Review article Ability to pay for health care: concepts and evidence
Review article Ability to pay for health care: concepts and evidence
Review article Ability to pay for health care: concepts and evidence

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
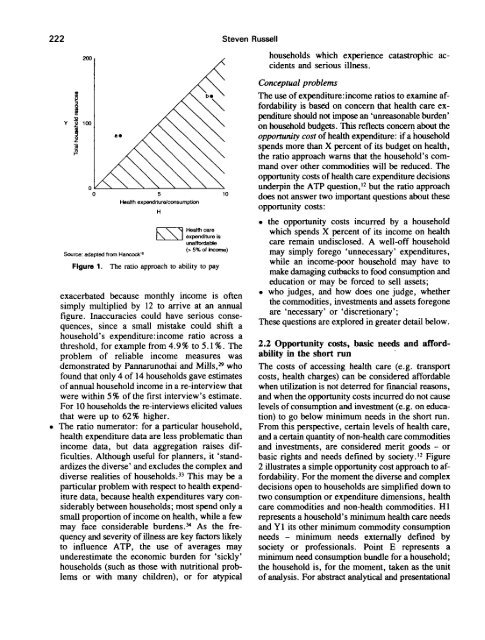
222 Steven Russell200Source: adapted from Hancock 11Figure 1.Health expenditure/consumptionHHealth <strong>care</strong>expenditure launai<strong>for</strong>dabte(> 5% of Income)The ratio approach <strong>to</strong> ability <strong>to</strong> <strong>pay</strong>exacerbated because monthly income is oftensimply multiplied by 12 <strong>to</strong> arrive at an annualfigure. Inaccuracies could have serious consequences,since a small mistake could shift ahousehold's expenditure:income ratio across athreshold, <strong>for</strong> example from 4.9% <strong>to</strong> 5.1%. Theproblem of reliable income measures wasdemonstrated by Pannarunothai <strong>and</strong> Mills, 29 whofound that only 4 of 14 households gave estimatesof annual household income in a re-interview thatwere within 5% of the first interview's estimate.For 10 households the re-interviews elicited valuesthat were up <strong>to</strong> 62% higher.The ratio numera<strong>to</strong>r: <strong>for</strong> a particular household,<strong>health</strong> expenditure data are less problematic thanincome data, but data aggregation raises difficulties.Although useful <strong>for</strong> planners, it 'st<strong>and</strong>ardizesthe diverse' <strong>and</strong> excludes the complex <strong>and</strong>diverse realities of households. 33 This may be aparticular problem with respect <strong>to</strong> <strong>health</strong> expendituredata, because <strong>health</strong> expenditures vary considerablybetween households; most spend only asmall proportion of income on <strong>health</strong>, while a fewmay face considerable burdens. 34 As the frequency<strong>and</strong> severity of illness are key fac<strong>to</strong>rs likely<strong>to</strong> influence ATP, the use of averages mayunderestimate the economic burden <strong>for</strong> 'sickly'households (such as those with nutritional problemsor with many children), or <strong>for</strong> atypicalhouseholds which experience catastrophic accidents<strong>and</strong> serious illness.Conceptual problemsThe use of expenditure:income ratios <strong>to</strong> examine af<strong>for</strong>dabilityis based on concern that <strong>health</strong> <strong>care</strong> expenditureshould not impose an 'unreasonable burden'on household budgets. This reflects concern about theopportunity cost of <strong>health</strong> expenditure: if a householdspends more than X percent of its budget on <strong>health</strong>,the ratio approach warns that the household's comm<strong>and</strong>over other commodities will be reduced. Theopportunity costs of <strong>health</strong> <strong>care</strong> expenditure decisionsunderpin the ATP question, 12 but the ratio approachdoes not answer two important questions about theseopportunity costs:• the opportunity costs incurred by a householdwhich spends X percent of its income on <strong>health</strong><strong>care</strong> remain undisclosed. A well-off householdmay simply <strong>for</strong>ego 'unnecessary' expenditures,while an income-poor household may have <strong>to</strong>make damaging cutbacks <strong>to</strong> food consumption <strong>and</strong>education or may be <strong>for</strong>ced <strong>to</strong> sell assets;• who judges, <strong>and</strong> how does one judge, whetherthe commodities, investments <strong>and</strong> assets <strong>for</strong>egoneare 'necessary' or 'discretionary';These questions are explored in greater detail below.2.2 Opportunity costs, bask needs <strong>and</strong> af<strong>for</strong>dabilityin the short runThe costs of accessing <strong>health</strong> <strong>care</strong> (e.g. transportcosts, <strong>health</strong> charges) can be considered af<strong>for</strong>dablewhen utilization is not deterred <strong>for</strong> financial reasons,<strong>and</strong> when the opportunity costs incurred do not causelevels of consumption <strong>and</strong> investment (e.g. on education)<strong>to</strong> go below minimum needs in the short run.From this perspective, certain levels of <strong>health</strong> <strong>care</strong>,<strong>and</strong> a certain quantity of non-<strong>health</strong> <strong>care</strong> commodities<strong>and</strong> investments, are considered merit goods - orbasic rights <strong>and</strong> needs defined by society. 12 Figure2 illustrates a simple opportunity cost approach <strong>to</strong> af<strong>for</strong>dability.For the moment the diverse <strong>and</strong> complexdecisions open <strong>to</strong> households are simplified down <strong>to</strong>two consumption or expenditure dimensions, <strong>health</strong><strong>care</strong> commodities <strong>and</strong> non-<strong>health</strong> commodities. HIrepresents a household's minimum <strong>health</strong> <strong>care</strong> needs<strong>and</strong> Y1 its other minimum commodity consumptionneeds - minimum needs externally defined bysociety or professionals. Point E represents aminimum need consumption bundle <strong>for</strong> a household;the household is, <strong>for</strong> the moment, taken as the uni<strong>to</strong>f analysis. For abstract analytical <strong>and</strong> presentational