

Management of Proximal Femoral Fractures 2011 - aagbi
Management of Proximal Femoral Fractures 2011 - aagbi
Management of Proximal Femoral Fractures 2011 - aagbi

You also want an ePaper? Increase the reach of your titles
YUMPU automatically turns print PDFs into web optimized ePapers that Google loves.
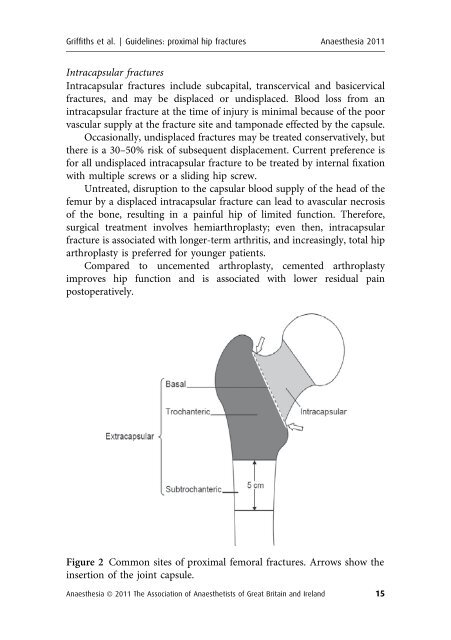
Griffiths et al. | Guidelines: proximal hip fractures Anaesthesia <strong>2011</strong>Intracapsular fracturesIntracapsular fractures include subcapital, transcervical and basicervicalfractures, and may be displaced or undisplaced. Blood loss from anintracapsular fracture at the time <strong>of</strong> injury is minimal because <strong>of</strong> the poorvascular supply at the fracture site and tamponade effected by the capsule.Occasionally, undisplaced fractures may be treated conservatively, butthere is a 30–50% risk <strong>of</strong> subsequent displacement. Current preference isfor all undisplaced intracapsular fracture to be treated by internal fixationwith multiple screws or a sliding hip screw.Untreated, disruption to the capsular blood supply <strong>of</strong> the head <strong>of</strong> thefemur by a displaced intracapsular fracture can lead to avascular necrosis<strong>of</strong> the bone, resulting in a painful hip <strong>of</strong> limited function. Therefore,surgical treatment involves hemiarthroplasty; even then, intracapsularfracture is associated with longer-term arthritis, and increasingly, total hiparthroplasty is preferred for younger patients.Compared to uncemented arthroplasty, cemented arthroplastyimproves hip function and is associated with lower residual painpostoperatively.Figure 2 Common sites <strong>of</strong> proximal femoral fractures. Arrows show theinsertion <strong>of</strong> the joint capsule.Anaesthesia ª <strong>2011</strong> The Association <strong>of</strong> Anaesthetists <strong>of</strong> Great Britain and Ireland 15













