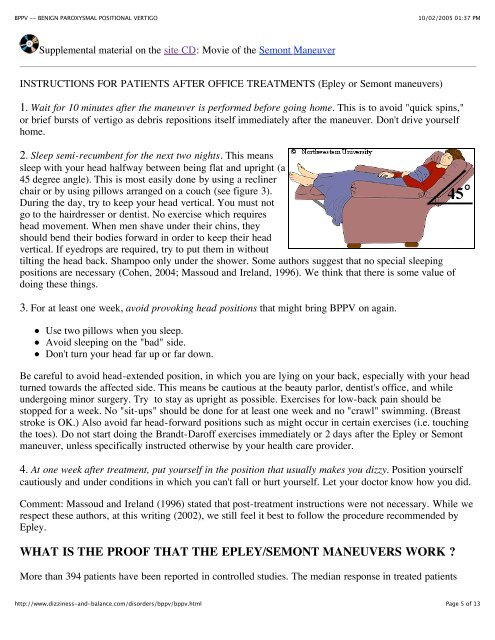
BPPV -- <strong>BENIGN</strong> <strong>PAROXYSMAL</strong> <strong>POSITIONAL</strong> <strong>VERTIGO</strong>10/02/2005 01:37 PMmove debris or "ear rocks" out of the sensitive part of the ear(posterior <strong>ca</strong>nal) to a less sensitive lo<strong>ca</strong>tion. Each maneuver takesabout 15 minutes to complete. The Semont maneuver (also<strong>ca</strong>lled the "liberatory" maneuver) involves a procedure wherebythe patient is rapidly moved from lying on one side to lying onthe other (Levrat et al, 2003). It is a brisk maneuver that is notcurrently favored in the United States, but it is 90% effective after4 treatment sessions. In our opinion, it is equivalent to the Epleymaneuver as the head positioning is very similar, omitting only'C' from the figure to the right.The Epley maneuver is also <strong>ca</strong>lled the particle repositioning, <strong>ca</strong>nalith repositioning procedure, andmodified liberatory maneuver. It is illustrated in figure 2. Click here for a low bandwidth animation. Itinvolves sequential movement of the head into four positions, staying in each position for roughly 30seconds. The recurrence rate for BPPV after these maneuvers is about 30 percent at one year, and in someinstances a second treatment may be necessary.Variants: While some authors advo<strong>ca</strong>te use of vibration in the Epley maneuver, we have not found thisuseful in a study of our patients (Hain et al, 2000). Use of an antiemetic prior to the maneuver may behelpful if nausea is anticipated. Some authors suggest that position 'D' in the figure is not necessary (e.g.(Cohen et al. 1999; Cohen et al. 2004 ). In our opinion, this is a mistake as mathemati<strong>ca</strong>l modeling of BPPVsuggests that position 'D' is the most important position (Squires et al, 2004).When performing the Epley maneuver, <strong>ca</strong>ution is advised should neurologi<strong>ca</strong>l symptoms (for example,weakness, numbness, visual changes other than vertigo) occur. Oc<strong>ca</strong>sionally such symptoms are <strong>ca</strong>used bycompression of the vertebral arteries (Sakaguchi et al, 2003), and if one persists, a stroke could occur. If theexercises are being performed without medi<strong>ca</strong>l supervision, we advise stopping the exercises and consultinga physician. If the exercises are being supervised, given that the diagnosis of BPPV is well established, inmost <strong>ca</strong>ses we modify the maneuver so that the positions are attained with body movements rather than headmovements.After either of these maneuvers, you should be prepared to follow the instructions below, which are aimedat reducing the chance that debris might fall back into the sensitive back part of the ear.The "Gans" maneuver. This is a little used treatment maneuver, <strong>ca</strong>lled the "Gans maneuver by it'sinventor (R. Gans, Ph.D.), that is a hybrid between the Epley and Semont maneuvers. It incorporates thehead orientations to gravity of "B" and "D" in the Epley figure above, using the body positions of theSemont maneuver. There is too little published experience with this maneuver to say whether it is aseffective as the Epley/Semont but we suspect that it has the same effi<strong>ca</strong>cy, as it uses the same headpositions.Supplemental material on the site CD: Animation of Epley Maneuver.Note that this maneuver is done faster in the animation than in the clinic. Usually one allows 30 secondsbetween positions.http://www.dizziness-and-balance.com/disorders/bppv/bppv.htmlPage 4 of 13