COMMERCIAL DRIVER APPLICATION
COMMERCIAL DRIVER APPLICATION
COMMERCIAL DRIVER APPLICATION

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
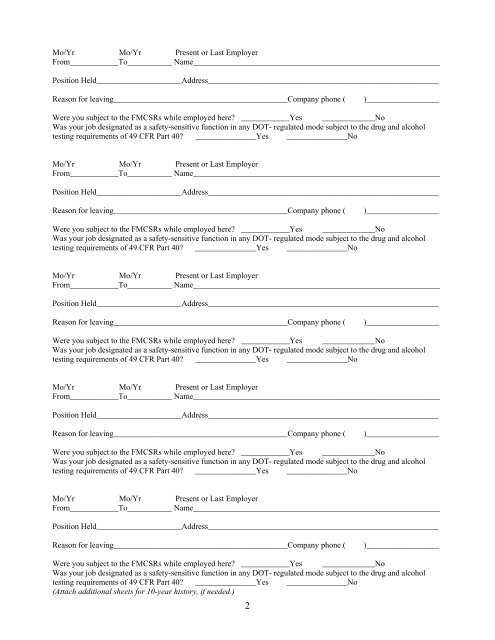
Mo/Yr Mo/Yr Present or Last EmployerFrom____________To___________ Name_____________________________________________________________Position Held_____________________Address_________________________________________________________Reason for leaving___________________________________________Company phone ()__________________Were you subject to the FMCSRs while employed here? ____________Yes _____________NoWas your job designated as a safety-sensitive function in any DOT- regulated mode subject to the drug and alcoholtesting requirements of 49 CFR Part 40? _______________Yes _______________NoMo/Yr Mo/Yr Present or Last EmployerFrom____________To___________ Name_____________________________________________________________Position Held_____________________Address_________________________________________________________Reason for leaving___________________________________________Company phone ()__________________Were you subject to the FMCSRs while employed here? ____________Yes _____________NoWas your job designated as a safety-sensitive function in any DOT- regulated mode subject to the drug and alcoholtesting requirements of 49 CFR Part 40? _______________Yes _______________NoMo/Yr Mo/Yr Present or Last EmployerFrom____________To___________ Name_____________________________________________________________Position Held_____________________Address_________________________________________________________Reason for leaving___________________________________________Company phone ()__________________Were you subject to the FMCSRs while employed here? ____________Yes _____________NoWas your job designated as a safety-sensitive function in any DOT- regulated mode subject to the drug and alcoholtesting requirements of 49 CFR Part 40? _______________Yes _______________NoMo/Yr Mo/Yr Present or Last EmployerFrom____________To___________ Name_____________________________________________________________Position Held_____________________Address_________________________________________________________Reason for leaving___________________________________________Company phone ()__________________Were you subject to the FMCSRs while employed here? ____________Yes _____________NoWas your job designated as a safety-sensitive function in any DOT- regulated mode subject to the drug and alcoholtesting requirements of 49 CFR Part 40? _______________Yes _______________NoMo/Yr Mo/Yr Present or Last EmployerFrom____________To___________ Name_____________________________________________________________Position Held_____________________Address_________________________________________________________Reason for leaving___________________________________________Company phone ()__________________Were you subject to the FMCSRs while employed here? ____________Yes _____________NoWas your job designated as a safety-sensitive function in any DOT- regulated mode subject to the drug and alcoholtesting requirements of 49 CFR Part 40? _______________Yes _______________No(Attach additional sheets for 10-year history, if needed.)2