Completing request forms - Sullivan Nicolaides Pathology
Completing request forms - Sullivan Nicolaides Pathology
Completing request forms - Sullivan Nicolaides Pathology
- No tags were found...

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
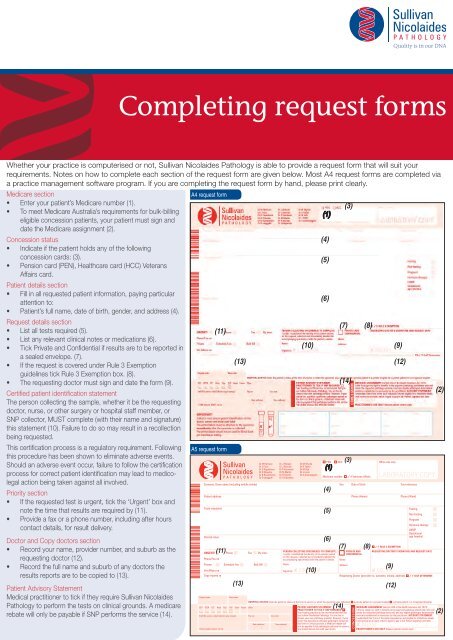
<strong>Completing</strong> <strong>request</strong> <strong>forms</strong>Whether your practice is computerised or not, <strong>Sullivan</strong> <strong>Nicolaides</strong> <strong>Pathology</strong> is able to provide a <strong>request</strong> form that will suit yourrequirements. Notes on how to complete each section of the <strong>request</strong> form are given below. Most A4 <strong>request</strong> <strong>forms</strong> are completed viaa practice management software program. If you are completing the <strong>request</strong> form by hand, please print clearly.Medicare section• Enter your patient’s Medicare number (1).• To meet Medicare Australia’s requirements for bulk-billingeligible concession patients, your patient must sign anddate the Medicare assignment (2).Concession status• Indicate if the patient holds any of the followingconcession cards: (3).• Pension card (PEN), Healthcare card (HCC) VeteransAffairs card.Patient details section• Fill in all <strong>request</strong>ed patient information, paying particularattention to:• Patient’s full name, date of birth, gender, and address (4).Request details section• List all tests required (5).• List any relevant clinical notes or medications (6).• Tick Private and Confidential if results are to be reported ina sealed envelope. (7).• If the <strong>request</strong> is covered under Rule 3 Exemptionguidelines tick Rule 3 Exemption box. (8).• The <strong>request</strong>ing doctor must sign and date the form (9).Certified patient identification statementThe person collecting the sample, whether it be the <strong>request</strong>ingdoctor, nurse, or other surgery or hospital staff member, orSNP collector, MUST complete (with their name and signature)this statement (10). Failure to do so may result in a recollectionbeing <strong>request</strong>ed.This certification process is a regulatory requirement. Followingthis procedure has been shown to eliminate adverse events.Should an adverse event occur, failure to follow the certificationprocess for correct patient identification may lead to medicolegalaction being taken against all involved.Priority section• If the <strong>request</strong>ed test is urgent, tick the ‘Urgent’ box andnote the time that results are required by (11).• Provide a fax or a phone number, including after hourscontact details, for result delivery.Doctor and Copy doctors section• Record your name, provider number, and suburb as the<strong>request</strong>ing doctor (12).• Record the full name and suburb of any doctors theresults reports are to be copied to (13).Patient Advisory StatementMedical practitioner to tick if they require <strong>Sullivan</strong> <strong>Nicolaides</strong><strong>Pathology</strong> to perform the tests on clinical grounds. A medicarerebate will only be payable if SNP per<strong>forms</strong> the service (14).A4 <strong>request</strong> form(11)A5 <strong>request</strong> form(13)ITEM 08534: A5 REQUEST: REQUEST FORM: PRINTS PMS 485: ISSUED 22 MAY 2012*08534-05-12*Surname, Given name (including middle initials)Patient addressTests <strong>request</strong>edClinical notesURGENT!Phone/Fax noPrivateVet Affairs no(11)PhoneSchedule FeeFaxBy time:Bulk Bill(10)(1)(4)(5)(6)PERSON COLLECTING SPECIMEN(S) TO COMPLETE:I certify I established the identity of the patient namedon this <strong>request</strong>, collected and immediately labelled theaccompanying specimen(s) with the patient’s details.Name:Signature: ✘ COLLECTORMedicare number(3)(7) (8)Copy reports to Requesting Doctor (provider no, surname, initials, address) ✓ IF SELF DETERMINE(13)Dr M HarrisonDr L PriceDr D PapadimosDr D WeedonDr B RowbothamDr D LangguthDr J RobsonDr J KencianDr P KanowskiDr M MartinDr N BuxtonDr I KrajewskaDr M WycheDr D TaylorDr M AshDr J LukinDr S Arianayagam(10)(14)SexDate of birthPhone (Home)PRIVATE ANDCONFIDENTIAL(9)(12)Your referencePhone (Work)Hospital codeWard codeHOSPITAL STATUS State the patient’s status at the time of service or when the specimen was collected: a private patient in a private hospital a private patient in a recognised hospitalSST EDTA CIT Histo Pap ThP Swab Frozen OtherPATIENT ADVISORY STATEMENT (14)MEDICARE ASSIGNMENT (Section 20A of the Health Insurance Act 1973):ThinPRACTITIONER TO TICK IF SNP REQUIRED:I offer to assign my right to benefits to the approved pathology practitioner who willTube Tube Tube Cont Slide PrepYour treating practitioner has recommended