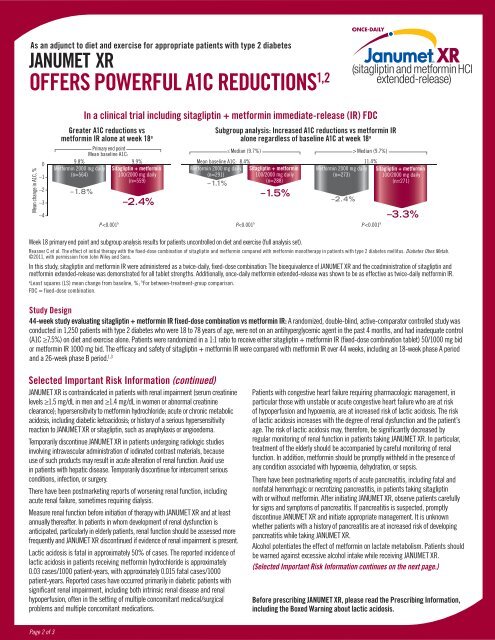
As an adjunct to diet and exercise <strong>for</strong> appropriate patients <strong>with</strong> type 2 diabetes<strong>JANUMET</strong> <strong>XR</strong>OFFERS POWERFUL A1C REDUCTIONS 1,2Mean change in A1C, %0–1–2–3–49.8%Met<strong>for</strong>min 2000 mg <strong>daily</strong>(n=564)–1.8%In a clinical trial including sitagliptin + met<strong>for</strong>min immediate-release (IR) FDCGreater A1C reductions vsmet<strong>for</strong>min IR alone at week 18 aPrimary end pointMean baseline A1C:P Median (9.7%)Mean baseline A1C: 8.4%11.4%Met<strong>for</strong>min 2000 mg <strong>daily</strong> Sitagliptin + met<strong>for</strong>min Met<strong>for</strong>min 2000 mg <strong>daily</strong> Sitagliptin + met<strong>for</strong>min(n=291)100/2000 mg <strong>daily</strong>(n=273)100/2000 mg <strong>daily</strong>–1.1%(n=288)(n=271)P
IN THIS STUDY, SIMILAR WEIGHT CHANGE,RATES OF HYPOGLYCEMIA, AND GI EVENTSVS METFORMIN IR ALONE 1• Weight loss <strong>for</strong> sitagliptin + met<strong>for</strong>min IR FDC similar to met<strong>for</strong>min IR alone at week 18 (LS mean change from baseline: –3.5 lb <strong>for</strong> both groups)• Incidence of hypoglycemia <strong>for</strong> sitagliptin + met<strong>for</strong>min IR FDC similar to met<strong>for</strong>min IR alone over 18 weeks (2.1% [n/N=13/625] vs 1.8% [n/N=11/621], respectively)• Similar rate of GI adverse events vs met<strong>for</strong>min IR alone over 18 weeksWhen added to a sulfonylurea (glimepiride) or insulin, patients treated <strong>with</strong> sitagliptin + met<strong>for</strong>min IR experiencedincreased weight and incidence of hypoglycemia• Weight gain: +0.9 lb <strong>for</strong> patients treated <strong>with</strong> sitagliptin + met<strong>for</strong>min IR + glimepiride vs –1.5 lb <strong>for</strong> placebo + met<strong>for</strong>min IR + glimepiride• Hypoglycemia: 16% <strong>for</strong> patients treated <strong>with</strong> sitagliptin + met<strong>for</strong>min IR + glimepiride vs 1% <strong>for</strong> placebo + met<strong>for</strong>min IR + glimepiride and 15% <strong>for</strong> patients treated <strong>with</strong>sitagliptin + met<strong>for</strong>min IR + insulin vs 8% <strong>for</strong> placebo + met<strong>for</strong>min IR + insulin. A lower dose of sulfonylurea or insulin may be required to reduce the risk of hypoglycemiaGI = gastrointestinal.Please see Study Design on page 2 <strong>for</strong> more in<strong>for</strong>mation.Selected Important Risk In<strong>for</strong>mation (continued)Intravascular contrast studies <strong>with</strong> iodinated materials can lead to acutealteration of renal function and have been associated <strong>with</strong> lactic acidosis inpatients receiving met<strong>for</strong>min. There<strong>for</strong>e, in patients in whom any such studyis planned, <strong>JANUMET</strong> <strong>XR</strong> should be temporarily discontinued at the time of orbe<strong>for</strong>e the procedure, <strong>with</strong>held <strong>for</strong> 48 hours subsequent to the procedure, andreinstituted only after renal function has been re-evaluated and found tobe normal.There have been no clinical studies establishing conclusive evidence ofUse With Medications Known to Cause HypoglycemiaSitagliptinWhen sitagliptin was used in combination <strong>with</strong> a sulfonylurea or insulin,medications known to cause hypoglycemia, the incidence of hypoglycemiawas increased over that of placebo used in combination <strong>with</strong> a sulfonylurea orinsulin. There<strong>for</strong>e, patients also receiving insulin or an insulin secretagogue (eg,sulfonylurea) may require a lower dose of insulin or the insulin secretagogue toreduce the risk of hypoglycemia.The incidence (and rate) of hypoglycemia based on all reports of symptomatichypoglycemia were: 16.4% (0.82 episodes/patient-year) <strong>for</strong> sitagliptin 100 mg incombination <strong>with</strong> met<strong>for</strong>min and glimepiride, 0.9% (0.02 episodes/patient-year)<strong>for</strong> placebo in combination <strong>with</strong> met<strong>for</strong>min and glimepiride, 8.2% (0.61 episodes/patient-year) <strong>for</strong> placebo in combination <strong>with</strong> met<strong>for</strong>min and insulin, and 15.3%(0.98 episodes/patient-year) <strong>for</strong> sitagliptin in combination <strong>with</strong> met<strong>for</strong>minand insulin.Adverse reactions <strong>with</strong> sitagliptin in combination <strong>with</strong> met<strong>for</strong>min and rosiglitazonethrough Week 18 were: upper respiratory tract infection (sitagliptin, 5.5%; placebo,5.2%) and nasopharyngitis (6.1%, 4.1%). Through Week 54 they were: upperrespiratory tract infection (sitagliptin, 15.5%; placebo, 6.2%), nasopharyngitis(11.0%, 9.3%), peripheral edema (8.3%, 5.2%), and headache (5.5%, 4.1%).Met<strong>for</strong>min hydrochlorideHypoglycemia does not occur in patients receiving met<strong>for</strong>min alone under usualcircumstances of use but could occur when caloric intake is deficient, whenstrenuous exercise is not compensated by caloric supplementation, or duringCopyright © 2013 Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc. All rights reserved.DIAB-1079801-0001 07/13Janumet<strong>XR</strong>.comconcomitant use <strong>with</strong> other glucose-lowering agents (such as sulfonylureas andinsulin) or ethanol. Elderly, debilitated, or malnourished patients and those <strong>with</strong>adrenal or pituitary insufficiency or alcohol intoxication are particularly susceptible tohypoglycemic effects.There have been postmarketing reports of serious hypersensitivity reactions inpatients treated <strong>with</strong> sitagliptin, one of the components of <strong>JANUMET</strong> <strong>XR</strong>, such asanaphylaxis, angioedema, and exfoliative skin conditions including Stevens-Johnsonsyndrome. Onset of these reactions occurred <strong>with</strong>in the first 3 months after initiationof treatment <strong>with</strong> sitagliptin, <strong>with</strong> some reports occurring after the first dose. If ahypersensitivity reaction is suspected, discontinue <strong>JANUMET</strong> <strong>XR</strong>, assess <strong>for</strong> otherpotential causes <strong>for</strong> the event, and institute alternative treatment <strong>for</strong> diabetes.Use caution in a patient <strong>with</strong> a history of angioedema to another dipeptidylpeptidase-4 (DPP-4) inhibitor because it is unknown whether such patients will bepredisposed to angioedema <strong>with</strong> <strong>JANUMET</strong> <strong>XR</strong>.In clinical studies, the most common adverse reactions reported, regardless ofinvestigator assessment of causality, in ≥5% of patients treated <strong>with</strong> eithersitagliptin in combination <strong>with</strong> met<strong>for</strong>min or placebo were as follows: diarrhea(7.5% vs 4.0%), upper respiratory tract infection (6.2% vs 5.1%), and headache(5.9% vs 2.8%). In patients treated <strong>with</strong> sitagliptin in combination <strong>with</strong> met<strong>for</strong>minand sulfonylurea or placebo in combination <strong>with</strong> met<strong>for</strong>min and sulfonylurea:hypoglycemia (16.4% vs 0.9%) and headache (6.9% vs 2.7%). In patients treated<strong>with</strong> sitagliptin in combination <strong>with</strong> met<strong>for</strong>min and insulin or placebo in combination<strong>with</strong> met<strong>for</strong>min and insulin: hypoglycemia (15.3% vs 8.2%). Other adverse events<strong>with</strong> an incidence of ≥5% included nasopharyngitis <strong>for</strong> sitagliptin monotherapy andhypoglycemia (13.7% vs 4.9%), diarrhea (12.5% vs 5.6%), and nausea (6.7% vs4.2%) <strong>for</strong> extended-release met<strong>for</strong>min vs placebo when added to glyburide.The incidence of selected gastrointestinal adverse reactions in patients treated <strong>with</strong>sitagliptin and met<strong>for</strong>min was similar to those of placebo and met<strong>for</strong>min: nausea(1.3%, 0.8%), vomiting (1.1%, 0.8%), abdominal pain (2.2%, 3.8%), and diarrhea(2.4%, 2.5%).Be<strong>for</strong>e prescribing <strong>JANUMET</strong> <strong>XR</strong>, please read the Prescribing In<strong>for</strong>mation,including the Boxed Warning about lactic acidosis.For additional copies of the Prescribing In<strong>for</strong>mation, please call 800-672-6372,visit Janumet<strong>XR</strong>.com, or contact your Merck representative.References: 1. Reasner C, Olansky L, Seck TL, et al. The effect of initial therapy <strong>with</strong> the fixed-dose combination of sitagliptin and met<strong>for</strong>min compared <strong>with</strong> met<strong>for</strong>min monotherapy in patients <strong>with</strong> type 2 diabetes mellitus. Diabetes ObesMetab. 2011;13(7):644–652. 2. Data available on request from Merck, Professional Services-DAP, WP1-27, PO Box 4, West Point, PA 19486-0004. Please specify in<strong>for</strong>mation package DIAB-1038791-0005. 3. Olansky L, Reasner C, Seck TL,et al. A treatment strategy implementing combination therapy <strong>with</strong> sitagliptin and met<strong>for</strong>min results in superior glycaemic control versus met<strong>for</strong>min monotherapy due to a low rate of addition of antihyperglycaemic agents. Diabetes ObesMetab. 2011;13(9):841–849.Page 3 of 3