

Guidence FP170 A4 - NHS Business Services Authority
Guidence FP170 A4 - NHS Business Services Authority
Guidence FP170 A4 - NHS Business Services Authority
- No tags were found...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
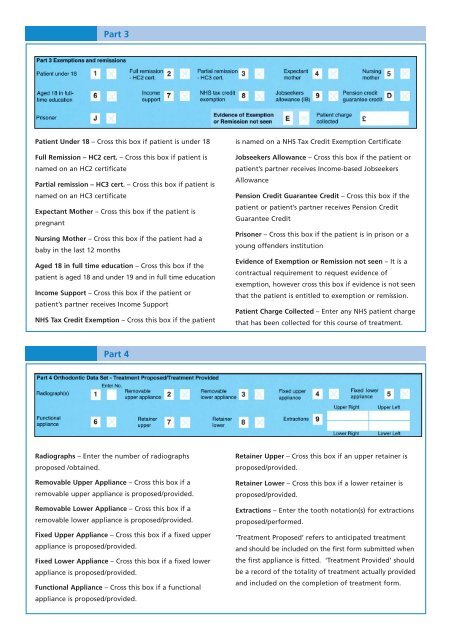
Part 3Patient Under 18 – Cross this box if patient is under 18Full Remission – HC2 cert. – Cross this box if patient isnamed on an HC2 certificatePartial remission – HC3 cert. – Cross this box if patient isnamed on an HC3 certificateExpectant Mother – Cross this box if the patient ispregnantNursing Mother – Cross this box if the patient had ababy in the last 12 monthsAged 18 in full time education – Cross this box if thepatient is aged 18 and under 19 and in full time educationIncome Support – Cross this box if the patient orpatient’s partner receives Income Support<strong>NHS</strong> Tax Credit Exemption – Cross this box if the patientis named on a <strong>NHS</strong> Tax Credit Exemption CertificateJobseekers Allowance – Cross this box if the patient orpatient’s partner receives Income-based JobseekersAllowancePension Credit Guarantee Credit – Cross this box if thepatient or patient’s partner receives Pension CreditGuarantee CreditPrisoner – Cross this box if the patient is in prison or ayoung offenders institutionEvidence of Exemption or Remission not seen – It is acontractual requirement to request evidence ofexemption, however cross this box if evidence is not seenthat the patient is entitled to exemption or remission.Patient Charge Collected – Enter any <strong>NHS</strong> patient chargethat has been collected for this course of treatment.Part 4Radiographs – Enter the number of radiographsproposed /obtained.Removable Upper Appliance – Cross this box if aremovable upper appliance is proposed/provided.Removable Lower Appliance – Cross this box if aremovable lower appliance is proposed/provided.Fixed Upper Appliance – Cross this box if a fixed upperappliance is proposed/provided.Fixed Lower Appliance – Cross this box if a fixed lowerappliance is proposed/provided.Functional Appliance – Cross this box if a functionalappliance is proposed/provided.Retainer Upper – Cross this box if an upper retainer isproposed/provided.Retainer Lower – Cross this box if a lower retainer isproposed/provided.Extractions – Enter the tooth notation(s) for extractionsproposed/performed.‘Treatment Proposed’ refers to anticipated treatmentand should be included on the first form submitted whenthe first appliance is fitted. ‘Treatment Provided’ shouldbe a record of the totality of treatment actually providedand included on the completion of treatment form.













