Imaging of Pulmonary Viral Pneumonia 1 - SIRM
Imaging of Pulmonary Viral Pneumonia 1 - SIRM
Imaging of Pulmonary Viral Pneumonia 1 - SIRM
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
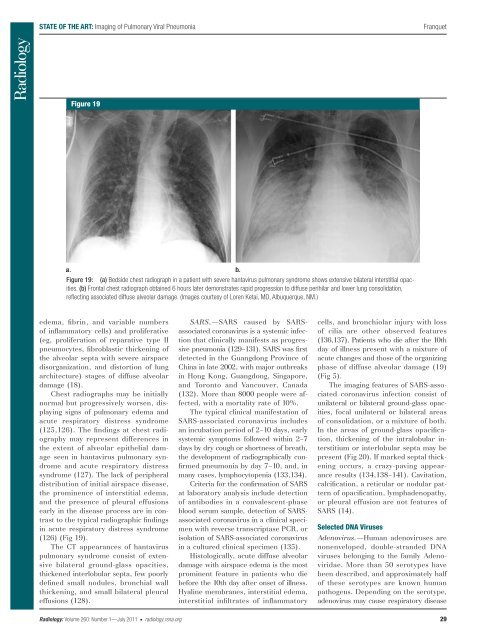
STATE OF THE ART: <strong>Imaging</strong> <strong>of</strong> <strong>Pulmonary</strong> <strong>Viral</strong> <strong>Pneumonia</strong>FranquetFigure 19Figure 19: (a) Bedside chest radiograph in a patient with severe hantavirus pulmonary syndrome shows extensive bilateral interstitial opacities.(b) Frontal chest radiograph obtained 6 hours later demonstrates rapid progression to diffuse perihilar and lower lung consolidation ,refl ecting associated diffuse alveolar damage. (Images courtesy <strong>of</strong> Loren Ketai, MD, Albuquerque, NM.)edema, fibrin, and variable numbers<strong>of</strong> inflammatory cells) and proliferative(eg, proliferation <strong>of</strong> reparative type IIpneumocytes, fibroblastic thickening <strong>of</strong>the alveolar septa with severe airspacedisorganization, and distortion <strong>of</strong> lungarchitecture) stages <strong>of</strong> diffuse alveolardamage ( 18 ).Chest radiographs may be initiallynormal but progressively worsen, displayingsigns <strong>of</strong> pulmonary edema andacute respiratory distress syndrome( 125 , 126 ). The findings at chest radiographymay represent differences inthe extent <strong>of</strong> alveolar epithelial damageseen in hantavirus pulmonary syndromeand acute respiratory distresssyndrome ( 127 ). The lack <strong>of</strong> peripheraldistribution <strong>of</strong> initial airspace disease,the prominence <strong>of</strong> interstitial edema,and the presence <strong>of</strong> pleural effusionsearly in the disease process are in contrastto the typical radiographic findingsin acute respiratory distress syndrome( 126 ) ( Fig 19 ).The CT appearances <strong>of</strong> hantaviruspulmonary syndrome consist <strong>of</strong> extensivebilateral ground-glass opacities,thickened interlobular septa, few poorlydefined small nodules, bronchial wallthick ening, and small bilateral pleuraleffusions ( 128 ).SARS.— SARS caused by SARSassociated coronavirus is a systemic infectionthat clinically manifests as progressivepneumonia ( 129 – 131 ). SARS was firstdetected in the Guangdong Province <strong>of</strong>China in late 2002, with major outbreaksin Hong Kong, Guangdong, Singapore,and Toronto and Vancouver, Canada( 132 ). More than 8000 people were affected,with a mortality rate <strong>of</strong> 10%.The typical clinical manifestation <strong>of</strong>SARS-associated coronavirus includesan incubation period <strong>of</strong> 2–10 days, earlysystemic symptoms followed within 2–7days by dry cough or shortness <strong>of</strong> breath,the development <strong>of</strong> radiographically confirmedpneumonia by day 7–10, and, inmany cases, lymphocytopenia ( 133 , 134 ).Criteria for the confirmation <strong>of</strong> SARSat laboratory analysis include detection<strong>of</strong> antibodies in a convalescent-phaseblood serum sample, detection <strong>of</strong> SARSassociatedcoronavirus in a clinical specimenwith reverse transcriptase PCR, orisolation <strong>of</strong> SARS-associated coronavirusin a cultured clinical specimen ( 135 ).Histologically, acute diffuse alveolardamage with airspace edema is the mostprominent feature in patients who diebefore the 10th day after onset <strong>of</strong> illness.Hyaline membranes, interstitial edema,interstitial infiltrates <strong>of</strong> inflammatorycells, and bronchiolar injury with loss<strong>of</strong> cilia are other observed features( 136 , 137 ). Patients who die after the 10thday <strong>of</strong> illness present with a mixture <strong>of</strong>acute changes and those <strong>of</strong> the organizingphase <strong>of</strong> diffuse alveolar damage ( 19 )( Fig 5 ).The imaging features <strong>of</strong> SARS-associatedcoronavirus infection consist <strong>of</strong>unilateral or bilateral ground-glass opacities,focal unilateral or bilateral areas<strong>of</strong> consolidation, or a mixture <strong>of</strong> both.In the areas <strong>of</strong> ground-glass opacification,thickening <strong>of</strong> the intralobular interstitiumor interlobular septa may bepresent ( Fig 20 ). If marked septal thickeningoccurs, a crazy-paving appearanceresults ( 134 , 138 – 141 ). Cavitation,calcification, a reticular or nodular pattern<strong>of</strong> opacification, lymphadenopathy,or pleural effusion are not features <strong>of</strong>SARS ( 14 ).Selected DNA VirusesAdenovirus.— Human adenoviruses arenonenveloped, double-stranded DNAviruses belonging to the family Adenoviridae.More than 50 serotypes havebeen described, and approximately half<strong>of</strong> these serotypes are known humanpathogens. Depending on the serotype,adenovirus may cause respiratory diseaseRadiology: Volume 260: Number 1—July 2011 n radiology.rsna.org 29