that you render the <strong>request</strong>ed pathology service(s) and any eligible pathologist determinableStaff ID/Location code/Collection type (stamp)Pay catCon codeuse <strong>Sullivan</strong> <strong>Nicolaides</strong> <strong>Pathology</strong>. You are free toservice(s) established as necessary by the practitioner. ACCOUNT STATEMENT:choose your own pathology provider. However, if your I understand that if any of the tests <strong>request</strong>ed are not eligible for a Medicare rebate,doctor has specified a particular pathologist named on I will receive an account, which I agree to pay in full. Patient signature and date:Date collectedTime collected this form on clinical grounds, a Medicare rebate willonly be payable if that pathologist per<strong>forms</strong> the service.ITEM 08534 MAY 2012/––––––/–:You should discuss this with your doctor.PRACTITIONER’S USE ONLY (Reason patient cannot sign):PEN—(1)(4)(5)(6)HCC(3)Name:Address:✓ if Veterans Affairs(7) (8)CONCESSIONOffice use onlyLABORATORY COPY✓ IF RULE 3 EXEMPTIONREQUESTING DOCTOR’S SIGNATURE AND REQUEST DATE(9)✘ DOCTOR(12)FastingNon-fastingPregnantHormone therapyLNMPGestationalage (weeks)✘ PATIENT /–––––––/–––––––––(2)(2)
Responsibilities of treating/<strong>request</strong>ing practitionersForm of RequestA treating practitioner may <strong>request</strong> a pathology service either orally or inwriting but oral <strong>request</strong>s must be confirmed in writing within fourteen daysfrom the day when the oral <strong>request</strong> was made.<strong>Pathology</strong> <strong>request</strong> <strong>forms</strong> and combined pathology <strong>request</strong>/offer to assign<strong>forms</strong> which are prepared by the pathologists and distributed to <strong>request</strong>ingpractitioners must be in accordance with the Medicare Australia approvedform (Ref: Australian Government Department of Health and Ageing,Medicare Benefits Schedule Book, Category 6, P.2.2 – operating from 01March 2012).Written pathology <strong>request</strong>s from treating practitioners thatare not on a form prepared and distributed by a pathologist do not need tobe approved. However, all written <strong>request</strong>s for pathology services shouldcontain the following particulars:1. the individual pathology services, or recognised groups of pathologytests to be rendered The description must be sufficient to enable theitem in which the service is specified to be identified;2. the date of <strong>request</strong>;3. the surname, initials of given names, practice address and providernumber of the <strong>request</strong>ing practitioner;4. the patient’s name and address;5. details of the hospital status of the patient, as follows (for benefit rateassessment). That is, whether the patient was or will be, at the time ofthe service and when the specimen is obtained:• a private patient in a private hospital, or approved day hospitalfacility;• a private patient in a recognised hospital;• a public patient in a recognised hospital;• an outpatient of a recognised hospital;6. details of the person to whom the <strong>request</strong> is directed. A pathology<strong>request</strong> can be directed to an Approved <strong>Pathology</strong> Practitioner oran Approved <strong>Pathology</strong> Authority. If the <strong>request</strong> is directed to anApproved <strong>Pathology</strong> Authority, the form must show the full nameand address of the Approved <strong>Pathology</strong> Authority. If the <strong>request</strong> isdirected to an Approved <strong>Pathology</strong> Practitioner, the form must showthe surname, initials or given names and place of practice of theApproved <strong>Pathology</strong> Practitioner to whom the <strong>request</strong> is addressed.Offence Not to Confirm an Oral RequestA <strong>request</strong>ing practitioner who, without reasonable excuse, does notconfirm in writing an oral <strong>request</strong> within fourteen days of making theoral <strong>request</strong> is guilty of an offence under the Health Insurance Act 1973punishable, upon conviction, by a fine not exceeding $1000, and the<strong>request</strong> is deemed never to have been made.ReferenceAustralian Government Department of Health and Ageing, Medicare Benefits ScheduleBook, Category 6, operating from July 2013.Item 09727 June 2013Correct at time of printing.SULLIVAN NICOLAIDES PTY LTD • ABN 38 078 202 196 • a subsidiary of Sonic Healthcare Limited • ABN 24 004 196 909134 WHITMORE STREET • TARINGA • QLD 4068 • AUSTRALIATEL (07) 3377 8666 • FAX (07) 3870 0549P O BOX 344 • INDOOROOPILLY • QLD 4068 • AUSTRALIAwww.snp.com.au©<strong>Sullivan</strong> <strong>Nicolaides</strong> Pty Ltd 2012– 2013