Sickle Cell Form/Waiver - University of Texas at Dallas
Sickle Cell Form/Waiver - University of Texas at Dallas
Sickle Cell Form/Waiver - University of Texas at Dallas

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
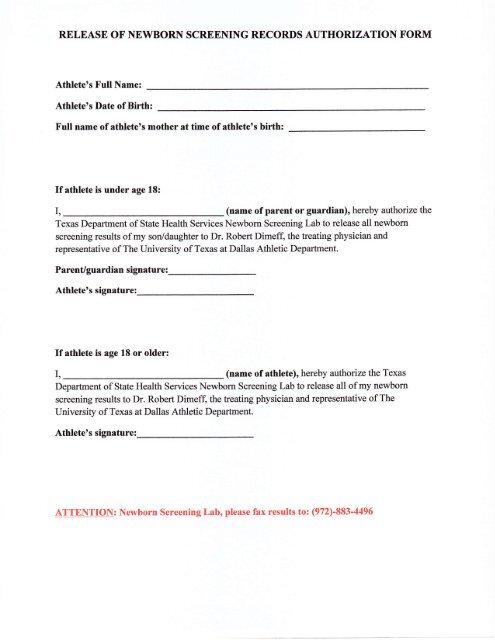
RELEASE OF NEWBORN SCREENING RECORDS AUTHORIZATION FORMAthleteos Full Name:Athlete's D<strong>at</strong>e <strong>of</strong> Birth:FuIl name <strong>of</strong> <strong>at</strong>hlete's mother <strong>at</strong> time <strong>of</strong> <strong>at</strong>hlete's birth:If <strong>at</strong>hlete is under age 18:I, (name <strong>of</strong> parent or guardian), hereby authorize the<strong>Texas</strong> Department <strong>of</strong> St<strong>at</strong>e Health Services Newborn Screening Lab to release all newbomscreening results <strong>of</strong> my son/daughter to Dr. Robert Dimeff, the tre<strong>at</strong>ing physician andrepresent<strong>at</strong>ive <strong>of</strong> The <strong>University</strong> <strong>of</strong> <strong>Texas</strong> <strong>at</strong> <strong>Dallas</strong> Athletic Department.Parent/guardian sign<strong>at</strong>ure:Athletets sign<strong>at</strong>ure:If <strong>at</strong>hlete is age 18 or older:I, (name <strong>of</strong> <strong>at</strong>hlete), hereby authorize the <strong>Texas</strong>Department <strong>of</strong> St<strong>at</strong>e Health Services Newborn Screening Lab to release all <strong>of</strong> my newbornscreening results to Dr. Robert Dimeff, the tre<strong>at</strong>ing physician and represent<strong>at</strong>ive <strong>of</strong> The<strong>University</strong> <strong>of</strong> <strong>Texas</strong> <strong>at</strong> <strong>Dallas</strong> Athletic Department.Athlete's sign<strong>at</strong>ure:ATTENTION: Newborn Screening Lab, please fax results to: (972)-883-4496