DCS & HPCA – care in correctional services - Hospice Palliative ...
DCS & HPCA – care in correctional services - Hospice Palliative ...
DCS & HPCA – care in correctional services - Hospice Palliative ...

Create successful ePaper yourself
Turn your PDF publications into a flip-book with our unique Google optimized e-Paper software.
HEALTH CARE SERVICES IN THE<br />
DEPARTMENT OF CORRECTIONAL<br />
SERVICES<br />
PRESENTATION TO <strong>HPCA</strong> CONFERENCE<br />
18 SEPTEMBER 2012<br />
K M MABENA
Confidential<br />
1. Introduction.<br />
2. Background<br />
3. The most prevalent diseases<br />
4. Functions of the Directorate<br />
5. <strong>Palliative</strong> <strong>care</strong> <strong>in</strong> <strong>DCS</strong><br />
6. Challenges<br />
7. Recommendations<br />
PRESENTATION OVERVIEW<br />
Document ref number<br />
1
Confidential<br />
INTRODUCTION<br />
� Incarcerated persons represent a small proportion of the total South<br />
African population, who are also at risk of develop<strong>in</strong>g health and social<br />
problems.<br />
� International norms and standards require that <strong>in</strong>mates must have<br />
access to the same quality and range of health <strong>care</strong> <strong>services</strong> as the<br />
general public receives from the National Health Services. A person’s<br />
capacity to access these <strong>services</strong> should not be compromised by<br />
reasons of <strong>in</strong>carceration s<strong>in</strong>ce all people have a basic right to health,<br />
nutrition, clean and safe environment as obligated by the Constitution of<br />
the Republic of South Africa..<br />
� In terms of the Correctional Services Act, (Act 111 of 1998), the<br />
department provides primary health <strong>care</strong> <strong>services</strong> and refer patients to<br />
external health <strong>care</strong> facilities for secondary and tertiary levels of health<br />
<strong>care</strong>.<br />
� The Department has been faced with a number of challenges with<br />
regard to the provision of primary health <strong>services</strong> to the <strong>in</strong>mates.<br />
Document ref number<br />
2
Confidential<br />
INTRODUCTION (Cont’)<br />
� A number of offenders and remand deta<strong>in</strong>ees suffer from various<br />
illnesses with poor prognosis which are progressive and non-reversible.<br />
� Some offenders suffer from medical conditions which are related to<br />
ag<strong>in</strong>g and are progressive <strong>in</strong> nature.<br />
� Only a small number of these offenders are considered for placement on<br />
medical grounds and released before they can die whilst others die <strong>in</strong><br />
custody.<br />
� Seriously ill offenders and remand deta<strong>in</strong>ees can be categorized <strong>in</strong>to<br />
those with:<br />
� a term<strong>in</strong>al illness with poor prognosis;<br />
� Alzheimer’s and related dementia; and<br />
� a serious, progressive and non-reversible illness with poor prognosis,<br />
which has profound functional and cognitive impairments.<br />
� On referral to external health facilities offenders and remand deta<strong>in</strong>ees<br />
are discharged with recommendations that palliative <strong>care</strong> must be<br />
provided.<br />
Document ref number<br />
3
BACKGROUND<br />
� The department is comprised of six Regions (Eastern Cape, Free<br />
State/Northern Cape, KwaZulu-Natal, Limpopo/Mpumalanga/North<br />
West), 48 Management Areas (similar to District) and 242 Correctional<br />
Centres (similar to PHC facility).<br />
� There is at least one Primary Health Care (PHC) cl<strong>in</strong>ic per Correctional<br />
Centre and one <strong>in</strong>-patient facility /sickbay with beds rang<strong>in</strong>g from 5-120.<br />
� An <strong>in</strong>-patient facility is def<strong>in</strong>ed as a facility that has been established <strong>in</strong> a<br />
Correctional Centre for the purpose of accommodat<strong>in</strong>g <strong>in</strong>mates that are<br />
either ill or recover<strong>in</strong>g from post-operative procedures and cannot be<br />
accommodated <strong>in</strong> the general cells whilst on treatment. The facility<br />
usually does not meet the requirements for be<strong>in</strong>g classified as a<br />
hospital.<br />
� Patients requir<strong>in</strong>g palliative <strong>care</strong> are admitted <strong>in</strong> these facilities.<br />
� The department recruits health <strong>care</strong> professionals (professional nurses,<br />
pharmacists, medical practitioners, psychologists), spiritual <strong>care</strong> workers<br />
and social workers as members of the multidiscipl<strong>in</strong>ary team.<br />
� The health facilities have not been fully <strong>in</strong>tegrated <strong>in</strong>to the District Health<br />
System.
