Start with once-daily JANUMET XR for convenient dosing - Januvia
Start with once-daily JANUMET XR for convenient dosing - Januvia
Start with once-daily JANUMET XR for convenient dosing - Januvia

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
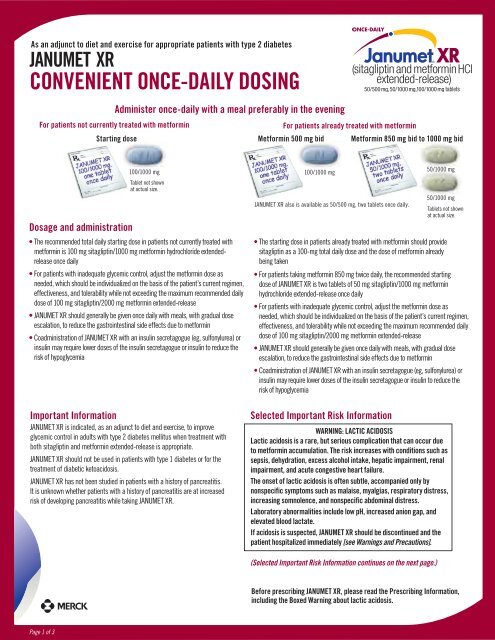
As an adjunct to diet and exercise <strong>for</strong> appropriate patients <strong>with</strong> type 2 diabetes<strong>JANUMET</strong> <strong>XR</strong>CONVENIENT ONCE-DAILY DOSINGFor patients not currently treated <strong>with</strong> met<strong>for</strong>minAdminister <strong>once</strong>-<strong>daily</strong> <strong>with</strong> a meal preferably in the evening<strong>Start</strong>ing doseFor patients already treated <strong>with</strong> met<strong>for</strong>minMet<strong>for</strong>min 500 mg bid Met<strong>for</strong>min 850 mg bid to 1000 mg bidDosage and administration100/1000 mgTablet not shownat actual size.• The recommended total <strong>daily</strong> starting dose in patients not currently treated <strong>with</strong>met<strong>for</strong>min is 100 mg sitagliptin/1000 mg met<strong>for</strong>min hydrochloride extendedrelease<strong>once</strong> <strong>daily</strong>• For patients <strong>with</strong> inadequate glycemic control, adjust the met<strong>for</strong>min dose asneeded, which should be individualized on the basis of the patient’s current regimen,effectiveness, and tolerability while not exceeding the maximum recommended <strong>daily</strong>dose of 100 mg sitagliptin/2000 mg met<strong>for</strong>min extended-release• <strong>JANUMET</strong> <strong>XR</strong> should generally be given <strong>once</strong> <strong>daily</strong> <strong>with</strong> meals, <strong>with</strong> gradual doseescalation, to reduce the gastrointestinal side effects due to met<strong>for</strong>min• Coadministration of <strong>JANUMET</strong> <strong>XR</strong> <strong>with</strong> an insulin secretagogue (eg, sulfonylurea) orinsulin may require lower doses of the insulin secretagogue or insulin to reduce therisk of hypoglycemiaImportant In<strong>for</strong>mation<strong>JANUMET</strong> <strong>XR</strong> is indicated, as an adjunct to diet and exercise, to improveglycemic control in adults <strong>with</strong> type 2 diabetes mellitus when treatment <strong>with</strong>both sitagliptin and met<strong>for</strong>min extended-release is appropriate.<strong>JANUMET</strong> <strong>XR</strong> should not be used in patients <strong>with</strong> type 1 diabetes or <strong>for</strong> thetreatment of diabetic ketoacidosis.<strong>JANUMET</strong> <strong>XR</strong> has not been studied in patients <strong>with</strong> a history of pancreatitis.It is unknown whether patients <strong>with</strong> a history of pancreatitis are at increasedrisk of developing pancreatitis while taking <strong>JANUMET</strong> <strong>XR</strong>.100/1000 mg<strong>JANUMET</strong> <strong>XR</strong> also is available as 50/500 mg, two tablets <strong>once</strong> <strong>daily</strong>.• The starting dose in patients already treated <strong>with</strong> met<strong>for</strong>min should providesitagliptin as a 100-mg total <strong>daily</strong> dose and the dose of met<strong>for</strong>min alreadybeing taken• For patients taking met<strong>for</strong>min 850 mg twice <strong>daily</strong>, the recommended startingdose of <strong>JANUMET</strong> <strong>XR</strong> is two tablets of 50 mg sitagliptin/1000 mg met<strong>for</strong>minhydrochloride extended-release <strong>once</strong> <strong>daily</strong>• For patients <strong>with</strong> inadequate glycemic control, adjust the met<strong>for</strong>min dose asneeded, which should be individualized on the basis of