartfordign.orgCLINICAL NURSING WEBSITE www.ConsultGeriRN.org