160000<br />
140000<br />
120000<br />
100000<br />
80000<br />
60000<br />
40000<br />
20000<br />
0<br />
BACKGROUND<br />
Total <strong>in</strong>mate population end July 2012<br />
EC FS.NC GP KZN LMN WC TOTAL<br />
Males 17692 20170 35537 24717 20500 24144 142760<br />
Females 300 288 1138 471 301 777 3275<br />
TOTAL 17992 20458 36675 25188 20801 24921 146035<br />
Males<br />
Females<br />
TOTAL
1200<br />
1000<br />
800<br />
600<br />
400<br />
200<br />
0<br />
BACKGROUND<br />
Females <strong>in</strong>mates end July 2012<br />
EC FS.NC GP KZN LMN WC<br />
Females
5628<br />
BACKGROUND<br />
Remand deta<strong>in</strong>ees vs the sentenced population<br />
12064<br />
49<br />
251<br />
MALE FEMALE MALE FEMALE<br />
REMAND DETAINEES SENTENCED OFFENDERS
THE MOST COMMON PREVALENT CONDITIONS AMONGST<br />
OFFENDERS<br />
Respiratory tract <strong>in</strong>fections: TB,<br />
pneumonia, asthma and bronchitis<br />
Sexually transmitted <strong>in</strong>fections, HIV<br />
and AIDS<br />
Cardiovascular (Hypertension)<br />
Gastro Intest<strong>in</strong>al Tract Illnesses<br />
(haemorrhoids, ulcers, gastritis)<br />
Mental health conditions<br />
Cancer<br />
Seasonal viral <strong>in</strong>fections<br />
Musculoskeletal conditions<br />
Ear, nose and throat conditions<br />
Neurological (epilepsy)<br />
Dermatological<br />
Endocr<strong>in</strong>e (diabetes)
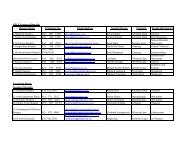
FUNCTIONS OF HEALTH CARE SERVICES IN THE<br />
DEPARTMENT<br />
COMPONENT CORE FUNCTION<br />
Primary Health<br />
Care<br />
Nutrition and<br />
Hygiene Services<br />
Pharmaceutical<br />
Services<br />
To facilitate the provision of Primary Health Care<br />
Services (<strong>in</strong>cludes disease prevention, health<br />
promotion, curative, rehabilitative and referral <strong>services</strong><br />
for secondary and tertiary <strong>services</strong>) .<br />
To facilitate the provision of basic food <strong>services</strong> <strong>in</strong> l<strong>in</strong>e<br />
with the applicable prescripts as well as personal and<br />
environmental hygiene <strong>services</strong> .<br />
To ensure implementation of the National Drug Policy<br />
and adequate supply of safe, cost effective drugs of<br />
acceptable quality and the rational use of medic<strong>in</strong>es by<br />
prescribers, dispensers and patients.