the patient’s current regimen,effectiveness, and tolerability while not exceeding the maximum recommended <strong>daily</strong>dose of 100 mg sitagliptin/2000 mg met<strong>for</strong>min extended-release• <strong>JANUMET</strong> <strong>XR</strong> should generally be given <strong>once</strong> <strong>daily</strong> <strong>with</strong> meals, <strong>with</strong> gradual doseescalation, to reduce the gastrointestinal side effects due to met<strong>for</strong>min• Coadministration of <strong>JANUMET</strong> <strong>XR</strong> <strong>with</strong> an insulin secretagogue (eg, sulfonylurea) orinsulin may require lower doses of the insulin secretagogue or insulin to reduce therisk of hypoglycemiaSelected Important Risk In<strong>for</strong>mation50/1000 mg50/1000 mgTablets not shownat actual size.WARNING: LACTIC ACIDOSISLactic acidosis is a rare, but serious complication that can occur dueto met<strong>for</strong>min accumulation. The risk increases <strong>with</strong> conditions such assepsis, dehydration, excess alcohol intake, hepatic impairment, renalimpairment, and acute congestive heart failure.The onset of lactic acidosis is often subtle, accompanied only bynonspecific symptoms such as malaise, myalgias, respiratory distress,increasing somnolence, and nonspecific abdominal distress.Laboratory abnormalities include low pH, increased anion gap, andelevated blood lactate.If acidosis is suspected, <strong>JANUMET</strong> <strong>XR</strong> should be discontinued and thepatient hospitalized immediately [see Warnings and Precautions].(Selected Important Risk In<strong>for</strong>mation continues on the next page.)Be<strong>for</strong>e prescribing <strong>JANUMET</strong> <strong>XR</strong>, please read the Prescribing In<strong>for</strong>mation,including the Boxed Warning about lactic acidosis.Page 1 of 3
As an adjunct to diet and exercise <strong>for</strong> appropriate patients <strong>with</strong> type 2 diabetes<strong>JANUMET</strong> <strong>XR</strong>OFFERS POWERFUL A1C REDUCTIONS 1,2Mean change in A1C, %0–1–2–3–49.8%Met<strong>for</strong>min 2000 mg <strong>daily</strong>(n=564)–1.8%In a clinical trial including sitagliptin + met<strong>for</strong>min immediate-release (IR) FDCGreater A1C reductions vsmet<strong>for</strong>min IR alone at week 18 aPrimary end pointMean baseline A1C:P Median (9.7%)Mean baseline A1C: 8.4%11.4%Met<strong>for</strong>min 2000 mg <strong>daily</strong> Sitagliptin + met<strong>for</strong>min Met<strong>for</strong>min 2000 mg <strong>daily</strong> Sitagliptin + met<strong>for</strong>min(n=291)100/2000 mg <strong>daily</strong>(n=273)100/2000 mg <strong>daily</strong>–1.1%(n=288)(n=271)P
IN THIS STUDY, SIMILAR WEIGHT CHANGE,RATES OF HYPOGLYCEMIA, AND GI EVENTSVS METFORMIN IR ALONE 1• Weight loss <strong>for</strong> sitagliptin + met<strong>for</strong>min IR FDC similar to met<strong>for</strong>min IR alone at week 18 (LS mean change from baseline: –3.5 lb <strong>for</strong> both groups)• Incidence of hypoglycemia <strong>for</strong> sitagliptin + met<strong>for</strong>min IR FDC similar to met<strong>for</strong>min IR alone over 18 weeks (2.1% [n/N=13/625] vs 1.8% [n/N=11/621], respectively)• Similar rate of GI adverse events vs met<strong>for</strong>min IR alone over 18 weeksWhen added to a sulfonylurea (glimepiride) or insulin, patients treated <strong>with</strong> sitagliptin + met<strong>for</strong>min IR experiencedincreased weight and incidence of hypoglycemia• Weight gain: +0.9 lb <strong>for</strong> patients treated <strong>with</strong> sitagliptin + met<strong>for</strong>min IR + glimepiride vs –1.5 lb <strong>for</strong> placebo + met<strong>for</strong>min IR + glimepiride• Hypoglycemia: 