Role of radiology and imaging in the daignosis of ... - Orion Group
Role of radiology and imaging in the daignosis of ... - Orion Group
Role of radiology and imaging in the daignosis of ... - Orion Group

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
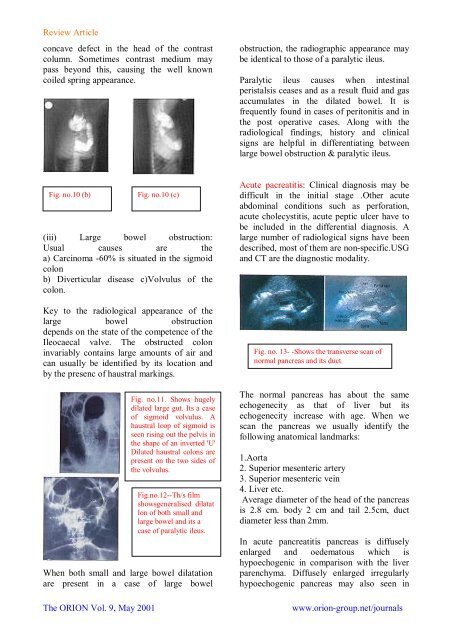
Review Articleconcave defect <strong>in</strong> <strong>the</strong> head <strong>of</strong> <strong>the</strong> contrastcolumn. Sometimes contrast medium maypass beyond this, caus<strong>in</strong>g <strong>the</strong> well knowncoiled spr<strong>in</strong>g appearance.obstruction, <strong>the</strong> radiographic appearance maybe identical to those <strong>of</strong> a paralytic ileus.Paralytic ileus causes when <strong>in</strong>test<strong>in</strong>alperistalsis ceases <strong>and</strong> as a result fluid <strong>and</strong> gasaccumulates <strong>in</strong> <strong>the</strong> dilated bowel. It isfrequently found <strong>in</strong> cases <strong>of</strong> peritonitis <strong>and</strong> <strong>in</strong><strong>the</strong> post operative cases. Along with <strong>the</strong>radiological f<strong>in</strong>d<strong>in</strong>gs, history <strong>and</strong> cl<strong>in</strong>icalsigns are helpful <strong>in</strong> differentiat<strong>in</strong>g betweenlarge bowel obstruction & paralytic ileus.Fig. no.10 (b)(iii) Large bowel obstruction:Usual causes are <strong>the</strong>a) Carc<strong>in</strong>oma -60% is situated <strong>in</strong> <strong>the</strong> sigmoidcolonb) Diverticular disease c)Volvulus <strong>of</strong> <strong>the</strong>colon.Key to <strong>the</strong> radiological appearance <strong>of</strong> <strong>the</strong>large bowel obstructiondepends on <strong>the</strong> state <strong>of</strong> <strong>the</strong> competence <strong>of</strong> <strong>the</strong>Ileocaecal valve. The obstructed colon<strong>in</strong>variably conta<strong>in</strong>s large amounts <strong>of</strong> air <strong>and</strong>can usually be identified by its location <strong>and</strong>by <strong>the</strong> presenc <strong>of</strong> haustral mark<strong>in</strong>gs.When both small <strong>and</strong> large bowel dilatationare present <strong>in</strong> a case <strong>of</strong> large bowelThe ORION Vol. 9, May 2001Fig. no.10 (c)Fig. no.11. Shows hugelydilated large gut. Its a case<strong>of</strong> sigmoid volvulus. Ahaustral loop <strong>of</strong> sigmoid isseen ris<strong>in</strong>g out <strong>the</strong> pelvis <strong>in</strong><strong>the</strong> shape <strong>of</strong> an <strong>in</strong>verted 'U'Dilated haustral colons arepresent on <strong>the</strong> two sides <strong>of</strong><strong>the</strong> volvulus.Fig.no.12--Th/s filmshowsgeneralised dilatatlon <strong>of</strong> both small <strong>and</strong>large bowel <strong>and</strong> its acase <strong>of</strong> paralytic ileus.Acute pacreatitis: Cl<strong>in</strong>ical diagnosis may bedifficult <strong>in</strong> <strong>the</strong> <strong>in</strong>itial stage .O<strong>the</strong>r acuteabdom<strong>in</strong>al conditions such as perforation,acute cholecystitis, acute peptic ulcer have tobe <strong>in</strong>cluded <strong>in</strong> <strong>the</strong> differential diagnosis. Alarge number <strong>of</strong> radiological signs have beendescribed, most <strong>of</strong> <strong>the</strong>m are non-specific.USG<strong>and</strong> CT are <strong>the</strong> diagnostic modality.Fig. no. 13- -Shows <strong>the</strong> transverse scan <strong>of</strong>normal pancreas <strong>and</strong> its duct.The normal pancreas has about <strong>the</strong> sameechogenecity as that <strong>of</strong> liver but itsechogenecity <strong>in</strong>crease with age. When wescan <strong>the</strong> pancreas we usually identify <strong>the</strong>follow<strong>in</strong>g anatomical l<strong>and</strong>marks:1.Aorta2. Superior mesenteric artery3. Superior mesenteric ve<strong>in</strong>4. Liver etc.Average diameter <strong>of</strong> <strong>the</strong> head <strong>of</strong> <strong>the</strong> pancreasis 2.8 cm. body 2 cm <strong>and</strong> tail 2.5cm, ductdiameter less than 2mm.In acute pancreatitis pancreas is diffuselyenlarged <strong>and</strong> oedematous which ishypoechogenic <strong>in</strong> comparison with <strong>the</strong> liverparenchyma. Diffusely enlarged irregularlyhypoechogenic pancreas may also seen <strong>in</strong>www.orion-group.net/journals