PALLIATIVE CARE IN <strong>DCS</strong><br />
� As the burden of diseases <strong>in</strong>creased, the need for palliative arouse<br />
<strong>in</strong> the Department.<br />
� This need was further <strong>in</strong>tensified after the Special Assignment<br />
documentary <strong>in</strong> 2008.<br />
� A relationship was established between <strong>DCS</strong> and <strong>HPCA</strong> <strong>in</strong> order to<br />
implement palliative <strong>care</strong> <strong>in</strong> <strong>DCS</strong>.<br />
� A recommendation was made and <strong>in</strong> consultation with KZN Region,<br />
decision was then taken to pilot palliative <strong>care</strong> there.<br />
� A plan was developed to address amongst others the follow<strong>in</strong>g:<br />
� Establishment of relationship with <strong>HPCA</strong>.<br />
� Approval by management of KZN Region.<br />
� Establishment of a multidiscipl<strong>in</strong>ary team.<br />
� Market<strong>in</strong>g of palliative <strong>care</strong> the officials, <strong>in</strong>mates and families.<br />
� Identification of pilot sites.<br />
� Resourc<strong>in</strong>g of the facilities.<br />
� Tra<strong>in</strong><strong>in</strong>g of the multidiscipl<strong>in</strong>ary team members and offenders (43 ).
SPECIFIC EQUIPMENT FOR PALLIATIVE CARE<br />
SPECIAL BED FOR A BED RIDDEN PATIENT IN DURBAN<br />
MED B.
A MIXED WARD IN DURBAN MED B FOR THE PROVISION<br />
OF PALLAITIVE CARE. CARE GIVER CLEANING THE<br />
WARD.
Some Of The Infrastructure Adaptations: Wall Mounted<br />
Central Oxygen Supply Po<strong>in</strong>ts <strong>in</strong> Durban Med B and Also A<br />
Mobile Unit For Backup
Mixed palliative <strong>care</strong> ward <strong>in</strong> Pietermaritzburg Med A (permanent<br />
Medical practitioner, patient and a Custodial Official
PALLIATIVE CARE IN <strong>DCS</strong><br />
� Order<strong>in</strong>g, storage and control of palliative <strong>care</strong> medic<strong>in</strong>es.<br />
� Conven<strong>in</strong>g of regular meet<strong>in</strong>gs to monitor progress and address<br />
challenges.<br />
� Development of record<strong>in</strong>g and report<strong>in</strong>g tools as well as system.<br />
� Review of visit<strong>in</strong>g policies to term<strong>in</strong>ally ill patients to allow for longer<br />
hours, contact visits, frequency, etc<br />
� Piloted successfully <strong>in</strong> Durban Westville and Pietermaritzburg.<br />
� SLA signed between KZN Region and <strong>HPCA</strong> <strong>in</strong> October 2009.<br />
Role and support of <strong>HPCA</strong>:<br />
� Facilitation of tra<strong>in</strong><strong>in</strong>g,<br />
� Mentor<strong>in</strong>g.<br />
� Establishment of referral systems.<br />
� Ward rounds (Durban).<br />
� Establishment of records systems.
SIGNING OF THE SLA IN 2009 IN DURBAN: US EMBASSY REP,<br />
ACT DEPUTY REGIONAL COMMISSIONER, CEO OF <strong>HPCA</strong><br />
AND DIR HEALTH
A medical practitioner car<strong>in</strong>g for a patient
PALLIATIVE CARE IN <strong>DCS</strong><br />
� A national Memorandum of Understand<strong>in</strong>g has been approved and<br />
signed by the National Commissioner and the CEO of <strong>HPCA</strong> <strong>in</strong> May<br />
2012.<br />
� A need was identified to roll out palliative <strong>care</strong> start<strong>in</strong>g <strong>in</strong> 2<br />
Management Areas per Region.<br />
� <strong>HPCA</strong> has sought fund<strong>in</strong>g to cont<strong>in</strong>ue support<strong>in</strong>g the <strong>DCS</strong> <strong>in</strong> the<br />
implementation of palliative <strong>care</strong>.<br />
� These Management Areas are at different levels of preparation.<br />
� A number of professional nurses are currently attend<strong>in</strong>g tra<strong>in</strong><strong>in</strong>g on<br />
palliative <strong>care</strong>.<br />
� Spiritual Care has become part of the of multidiscipl<strong>in</strong>ary team <strong>in</strong> the<br />
provision of palliative <strong>care</strong> to the <strong>in</strong>mates <strong>in</strong> <strong>DCS</strong> and the chapla<strong>in</strong>s<br />
had a tra<strong>in</strong><strong>in</strong>g workshop on bereavement counsell<strong>in</strong>g.<br />
� <strong>HPCA</strong> has facilitated a session for the draft<strong>in</strong>g of Guidel<strong>in</strong>es on the<br />
Provision of <strong>Palliative</strong> Care <strong>in</strong> Correctional Services.