16% <strong>for</strong> patients treated <strong>with</strong> sitagliptin + met<strong>for</strong>min IR + glimepiride vs 1% <strong>for</strong> placebo + met<strong>for</strong>min IR + glimepiride and 15% <strong>for</strong> patients treated <strong>with</strong>sitagliptin + met<strong>for</strong>min IR + insulin vs 8% <strong>for</strong> placebo + met<strong>for</strong>min IR + insulin. A lower dose of sulfonylurea or insulin may be required to reduce the risk of hypoglycemiaGI = gastrointestinal.Please see Study Design on page 2 <strong>for</strong> more in<strong>for</strong>mation.Selected Important Risk In<strong>for</strong>mation (continued)Intravascular contrast studies <strong>with</strong> iodinated materials can lead to acutealteration of renal function and have been associated <strong>with</strong> lactic acidosis inpatients receiving met<strong>for</strong>min. There<strong>for</strong>e, in patients in whom any such studyis planned, <strong>JANUMET</strong> <strong>XR</strong> should be temporarily discontinued at the time of orbe<strong>for</strong>e the procedure, <strong>with</strong>held <strong>for</strong> 48 hours subsequent to the procedure, andreinstituted only after renal function has been re-evaluated and found tobe normal.There have been no clinical studies establishing conclusive evidence ofUse With Medications Known to Cause HypoglycemiaSitagliptinWhen sitagliptin was used in combination <strong>with</strong> a sulfonylurea or insulin,medications known to cause hypoglycemia, the incidence of hypoglycemiawas increased over that of placebo used in combination <strong>with</strong> a sulfonylurea orinsulin. There<strong>for</strong>e, patients also receiving insulin or an insulin secretagogue (eg,sulfonylurea) may require a lower dose of insulin or the insulin secretagogue toreduce the risk of hypoglycemia.The incidence (and rate) of hypoglycemia based on all reports of symptomatichypoglycemia were: 16.4% (0.82 episodes/patient-year) <strong>for</strong> sitagliptin 100 mg incombination <strong>with</strong> met<strong>for</strong>min and glimepiride, 0.9% (0.02 episodes/patient-year)<strong>for</strong> placebo in combination <strong>with</strong> met<strong>for</strong>min and glimepiride, 8.2% (0.61 episodes/patient-year) <strong>for</strong> placebo in combination <strong>with</strong> met<strong>for</strong>min and insulin, and 15.3%(0.98 episodes/patient-year) <strong>for</strong> sitagliptin in combination <strong>with</strong> met<strong>for</strong>minand insulin.Adverse reactions <strong>with</strong> sitagliptin in combination <strong>with</strong> met<strong>for</strong>min and rosiglitazonethrough Week 18 were: upper respiratory tract infection (sitagliptin, 5.5%; placebo,5.2%) and nasopharyngitis (6.1%, 4.1%). Through Week 54 they were: upperrespiratory tract infection (sitagliptin, 15.5%; placebo, 6.2%), nasopharyngitis(11.0%, 9.3%), peripheral edema (8.3%, 5.2%), and headache (5.5%, 4.1%).Met<strong>for</strong>min hydrochlorideHypoglycemia does not occur in patients receiving met<strong>for</strong>min alone under usualcircumstances of use but could occur when caloric intake is deficient, whenstrenuous exercise is not compensated by caloric supplementation, or duringCopyright © 2013 Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc. All rights reserved.DIAB-1079801-0001 07/13Janumet<strong>XR</strong>.comconcomitant use <strong>with</strong> other glucose-lowering agents (such as sulfonylureas andinsulin) or ethanol. Elderly, debilitated, or malnourished patients and those <strong>with</strong>adrenal or pituitary insufficiency or alcohol intoxication are particularly susceptible tohypoglycemic effects.There have been postmarketing reports of