MVP Medco Mail Order Form
MVP Medco Mail Order Form
MVP Medco Mail Order Form

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
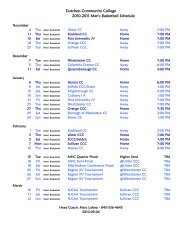
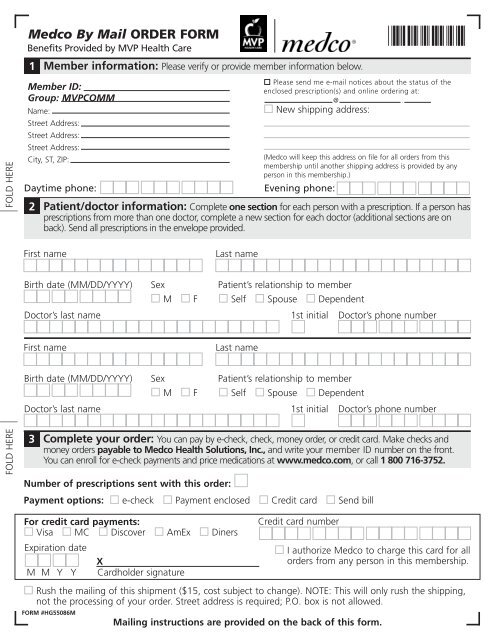
FOLD HERE FOLD HERE<strong>Medco</strong> By <strong>Mail</strong> ORDER FORMBenefits Provided by <strong>MVP</strong> Health Care13Member information: Please verify or provide member information below.Member ID:Group: <strong>MVP</strong>COMMName:Street Address:Street Address:Street Address:City, ST, ZIP:Daytime phone:2Complete your order: You can pay by e-check, check, money order, or credit card. Make checks andmoney orders payable to <strong>Medco</strong> Health Solutions, Inc., and write your member ID number on the front.You can enroll for e-check payments and price medications at www.medco.com, or call 1 800 716-3752.Number of prescriptions sent with this order:Payment options: e-check Payment enclosed Credit card Send bill*6101*Please send me e-mail notices about the status of theenclosed prescription(s) and online ordering at:@ .New shipping address:(<strong>Medco</strong> will keep this address on file for all orders from thismembership until another shipping address is provided by anyperson in this membership.)Evening phone:Patient/doctor information: Complete one section for each person with a prescription. If a person hasprescriptions from more than one doctor, complete a new section for each doctor (additional sections are onback). Send all prescriptions in the envelope provided.First nameBirth date (MM/DD/YYYY)Doctor’s last nameFirst nameBirth date (MM/DD/YYYY)Doctor’s last nameSexMSexMFFLast namePatient’s relationship to memberSelf Spouse DependentLast name1st initialPatient’s relationship to memberSelf Spouse Dependent1st initialDoctor’s phone numberDoctor’s phone numberFor credit card payments:Visa MC Discover AmEx DinersExpiration dateXM M Y Y Cardholder signatureCredit card numberI authorize <strong>Medco</strong> to charge this card for allorders from any person in this membership.Rush the mailing of this shipment ($15, cost subject to change). NOTE: This will only rush the shipping,not the processing of your order. Street address is required; P.O. box is not allowed.FORM #HG55086MX00000-00000-000-0000 7/06<strong>Mail</strong>ing instructions are provided on the back of this form.
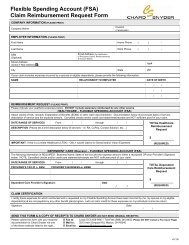
Patient/doctor information continuedFirst nameLast nameBirth date (MM/DD/YYYY)SexMFPatient’s relationship to memberSelf Spouse DependentDoctor’s last name1st initial Doctor’s phone numberFirst nameLast nameFOLD HERE FOLD HEREBirth date (MM/DD/YYYY)Doctor’s last nameSexMImportant reminders and other informationCheck that your doctor has prescribed the maximumdays’ supply allowed by your plan, plus refills for up to1 year, if appropriate (not a 30-day supply plus refills).Also, ask your doctor or pharmacist about safe,effective, and less expensive generic drugs.Complete the Health, Allergy & MedicationQuestionnaire.There may be a limit to the balance that you can carryon your account. If this order takes you over the limit, youmust include payment. Avoid delays in processing byusing e-checks or a credit card. (See Section 3 for details.)If you are a Medicare Part B beneficiary ANDhave private health insurance, check yourprescription drug benefit materials to determine thebest way to get Medicare Part B drugs and supplies. Or,call Member Services at 1 800 716-3752. To verifyMedicare Part B prescription coverage, call Medicare at1 800 MEDICARE (1 800 633-4227).FPatient’s relationship to memberSelf Spouse Dependent1st initialDoctor’s phone numberAutomatic generic equivalent substitution ofcertain brand-name drugs is allowed by law inTexas, Florida, and Ohio, unless you or your doctorspecifically directs otherwise.If you live in Texas, you have a right to refuse safe,effective generics. Check the box if you do not wantthe less expensive, generic drug. This applies only tothe prescription drug(s) on this order.Pennsylvania law permits pharmacists to substitutea less expensive generically equivalent drug for abrand name drug unless you or your physician directotherwise. Check the box if you do not wish a lessexpensive brand or generic drug “product.”Please note that this applies only to new prescriptionsand to any future refills of that prescription.For additional information or help, visit us atwww.medco.com or call Member Services at 1 800 716-3752.TTY/TDD users should call 1 800 759-1089.Place your prescription(s), this form,and your payment in the envelopeprovided. Be sure the <strong>Medco</strong> addressshows through the window. Do not usestaples or paper clips.FORM #HG55086MMEDCO HEALTH SOLUTIONS OF NETPARK, L.L.C.PO BOX 30493TAMPA FL 33630-3493!3363034936!