DR. LIZ GWYTHER HANDING OUT CERTIFICATES TO<br />
OFFENDERS WHO COMPLETED PALLIATIVE CARE TRAINING<br />
2011
BENEFITS OF PALLIATIVE CARE IN <strong>DCS</strong><br />
• <strong>Palliative</strong> <strong>care</strong> ma<strong>in</strong>ta<strong>in</strong>s quality of life by address<strong>in</strong>g physical<br />
symptoms such as pa<strong>in</strong> or nausea as well as help<strong>in</strong>g with emotional,<br />
spiritual and social needs of the term<strong>in</strong>ally ill.<br />
• The <strong>in</strong>mate population becomes more <strong>in</strong>formed on palliative <strong>care</strong>.<br />
• Improved confidence amongst health <strong>care</strong> providers.<br />
• Provision of a higher quality of comprehensive health <strong>care</strong> to the<br />
<strong>in</strong>mate patient population.<br />
• Strengthen<strong>in</strong>g relationships amongst the patients and their families<br />
as well as the multidiscipl<strong>in</strong>ary team members.
PALLIATIVE CARE AND MEDICAL PAROLE<br />
• Correctional Matters Amendment Act- May 2012.<br />
• Regulations <strong>–</strong> February 2012.<br />
• Policy and procedures - February 2012.<br />
• Launch of Medical Parole Advisory Board.<br />
• Criteria:<br />
� Chronic disease, progressive, irreversible and term<strong>in</strong>al.<br />
� Medical conditions (<strong>in</strong>fectious and non-<strong>in</strong>fectious)<br />
• A number of patients recommended for medical parole and<br />
released.<br />
• Those without external support (reluctance by families and lost<br />
contact with friend and families) kept <strong>in</strong> Correctional facilities and<br />
provided with palliative <strong>care</strong>.
Confidential<br />
Health facilities:<br />
� The designs of Correctional Centres were focused on security and<br />
do not complement health <strong>care</strong> delivery for patients, result<strong>in</strong>g <strong>in</strong><br />
<strong>in</strong>adequate primary health <strong>care</strong> cl<strong>in</strong>ics and <strong>in</strong>-patient facilities that<br />
are not up to standard regard<strong>in</strong>g the equipment, <strong>in</strong>-patient facilities<br />
and isolation cells. In some areas, cells and offices have been<br />
converted <strong>in</strong>to primary health <strong>care</strong> cl<strong>in</strong>ics.<br />
Attitudes:<br />
CHALLENGES<br />
There was “Fear of the unknown” and resistance to change.<br />
Document ref number<br />
22
Confidential<br />
Human resources:<br />
CHALLENGES (Cont’)<br />
� The <strong>in</strong>ability to recruit and reta<strong>in</strong> health <strong>care</strong> professionals<br />
(professional nurses, medical practitioners, pharmacists and<br />
psychologists),<br />
� Lack of a structure for other categories of health <strong>care</strong> professionals<br />
(dietitians, enrolled nurs<strong>in</strong>g assistants, nurs<strong>in</strong>g assistants,<br />
pharmacist assistants, emergency medical <strong>services</strong> etc).<br />
� Lack of mechanisms to address tra<strong>in</strong><strong>in</strong>g needs for emerg<strong>in</strong>g<br />
diseases, patients’ needs such as palliative <strong>care</strong> and new treatment<br />
guidel<strong>in</strong>es; hence the Department is dependent on over-stretched<br />
Districts.<br />
Lack of supplies and other pharmaceuticals<br />
� Lack of adequate and access to pa<strong>in</strong> medication when required.<br />
Document ref number<br />
23
CATEGORY TOTAL NO.<br />
Prof nurses 820<br />
Medical<br />
practitioners<br />
8<br />
Pharmacists 21<br />
Community<br />
Service<br />
Pharmacists<br />
13<br />
Psychologists 16<br />
Spiritual Care<br />
Workers<br />
1427<br />
Social Workers 650<br />