serious hypersensitivity reactions inpatients treated <strong>with</strong> sitagliptin, one of the components of <strong>JANUMET</strong> <strong>XR</strong>, such asanaphylaxis, angioedema, and exfoliative skin conditions including Stevens-Johnsonsyndrome. Onset of these reactions occurred <strong>with</strong>in the first 3 months after initiationof treatment <strong>with</strong> sitagliptin, <strong>with</strong> some reports occurring after the first dose. If ahypersensitivity reaction is suspected, discontinue <strong>JANUMET</strong> <strong>XR</strong>, assess <strong>for</strong> otherpotential causes <strong>for</strong> the event, and institute alternative treatment <strong>for</strong> diabetes.Use caution in a patient <strong>with</strong> a history of angioedema to another dipeptidylpeptidase-4 (DPP-4) inhibitor because it is unknown whether such patients will bepredisposed to angioedema <strong>with</strong> <strong>JANUMET</strong> <strong>XR</strong>.In clinical studies, the most common adverse reactions reported, regardless ofinvestigator assessment of causality, in ≥5% of patients treated <strong>with</strong> eithersitagliptin in combination <strong>with</strong> met<strong>for</strong>min or placebo were as follows: diarrhea(7.5% vs 4.0%), upper respiratory tract infection (6.2% vs 5.1%), and headache(5.9% vs 2.8%). In patients treated <strong>with</strong> sitagliptin in combination <strong>with</strong> met<strong>for</strong>minand sulfonylurea or placebo in combination <strong>with</strong> met<strong>for</strong>min and sulfonylurea:hypoglycemia (16.4% vs 0.9%) and headache (6.9% vs 2.7%). In patients treated<strong>with</strong> sitagliptin in combination <strong>with</strong> met<strong>for</strong>min and insulin or placebo in combination<strong>with</strong> met<strong>for</strong>min and insulin: hypoglycemia (15.3% vs 8.2%). Other adverse events<strong>with</strong> an incidence of ≥5% included nasopharyngitis <strong>for</strong> sitagliptin monotherapy andhypoglycemia (13.7% vs 4.9%), diarrhea (12.5% vs 5.6%), and nausea (6.7% vs4.2%) <strong>for</strong> extended-release met<strong>for</strong>min vs placebo when added to glyburide.The incidence of selected gastrointestinal adverse reactions in patients treated <strong>with</strong>sitagliptin and met<strong>for</strong>min was similar to those of placebo and met<strong>for</strong>min: nausea(1.3%, 0.8%), vomiting (1.1%, 0.8%), abdominal pain (2.2%, 3.8%), and diarrhea(2.4%, 2.5%).Be<strong>for</strong>e prescribing <strong>JANUMET</strong> <strong>XR</strong>, please read the Prescribing In<strong>for</strong>mation,including the Boxed Warning about lactic acidosis.For additional copies of the Prescribing In<strong>for</strong>mation, please call 800-672-6372,visit Janumet<strong>XR</strong>.com, or contact your Merck representative.References: 1. Reasner C, Olansky L, Seck TL, et al. The effect of initial therapy <strong>with</strong> the fixed-dose combination of sitagliptin and met<strong>for</strong>min compared <strong>with</strong> met<strong>for</strong>min monotherapy in patients <strong>with</strong> type 2 diabetes mellitus. Diabetes ObesMetab. 2011;13(7):644–652. 2. Data available on request from Merck, Professional Services-DAP, WP1-27, PO Box 4, West Point, PA 19486-0004. Please specify in<strong>for</strong>mation package DIAB-1038791-0005. 3. Olansky L, Reasner C, Seck TL,et al. A treatment strategy implementing combination therapy <strong>with</strong> sitagliptin and met<strong>for</strong>min results in superior glycaemic control versus met<strong>for</strong>min monotherapy due to a low rate of addition of antihyperglycaemic agents. Diabetes ObesMetab. 2011;13(9):841–849.Page 3 of 3