HUMAN RESOURCE CAPACITY
Confidential<br />
IMPACT OF INADEQUATE RESOURCES<br />
� Limited or <strong>in</strong>adequate management of diseases which may lead to<br />
complications and deaths.<br />
� Increased spread of communicable diseases and deaths due to lack of<br />
adequate prevention, health promotion and timeous curative <strong>care</strong>.<br />
� Increased referrals to external health <strong>care</strong> providers even for <strong>in</strong>fections<br />
that could be treated at primary health <strong>care</strong> level result<strong>in</strong>g <strong>in</strong> <strong>in</strong>creased<br />
health <strong>care</strong> costs and security risks.<br />
� Limited or <strong>in</strong>adequate provision of palliative <strong>care</strong> which leads to more<br />
suffer<strong>in</strong>g by the patients.<br />
� Limited access to medical <strong>services</strong> result<strong>in</strong>g <strong>in</strong> delays on some<br />
<strong>in</strong>terventions, e.g. prescription of pa<strong>in</strong> medication.<br />
� Management Areas without access to departmental pharmacies utilize<br />
retail pharmacies for the procurement of medication and the costs are<br />
higher than the public tender prices and delays <strong>in</strong> provid<strong>in</strong>g pa<strong>in</strong><br />
medication to the patients.<br />
Document ref number<br />
25
RECOMMENDATIONS<br />
• Need for management leadership and commitment for palliative<br />
to be a success. All role players to cont<strong>in</strong>ue advocat<strong>in</strong>g for palliative<br />
<strong>care</strong> <strong>in</strong> Correctional environments.<br />
• Evidence-based practice: policies and programmes must be<br />
reviewed and/or developed based upon established need, on<br />
empirical evidence of effectiveness, and evaluated models of<br />
palliative <strong>care</strong> best practices<br />
• Health standards and cont<strong>in</strong>uity of <strong>care</strong> and treatment: the<br />
department must ensure that it meets <strong>in</strong>ternational obligations to<br />
provide health <strong>care</strong> which is equivalent to that available to the<br />
outside population, and to ensure cont<strong>in</strong>uity of <strong>care</strong> and not let<br />
<strong>in</strong>mates suffer.<br />
• Conditions: they must not violate the <strong>in</strong>mates rights to dignity.<br />
• Tra<strong>in</strong><strong>in</strong>g and support : all relevant professionals must be provided<br />
with the knowledge, tra<strong>in</strong><strong>in</strong>g, and support on palliative <strong>care</strong><br />
necessary to meet the requirements and responsibilities of their<br />
work.
RECOMMENDATIONS (Cont’)<br />
• International, national, and regional collaboration: South Africa<br />
and <strong>HPCA</strong> to share knowledge and expertise on effective palliative<br />
<strong>care</strong> with<strong>in</strong> the Correctional environment both nationally and<br />
<strong>in</strong>ternationally and to enhance the development of evidence-based<br />
practices <strong>in</strong> this area.<br />
• Fund<strong>in</strong>g and resources: The Department to develop and<br />
implement national fund<strong>in</strong>g plans to address palliative <strong>care</strong> at<br />
national, regional, and local levels.
Confidential<br />
CONCLUSION<br />
With the assistance and collaboration ALL RELEVANT STAKEHOLDERS,<br />
the Department rema<strong>in</strong>s committed <strong>in</strong> improv<strong>in</strong>g health <strong>care</strong> <strong>services</strong><br />
rendered to those entrusted to its <strong>care</strong> despite the numerous challenges it is<br />
faced with.<br />
Document ref number<br />
28
Thank you